dm-dental
DESCRIPTION
jurnalTRANSCRIPT
R ESEA R C H A N D P R A C T IC E
The Potential for Glycemic Control Monitoring and Screening for Diabetes at Dental Visits Using Oral Blood| Shiela M. Strauss, PhD, Mary T. Rosedale, PhD, PMHNP-BC, NEA-BC, Michael A. Pesce, PhD, David M. Rindskopf, PhD, Navjot Kaur, RN, Caroline M. Juterbock, RN, Mark S. Wolff, DDS, PhD, Dolores Malaspina, MD, MS, MSPH, and Ann Danoff, MD
Objectives. We examined the potential for glycemic control monitoring and screening for diabetes in a dental setting among adults (n = 408) with or at risk for diabetes.
Methods. In 2013 and 2014, we performed hemoglobin A1c (HbA1c) tests on dried blood samples of gingival crevicular blood and compared these with paired "gold-standard" HbA1c tests with dried finger-stick blood samples in New York City dental clinic patients. We examined differences in sociodemographics and diabetes-related risk and health care characteristics for 3 groups of at-risk patients.
Results. About half of the study sample had elevated HbA1c values in the combined prediabetes and diabetes ranges, with approximately one fourth of those in the diabetes range. With a correlation of 0.991 between gingival crevicular and finger-stick blood HbA1c, measures of concurrence between the tests were extremely high for both elevated HbA1c and diabetes-range HbA1c levels. Persons already diagnosed with diabetes and undiagnosed persons aged 45 years or older could especially benefit from HbA1c testing at dental visits.
Conclusions. Gingival crevicular blood collected at the dental visit can be used to screen for diabetes and monitor glycemic control for many at-risk patients. (Am J Public Health. 2015;105:796-801. doi:10.2105/AJPH.2014.302357)
Although diabetes has reached epidemic proportions in the United States,1 many diabetes complications could be mitigated by early detection coupled with lifestyle modification and therapeutic interventions to optimize glycemic control.2 Unfortunately, 8.1 million of the 29.1 million persons in the United States who have diabetes are undiagnosed,3 and among those diagnosed with diabetes, many are not likely to have received regular testing to monitor their glycemic control.4 An additional 86 million US adults have prediabetes, a condition that often progresses to diabetes, but only 11.1% of these persons have been told of their condition.3 Importantly, early identification and treatment of prediabetes can interrupt its progression.5,6 Thus, more opportunities are needed to screen for prediabetes and diabetes and to monitor glycemic control in those already diagnosed.
Because many persons in the United States visit a dental provider but not a primary care provider (PCP) each year,7 the dental visit may serve as an opportune site for diabetes screening and monitoring blood glucose.8-10 However, both dental patients and dental providers are accustomed to having dental providers only administer care in the mouth. In an earlier pilot study, we therefore investigated and demonstrated the acceptability and feasibility of using oral blood to screen for diabetes in persons with bleeding on dental probing.11,12 Many patients appreciated the use of oral blood for this screening, indicating that its collection felt like a routine dental cleaning, and most dental providers felt that the oral blood collection was fast and easy.12
In the current study, we refined our examination of the use of oral blood to screen for diabetes by implementing a laboratoiy-based approach to diabetes testing that enabled definitive and accurate analysis of all of the samples for which sufficient blood was collected. We included a large sample of patients (n = 408) at risk for diabetes or its
complications who presented for regular dental visits at a dental college’s comprehensive care clinics. We analyzed the sociodemographic and diabetes risk-related characteristics of the sample, and compared the results of diabetes screening and glycemic control monitoring with dried blood samples of gingival crevicular blood (GCB) and gold-standard finger-stick blood (FSB) to determine the validity of using GCB for this purpose. This screening and monitoring was performed by testing the samples for hemoglobin A le (HbAlc), a test promoted by the American Diabetes Association for diabetes diagnostic purposes and glycemic control monitoring.2 By providing an average measure of glycemic control over a 3-month period, this test is especially advantageous because fasting is not needed for HbAlc assessment, and no acute perturbations (e.g., stress, diet, exercise) affect HbAlc.2 Finally, we examined the potential benefits of this approach to diabetes screening and glycemic control monitoring according to whether study
participants had previous-year tests for blood glucose and previous-year visits to PCPs and dental providers.
METHODS
Study recruitment, participation, and data collection took place in the comprehensive care clinics at the New York University College of Dentistry from June 2013 to April 2014.
