Consultation draft not for publication
HBN 10-01 January 2020 1
1
Health Building Note 10-01 2
Facilities for surgery 3
4
Version 1.1 5
February 2020 6
7
8
Consultation draft not for publication
HBN 10-01 January 2020 2
9
Version
history/revisions
Version
Date Author Changes
Version 1.0 24/02/20 Archus project team Consultation draft for technical engagement – wider reference group.
Version 1.1 25/02/20 Archus project team Updated in response to NHS England and Improvement comments
(deletions and clarifications / policy-related) prior to release for
technical engagement.
10
11
Consultation draft not for publication
HBN 10-01 January 2020 3
Introduction to the Technical Standards 12
The Technical Standards provide best practice guidance for all those involved in 13
strategic planning and design of new healthcare buildings and on the adaptation or 14 extension of existing facilities; also on the design, installation and operation of 15 specialised building and engineering technologies used in the delivery of health care. 16 They provide tools to assist with the calculations required to produce schedules of 17 accommodation, exemplar data sheets and case studies of recent schemes. 18
Developed by multi-disciplinary teams, they reflect latest best practice and current 19 policy. They are peer-reviewed and assessed for equality impact prior to dissemination 20
via www.gov.uk2. 21
What is best practice guidance? 22
The Technical Standards provide best practice guidance inasmuch as they describe 23 methods, techniques and exemplar technical solutions that are generally accepted as 24 superior to any alternatives – because: 25
they produce results that are superior to those achieved by other means; 26
they have become standard ways of successfully doing things (e.g., a 27
standard way of complying with legal or ethical requirements). 28
The Technical Standards are published in two formats: 29
Health Building Notes (HBNs) 30
HBNs provide technical information in the form of best practice guidance to support 31
the briefing and design processes for individual projects in the NHS building 32 programme. They are based on the patient’s experience across the spectrum of care 33
from home to healthcare setting and back. 34
Most of the content will be familiar to healthcare planners, architects and others with 35 formal design education. However, it will also be useful for the informed client, 36 commissioners and regulators – those who do not have detailed knowledge of capital 37
investment projects but who want more involvement and information on the issues that 38 are encountered in these types of project. 39
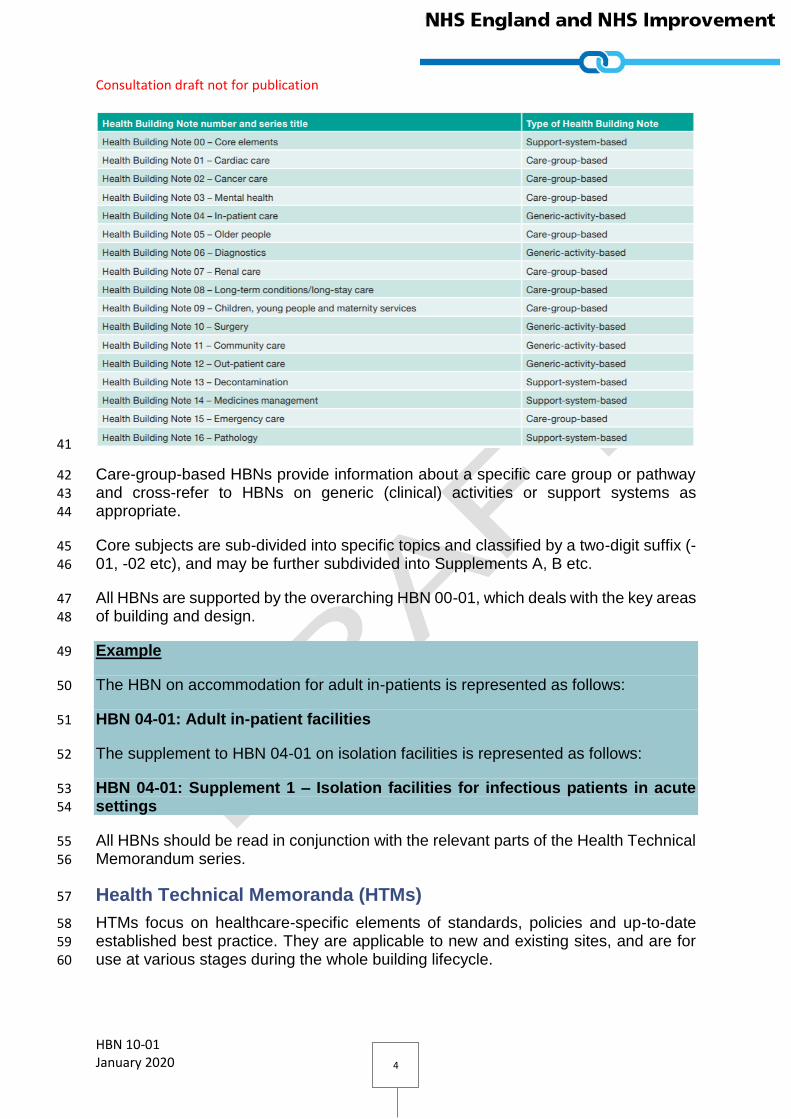
HBNs are published as a suite of 17 core subjects: 40
1 See https://www.gov.uk/government/collections/health-building-notes-core-elements and https://www.gov.uk/government/collections/health-technical-memorandum-disinfection-and-sterilization and https://www.gov.uk/government/publications/complete-list-of-nhs-estates-related-guidance 2 See https://www.gov.uk/government/collections/health-building-notes-core-elements and https://www.gov.uk/government/collections/health-technical-memorandum-disinfection-and-sterilization and https://www.gov.uk/government/publications/complete-list-of-nhs-estates-related-guidance
Consultation draft not for publication
HBN 10-01 January 2020 4
41
Care-group-based HBNs provide information about a specific care group or pathway 42
and cross-refer to HBNs on generic (clinical) activities or support systems as 43 appropriate. 44
Core subjects are sub-divided into specific topics and classified by a two-digit suffix (-45 01, -02 etc), and may be further subdivided into Supplements A, B etc. 46
All HBNs are supported by the overarching HBN 00-01, which deals with the key areas 47
of building and design. 48
Example 49
The HBN on accommodation for adult in-patients is represented as follows: 50
HBN 04-01: Adult in-patient facilities 51
The supplement to HBN 04-01 on isolation facilities is represented as follows: 52
HBN 04-01: Supplement 1 – Isolation facilities for infectious patients in acute 53
settings 54
All HBNs should be read in conjunction with the relevant parts of the Health Technical 55 Memorandum series. 56
Health Technical Memoranda (HTMs) 57
HTMs focus on healthcare-specific elements of standards, policies and up-to-date 58 established best practice. They are applicable to new and existing sites, and are for 59
use at various stages during the whole building lifecycle. 60

Consultation draft not for publication
HBN 10-01 January 2020 5
Healthcare providers have a duty of care to ensure that appropriate governance 61 arrangements are in place and are managed effectively: HTMs provide best practice 62 engineering standards and policy to enable management of this duty of care. 63
It is not the intention within this suite of 64 documents to unnecessarily repeat 65
international or European standards, 66 industry standards or UK Government 67 legislation. Where appropriate, these will 68 be referenced. 69
Healthcare-specific technical engineering 70 guidance is a vital tool in the safe and 71 efficient operation of healthcare facilities. 72
HTM guidance is the main source of 73
specific healthcare-related guidance for estates and facilities professionals. 74
The core suite of nine subject areas provides access to guidance which: 75
is more streamlined and 76
accessible; 77
encapsulates the latest 78
standards and best practice 79
in healthcare engineering, 80
technology and sustainability; 81
provides a structured 82
reference for healthcare 83
engineering. 84
All Health Technical Memoranda are 85 supported by the initial document HTM 86
00, which embraces the management 87 and operational policies from previous 88
documents and explores risk 89 management issues. 90
Compliance matters 91
There are numerous statutes, legal requirements and industry standards with which 92 healthcare organisations, supporting professionals, contractors and suppliers must 93 comply. Guidance on how to comply with these is given in the respective Technical 94 Standards and the NHS Premises Assurance Model (PAM).3 95
[DN: any other sources to be added here? Suggest also add see www.gov.uk/??? for 96 up-to-date information IF a home page is established in addition to those existing for 97
downloads of current HBNs and HTMs.] 98
3 See https://www.gov.uk/government/publications/nhs-premises-assurance-model-launch
Consultation draft not for publication
HBN 10-01 January 2020 6
In England, compliance with HTM 05-01 Firecode4 Managing Healthcare Fire Safety 99 is mandatory. It sets out the Department of Health and Social Care’s (DHSC’s) policy 100 on fire safety in the NHS. It includes best practice guidance on management 101 arrangements for fire safety. 102
Compliance with the Technical Standards is not statutory but it may be used as 103
evidence in legal proceedings. 104
[DN: text to be reviewed by legal advisors.] 105
Evidencing that Technical Standards have been followed – or being able to explain 106
why not – will be relevant in demonstrating compliance with the above legal 107 requirements and standards. 108
[DN: text to be reviewed by legal advisors.] 109
Assurance of healthcare infrastructure 110
The foundations for the assurance of estates and facilities are laid in a set of legal 111 requirements and standards, primarily: 112
Regulations 12 and 15 of the Health and Social Care Act 2008 (Regulated 113
Activities) 2014 on the safety and suitability of premises. 114
o Both of these regulations also form part of the Care Quality 115
Commission’s (CQC) fundamental standards. 116
o Health Building Notes (HBNs) and Health Technical Memoranda 117
(HTMs), among others, are specifically referenced in the CQC’s 118
Guidance for providers on meeting the regulations5 as a means of 119
complying with these Regulations. 120
The Health Act 2009 includes provisions that place a statutory duty on 121
healthcare organisations, providers of primary care services, and voluntary 122
organisations providing NHS care in England to have regard to the NHS 123
Constitution, which stipulates that patients have a right “to be cared for in a 124
clean, safe, secure and suitable environment”. 125
Language usage in Technical Standards 126
In HTMs and HBNs, modal verbs such as “must”, “should” and “may” are used to 127 convey notions of obligation, recommendation or permission. The choice of modal 128 verb will reflect the level of obligation needed to be compliant. 129
[DN: text to be reviewed by legal advisors.] 130
4 See https://www.gov.uk/government/publications/managing-healthcare-fire-safety 5 See https://www.cqc.org.uk/file/182052
Consultation draft not for publication
HBN 10-01 January 2020 7
The following describes the implications and use of these modal verbs in HTMs/HBNs 131 (readers should note that these meanings may differ from those of industry standards 132 and legal documents): 133
“Must” is used when indicating compliance with the law. 134
“Should” is used to indicate a recommendation (not 135
mandatory/obligatory), i.e. among several possibilities or methods, one is 136
recommended as being particularly suitable – without excluding other 137
possibilities or methods. 138
“May” is used for permission, i.e. to indicate a course of action permissible 139
within the limits of the HTM or HBN. 140
[DN: text to be reviewed by legal advisors.] 141
142
Typical usage examples: 143
“All publicly-funded organisations must ensure that all contracts 144
established to collect and treat waste conform to the Public Contracts 145
Regulations.” [obligation] 146
“All low voltage (LV) distributions should be configured as TN systems.” 147
[recommendation] 148
“Alcohol hand gels that do not contain siloxanes may be rinsed out and 149
the packaging recycled or placed into the municipal waste stream.” 150
[permission] 151
“Shall”, in the obligatory sense of the word, is never used in current 152
HTMs/HBNs. 153
Project derogations from the Technical Standards 154
Healthcare facilities built for the NHS are expected to support the provision of high-155
quality healthcare and ensure the NHS Constitution right to a clean, safe and secure 156 environment. It is therefore critical that they are designed and constructed to the 157 highest and most appropriate technical standards and guidance[1]. This applies when 158
organisations, providers or commissioners invest in healthcare accommodation 159
(irrespective of status, e.g. Foundation and non-Foundation trusts). 160
The need to demonstrate a robust process for agreeing any derogation from Technical 161 Standards and guidance is a core component of the business case assurance 162
process. 163
The starting point for all NHS healthcare projects at Project Initiation Document (PID) 164 and/or Strategic Outline Case (SOC) stage is one of full compliance. 165
[1] Statutory standards plus technical standards and guidance specific to NHS facilities : https://www.gov.uk/government/collections/health-building-notes-core-elements https://www.gov.uk/government/collections/health-technical-memorandum-disinfection-and-sterilization https://www.gov.uk/government/publications/complete-list-of-nhs-estates-related-guidance

