
1
Behavioral Consultation in Your Child's School :
Improving Outcomes
Jane Barbin, Ph.D., [email protected]

2
What is Behavioral Consultation?
• Professional guidance to and for individuals with autism spectrum disorders and the educational, vocational, residential, and family systems supporting those individuals
• Focus is on using technology based in principles of learning
3
Research-based Intervention
• Intervention focus is Applied Behavior Analysis (ABA)
• Extensive research supports effectiveness of ABA for individuals with ASD
• Behavioral contingencies which lead to successful consultation can be analyzed

4
Consultation: To Whom?
• Parents• Extended family members• Caregivers• Instructional personnel• Related service providers• Administrators• Governing boards

5
Consultation: About what?
• Instructional strategies• Skill acquisition• Challenging behavior• Motivational systems• Curricula• Organizational systems

6
Flawless Consulting
(Block, 2000)
Consultant
“A person in a position to have some influence over an individual, a group, or an organization, but who has no direct power to make changes or implement programs.”
Manager
“Someone who has direct responsibility over the action.”

7
Shared Assumptions ~though not sufficient~
• Uses procedures with scientific backing
• Consultant has adequate training and experience: BCBA / Autism SIG Consumer Guidelines
(listed by parents as factor much associated with success)
• Sufficient economic resources (cost, materials, time)
• Individual factors considered (cognitive state, dual diagnosis)

8
Further…• Behavioral consultants should be obligated to:
• Describe their credentials and experience
• Explain the intervention method in detail
• Take concurrent variables into consideration
• Describe the process for objective treatment evaluation (e.g., effectiveness). How will success be measured? Will data be collected?
9
Survey Questionnaire “Factors Related to Successful
Consultation”Collected 2005-06Respondents: 49 Consumers (Parents/ School Staff)
73 Providers
9 items using 5 point Likert scale rating
Examples: Research-based treatment, training, costs, ease of implementation, generalization, data collection
Descriptive Data: • 3 factors associated with success • 3 barriers to success • Open –ended section
10
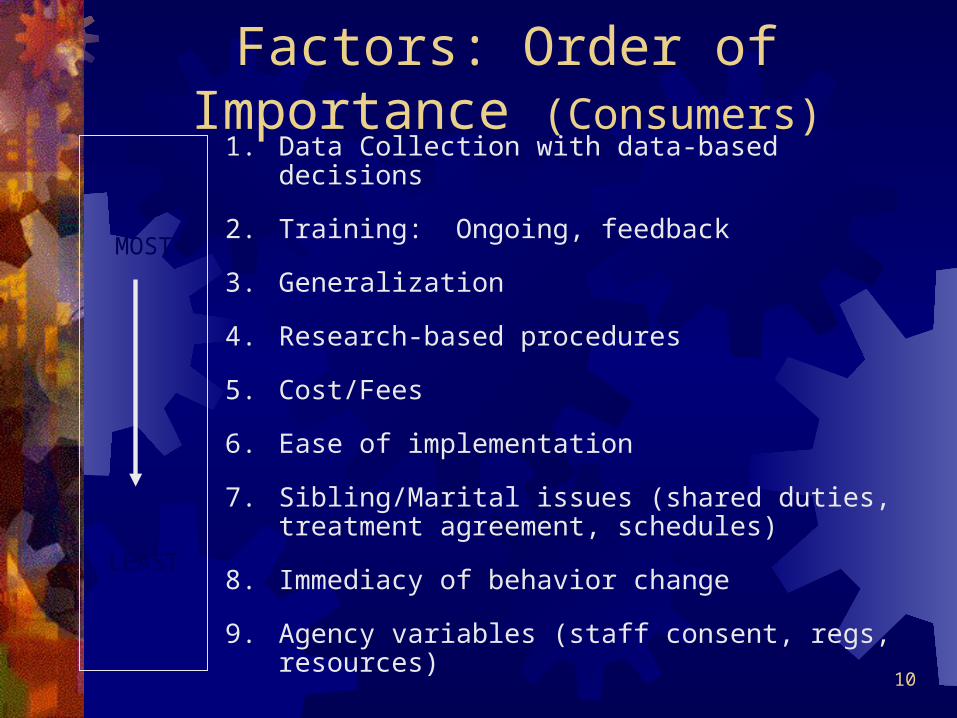
1. Data Collection with data-based decisions
2. Training: Ongoing, feedback
3. Generalization
4. Research-based procedures
5. Cost/Fees
6. Ease of implementation
7. Sibling/Marital issues (shared duties, treatment agreement, schedules)
8. Immediacy of behavior change
9. Agency variables (staff consent, regs, resources)
MOST
LEAST
Factors: Order of Importance (Consumers)