Study ParticipantsPersons were eligible for the research if they
indicated that their gums bled on brushing or flossing and if they (1) were aged at least 18 years; (2) did not require antibiotics before dental treatment; (3) did not have a history of severe cardiovascular, hepatic, immunologic, renal, hematologic, or other organ impairment; and (4) had been told by a health care provider that they had diabetes (group 1) or they were at risk for diabetes according to American Diabetes Association criteria (groups 2 and 3).2
796 I Research and Practice | Peer Reviewed | Strauss et al. American Journal o f Public Health | April 2015, Vol 105, No. 4

These criteria included (1) being aged at least 45 years (group 2) or (2) being aged between 18 and 44 years, having a body mass index (BMI; defined as weight in kilograms divided by the square of height in meters [kg/m2]) of 25 kg/m2 or greater, and having at least 1 of the following additional diabetes risk factors: little or no exercise on a given day; first-degree relative (parent or sibling) with diabetes; Latino ethnicity; Black, Native American, or Pacific Islander race; or being a woman who gave birth to a baby weighing 9 pounds or more (group 3).
Study ProceduresResearch assistants recruited New York
University College of Dentistry patients when the patients were seated in the clinics’ waiting areas before their scheduled dental appointments, where they were screened for study eligibility. The research assistants oversaw the eligible participant’s completion of a 30-minute survey that assessed sociodemographic characteristics and health care utilization. With the patient seated in the dental chair for the dental procedure, the research assistants collected two 10-pm blood samples (FSB and GCB) with micropipettes. The 2 samples were placed on separate Whatman 903 filter papers (GE Healthcare, Bio-Sciences Corp, Westborough, MA), labeled with separate identification codes, and allowed to dry for 1 hour at room temperature. They were then separately sealed in plastic bags, stored at 4°C, and transported to the laboratory for H bA lc analysis. Only research team members knew the correspondence between FSB and GCB identification codes; the laboratory was masked to this information and analyzed the samples as unique specimens for H bA lc testing.
The laboratory used a high-performance liquid chromatography D-10 program (Bio- Rad Laboratories Inc, Hercules, CA), which is traceable to the reference methods of both the National Glycohemoglobin Standardization Program and the International Federation of Clinical Chemistry and Laboratory Medicine, to analyze the blood samples for HbAlc.
Statistical MethodsWe assessed the study sample in terms of its
sododemographic and diabetes-related risk characteristics according to the 3 diabetes-related risk groups described in the study’s eligibility criteria
RESEARCH AND PRACTICE
We used x2 analysis to determine statistically significant differences among these groups and between pairs of these groups.
We measured central tendency, dispersion, and correlation of FSB H bAlc and GCB HbAl c; regression of GCB H bA lc on FSB HbAlc; and the proportion of the sample’s out-of-range FSB H bAlc and GCB H bA lc values in the prediabetes and diabetes ranges. We used these data and analyses, as well as those from 2 Receiver Operating Characteristic Curve (ROC) analyses, to determine GCB H bA lc values that could serve as criteria for positive diabetes screening and glycemic control monitoring results. These GCB H bA lc values correspond to elevated FSB FlbAlc readings (ie., in the prediabetes or diabetes ranges: > 5.7%) and diabetes-range readings (i.e., > 6.5%) We then assessed the concurrence of elevated H bA lc in FSB and GCB samples by using percent agreement and Cohen’s k .13 We also examined the specificity and sensitivity of elevated GCB HbAlc readings relative to gold-standard FSB HbAlc levels. In addition, we evaluated the predictive power of both a positive GCB HbAlc test (> 5.7%) and a negative GCB HbAlc test (< 5.7%). We similarly examined concurrence of HbAlc in the diabetes range in FSB and GCB samples. We performed all statistical analyses with IBM PASW version 21 (IBM, Somers, NY).
To determine whether H bA lc testing at the dental visit could benefit persons with or at risk for diabetes, we report the proportion of persons diagnosed with diabetes and for whom glycemic control monitoring would be especially helpful. We also used x2 analysis to determine the types of persons at risk for diabetes who could most benefit from diabetes screening based on whether they had previous-year testing for blood glucose and clinical visits to PCPs and dental providers within the previous year.
RESULTS
A total of 518 individuals volunteered to participate in the study, and 454 were eligible. Of these 454 individuals, we collected and measured an FSB sample for H bA lc from 441 participants. Paired H bA lc values from GCB were unavailable for 33 of these 441 participants: 17 were not collected because of insufficient bleeding on dental probing during the dental visit and 16 had insufficient oral
blood collected on filter paper for laboratory analysis. Thus, there were 408 eligible individuals in the study sample, all of whom had paired FlbAlc values from FSB and GCB specimens. On the basis of study eligibility criteria, we divided the study sample into 3 diabetes risk groups: group 1 with 67 persons; group 2 with 245 persons; and group 3 with 96 persons. It is notable that, like the persons in group 3, 54.7% of those in group 2 had a BMI of 25 kg/m2 or greater, as well as at least 1 additional diabetes risk factor.