Consultation draft not for publication
HBN 10-01 January 2020 8
A schedule of derogations will be required for any project requiring external business 166 case approval and may be requested for those that have gone through an internal 167 approvals process. 168
While it is recognised that derogation is required in some cases, this must be risk-169 assessed and documented in order that it may be considered within the appraisal and 170
approval process. 171
Derogations must be properly authorised by the project’s senior responsible owner 172 and informed and supported by appropriate technical advice (irrespective of a project’s 173 internal or external approval processes). 174
[DN: NHS England and NHS Improvement is piloting a standardised approach to the 175 derogations process: this will be referred to here, once agreed.] 176
Overview of the healthcare planning 177
process 178
At the heart of the healthcare planning process is the design of the model of care, 179 which is the overarching philosophy identifying how the health economy, and 180
organisations within it, will deliver care in the future. This should reflect the health care 181
philosophy and particular circumstances of the whole health economy / organisation, 182
national and local. 183
Models of care should assess the opportunities for future provision, with particular 184
emphasis on modernising: 185
The care process and integrated patient pathways; 186
Use of technology; 187
Use of design; 188
Workforce considerations. 189
190
Healthcare planning allows healthcare providers to reflect on current ways of working 191
and provides a framework to refine / alter / improve service delivery. Robust healthcare 192 planning has much to offer as a discipline: from understanding the health needs of a 193 population through to planning and mapping best practice in the delivery of services 194
and informing the design and configuration of buildings. 195
Consultation draft not for publication
HBN 10-01 January 2020 9
Evidence suggests that the earlier the planning 196 process starts, the more detailed the brief and the 197 smoother the procurement process. 198
The design brief needs to be comprehensive to 199 enable private sector bidders to correctly interpret 200
requirements and develop robust and innovative 201 design solutions. 202
Healthcare planning is an essential part of the work 203 leading up to and including the development of the 204
business case of a healthcare service development 205 – for infrastructure, this may involve a new-build or 206 refurbishment capital scheme. 207
The benefits of a robust healthcare planning process include: 208
the opportunity for healthcare providers to embrace new ways of working 209
a vehicle by which space and environmental requirements can be 210
reconfigured to optimise efficiency 211
support for the production of an informed design brief that balances the 212
relationships between the care process, development and use of medical 213
technologies and the design of the physical environment 214
enabling healthcare providers to develop new models of care and then: 215
o translate them into detailed service specifications 216
o suggest ways in which the services and departments could be 217
configured for optimal performance and efficiency. 218
In summary, the process is about translating opportunities presented in new models 219 of healthcare delivery and new technologies into the requirements for physical space 220
and design. 221
Purpose of the design brief 222
Good briefing and design improves the efficiency of operational relationships. Each 223
HBN identifies unique design quality requirements and aspirations. Every new 224 department will be unique as the demands will be different depending on location, 225 whether a new-build or refurbishment, local staffing issues and demographics. 226
The initial briefing document is vitally important and the make-up of the client project 227 team should encompass all sections of the workforce. The design brief details client 228
requirements and informs the development of the design as it progresses and: 229
provides a clear set of instructions setting out the overarching goals 230
can be used to assess proposals as they are refined. It enables all 231
stakeholders to be aware of the project scope and intended functionality. 232
When finalised, it ensures that there is no scope creep or shortfall. 233

Consultation draft not for publication
HBN 10-01 January 2020 10
can be used to inform a feasibility study and can be used to develop cost 234
and time estimates (etc). 235
The project team should familiarise itself with the intentions of design guides. The 236
generic activity spaces described in this HBN are as described in the full suite of HBNs, 237 including the standard sizes described in HBNs 00-01, 00-02, 00-02 and 00-04 (and 238 also in the ProCure22 Repeatable Room documentation). 239
The design brief will start with a definition of the services or functions to be 240 accommodated, decomposing these functions into specific sub-functions and then to 241
activities. 242
A schedule of accommodation (in effect, a functional brief) is compiled. This sets out 243 the accommodation specifics for preparation of design options and includes: 244
the number and size of activity spaces / rooms 245
relationships between rooms and groups of rooms 246
equipment, furniture, finishes required that will fit the activity space / room 247
for its functional purpose 248
the environmental conditions required for each activity space / room 249
(temperature range, humidity, air movement, acoustics, etc) 250
functional specifications of the department / unit including considerations 251
such as: how it will interact with the whole hospital / healthcare facility; 252
inter-dependencies; fit with policies and organisational goals; intended 253
outputs and benefits; intended further phases of development. 254
Design and quality considerations 255
The healthcare planning and design process needs to be broad enough to include not 256 only the issues surrounding the treatment of disease, but also the promotion of health 257 and prevention of disease – essentially the creation of a safe and therapeutic care 258
environment. 259
Whole hospital policies will generally cover: 260
safety and security including lock-down; 261
privacy and dignity; 262
interior design; 263
wayfinding and access; 264
infection prevention and control; 265
supply and distribution; 266
fire safety strategy; 267
equality; 268
[DN: QUESTION FOR REVIEWERS: what other policies should be included 269
here?]. 270
The following sections cover recognised best practice in the healthcare planning and 271 design processes. 272

Consultation draft not for publication
HBN 10-01 January 2020 11
Involvement of patients and carers in planning and 273
design 274
It is strongly recommended that patients are involved in the co-production of planning 275 and design at a local level. 276
Patients and their carers are experts about themselves and as such are clearly 277 important members of the healthcare team. In the US, a 2017 scientific advisory panel 278 analysed research evidence and compiled a “Framework for Patient and Family 279
Engaged Care”6 (see Appendix X for a discussion document). 280
[DN: QUESTION FOR REVIEWERS: would it be useful to include this as an 281
appendix?] 282
The framework defines steps that healthcare organisations can take to make sure that 283 they are partnering with patients and families in their care: “Patient and family engaged 284 care (PFEC) is care planned, delivered, managed, and continuously improved in active 285 partnership with patients and their families (or care partners as defined by the patient) 286
to ensure integration of their health and health care goals, preferences, and values. It 287
includes explicit and partnered determination of goals and care options, and it requires 288 ongoing assessment of the care match with patient goals.” 289
Successful PFEC requires conversations with healthcare providers about what health 290
means to patient groups and to individual patients and what they need from them in 291 order to live their healthiest lives. Research shows that PFEC leads to: 292
better relationships between patients, carers and healthcare providers; 293
improved patient safety; 294
reduced healthcare costs; 295
reduced unnecessary readmissions to hospital; 296
healthcare staff feeling ‘more connected’ to their work. 297
The Planetree organisation7 based in the US is involved in developing the PFEC 298
framework. It describes person-centred care as “… more than hospitality. It is more 299
than amenities and inviting surroundings. [It] care creates positive impressions and 300 satisfying experiences, but beyond that, it improves lives. [It] creates workplaces that 301 energise and inspire joy at work. It improves health outcomes and unites communities 302
around health and wellness. It can be defined and is attainable and measurable.” 303
Similarly, the Point of Care Foundation (POCF)8 in the UK and Ireland is working to 304 “radically improve the way people are cared for and to support the staff who deliver 305 care”. It uses methodologies such as “Experience-Based Co-Design and Patient and 306 Family-Centred Care” to deliver improvements in care quality. It has programmes 307
6 See https://nam.edu/wp-content/uploads/2017/01/Harnessing-Evidence-and-Experience-to-Change-Culture-A-Guiding-Framework-for-Patient-and-Family-Engaged-Care.pdf?__hssc=139852332.3.1582387943634&__hstc=139852332.f66068011fefdb5e1797d312a2bbb842.1582387943634.1582387943634.1582387943634.1&__hsfp=3419937260&hsCtaTracking=3e06a622-355d-441e-aed6-a06f9a4609a7%7C22d6c8f5-69b5-4e23-ad25-c9762eac5855 7 See https://www.planetree.org/ for details 8 See https://www.pointofcarefoundation.org.uk/ for details
Consultation draft not for publication
HBN 10-01 January 2020 12
running in over 200 hospitals, hospices and other organisations. For an example of 308 the POCF’s work see videos (February 2020) by Our Dorset showing training in patient 309 and engagement – and its impact: 310
https://www.pointofcarefoundation.org.uk/news/new-films-show-impact-of-311 engagement-for-an-integrated-care-system/. 312
Eliminating mixed-sex accommodation 313
Compliance with prevailing standards and guidance in respect of elimination of mixed-314 sex accommodation is required. The DHSC requires all providers of NHS-funded care 315
to confirm that they are compliant with the national definition “to eliminate mixed sex 316 accommodation except where it is in the overall best interests of the patient or reflects 317 the patient's choice”. 318
Care Quality Commission (CQC9) inspections regularly assess compliance of 319 essential standards of quality and safety by those providing NHS services, including 320
NHS-funded care and hospices.10 NHS services should eliminate mixed sex 321 accommodation where it is in the best interests of the individual or reflects personal 322
choice. However, the CQC advises its inspectors that there are some exceptions, 323 including: 324
in the event of a life-threatening emergency; 325
where critically ill patients need one-to-one nursing care in ITU; 326
where a nurse must be physically present in the room/bay at all times e.g. 327
in level 2 (high dependency care); 328
where a short period of close patient observation is needed e.g. post 329
anaesthetic recovery; 330
on the joint admission of couples or family groups. 331
The CQC advises that there is no justification for placing a person in mixed sex 332
accommodation for the following reasons (or similar): 333
more convenient for staff; 334
a shortage of staff or poor skill mix; 335
a shortage of beds; 336
predictable fluctuations in activity or seasonal pressures; 337
predictable non-clinical incidents e.g. ward closures; 338
while waiting for assessment, treatment or a clinical decision; 339
because of restrictions imposed by old estate (i.e. old buildings and 340
facilities are not considered an excuse for non-compliance); 341
9 The CQC is an independent regulator of health and adult social care services in England and protects the interests of those whose rights are restricted under the Mental Health Act 10 See https://services.cqc.org.uk/sites/default/files/gac_-_dec_2011_update.pdf Essential standards of quality and safety