11
Top 3 Factors Related to Success
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Ave
rag
e R
atin
g
Data-BasedDecisions
Ongoing Training Generalization
Providers
Consumers

12
Factor #1-Data Collected/ Data-Based Decisions
• Basic assumption of behavioral intervention• Both providers and consumers ranked this as
the #1 factor related to success
~The scientific study (of behavior) requires precise measurement”
(Baer, Wolf, & Risley,1968)

13
Data Collection & Data-Based Decision Making
Consumers: • data collection can be overwhelming• consultants stuck on taking data
Providers:• would like data to play a more significant role• shaping procedure, (do it, then team sees value)

14
Data collectionData collection for behavior reduction & skill acquisition!
Include use of data collection in IEP to measure progress
Operationalize all IEP goals and targeted behaviors
Get all parties involved (SLP, OT, Teacher, 1:1)
Interobserver reliability –ideal!
Adds integrity, accuracy and ACCOUNTABILITY
15
DATA SAMPLE SHEET (Skill Acquisition)Instructor: ___________________________________ Date: ______________________
IEP Goal/ Program Name: ________________________________
(Yes= independent No= prompted or incorrect) TRIALS
Targets 1 2 3 4 5 6 7 8 9 10
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
Y N
16
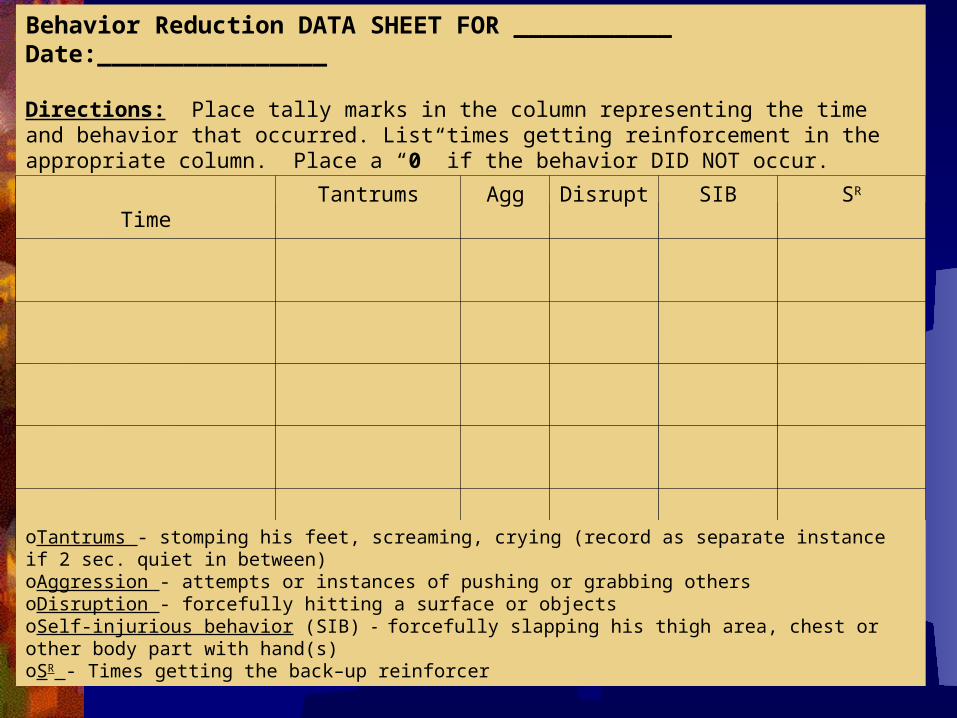
