double trouble: concurrent atrial fibrillation and
TRANSCRIPT
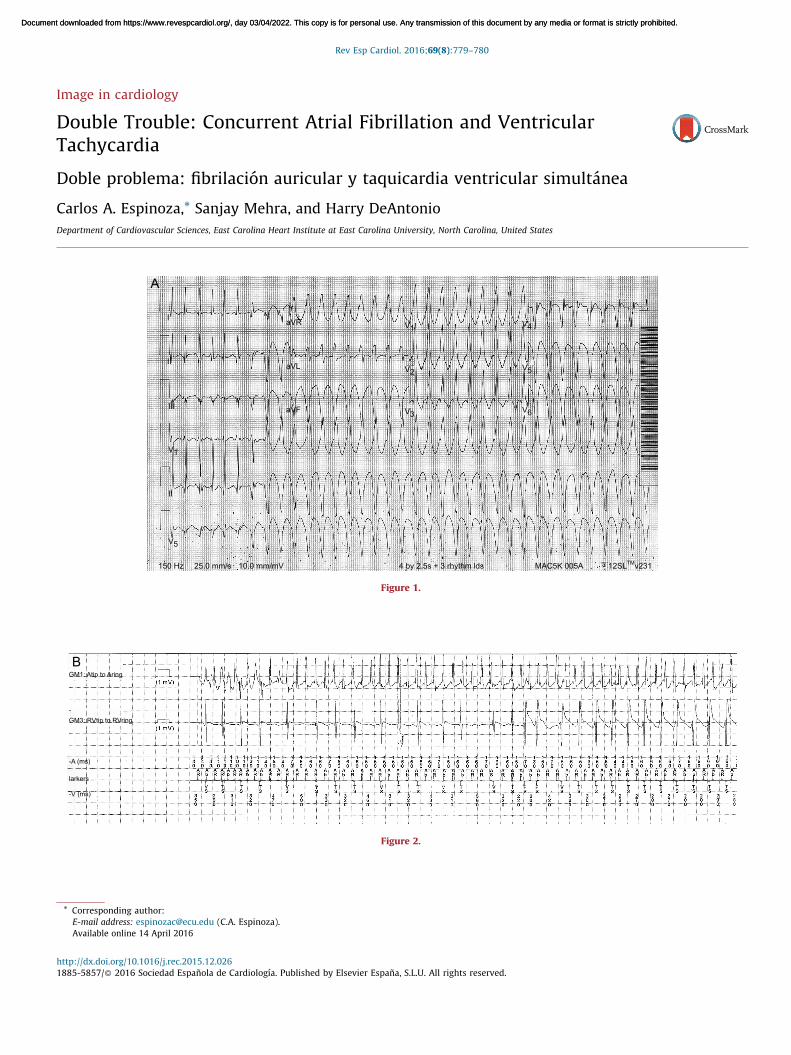
Image in cardiology
Double Trouble: Concurrent Atrial Fibrillation and VentricularTachycardia
Doble problema: fibrilacion auricular y taquicardia ventricular simultanea
Carlos A. Espinoza,* Sanjay Mehra, and Harry DeAntonio
Department of Cardiovascular Sciences, East Carolina Heart Institute at East Carolina University, North Carolina, United States
Rev Esp Cardiol. 2016;69(8):779–780
A
aVRI
II
III
V1
V5
II
150 Hz 25.0 mm/s 10.0 mm/mV 4 by 2.5s + 3 rhythm lds MAC5K 005A 12SLTM v231
aVL
aVF
V1
V2
V3
V4
V5
V6
Figure 1.
BGM1: Atip to Aring
GM3: RVtip to RVring
-A (ms)
-V (ms)
larkers
Figure 2.
* Corresponding author:
E-mail address: [email protected] (C.A. Espinoza).
Available online 14 April 2016
http://dx.doi.org/10.1016/j.rec.2015.12.026
1885-5857/� 2016 Sociedad Espanola de Cardiologıa. Published by Elsevier Espana, S.L.U. All rights reserved.