Consultation draft not for publication
HBN 10-01 January 2020 13
based on a clinical specialism (i.e. caring for people within the same 342
clinical specialty e.g. respiratory or orthopdaedics is not an excuse for 343
noncompliance); 344
a ‘take it or leave it’ approach (i.e. if the patient had to choose between 345
accepting mixed sex accommodation and going elsewhere); 346
custom and practice. 347
Mixed sex accommodation refers not only to sleeping arrangements, but also to 348 bathrooms or WCs and the need for patients to pass through areas for the opposite 349 sex to reach their own facilities. 350
There is an additional requirement for mental health and learning disability inpatient 351 units in relation to the availability of same-sex day space, particularly for women who 352
use services. In mental health, promoting physical and sexual safety through 353 eliminating mixed sex accommodation is one of the key things that is cited in terms of 354 promoting sexual safety. 355
Children, and in particular adolescents, need special consideration. 356
The national guidance on eliminating mixed-sex accommodation is only relevant in 357 areas where patients are admitted. Therefore, mixed-sex units are not in breach of the 358
guidance if patients treated will go home the same day their care is provided. 359
NHS organisations should have a policy on mixed sex accommodation. The policy 360
should state what exceptions are permissible and what action staff should take if there 361 is a potential or actual breach. All staff should be aware of the policy. There should be 362 clear monitoring procedures to record where and why a breach has occurred and 363
actions taken to avoid a repeat. (See Appendix 2, Policies Checklist.) 364
Providing privacy and dignity 365
Privacy and dignity are very important to people receiving care. There may be 366
evidence linked to Outcome 1 (of 28) of the CQC’s 16 essential standards: ‘Staff must 367 be aware of the importance of maintaining dignity and privacy at all times and take 368
action’. These outcomes outline what the CQC expects people using a service to 369 experience when the provider is meeting the essential standards. 370
The focus should be on people’s experiences of care, and the quality of the treatment 371
and support that they receive. (This is what matters most to people who use services, 372 rather than the underpinning systems, policies and processes needed to deliver their 373
care.) 374
Creating a therapeutic environment 375
“Environments are considered therapeutic (with healing qualities) when 376 there is direct evidence that a design intervention contributes to 377
improved patient outcomes.” 378
(Chapter 12 of ‘Investing in hospitals of the future’ (WHO, 2009)). 379
Consultation draft not for publication
HBN 10-01 January 2020 14
Healthcare facilities should provide a therapeutic environment in which the overall 380 design of the building contributes to the process of healing and reduces the risk of 381 healthcare-associated infections rather than simply being a place where treatment 382 takes place. 383
Ideally, the following should be provided, but will depend on the location of the unit 384
and whether on a community or acute site: 385
attractive external views; 386
access to nature and outdoors; 387
acoustic benefits; 388
ability to control the environment, where practicable; 389
legibility of place11, including wayfinding aids12. 390
Patients will also spend some time waiting and consideration should be given to the 391 environment and appropriate entertainment/refreshments. Emphasise importance of 392 visual and physical access to nature & outdoors for orientation, stress relief, reduce 393
aggression etc. 394
There needs to be inclusion of the suitability of the unit space to enable some patients 395 to be accompanied by carers/relatives. 396
To be mindful of older people, some of whom will have dementia, refer to design 397 features in Health Building Note 08-02 – ‘General design guidance for dementia-398 friendly health and social care healthcare buildings environments13’ and The King’s 399
Fund Enhancing the Healing Environment Programme’s14 Environmental Assessment 400 Tool15. 401
Ensuring equality 402
Healthcare providers must meet all regulatory requirements with regard to equality. In 403 England, the Disability Discrimination Act (DDA)16 was repealed and replaced by the 404
11 See HBN 00-01 General design guidance for healthcare buildings (2014) especially Chapter 6, ‘Evidence-based design ideas for a therapeutic environment’ https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/316247/HBN_00-01-2.pdf 12 See the 2005 HBN on effective wayfinding and signing systems https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/148500/Wayfinding.pdf 13 See https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/416780/HBN_08-02.pdf 14 The King’s Fund’s Enhancing the Healing Environment Programme encouraged and enabled nurse-led teams to work in partnership with patients to improve the environment in which they deliver care. The EHE programme has now been completed and the work on dementia friendly-design is being taken forward by the Association for Dementia Studies, University of Worcester, see https://www.worcester.ac.uk/about/academic-schools/school-of-allied-health-and-community/allied-health-research/association-for-dementia-studies/home.aspx 15 See https://www.kingsfund.org.uk/sites/default/files/EHE-dementia-assessment-tool.pdf for this PDF tool 16 See http://www.legislation.gov.uk/ukpga/1995/50/contents and https://www.gov.uk/definition-of-disability-under-equality-act-2010

Consultation draft not for publication
HBN 10-01 January 2020 15
Equality Act (2010)17. The Equality Act covers the same groups that 405 were protected by existing equality legislation – age, disability, gender reassignment, 406 race, religion or belief, sex, sexual orientation, marriage and civil partnership and 407 pregnancy and maternity. 408
Equality Act protected characteristics 409
The following are protected characteristics: 410
age; 411
disability; 412
gender reassignment; 413
marriage and civil partnership; 414
pregnancy and maternity; 415
race; 416
religion or belief; 417
sex; 418
sexual orientation. 419
420
The NHS Long Term Plan Section 218 makes the commitment that the service will take 421
appropriate action on prevention of ill-health and health inequalities. 422
Considering adaptability / future-proofing 423
For the majority of services, there is a likelihood that there will be changes in service 424 provision and growth in demand over time, due to advances in treatment and changes 425
in local demographics (and so on). Therefore, it is essential that local project teams 426 develop robust future-proofing / activity modelling as part of the business case process 427 for any new-build or refurbishment scheme. 428
Building in flexibility 429
Healthcare planners should ensure that the unit is designed such that it can be as 430
flexible as possible. 431
Design/decoration considerations will be dependent on infection prevention and 432 control protocols and FM cleaning regimes. See HBN 00-09 on infection control in the 433
built environment. 434
When project-specific, this will be covered within Whole Hospital Policies. 435
17 See http://www.legislation.gov.uk/ukpga/2010/15/contents and https://www.england.nhs.uk/wp-content/uploads/2016/02/nhse-specific-duties-equality-act.pdf for the NHS England response to the specific duties of the Equality Act Equality information relating to public facing functions (2016) 18 See https://www.longtermplan.nhs.uk/online-version/chapter-2-more-nhs-action-on-prevention-and-health-inequalities/

Consultation draft not for publication
HBN 10-01 January 2020 16
[DN: QUESTION FOR REVIEWERS: would it be helpful to include a checklist of 436 policies as an appendix for all HBNs?] 437
Sustainability and ‘Net Zero Carbon’ targets 438
Healthcare provision is a significant contributor to the UK’s carbon footprint. (In 2019, 439 this was estimated to be around 5.4% of our greenhouse gases.) Accordingly, all NHS 440 organisations have their part to play in meeting Net Zero Carbon targets alongside 441
other sustainability measures19. 442
In January 2020, Health chief Sir Simon Stevens announced three steps the NHS will 443
take during 2020 to tackle this problem: 444
1. NHS England has established an expert panel to chart a practical route map to 445 enable the NHS to get to ‘net zero’. The panel will submit an interim report to 446 NHS England in summer 2020 and a final report ahead of the November 2020 447
UN Climate Change Conference (COP26) in Glasgow20. The panel will 448
consider changes the NHS can make in its own activities; in its supply chain; 449 and through wider partnerships; 450
2. the NHS Long Term Plan21 commits to better use of technologies22 to make up 451
to 30 million outpatient appointments redundant, sparing patients thousands of 452
unnecessary trips to and from hospital. It is estimated that 6.7 billion road miles 453 each year are from patients and their visitors travelling to the NHS; 454
3. the panel will consider changes that can be made in the NHS’s medical devices, 455
consumables and pharmaceutical supply, and areas the NHS can influence 456 such as the energy sector as the health service moves to using more renewable 457
energy. 458
Providing a safe and secure environment 459
Design solutions can assist in making healthcare facilities safer and more secure. 460 Security is always an important aspect to consider, involving: 461
the security of the unit; 462
security and safety of the people who use the unit including staff, patients 463
and visitors; 464
potential for lockdown as required (which will be covered by the 465
organisation’s Lockdown Policy). Process of controlling the movement and 466
access – both entry and exit – of people (NHS staff, patients and visitors) 467
around a Trust site or other specific Trust buildings or area in response to 468
an identified risk, threat or hazard that might impact upon the security 469
19 See https://www.england.nhs.uk/2020/01/greener-nhs-campaign-to-tackle-climate-health-emergency/ 20 See https://sdg.iisd.org/events/2020-un-climate-change-conference-unfccc-cop-26/ 21 See https://www.longtermplan.nhs.uk/ 22 See https://www.longtermplan.nhs.uk/online-version/chapter-5-digitally-enabled-care-will-go-mainstream-across-the-nhs/
Consultation draft not for publication
HBN 10-01 January 2020 17
and/or safety of patients, staff and assets or, indeed, the capacity of that 470
facility/service to continue to operate. 471
See HBN 00-07, Resilience planning for NHS facilities23, which provides guidance on 472 designing and planning for a resilient healthcare estate. (This Technical Standard aims 473 to help NHS-funded providers to determine appropriate levels of resilience for sites, 474 buildings and installations against a wide range of emergencies, hazards and threats 475
and their impacts and consequences including resilience to the impacts of climate 476 change.) 477
478
479
480
23 See https://www.gov.uk/government/publications/resilience-planning-for-nhs-facilities