Behavior Reduction DATA SHEET FOR ___________ Date:________________
Directions: Place tally marks in the column representing the time and behavior that occurred. List times getting reinforcement in the appropriate column. Place a “0” if the behavior DID NOT occur.
TimeTantrums Agg Disrupt SIB SR
oTantrums - stomping his feet, screaming, crying (record as separate instance if 2 sec. quiet in between)oAggression - attempts or instances of pushing or grabbing othersoDisruption - forcefully hitting a surface or objectsoSelf-injurious behavior (SIB) - forcefully slapping his thigh area, chest or other body part with hand(s)oSR - Times getting the back–up reinforcer
17
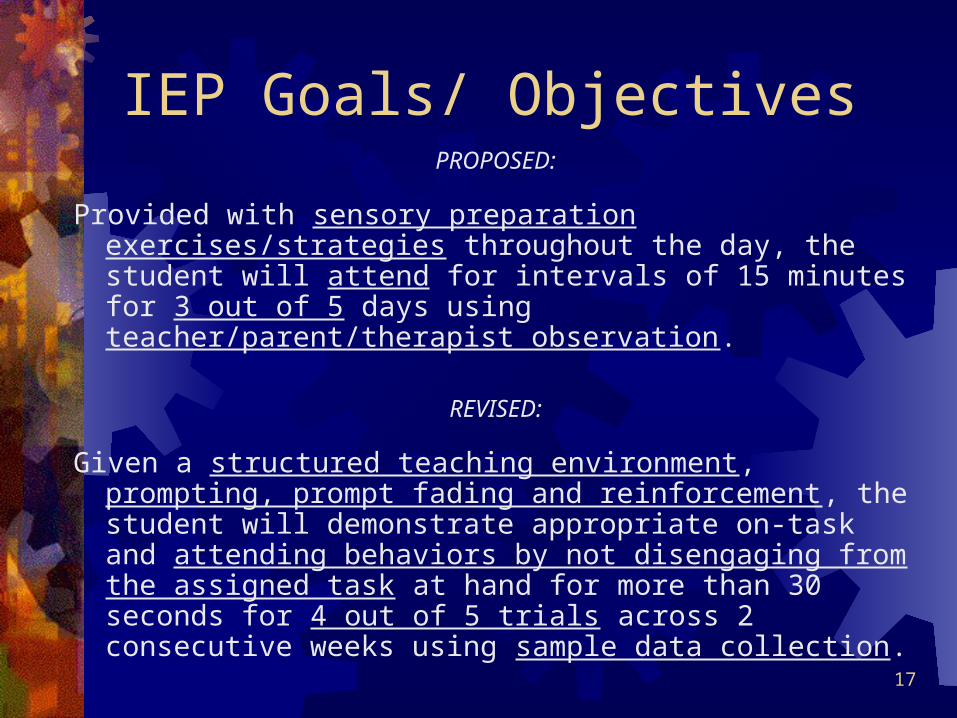
IEP Goals/ ObjectivesPROPOSED:
Provided with sensory preparation exercises/strategies throughout the day, the student will attend for intervals of 15 minutes for 3 out of 5 days using teacher/parent/therapist observation.
REVISED:
Given a structured teaching environment, prompting, prompt fading and reinforcement, the student will demonstrate appropriate on-task and attending behaviors by not disengaging from the assigned task at hand for more than 30 seconds for 4 out of 5 trials across 2 consecutive weeks using sample data collection.
18
Factor #2-Training
Consumers: • school staff do not train parents
Providers:• need for step by step instruction guide