As shown in Table 1, 56.9% of study participants were female, and two thirds either had some college education (23.4%) or had completed technical school or college (43.1%). Overall, 55.9% were aged between 45 and 64 years, and 18.9% were aged at least 65 years. Their allocations to the diabetes risk groups were dependent, in part, on both age and BMI. Thus, there were statistically significant differences between the groups in terms of age CP<.001), including for all pairwise group comparisons (P< .001). There were also statistically significant differences among the groups in terms of BMI of 25 kg/m2 or greater (P<,001), with groups 1 and 2 each differing significantly from group 3 (P<.001). In all, 70% of the study sample had a BMI of 25 kg/m2 or greater. The majority (59.9%) had little or no daily exercise.
Although there were no statistically significant differences in the 3 study sample groups regarding increased diabetes risk because of race (36.7% were Black, Native American, or Pacific Islander), there were statistically significant differences regarding increased risk for participants because of Latino ethnicity (P<.001). Latinos constituted almost half (46.9%) of the persons in group 3, compared with 29.9% in group 1 (P= .029) and 24.7% in group 2 (P<.001). The groups also differed significantly regarding having a parent or sibling with diabetes (P= .003). Almost two thirds (64.2%) of persons in group 1 had a first- degree relative with diabetes, compared with 40.8% in group 2 (P< .001) and 44.8% in group 3 (P= .015). There were also statistically significant differences among the groups regarding women who had a baby weighing at least 9 pounds at birth (17.6%, 4.9%, and 10.7% in groups 1, 2, and 3, respectively; P= .038), with women in group 1 differing significantly from women in group 2 (P= .011).
April 2015, Vol 105, No. 4 | American Journal o f Public Health Strauss et al. | Peer Reviewed | Research and Practice | 797

RESEARCH AND PRACTICE
TABLE 1—Sociodemographic and D iabetes-Related Risk Characteristics of a Sam ple of Dental Clinic Patients, by D iabetes Risk Groups:
New York City, 2 0 1 3 -2 0 1 4
C haracteristicGroup 1: Told H ad D iabe tes
(n - 6 7 ) , %Group 2: N o t Told H ad D iabe tes
and Aged > 4 5 Years (n = 2 4 5 ) , %Group 3: O ther3
(n - 9 6 ) , %Total
(n = 4 0 8 ) , %
Fem ale 5 0 .7 5 8 .0 5 8 .3 5 6 .9
A g e * * *
1 8 - 4 4 y 1 0 .4 0 .0 1 0 0 .0 2 5 .2
4 5 - 6 4 y 6 5 .7 7 5 .1 0 .0 5 5 .9
> 6 5 y 2 3 .9 2 4 .9 0 .0 1 8 .9
H ighest education
< high-school g raduate 3 7 .9 3 1 .7 3 4 .7 3 3 .4
S om e college 2 4 .2 2 0 .8 2 9 .5 2 3 .4
Technical school or college 3 7 .9 4 7 .5 3 5 .8 4 3 .1
graduate
BMI > 2 5 k g /m 2* * * 6 8 .7 5 8 .4 1 0 0 .0 7 0 .0
L ittle or no dally exercise 6 1 .2 5 8 .8 6 1 .5 5 9 .9
F irs t-degree re lative with 6 4 .2 4 0 .8 4 4 .8 4 5 .6
d ia b e te s **
Latino e th n ic ity * * * 2 9 .9 2 4 .7 4 6 .9 3 0 .8
Black, N ative A m erican, or Pacific 4 3 .1 3 6 .4 3 3 .3 3 6 .7
Is lander race
Am ong w om en, had baby > 9 1 7 .6 4 .9 1 0 .7 8 .2
p ounds*
Note. BM I = body m ass index (de fin ed as weight in kilogram s divided by th e square o f height in m eters).aN ot to ld he or she had d ia be tes , aged 1 8 - 4 4 y, BMI > 2 5 k g /m 2, and > 1 o f the fo llow ing ad d itio n a l d ia be tes risk factors: little or no exercise on a given day; firs t-degree re la tive (p a re n t, s ib ling) with d iabe tes ; Latino ethnicity; Black, N ative Am erican , or Pacific Is lander race; w om an who gave b irth to a baby > 9 pounds.* P < .0 5 ; * * P < .0 1 ; * * * P < . 0 0 1 .