Consultation draft not for publication
HBN 10-01 January 2020 18
Contents 481
482
Introduction to the Technical Standards ................................................................................................ 3 483
What is best practice guidance? ......................................................................................................... 3 484
Health Building Notes (HBNs) ......................................................................................................... 3 485
Health Technical Memoranda (HTMs) ............................................................................................ 4 486
Compliance matters ............................................................................................................................ 5 487
Assurance of healthcare infrastructure .............................................................................................. 6 488
Language usage in Technical Standards.............................................................................................. 6 489
Project derogations from the Technical Standards ............................................................................ 7 490
Overview of the healthcare planning process ........................................................................................ 8 491
Purpose of the design brief ................................................................................................................. 9 492
Design and quality considerations ........................................................................................................ 10 493
Involvement of patients and carers in planning and design ............................................................. 11 494
Eliminating mixed-sex accommodation ............................................................................................ 12 495
Providing privacy and dignity ............................................................................................................ 13 496
Creating a therapeutic environment ................................................................................................ 13 497
Ensuring equality............................................................................................................................... 14 498
Equality Act protected characteristics .......................................................................................... 15 499
Considering adaptability / future-proofing ....................................................................................... 15 500
Building in flexibility .......................................................................................................................... 15 501
Sustainability and ‘Net Zero Carbon’ targets .................................................................................... 16 502
Providing a safe and secure environment ........................................................................................ 16 503
1.0 Introduction to Health Building Note 10-01 ................................................................................... 23 504
Policy context .................................................................................................................................... 23 505
Adaptability / flexibility and future-proofing .................................................................................... 24 506
2.0 Access .............................................................................................................................................. 24 507
Patient journey / patient pathway .................................................................................................... 24 508
In-patient surgery ............................................................................................................................. 25 509
Day surgery ....................................................................................................................................... 25 510
‘Loop’ pathway .............................................................................................................................. 25 511
‘Shuffle’ pathway .......................................................................................................................... 25 512
3.0 Activity spaces ................................................................................................................................. 26 513
Functional Content & Space Standards ............................................................................................ 26 514

Consultation draft not for publication
HBN 10-01 January 2020 19
Space standards: HBN 10-01 ......................................................................................................... 26 515
Space standards: HBN 00 series .................................................................................................... 26 516
Space standards: ProCure 22 Framework ‘Repeatable Rooms’ ................................................... 27 517
Developing the schedule of accommodation ................................................................................... 27 518
Front of House / Entrance Facilities .................................................................................................. 29 519
Reception & Staff Base:................................................................................................................. 29 520
Waiting Room: .............................................................................................................................. 29 521
Admissions Lounge: ...................................................................................................................... 29 522
Interview / Counselling Room: ...................................................................................................... 30 523
Operating Theatre Suite .................................................................................................................... 30 524
Traditional UK General Arrangement: .......................................................................................... 30 525
Patient & Staff Flows: .................................................................................................................... 31 526
Air Pressure Regime: ..................................................................................................................... 31 527
General Operating Theatre ............................................................................................................... 31 528
The space will be used by: ............................................................................................................ 32 529
The area will accommodate: ......................................................................................................... 32 530
Activities: ....................................................................................................................................... 32 531
Adjacencies: .................................................................................................................................. 33 532
Suggested Room Layout:............................................................................................................... 34 533
Minor Operating Theatre .................................................................................................................. 35 534
The space will be used by: ............................................................................................................ 35 535
The area will accommodate: ......................................................................................................... 35 536
Activities: ....................................................................................................................................... 35 537
Suggested Room Layout:............................................................................................................... 37 538
Enhanced Treatment ........................................................................................................................ 38 539
The space will be used by: ............................................................................................................ 38 540
The area will accommodate: ......................................................................................................... 38 541
Activities: ....................................................................................................................................... 38 542
Adjacencies: .................................................................................................................................. 39 543
Suggested Room Layout:............................................................................................................... 40 544
Anaesthetic Room ............................................................................................................................. 41 545
The space will be used by: ............................................................................................................ 41 546
Activities: ....................................................................................................................................... 41 547
Adjacencies: .................................................................................................................................. 42 548
Suggested Room Layout:............................................................................................................... 43 549
Consultation draft not for publication
HBN 10-01 January 2020 20
Preparation Room ............................................................................................................................. 43 550
The space will be used by: ............................................................................................................ 44 551
Activities: ....................................................................................................................................... 44 552
Adjacencies: .................................................................................................................................. 44 553
Suggested Room Layout:............................................................................................................... 45 554
Scrub up & Gowning ......................................................................................................................... 45 555
The space will be used by: ............................................................................................................ 45 556
Activities: ....................................................................................................................................... 45 557
Adjacencies: .................................................................................................................................. 46 558
Suggested Room Layout:............................................................................................................... 47 559
Theatre Dirty Utility .......................................................................................................................... 47 560
The space will be used by: ............................................................................................................ 47 561
Activities: ....................................................................................................................................... 47 562
Adjacencies: .................................................................................................................................. 48 563
Suggested Room Layout:............................................................................................................... 48 564
Exit Bay .............................................................................................................................................. 48 565
Alternative Theatre Suite Model ...................................................................................................... 49 566
General Department Arrangement:.............................................................................................. 49 567
Sedation within the theatre: ......................................................................................................... 49 568
Scrub on entry to the department: ............................................................................................... 49 569
Dirty items bagged and taken to disposal hold: ........................................................................... 49 570
Disposal Hold .................................................................................................................................... 50 571
Suggested Room Layout:............................................................................................................... 50 572
Storage .............................................................................................................................................. 51 573
Bulk Store: ..................................................................................................................................... 51 574
Clinical Equipment Store: .............................................................................................................. 51 575
Linen Store: ................................................................................................................................... 51 576
Ready-use Store: ........................................................................................................................... 52 577
Blood Storage: ............................................................................................................................... 52 578
Storage Requirement Calculator: .................................................................................................. 52 579
Recovery Unit .................................................................................................................................... 52 580
Suggested General Arrangement: ................................................................................................. 52 581
Recovery Room / Bays: ................................................................................................................. 53 582
Recovery Staff Base ....................................................................................................................... 53 583
Recovery Clean Utility ................................................................................................................... 54 584
Consultation draft not for publication
HBN 10-01 January 2020 21
Recovery Dirty Utility .................................................................................................................... 54 585
Staff Accommodation ....................................................................................................................... 54 586
Rest Facilities:................................................................................................................................ 54 587
Beverage Bay:................................................................................................................................ 54 588
Changing Facilities: ........................................................................................................................ 54 589
Offices: .......................................................................................................................................... 54 590
Hybrid Operating Theatres ............................................................................................................... 54 591
The space will be used by: ............................................................................................................ 55 592
Adjacencies: .................................................................................................................................. 56 593
Suggested Room Layout:............................................................................................................... 56 594
Support/utility ............................................................................................................................... 57 595
4.0 Engineering requirements .............................................................................................................. 58 596
Introduction ...................................................................................................................................... 58 597
Environmental requirements ............................................................................................................ 58 598
Energy ............................................................................................................................................... 58 599
Maximum demands .......................................................................................................................... 59 600
Services distribution .......................................................................................................................... 59 601
Isolation ............................................................................................................................................ 59 602
Commissioning .................................................................................................................................. 59 603
The operating theatre ....................................................................................................................... 60 604
Mechanical services ...................................................................................................................... 60 605
Electrical services .......................................................................................................................... 61 606
Public health services .................................................................................................................... 63 607
First stage and second stage recovery .............................................................................................. 63 608
Mechanical services ...................................................................................................................... 63 609
Electrical services .......................................................................................................................... 65 610
Public health services .................................................................................................................... 67 611
References ............................................................................................................................................ 68 612
HBNs .............................................................................................................................................. 68 613
HTMs ............................................................................................................................................. 68 614
Acts and Regulations ..................................................................................................................... 68 615
Standards ...................................................................................................................................... 68 616
NHS national policies .................................................................................................................... 68 617
Other ............................................................................................................................................. 68 618
Wider sources of healthcare planning information, tools and support ........................................... 69 619
Consultation draft not for publication
HBN 10-01 January 2020 22
NHS England & NHS Improvement’s Model Hospital Portal......................................................... 69 620
The ProCure22 Framework ........................................................................................................... 69 621
Miscellaneous sources including professional membership organisations .................................. 69 622
Appendices ............................................................................................................................................ 72 623
Room data sheets ............................................................................................................................. 72 624
Useful reading ..................................................................................................................................... 116 625
626
627