19
Training• “…ongoing, hands on training (modeling, supervised practice, and
immediate verbal feedback) is needed.” (McClannahan & Krantz,1993)
• Didactic procedures alone are insufficient (McClannahan & Krantz, 1993)
• …week long parent training series, …parents can effectively implement strategies and teach others(Symon, 2005)
• “Parents and teachers require training in direct application for individual child otherwise it becomes a bad game of telephone.” (parent)

20
Training
“…the success of an intervention is dependent upon not only its effectiveness but also upon its precise delivery by a clinician and the consistency with which parents implement that treatment with all its essential features.”
Allen & Warzak (2000)

21
Training• Best for consultant to identify training needs first, then
offer support but school must be willing
• Take collaborative role – trying to understand school/class/teacher variables, adapt program as needed
• Set small goals and follow-up closely (email, repeat visits, agenda, offer help)
• Recognize school efforts and strengths in that environment to build team work
• Follow through and consistency are key!

22
Factor #3-Generalization
Stokes and Baer (1977)
… the occurrence of relevant learned behavior under different non-operant conditions.
Vary noncritical dimensions of antecedents and accept a wide range of responses.

23
Generalization
Consumers: • “My son has learned to generalize his language skills.”
Providers:• planning for generalization (e.g., fading Sr, training
caregivers); • no generalization from school to home as a problem
24
Generalization
Does the intervention result in a better quality of lives for the families? (Provider Response)
• Plan to intervene and program in natural setting from the start; settings other than school can be implemented by all providers

25
Only Research-based Interventions
• NYSDOH Early Intervention Program (1999)…recommends ABA as primary treatment approach
• Heflin and Simpson (1998)…one of most efficacious and controversial interventions (controversy relates to exclusion of other methods, intensity required, etc.)
• ABA is also controversial locally and expensive. Access to quality services is often parent-driven and a grassroots effort.

26
Scientific vs. Nonscientific Approach
• ABA is a science. Science relies on direct and objective evaluation
• Uses operational definitions
• Compares effects to pre-treatment (baseline) occurrence of behaviors using systematic measurement
• Considers alternative explanations / confounds
• Replicates results (e.g., reports are from different people) and presents the results in peer reviewed journals
27
Only Research-based Interventions
• ABA Standards – SIG Guidelines
• Association for Science in Autism Treatment (ASAT) and Organization for Autism Research (OAR)
• Both parties indicated “highly important,” yet consumers describe ABA providers as “rigid/inflexible”
• Providers spoke of, “Lack of buy-in,” resistance to ABA, competing programs
• Consumer protection is compromised

28
Only Research-based Interventions
• Realistic expectations
• Commitment to systematic intervention
• Identification / agreement of functional goals

29
Only Research-based Interventions
• Consumers:• Need to implement “all” behavioral applications,
need for language goals, be “open-minded”
• Providers:• Success: Shared philosophy-”Buy-in”• Barrier: Disagreement on philosophy

30
Only Research-based : ABA Practice
• General need for clarity in field to increase buy-inWhat ABA/ behavioral consultant is, what exactly they do?
• Behavior Analyst Certification Board Guidelines for Responsible Conduct For Behavior Analysts© (2004)
“When behavior analysts provide assessment, evaluation, treatment, counseling, supervision, teaching, consultation, research, or other behavior analytic services to an individual, a group, or an organization, they use language that is fully understandable to the recipient of those services. They provide appropriate information prior to service delivery about the nature of such services and appropriate information later about results and conclusions.”