Document downloaded from https://www.revespcardiol.org/, day 03/04/2022. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from https://www.revespcardiol.org/, day 03/04/2022. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
A 50-year-old woman with a history of chronic nonischemic systolic heart failure status after implantable cardioverter defibrillator
(ICD) placement presented to the emergency department with a history of palpitations and multiple ICD shocks. Her 12-lead
electrocardiogram demonstrated narrow complex, irregular tachycardia followed by wide complex tachycardia (Figure 1). The presence of
a fusion beat and atrioventricular dissociation suggested ventricular tachycardia (VT). A 150 mg bolus of amiodarone intravenously
restored sinus rhythm. Electrolyte and thyroid function tests were within the normal reference range. Echocardiogram showed
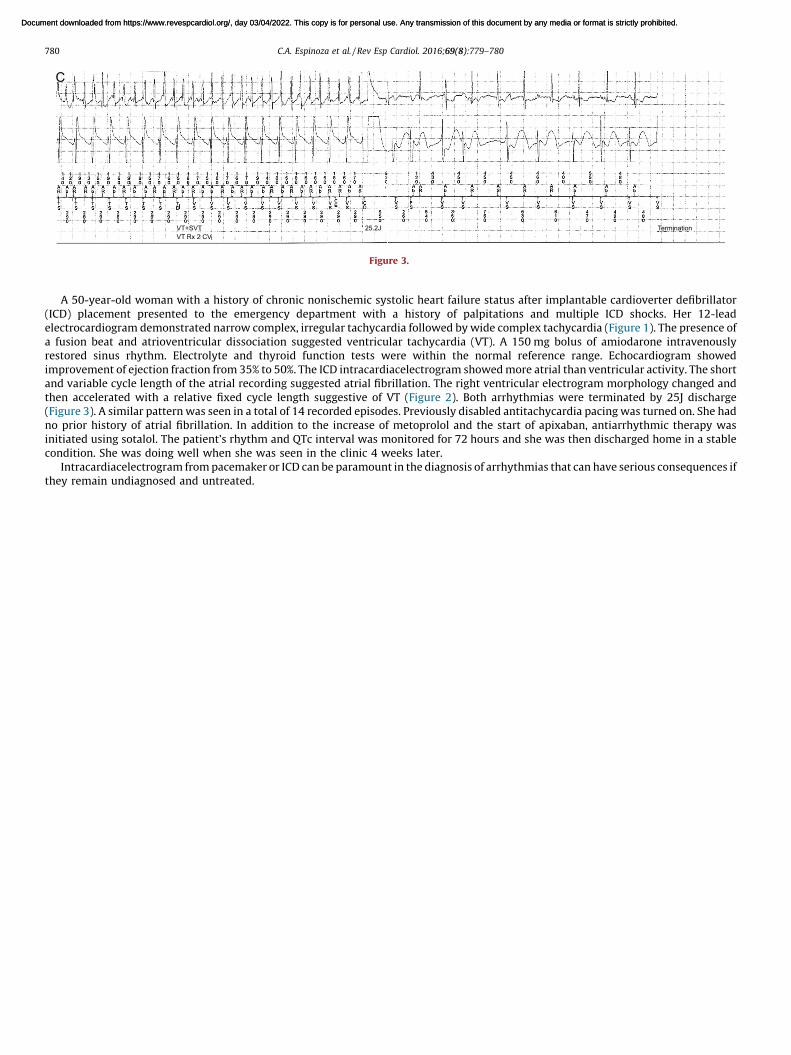
improvement of ejection fraction from 35% to 50%. The ICD intracardiacelectrogram showed more atrial than ventricular activity. The short
and variable cycle length of the atrial recording suggested atrial fibrillation. The right ventricular electrogram morphology changed and
then accelerated with a relative fixed cycle length suggestive of VT (Figure 2). Both arrhythmias were terminated by 25J discharge
(Figure 3). A similar pattern was seen in a total of 14 recorded episodes. Previously disabled antitachycardia pacing was turned on. She had
no prior history of atrial fibrillation. In addition to the increase of metoprolol and the start of apixaban, antiarrhythmic therapy was
initiated using sotalol. The patient’s rhythm and QTc interval was monitored for 72 hours and she was then discharged home in a stable
condition. She was doing well when she was seen in the clinic 4 weeks later.
Intracardiacelectrogram from pacemaker or ICD can be paramount in the diagnosis of arrhythmias that can have serious consequences if
they remain undiagnosed and untreated.
C
VT+SVT
VT Rx 2 CV
25.2J Termination
Figure 3.
C.A. Espinoza et al. / Rev Esp Cardiol. 2016;69(8):779–780780
Document downloaded from https://www.revespcardiol.org/, day 03/04/2022. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.Document downloaded from https://www.revespcardiol.org/, day 03/04/2022. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.