Concurrence of Hemoglobin A le Values
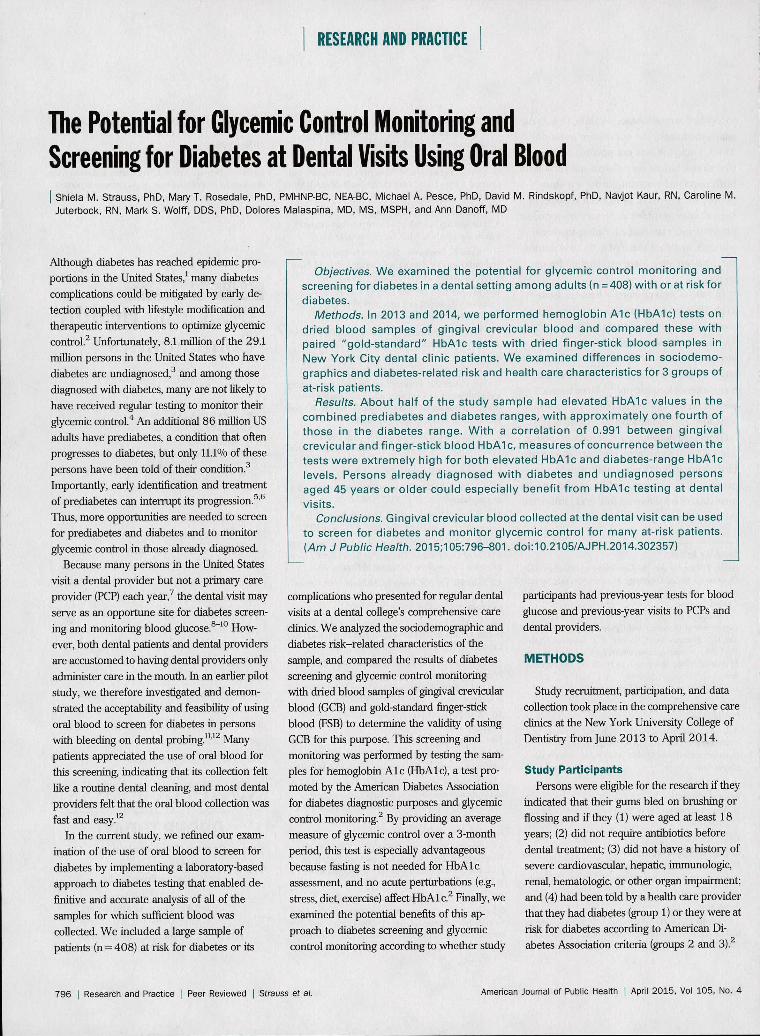
in Paired Blood Sam plesAs shown in Figure 1, HbAl c values assessed
with FSB and GCB were nearly identical, with a correlation of 0.991. Finger-stick blood HbAlc ranged from 4.2% to 10.8% and GCB HbAlc ranged from 4.1% to 10.9%. Each of the 2 FlbAlc measures had a mean of 5.9%, a median of 5.7%, a standard deviation of 0.93, and a standard error of the mean of 0.046. A regression analysis in which GCB FlbAlc was regressed on FSB HbAlc yielded
(1) GCB FFbAlc = 0.060 + 0.987 * FSB HbAlc.
We determined that 5.7% and 6.5% were GCB HbAlc values that could serve as criteria for elevated and diabetes-range HbAlc results corresponding to elevated and diabetes-range K B HbAlc readings, respectively. This determination was made because (1) the means, medians, standard deviations, and standard
errors of the means were identical for the study sample’s FSB FlbAlc and GCB HbAlc values; (2) the correlation of the 2 HbAlc values was 0.991; (3) the regression of GCB HbAlc on FSB HbAlc had an intercept close to 0 and a slope of almost 1; and (4) in 2 ROC analyses, the sum of (1-sensitivity)2 plus (1-specificity)2 for the GCB HbAlc value of 5.7% as a criterion for elevated HbAlc and 6.5% as a criterion for diabetes-range HbAlc were each close to 0 (0.010 and 0.004, respectively). In the ROC analysis for elevated FlbAlc, the area under the ROC curve was 0.976, and in the analysis for diabetes-range HbAlc, the area under the ROC curve was 0.998.