Consultation draft not for publication
HBN 10-01 January 2020 23
1.0 Introduction to Health Building Note 628
10-01 629
1.1 HBN 10-01 ‘Facilities for surgery’ is a new Technical Standard that replaces 630 HBN 26 ‘Facilities for surgical procedures’ (2004) and HBN 10-02 ‘Facilities for 631
day surgery units’ (2007). It provides guidance on the planning and design of 632 infrastructure for inpatient and day patient surgical services in the UK. Since 633 HBNs 26 and 10-02 were published, research shows that common problems in 634 operating theatre suites include: 635
Design-related factors: 636
o ventilation 637
o temperature and humidity 638
o acoustical environment 639
o lighting 640
o materials 641
Environmental threats to patient safety include: 642
o frequent door swings 643
o clutter 644
o poor air quality 645
o surface contamination 646
o excessive noise 647
Staff performance and satisfaction are impacted by factors such as: 648
o general layout 649
o equipment and furniture 650
o ergonomics 651
1.2 HBN 10-01 addresses these issues, providing new standards – activity space 652
layouts, adjacencies, functional content and exemplar schedules of 653 accommodation. Checklists for stakeholder needs and quality of patient/staff 654 experience are included. [DN: these to follow.] Engineering considerations have 655 been updated and reference the latest guidance, standards, regulations and 656
legislation. 657
Policy context 658
1.3 The design of operating suites requires a complete understanding of not only 659 built environment factors but also roles of different team members, the tasks 660 they perform, the processes involved during a procedure, and the myriad 661
equipment and technology that is integrated into the department / unit zones. 662
1.4 This HBN is a response to latest thinking. The strongest body of research deals 663
with environmental factors impacting bacterial contamination and SSIs: 664
Consultation draft not for publication
HBN 10-01 January 2020 24
Laminar flow ventilation systems have been shown to help reduce SSIs in 665
some studies while other studies showed no difference between laminar 666
flow systems and traditional ventilation systems. 667
Frequent door swings are also a major problem that affect airflow and 668
cause disruptions. 669
1.5 Persistent problems posed by the built environment to patient and staff safety 670 are generally in the form of contaminated surfaces, inadequate workspaces, 671 trip hazards, loud noises, poor furniture and equipment ergonomics, and 672 uncomfortable working environments (temperature, humidity, and air quality). 673 Appropriately-sized activity spaces are critical, given the increasing amount of 674
equipment and numbers of people in the modern theatre suite. Storage needs 675 are such that essential items must be immediately available at hand. 676
Adaptability / flexibility and future-proofing 677
1.6 Surgical practices evolve more rapidly than one can modify a corresponding 678 built environment. The complex interaction of these system components and 679 spaces will have an impact patient and staff safety, efficiency, and satisfaction. 680
1.7 Built environments will evolve over the coming years, as technology advances 681
rapidly, and as many different types of procedures can be done safely as day 682
cases. Innovation in design should keep pace with innovation in clinical 683 services. It must be based on a strong understanding of the evidence base and 684 be informed by a multidisciplinary systems approach to developing and testing 685
concepts and ideas. 686
687
2.0 Access 688
Patient journey / patient pathway 689
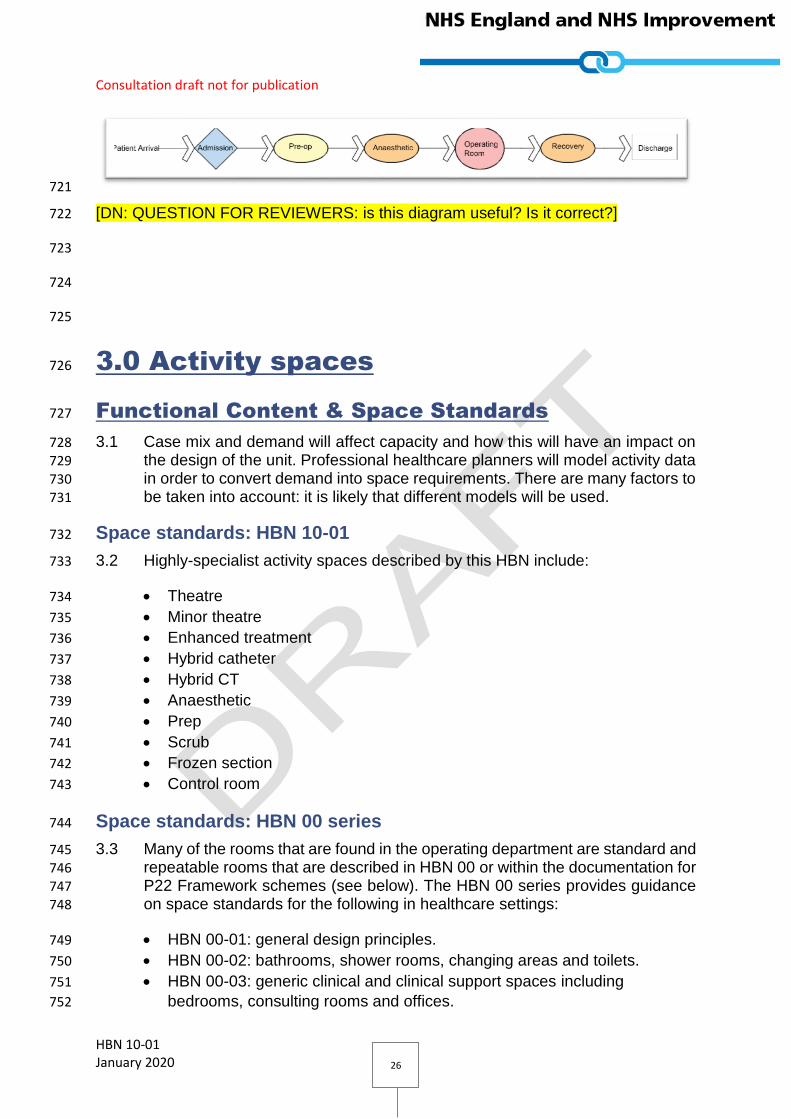
2.1 The design of the facility should facilitate uninterrupted patient flow. On their 690 operation day, patients make the following journey through: 691
main reception area; 692
admission suite; 693
sub-waiting area; 694
anaesthetic room; 695
operating theatre; 696
post-anaesthesia care unit (PACU); 697
second-stage recovery; 698
discharge lounge. 699
2.2 The operating theatres should be on the same floor as the admission suite and 700 recovery areas. 701

Consultation draft not for publication
HBN 10-01 January 2020 25
2.3 As an increasing number of patients undergo surgery without a general 702 anaesthetic, remaining conscious throughout the entire procedure, and hence 703 remain aware of their surroundings even in the operating theatre. 704
2.4 Designers should aim to create an environment that is conducive to making 705 patients feel at ease and giving them confidence, thus aiding the healing 706
process. At the same time, it should facilitate efficient working, and contribute 707 to staff morale. 708
In-patient surgery 709
710
711
[DN: QUESTION FOR REVIEWERS: is this diagram useful? Is it correct? Should 712 critical care be added as an alternative to recovery?] 713
Day surgery 714
‘Loop’ pathway 715
2.5 After Recovery Stage 1, patients go to post-op prior to discharge. 716
717
[DN: QUESTION FOR REVIEWERS: is this diagram useful? Is it correct?] 718
‘Shuffle’ pathway 719
2.6 Patients go to recovery prior to discharge. 720
Consultation draft not for publication
HBN 10-01 January 2020 26
721
[DN: QUESTION FOR REVIEWERS: is this diagram useful? Is it correct?] 722
723
724
725
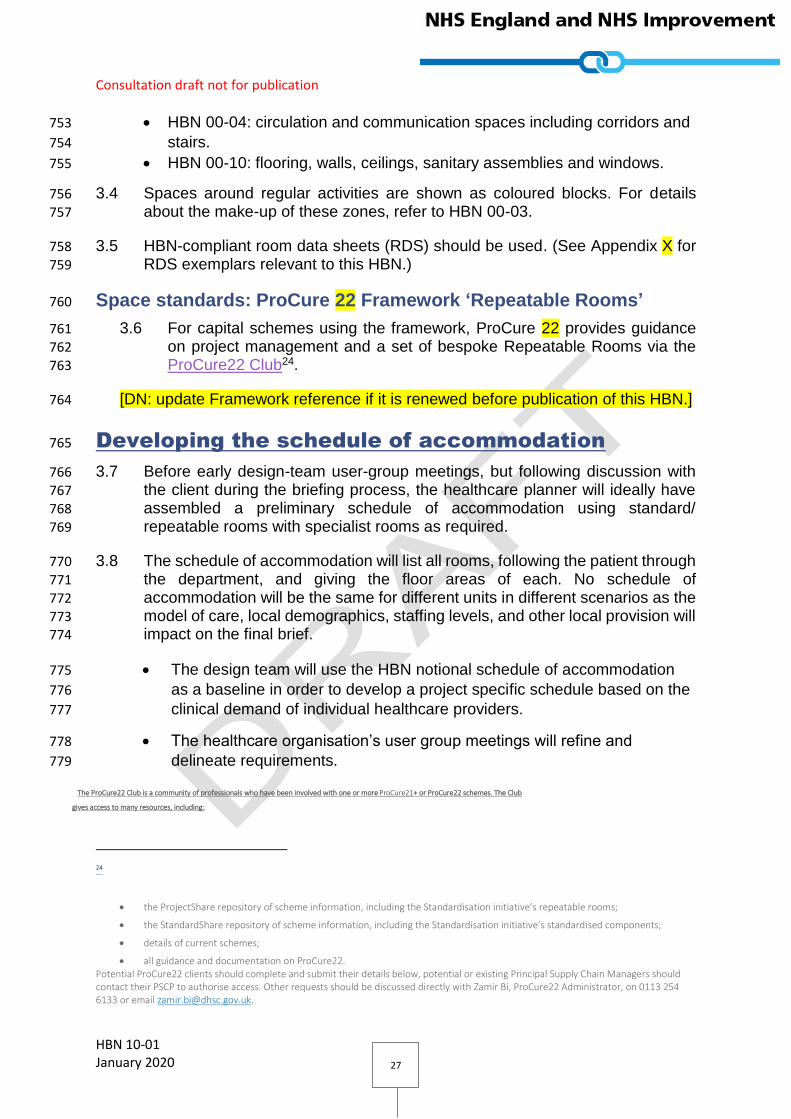
3.0 Activity spaces 726
Functional Content & Space Standards 727
3.1 Case mix and demand will affect capacity and how this will have an impact on 728 the design of the unit. Professional healthcare planners will model activity data 729 in order to convert demand into space requirements. There are many factors to 730
be taken into account: it is likely that different models will be used. 731
Space standards: HBN 10-01 732
3.2 Highly-specialist activity spaces described by this HBN include: 733
Theatre 734
Minor theatre 735
Enhanced treatment 736
Hybrid catheter 737
Hybrid CT 738
Anaesthetic 739
Prep 740
Scrub 741
Frozen section 742
Control room 743
Space standards: HBN 00 series 744
3.3 Many of the rooms that are found in the operating department are standard and 745 repeatable rooms that are described in HBN 00 or within the documentation for 746
P22 Framework schemes (see below). The HBN 00 series provides guidance 747 on space standards for the following in healthcare settings: 748
HBN 00-01: general design principles. 749
HBN 00-02: bathrooms, shower rooms, changing areas and toilets. 750
HBN 00-03: generic clinical and clinical support spaces including 751
bedrooms, consulting rooms and offices. 752
Consultation draft not for publication
HBN 10-01 January 2020 27
HBN 00-04: circulation and communication spaces including corridors and 753
stairs. 754
HBN 00-10: flooring, walls, ceilings, sanitary assemblies and windows. 755
3.4 Spaces around regular activities are shown as coloured blocks. For details 756 about the make-up of these zones, refer to HBN 00-03. 757
3.5 HBN-compliant room data sheets (RDS) should be used. (See Appendix X for 758 RDS exemplars relevant to this HBN.) 759
Space standards: ProCure 22 Framework ‘Repeatable Rooms’ 760
3.6 For capital schemes using the framework, ProCure 22 provides guidance 761 on project management and a set of bespoke Repeatable Rooms via the 762 ProCure22 Club24. 763
[DN: update Framework reference if it is renewed before publication of this HBN.] 764
Developing the schedule of accommodation 765
3.7 Before early design-team user-group meetings, but following discussion with 766
the client during the briefing process, the healthcare planner will ideally have 767 assembled a preliminary schedule of accommodation using standard/ 768
repeatable rooms with specialist rooms as required. 769
3.8 The schedule of accommodation will list all rooms, following the patient through 770
the department, and giving the floor areas of each. No schedule of 771 accommodation will be the same for different units in different scenarios as the 772
model of care, local demographics, staffing levels, and other local provision will 773 impact on the final brief. 774
The design team will use the HBN notional schedule of accommodation 775
as a baseline in order to develop a project specific schedule based on the 776
clinical demand of individual healthcare providers. 777
The healthcare organisation’s user group meetings will refine and 778
delineate requirements. 779
24
The ProCure22 Club is a community of professionals who have been involved with one or more ProCure21+ or ProCure22 schemes. The Club
gives access to many resources, including:
the ProjectShare repository of scheme information, including the Standardisation initiative’s repeatable rooms;
the StandardShare repository of scheme information, including the Standardisation initiative’s standardised components;
details of current schemes;
all guidance and documentation on ProCure22. Potential ProCure22 clients should complete and submit their details below, potential or existing Principal Supply Chain Managers should contact their PSCP to authorise access. Other requests should be discussed directly with Zamir Bi, ProCure22 Administrator, on 0113 254 6133 or email [email protected].