31
Only Research-based : ABA Practice
• We use the same words to mean many different things
• Once-size-fits-all terminology (Ex: “intensive,” “data-based”)
• Behavioral “sects” – VB, PBS, EIBI, Lovaas• Articulate specific treatment philosophy
and parameters • Assessment protocol – defining treatment
in relation to individual needs and environments

32
Only Research-based : ABA Practice
• Social significance of goals, social appropriateness of procedures, and social importance of effects.
(Baer, D.M., Wolf, M.M., Risley T.R., 1968)
• Ultimate goal: Life in the least restrictive environment with the least amount of support.
(Bannerman, Sheldon, Sherman, & Harchik, 1990)

33
What are my child’s learning needs?• Seek assistance from a qualified professional (e.g., Board
Certified Behavior Analyst, Licensed Psychologist, Speech Pathologist).
• Conduct indirect (e.g., parent/school staff interview) and direct
(e.g., school observation) assessments
• Operationally define strengths and weaknesses of current educational placement and alternatives
• Is the class size/teaching method appropriate?• Is the student engaging in problem behaviors?• Staff training and experience
34
Learning Needs –cont.• It is often helpful to obtain a written report with recommendations
based on assessment results
• Share recommendations with the school team; seek advocacy and support when convening IEP team; integrate recommendations into IEP
• Provide ongoing support to the school team to facilitate implementation of recommendations
• Training in how to address challenging behaviors.• Providing a review of I.E.P. goals/short-term objectives with needed
modifications and additions

35
Following Assessment• Is a change in school placement necessary?
It is an IEP team question.
• Possible Benefits of Placement Change• A program that more closely meets the student’s learning needs• Improved student academic progress• Access to more appropriate and effective teaching methodology• Reduced challenging behaviors
• Potential Disadvantages• Tuition for alternative placement• Travel• Removal from established peer group
• Determine if the current school placement is able, willing and can agree (“consents”) to implement proposed recommendations.
36
Agency Variables • Staff roles/ assent, limited resources & state regs
• Responsibility and authority of consultant
• Leader? Colleague? Team member? Separate roles of consultant and manager
• Does s/he make suggestions or give directions?• Does s/he have agreement amongst key participants?
• Models of consultation: individual, classroom-wide, school-wide, district-wide
(Putnam, Handler, Rey & McCarty, 2005)

37
Collaboration and Communication
Consumer
+ Open Honest
Ongoing Written
- Untimely Vague
Provider
+ Feedback system Accessibility
Schedule
- Poor communication
Consumer 51% Provider 41% state lack of collaboration / communication leads to problems
Weiss (1991)… arranging /collaborating with professionals is #1 stressor
38
Clarifying Expectations
• Do not assume expectations are self-evident, understood, or shared
• “…get all of the expectations out on the table…”
• “…real investment of time and effort up front…” Covey (1989)

39
“The road to success is always under construction.”
(unknown)
• Data-based decisions, ongoing training, and planning for generalization are key to your child’s progress.
• Contracting can assist both parties and facilitate communication. Keep written, organized records
• Maintain open communication whenever possible

40
Organizations / Resources• Autism Special Interest Group of ABA. www.autismsig.org; See the “Autism SIG
Consumer Guidelines for Identifying, Selecting and Evaluating Behavior Analysts Working with Individuals with ASD.”
• The Association for Behavior Analysis (ABA) – www.abainternational.org; phone: (269) 492-9310. This organization hosts an annual conference and parent attendance is encouraged.
• The Association for Science in Autism Treatment (ASAT) – www.asatonline.org; phone: 207-253-6008. This organization’s mission is to disseminate only scientifically sound assessment and treatment information.
• Behavior Analyst Certification Board (BACB) – www.bacb.com; This organization promotes a national and international certification process for behavior analytic practitioners. A database of certified practitioners is maintained on the site.
• Behavioral Directions, LLC – www.behavioraldirections.com; See “Resource” page for links to other organizations, references, recommended reading, etc.
• Organization for Autism Research (OAR) – www.researchautism.org; Hosts a research-based conference annually in Northern Virginia.