Concurrence of Out-of-Range Hemoglobin
A le Values in Paired Blood Sam plesWe measured the concurrence of HbAlc
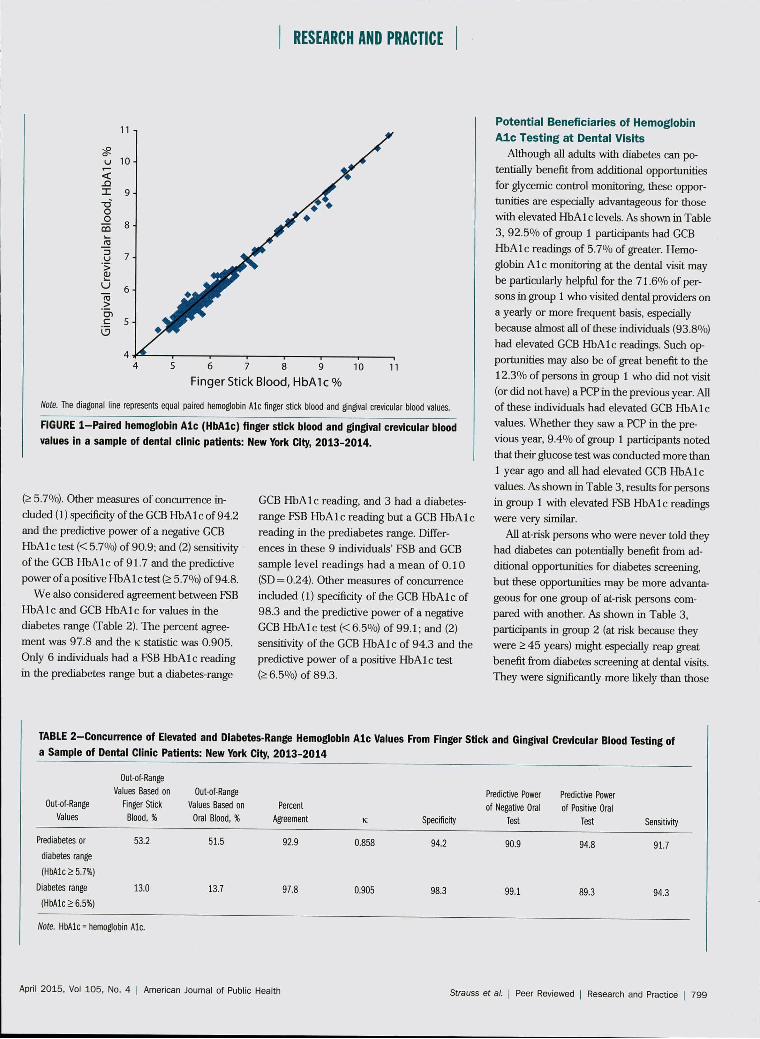
values in the FSB and GCB samples for both elevated HbAlc levels and for HbAlc levels in the diabetes range. As shown in Table 2,
53.2% of the study sample had FSB HbAlc values in the prediabetes or diabetes (elevated) ranges, including 13.0% in the diabetes range. When we measured HbAl c with GCB, 51.5% had elevated HbAlc values, including 13.7% in the diabetes range.
When we considered agreement between KB HbAlc and GCB HbAlc for elevated values in either prediabetes or diabetes ranges, the percent agreement was 92.9, remaining high at 85.8 when corrected for chance agreement as measured by k . Only 11 individuals had a normal FSB Hb A1 c reading but an elevated GCB HbAlc reading, and 18 had an elevated K B HbAlc reading but a normal GCB HbAlc reading. Although differences in these 29 individuals’ FSB and GCB sample level readings were small (mean = -0.03;SD = 0.23), a person whose HbAlc level was close to 5.7% could have 1 sample’s HbAlc level in the normal range (< 5.7%) and the other sample’s level in the elevated range
798 | Research and Practice | Peer Reviewed | Strauss et at. American Journal o f Public Health | April 2015, Vol 105, No. 4
RESEARCH AND PRACTICE
N ote . The d iagona l line represents equa l paired hem oglobin A le fin g er s tick b lood and gingival crev icu la r b lood values.
FIGURE 1 -P a ire d hemoglobin A le (H b A lc ) finger stick blood and gingival crevicular blood
values in a sam ple of dental clin ic patients: New York City, 2 0 1 3 -2 0 1 4 .
(> 5.7%). Other measures of concurrence included (1) specificity of the GCB H bA lc of 94.2 and the predictive power of a negative GCB H bA lc test (< 5.7%) of 90.9; and (2) sensitivity of the GCB H bA lc of 91.7 and the predictive power of a positive HbA 1 c test (> 5.7%) of 94.8.
We also considered agreement between FSB H bA lc and GCB H bA lc for values in the diabetes range (Table 2). The percent agreement was 97.8 and the k statistic was 0.905. Only 6 individuals had a FSB H bA lc reading in the prediabetes range but a diabetes-range
GCB H bA lc reading, and 3 had a diabetes- range FSB H bA lc reading but a GCB FlbAlc reading in the prediabetes range. Differences in these 9 individuals’ FSB and GCB sample level readings had a mean of 0 .10 (SD = 0.24). Other measures of concurrence included (1) specificity of the GCB H bA lc of 98.3 and the predictive power of a negative GCB H bA lc test (< 6.5%) of 99.1; and (2) sensitivity of the GCB H bA lc of 94.3 and the predictive power of a positive H bA lc test (>6.5%) of 89.3.