Consultation draft not for publication
HBN 10-01 January 2020 28
3.9 The client and design team should be aware that the choice of procurement 780 route may have an impact on the choice of activity spaces and thus the 781 schedule of accommodation. 782
783
784
785
786
787
788
Figure X: Design team response to procurement route 789
790
3.10 The process is as follows: 791
792
Design team develops
activity spaces compliant with procurement
route
Client chooses procurement route
Client directs design team to follow appropriate guidance
Design team responds to user requirements including model of care, local demographics, staffing levels and other local provisions
User group meetings delineate requirements
and refine the schedule of accommodation
Design team creates a project-specific schedule of accommodation based on local clinical demand
Design team uses the HBN exemplar schedule of accommodation as a
baseline
Project-specific
schedule of
accommodation
Consultation draft not for publication
HBN 10-01 January 2020 29
793
Front of House / Entrance Facilities 794
Reception & Staff Base: 795
3.11 On entering the department, the patient should be greeted by a reception desk. 796 Guidance for provision of reception desks can be found in HBN 00-03 Section 797 7. 798
3.12 Depending on the layout of the department, additional staff bases may be 799
required. 800
Waiting Room: 801
3.13 The area of the central waiting space area will be calculated to accommodate 802 the maximum number of predicted patients and will also allow for escorts, 803
carers and wheelchair users. A metric will be used to determine the numbers 804 which will depend on location and demographics. The patient may be ambulant 805 or in a wheelchair. The waiting area should be overseen by the staff base. 806 Beverage facilities and sanitary facilities should be close by. Information 807
systems should be provided and the ambience of the room should be calming 808 and relaxing. Refer to HBN 00-03, chapter 7 for guidance on waiting-area 809
provision. 810
Admissions Lounge: 811
3.14 If patients arrive in the operating department for surgery straight from their 812 homes, the waiting room should be utilised as part of the admissions lounge. 813
The size of the room should be increased to accommodate up to ten people at 814 one time. 815
3.15 Patients arriving in the lounge will have had their pre-operative assessment and 816 examination previously and should only require minimal physical assessment 817
on the day of surgery. A small number of consulting/ changing rooms with an 818
examination couch will be required, with entry from the waiting area and a 819
separate exit to the operating suite. 820
3.16 Under this system, patients will be formally identified and admitted once they 821 have entered a consulting room, in order to maintain their privacy. They will 822 change in this room and not return to the waiting area. All doors will require 823 secure access and should be wheelchair-accessible. The patients’ clothing will 824
be securely labelled and transferred to their in-patient accommodation via the 825 recovery unit. 826
3.17 Refer to HBN 00-03 for guidance on the provision of consulting rooms. 827
Consultation draft not for publication
HBN 10-01 January 2020 30
Interview / Counselling Room: 828
3.18 An Interview / counselling room should be provided for quiet conversations and 829 for breaking bad news to patients and their families. Examples of standard 830
counselling rooms are described within HBN 00-03. 831
3.19 This room can be used flexibly as required. 832
Operating Theatre Suite 833
3.20 Whilst each room will be described individually, it is important to first consider 834
the suite as a whole, for the purpose of patient and staff flows, clean and dirty 835 areas, and air pressure regimes. 836
Traditional UK General Arrangement: 837
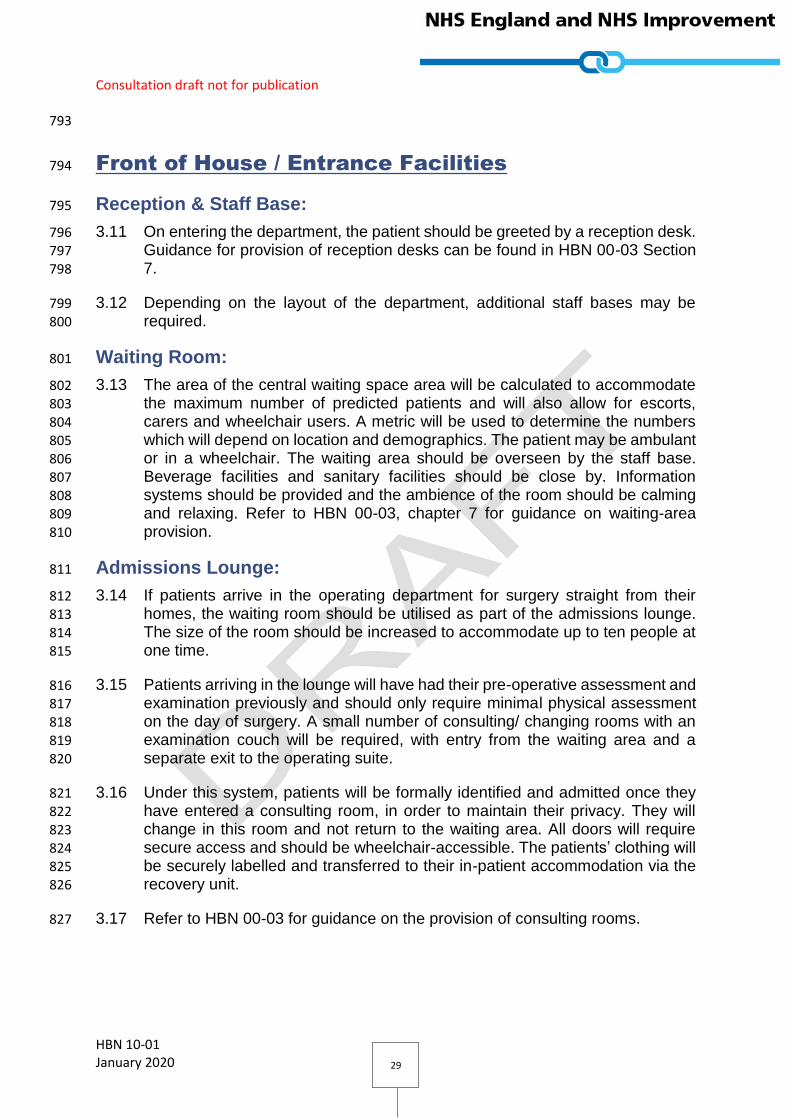
3.21 The majority of UK operating theatre suites consist of the following rooms: 838
Operating Theatre 839
Anaesthetic Room 840
Preparation 841
Scrub 842
Dirty Utility 843
Exit Bay. 844
3.22 This suite can then be multiplied to provide the requisite number of operating 845 theatres to meet demand. 846