P o te n tia l B e n e fic ia r ie s o f H em oglob in
A l e T e s tin g a t D e n ta l V is its
Although all adults with diabetes can potentially benefit from additional opportunities for glycemic control monitoring, these opportunities are especially advantageous for those with elevated HbA 1 c levels. As shown in Table 3, 92.5% of group 1 participants had GCB H bA lc readings of 5.7% of greater. Hemoglobin A le monitoring at the dental visit may be particularly helpful for the 71.6% of persons in group 1 who visited dental providers on a yearly or more frequent basis, especially because almost all of these individuals (93.8%) had elevated GCB H bA lc readings. Such opportunities may also be of great benefit to the 12.3% of persons in group 1 who did not visit (or did not have) a PCP in the previous year. All of these individuals had elevated GCB H bA lc values. W hether they saw a PCP in the previous year, 9.4% of group 1 participants noted that their glucose test was conducted more than 1 year ago and all had elevated GCB H bA lc values. As shown in Table 3, results for persons in group 1 with elevated FSB H bA lc readings were very similar.
All at-risk persons who were never told they had diabetes can potentially benefit from additional opportunities for diabetes screening, but these opportunities may be more advantageous for one group of at-risk persons compared with another. As shown in Table 3, participants in group 2 (at risk because they were > 45 years) might especially reap great benefit from diabetes screening at dental visits. They were significantly more likely than those
TABLE 2 -C o n c u rre n c e of Elevated and Diabetes-Range Hemoglobin A le Values From Finger S tick and Gingival Crevicular Blood Testing of
a Sam ple of Dental C linic Patients: New York City, 2 0 1 3 -2 0 1 4
O ut-o f-R angeValues
O ut-o f-R ange Values Based on
Finger Stick
B lood, %
Out-o f-R ange Values Based on
Oral B lood, %Percent
A greem ent K Specific ity
Predictive Power
o f N egative Oral Test
Predictive Power
of Positive Oral Test Sensitivity
P red iabe tes or
d ia be tes range
(H b A lc > 5 .7 % )
5 3 .2 5 1 .5 9 2 .9 0 .8 5 8 9 4 .2 9 0 .9 9 4 .8 9 1 .7
D ia be tes range
(H b A lc > 6 .5 % )
1 3 .0 1 3 .7 9 7 .8 0 .9 0 5 9 8 .3 9 9 .1 8 9 .3 9 4 .3
N ote . H b A lc = hem oglobin A le .
April 2015, Vol 105, No. 4 | American Journal o f Public Health Strauss e t at. | Peer Reviewed | Research and Practice | 799

RESEARCH AND PRACTICE
TABLE 3 —At-Risk Adults Who Could Especially Benefit From Glycemic Control Monitoring and Diabetes Screening at Dental Visits:
New York City, 2 0 1 3 -2 0 1 4
Variab lesGroup 1: Told Had
D ia be tes (n = 6 7 ) , %
Group 2: N o t Told Had
D ia be tes and Aged > 4 5
Years (n = 2 4 5 ) , %
Group 3: O ther3
(n = 9 6 ) , %
P C om paring Group
2 and Group 3
GCB H b A lc > 5 .7 % 9 2 .5 5 1 .4 2 2 .9 < .0 0 1
FSB H b A lc > 5 .7 % 8 9 .6 5 4 .7 2 4 .0 < .0 0 1
Have regular visits w ith den ta l 7 1 .6 6 1 .7 5 4 .2 .2 0 6
provider
GCB H b A lc > 5 .7 % 9 3 .8 5 0 .7 1 7 .3 < .0 0 1
FSB H b A lc > 5 .7 % 9 1 .7 5 2 .0 1 7 .3 < .0 0 1
Did not see prim ary care provider in 1 2 .3 2 0 .2 3 3 .3 .0 1 2
pas t y
GCB H b A lc > 5 .7 % 1 0 0 .0 5 1 .1 2 5 .8 .0 2 6
FSB H b A lc > 5 .7 % 8 7 .5 5 5 .3 2 9 .0 .0 2 2
N ever tes ted or tes ted > 1 y ago for 9 .4 4 2 .2 7 0 .1 < .0 0 1
blood glucose
GCB H b A lc > 5 .7 % 1 0 0 .0 5 1 .6 1 6 .4 < .0 0 1
FSB H b A lc > 5 .7 % 1 0 0 .0 5 3 .7 1 8 .0 < .0 0 1
N o te . BMI = body m ass index (de fined as weight in kilogram s d iv ided by th e s qu are o f heigh t in m eters); FSB - finger-stick b lood; GCB - gingival crev icu la r b lood; H b A lc * hem oglobin A le . “N ot to ld he o r she had d iabe tes , aged 1 8 - 4 4 y, BMI > 2 5 k g /m 2 , and had > 1 o f the fo llow ing ad d itio n a l d ia be tes risk factors: litt le or no exercise on a given day; firs t-degree re lative (pa re n t, sib ling) w ith d iabe tes ; Latino ethnicity; Black, N ative A m erican , o r Pacific Is lan d er race; w om an who gave birth to a baby > 9 pounds.