Consultation draft not for publication
HBN 10-01 January 2020 31
3.23 Some space efficiencies can be achieved through the sharing of either the 847 anaesthetic room, scrub, or dirty utility between two or more theatres. For this 848 reason, theatre suites are often paired and therefore it is recommended in any 849 new-build facilities that there are an even number of theatres. 850
Patient & Staff Flows: 851
852
3.24 The patient will enter the theatre through the anaesthetic room and will exit via 853
the exit bay. 854
3.25 Anaesthetic staff will enter via the anaesthetic room, whilst the surgeons and 855
scrub nurses will enter via the scrub room. 856
3.26 Clean supplies are delivered to the preparation room, where they are prepared 857 and laid out on trolleys for transfer to the theatre. Dirty waste is stored in the 858
dirty utility until it is transferred to the disposal hold. It is important that the dirty 859 flow is kept away from patient and staff movement as much as is practicable. 860
Air Pressure Regime: 861
3.27 [DN: QUESTION FOR REVIEWERS: Should we include a diagram and 862
supporting text describing the air pressure regime here (or in the engineering 863 section)? 864
Cross-reference HTM 03-01.] 865
General Operating Theatre 866
3.28 The general operating theatre will be used for the majority of complex 867
interventions. 868
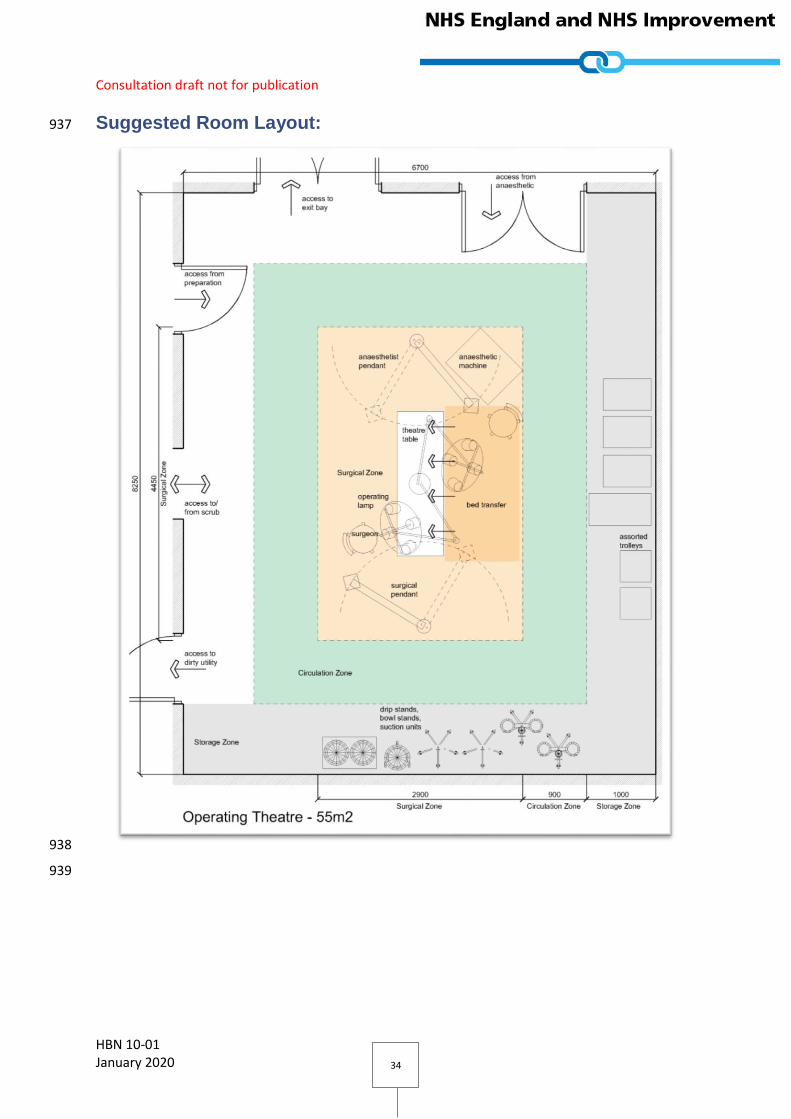
3.29 The recommended size for a general operating theatre is 55m2. 869
Consultation draft not for publication
HBN 10-01 January 2020 32
The space will be used by: 870
The patient; 871
Up to 10 staff, including: 872
o Surgical team & assisting staff; 873
o Anaesthetist & assisting staff; 874
o Circulating support staff 875
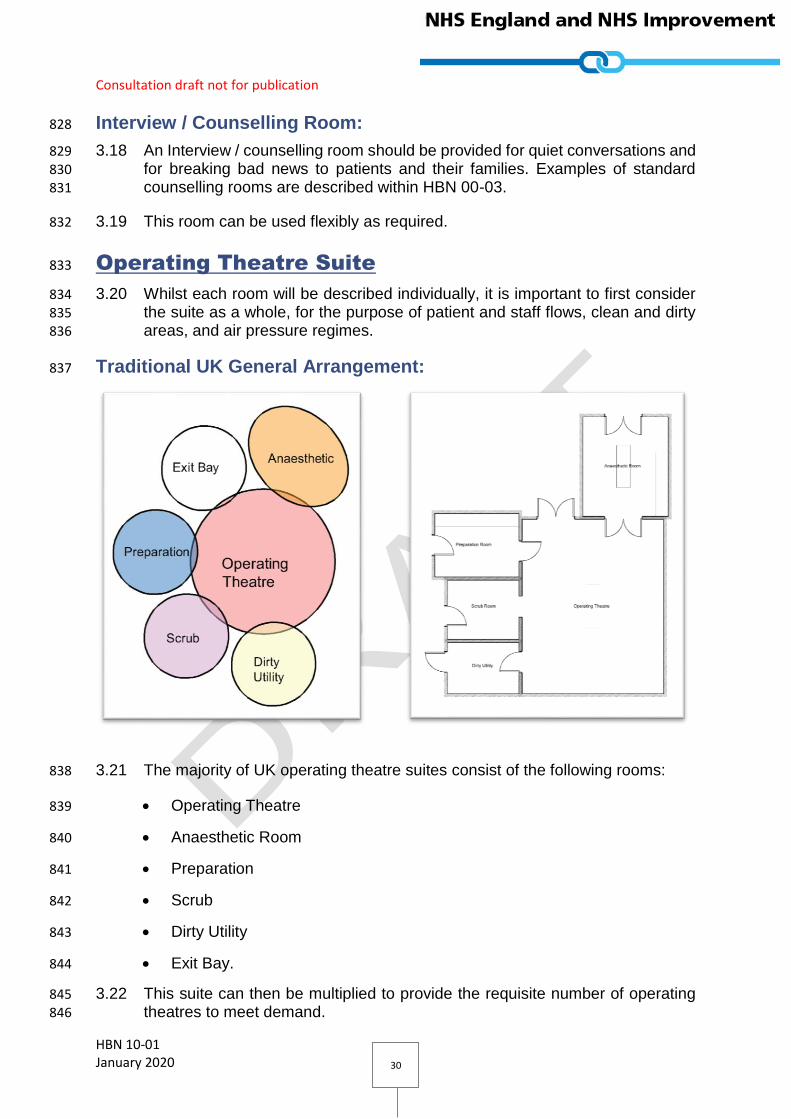
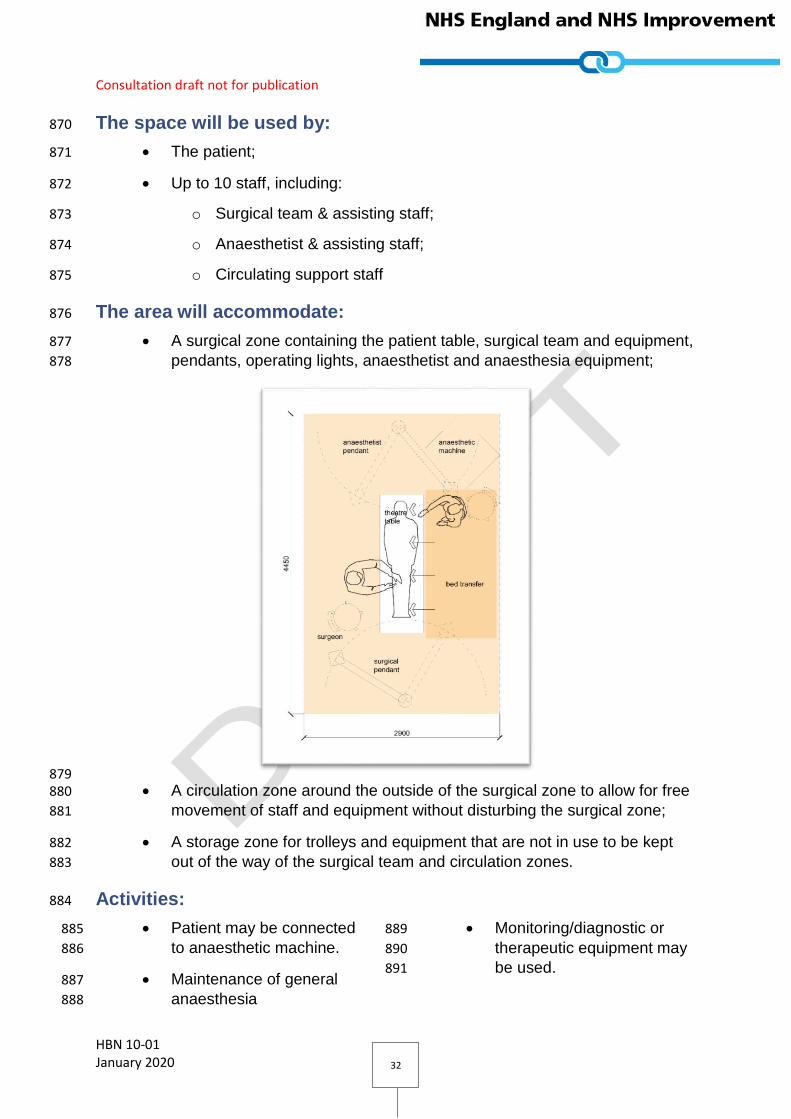
The area will accommodate: 876
A surgical zone containing the patient table, surgical team and equipment, 877
pendants, operating lights, anaesthetist and anaesthesia equipment; 878
879 A circulation zone around the outside of the surgical zone to allow for free 880
movement of staff and equipment without disturbing the surgical zone; 881
A storage zone for trolleys and equipment that are not in use to be kept 882
out of the way of the surgical team and circulation zones. 883
Activities: 884
Patient may be connected 885
to anaesthetic machine. 886
Maintenance of general 887
anaesthesia 888
Monitoring/diagnostic or 889
therapeutic equipment may 890
be used. 891
Consultation draft not for publication
HBN 10-01 January 2020 33
Assembling and connecting 892
mobile equipment. 893
Surgical instruments on 894
instrument trolley may be 895
used. 896
Surgical procedures may be 897
performed under local or 898
general anaesthetic. 899
Mobile image intensifier 900
may be used. 901
Computer generated 902
images are viewed using 903
ceiling or wall mounted 904
screens. 905
Used swabs may be 906
checked, weighed and 907
recorded. 908
Operating lists may be 909
displayed. 910
Recording patient 911
data/notes. 912
Electronic patient records 913
(EPRs) may be accessed 914
and updated. 915
Patient is transferred from 916
operating table to 917
bed/trolley. 918
Storage of small items of 919
equipment or consumables 920
as required 921
Theatre control panel 922
should be flush mounted. 923
"IN USE" sign sited outside 924
the doorway of the room. 925
anaesthetic machine may 926
be located on a dedicated 927
medical supply unit - project 928
team option929
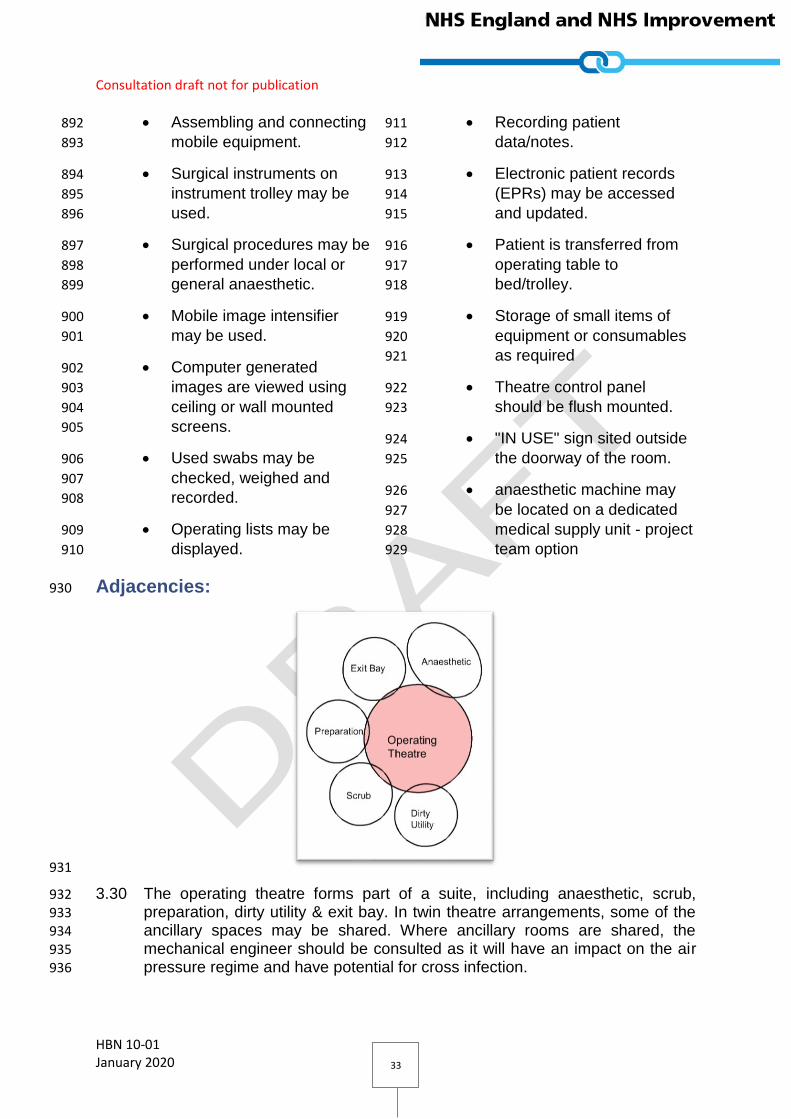
Adjacencies: 930
931
3.30 The operating theatre forms part of a suite, including anaesthetic, scrub, 932 preparation, dirty utility & exit bay. In twin theatre arrangements, some of the 933 ancillary spaces may be shared. Where ancillary rooms are shared, the 934
mechanical engineer should be consulted as it will have an impact on the air 935 pressure regime and have potential for cross infection. 936
Consultation draft not for publication
HBN 10-01 January 2020 34
Suggested Room Layout: 937
938
939
Consultation draft not for publication
HBN 10-01 January 2020 35
Minor Operating Theatre 940
3.31 Where less complex interventions are undertaken, a smaller minor operating 941 theatre may be used. The operations that can be accommodated include: 942
XYZ 943
[DN: QUESTION FOR REVIEWERS: please advise which procedures should 944
be included in this list.] 945
3.32 The recommended size for a minor operating theatre is 42m2. 946
3.33 The general arrangement of the minor operating theatre is similar to that of the 947 general operating theatre, but with smaller circulation and storage zones. 948
The space will be used by: 949
The patient; 950
Up to six staff, including: 951
o Surgical team & assisting staff; 952
o Anaesthetist & assisting staff; 953
o Circulating support staff 954
The area will accommodate: 955
A surgical zone containing the patient table, surgical team and equipment, 956
pendants, operating lights, anaesthetist and anaesthesia equipment; 957
A circulation zone around the outside of the surgical zone to allow for free 958
movement of staff and equipment without disturbing the surgical zone; 959
A storage zone for trolleys and equipment that are not in use to be kept 960
out of the way of the surgical team and circulation zones. 961
Activities: 962
Patient may be connected 963
to anaesthetic machine. 964
Maintenance of general 965
anaesthesia 966
Monitoring/diagnostic or 967
therapeutic equipment may 968
be used. 969
Assembling and connecting 970
mobile equipment. 971
Surgical instruments on 972
instrument trolley may be 973
used. 974
Surgical procedures may be 975
performed under local or 976
general anaesthetic. 977
Mobile image intensifier 978
may be used. 979
Computer generated 980
images are viewed using 981