in group 3 (at risk because they were aged 18- 44 years, had a BMI >25 kg/m2, and had > 1 additional diabetes risk factor) to have elevated GCB HbAlc readings (51.4% vs 22.9%; P<.001). This may especially be the case because, in addition to older age being a major risk factor for diabetes,2 the majority of persons in group 2 also had a BMI of 25 kg/m2 or greater and had at least 1 additional diabetes risk factor possessed by persons in group 3. Significantly higher GCB HbAlc readings for subgroups of persons in group 2 compared with group 3 were also the case for those who had regular visits with a dental provider (50.7% vs 17.3%; P< .001), those who did not see a PCP in the previous year (51.1% vs 25.8%; P=.026), and those who were never tested or were tested more than 1 year ago for blood glucose (51.6% vs 16.4%; P< .001). As shown in Table 3, results for persons in groups 2 and 3 with elevated FSB HbAlc readings were very similar.
DISCUSSION
Approximately 46% of all US adults have prediabetes or diabetes.'5 Whether measured
by using GCB or FSB, about half of our at-risk sample of adults appearing for dental care (51.5% vs 53.2%, respectively) had HbAlc values in prediabetes or diabetes ranges. In addition, 12.3% of all US adults have diabetes3; of our study sample, 13.7% had GCB HbAlc readings in the diabetes range and 13.0%had FSB HbAlc readings in this range. We acknowledge that there were some differences in classification according to prediabetes and diabetes-range HbAlc results with use of FSB and GCB. However, percent agreement, k, sensitivity, specificity, and the predictive powers of both positive and negative tests of GCB HbAlc relative to FSB HbAlc were extremely high for both elevated HbAlc and HbAlc levels in the diabetes range. Lack of concurrence between FSB HbAlc and GCB HbAlc regarding elevated and diabetes-range HbAlc values was the case for only 29 and 9 of 408 individuals, respectively. This supports the value of diabetes screening and glycemic control monitoring with the approach we employed.
Among persons who had been told that they had diabetes, three quarters had regular visits with dental providers at which time their
HbAlc could have been measured. Although only a small proportion of those with a previous diabetes diagnosis did not see a PCP or have a blood glucose test in the previous year, all of these individuals had elevated readings on the GCB HbAlc test, and all but 1 of these individuals had an elevated FSB HbAlc reading. Therefore, patients may benefit from additional glycemic control monitoring in the dental settings that they already use. For those who have a PCP but had not visited that provider in the previous year, the dental provider might encourage such a visit. For those without a regular PCP, the dental provider might emphasize the importance of identifying a PCP and make a referral, when appropriate.
Our findings indicate that at-risk adults aged at least 45 years who had never been told that they had diabetes could especially benefit from HbAlc testing at dental visits. Close to two thirds saw a dental provider on a regular basis, and about half of these persons had elevated HbAlc. Similarly, 1 in 5 did not see a PCP in the previous year, and about half of these individuals had HbAlc levels in the prediabetes or diabetes ranges. In addition, 2 in 5 did not have a blood glucose test in the past 12
800 | Research and Practice | Peer Reviewed | Strauss et at. American Journal o f Public Health ] April 2015, Vol 105, No. 4

RESEARCH AND PRACTICE
months, and about half had elevated HbAlc readings. Many persons aged at least 45 years with elevated HbAlc levels have never been told that they have prediabetes or diabetes, and may remain unaware of their diabetes risk. Therefore, screening for prediabetes and diabetes at alternate sites, such as at the dental visits that patients already attend, offers a key window of opportunity for health assessment and monitoring.
Several limitations to the study are acknowledged. The sample was nonrandom, composed of persons who were at risk for diabetes and its complications, self-selected to participate in the study, and whose gums bled on probing. Although bleeding on probing is widespread among all American adults (approximately half of US adults have periodontal disease and an additional proportion has gingivitis,14 most of whom bleed on probing), and bleeding on probing is especially common among persons with prediabetes and diabetes,1516 some patients do not bleed on gentle dental probing. For such patients, HbAlc testing could still be performed at dental visits by using blood collected from the finger.12 In addition, although HbAlc values were obtained through laboratory testing, another study limitation involves the use of other data in the analyses that were provided through participant self-report, some of which may have been subject to social desirability or inaccurate recall.
Despite these limitations, our study has considerable public health significance because we identify the value and importance of capitalizing on an opportunity at the dental visit (1) to screen at-risk, but as yet undiagnosed, patients for diabetes (especially those aged > 45 years) and (2) to monitor glycemic control in those already diagnosed so as to enable them to maintain their health to the greatest extent possible. ■
About the AuthorsAt the time of this study, Shield M. Strauss, Mary T. Rosedale, and Navjot Kaur were with the College of Nursing, New York University, New York, NY. Michael A. Pesce was with the Columbia University Medical Center, New York. David M. Rindskopf was with the Graduate School and University Center of the City of New York. Caroline M. futerbock, Dolores Malaspina, andAnnDanoff were with the NYU Langone Medical Center, New York University. Mark S. Wolff was with the College of Dentistry, New York University.
Correspondence should be sent to Shield M. Strauss, PhD, Associate Professor, New York University College of Nursing, 433 First Avenue, 6th Floor, New York, N Y 10010 (e-mail: [email protected]). Reprints can be ordered at http://www.ajph.org by clicking the “Reprints” link.
This article was accepted September 22, 2014.
ContributorsS. M. Strauss and M. T. Rosedale conceptualized the study and S. M. Strauss led the analyses with the support of D. M. Rindskopf. S. M. Strauss led the writing, with contributions from M. T. Rosedale, M. A. Pesce,D. M. Rindskopf, N. Kaur, C. M. Juterbock, M. S. Wolff, D. Malaspina, and A. Danoff. All authors contributed to the editing of the artide and collaborated on the interpretation of study results and their implications.
AcknowledgmentsFunding for this study was provided by the National Institute of Dental and Craniofacial Research (grant 1R15DE023201). Portions of the salaries of S. M. Strauss., M. T. Rosedale, N. Kaur, C. M. Juterbock, M. S. Wolff, and D. Malaspina were covered by this grant.
We wish to thank the many nursing students, dentists, dental hygienists, and dental and dental hygiene students who assisted with subject recruitment, blood sample collection, and survey collection support. We also thank the study participants, whose willingness to respond to our questions and allow the collection of finger stick and oral blood samples enabled us to perform the research.
Human Participant ProtectionThe study was approved by the institutional review board at the New York University School of Medicine.
References1. Diabetes report card 2012. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2012. Available at: http:// www.cdc.gov/diabetes/pubs/pdf/diabetesreportcard. pdf. Accessed September 15, 2014.
2. American Diabetes Association. Standards of medical care in diabetes-2014. Diabetes Care. 2014;37 (suppl 1):S14-S80.
3. American Diabetes Association. Fast facts. Data and statistics about diabetes. Available at: http://professional. diabetes.org/admin/UserFiles/0%20-°/o20Sean/ 14_fast_facts_june2014_final3.pdf. Accessed September 15,2014.
4. Krishna S, Gillespie KN, McBride TM. Diabetes burden and access to preventive care in the rural United States./Rural Health. 2010;26(1):3-11.
5. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl f Med. 2002;346(6):393-403.
6. Gillies CL, Abrams KR, Lambert PC, et al. Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: systematic review and meta-analysis. BMf. 2007;334(7588):299.
7. Strauss SM, Alfano MC, Shelley D, Fulmer T. Identifying unaddressed systemic health conditions at dental visits: patients who visited dental practices but not general health care providers in 2008. Am f Public Health 2012;102(2):253-255.
8. Lalla E, Kunzel C, Burkett S, Cheng B, Lamster IB. Identification of unrecognized diabetes and pre-diabetes in a dental setting. ] Dent Res. 2011;90(7):855-860.
9. Barasch A, Gilbert GH, Spurlock N, et al. Random plasma glucose values measured in community dental practices: findings from the Dental Practice-Based Research Network. Clin Oral Investig. 2013;17(5):1383- 1388.
10. Engstrom S, Berne C, Gahnberg L, Svardsudd K. Effectiveness of screening for diabetes mellitus in dental health care. Diabet Med. 2013;30(2):239-245.
11. Strauss SM, Tuthill J, Singh G, et al. A novel intra-oral diabetes screening approach in periodontal patients: results of a pilot study. JPeriodontol. 2012; 83(6):699-706.
12. Rosedale MT, Strauss SM. Diabetes screening at the periodontal visit: patient and provider experiences with two screening approaches. IntJ Dent Hyg. 2012; 10 (4):250-258.
13. Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960:20:37-46.
14. Eke PI, Dye BA, Wei L, et al. Prevalence of periodontitis in adults in the United States: 2009 and 2010 J Dent Res. 2012;91(10):914-920.
15. Javed F, Al-Askar M, Al-Rasheed A, Babay N, Al- Hezaimi K. Comparison of self-perceived oral health, periodontal inflammatory conditions and socioeconomic status in individuals with and without prediabetes. Am J MedSci. 2012;344(2):100-104.
16. Campus G, Salem A, Uzzau S, Baldoni E, Tonolo G. Diabetes and periodontal disease: a case-control study. J Periodontol. 2005;76(3):418-425.
April 2015, Vol 105, No. 4 | American Journal o f Public Health Strauss et al. Peer Reviewed | Research and Practice | 801
Copyright of American Journal of Public Health is the property of American Public HealthAssociation and its content may not be copied or emailed to multiple sites or posted to alistserv without the copyright holder's express written permission. However, users may print,download, or email articles for individual use.