Consultation draft not for publication
HBN 10-01 January 2020 36
ceiling or wall mounted 982
screens. 983
Used swabs may be 984
checked, weighed and 985
recorded. 986
Operating lists may be 987
displayed. 988
Recording patient 989
data/notes. 990
Electronic patient records 991
(EPRs) may be accessed 992
and updated. 993
Patient is transferred from 994
operating table to 995
bed/trolley. 996
Storage of small items of 997
equipment or consumables 998
as required 999
Theatre control panel 1000
should be flush mounted. 1001
"IN USE" sign sited outside 1002
the doorway of the room. 1003
anaesthetic machine may 1004
be located on a dedicated 1005
medical supply unit - project 1006
team option 1007
1008
1009

Consultation draft not for publication
HBN 10-01 January 2020 37
Suggested Room Layout: 1010
1011
1012

Consultation draft not for publication
HBN 10-01 January 2020 38
Enhanced Treatment 1013
3.34 Where minor interventions are required, an enhanced treatment room may be 1014 used. The operations that can be accommodated include: 1015
XYZ 1016
[DN: QUESTION FOR REVIEWERS: please advise which procedures should 1017
be included in this list.] 1018
3.35 The recommended size for an Enhanced Treatment Room is 24m2. 1019
3.36 Patients in an enhanced treatment room will not be placed under general 1020 anaesthetic. 1021
The space will be used by: 1022
The patient; 1023
Up to three staff, including: 1024
o Surgeon; 1025
o Scrub and support team. 1026
The area will accommodate: 1027
A surgical zone containing the patient table, surgical team and equipment, 1028
pendants, operating lights, anaesthetist and anaesthesia equipment; 1029
A circulation zone for entry from ancillary rooms and movement; 1030
A storage zone. 1031
Activities: 1032
Monitoring/diagnostic or 1033
therapeutic equipment may 1034
be used. 1035
Assembling and connecting 1036
mobile equipment. 1037
Surgical instruments on 1038
instrument trolley may be 1039
used. 1040
Surgical procedures may be 1041
performed under local or 1042
anaesthetic or nerve block 1043
Computer generated 1044
images are viewed using 1045
ceiling or wall mounted 1046
screens 1047
Used swabs may be 1048
checked, weighed and 1049
recorded. 1050
Operating lists may be 1051
displayed. 1052
Recording patient 1053
data/notes. 1054
Electronic patient records 1055
(EPRs) may be accessed 1056
and updated. 1057
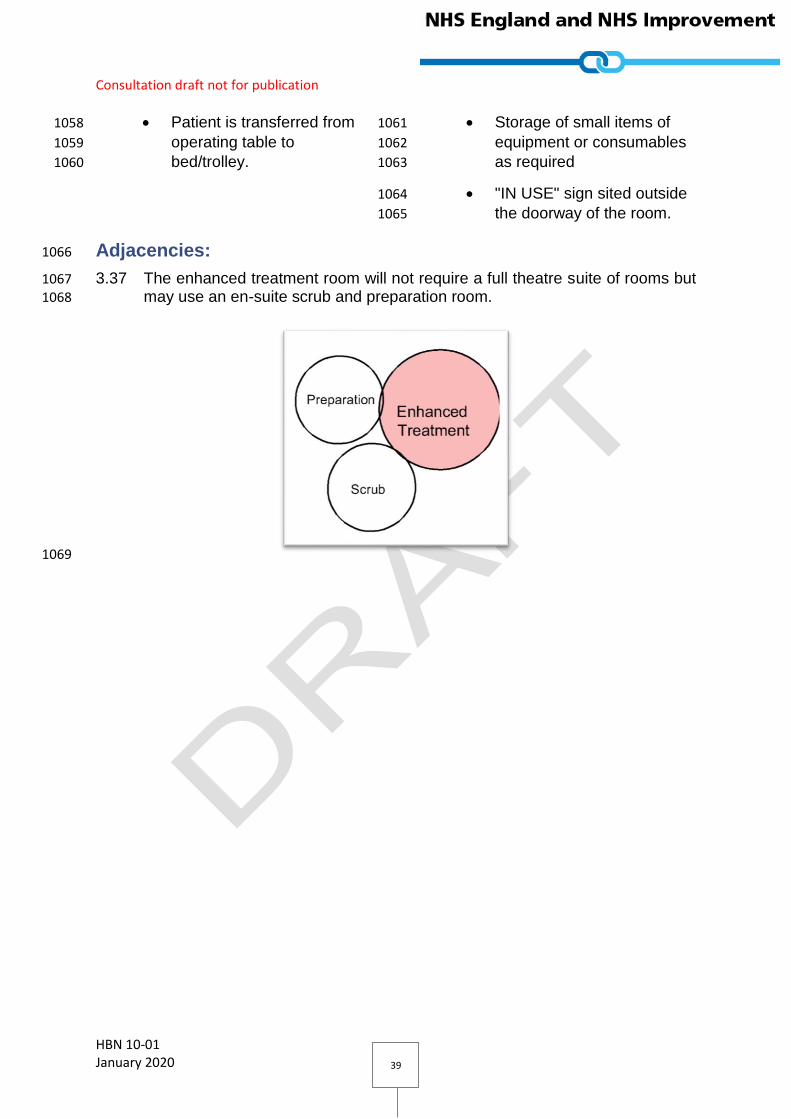
Consultation draft not for publication
HBN 10-01 January 2020 39
Patient is transferred from 1058
operating table to 1059
bed/trolley. 1060
Storage of small items of 1061
equipment or consumables 1062
as required 1063
"IN USE" sign sited outside 1064
the doorway of the room.1065
Adjacencies: 1066
3.37 The enhanced treatment room will not require a full theatre suite of rooms but 1067
may use an en-suite scrub and preparation room. 1068
1069
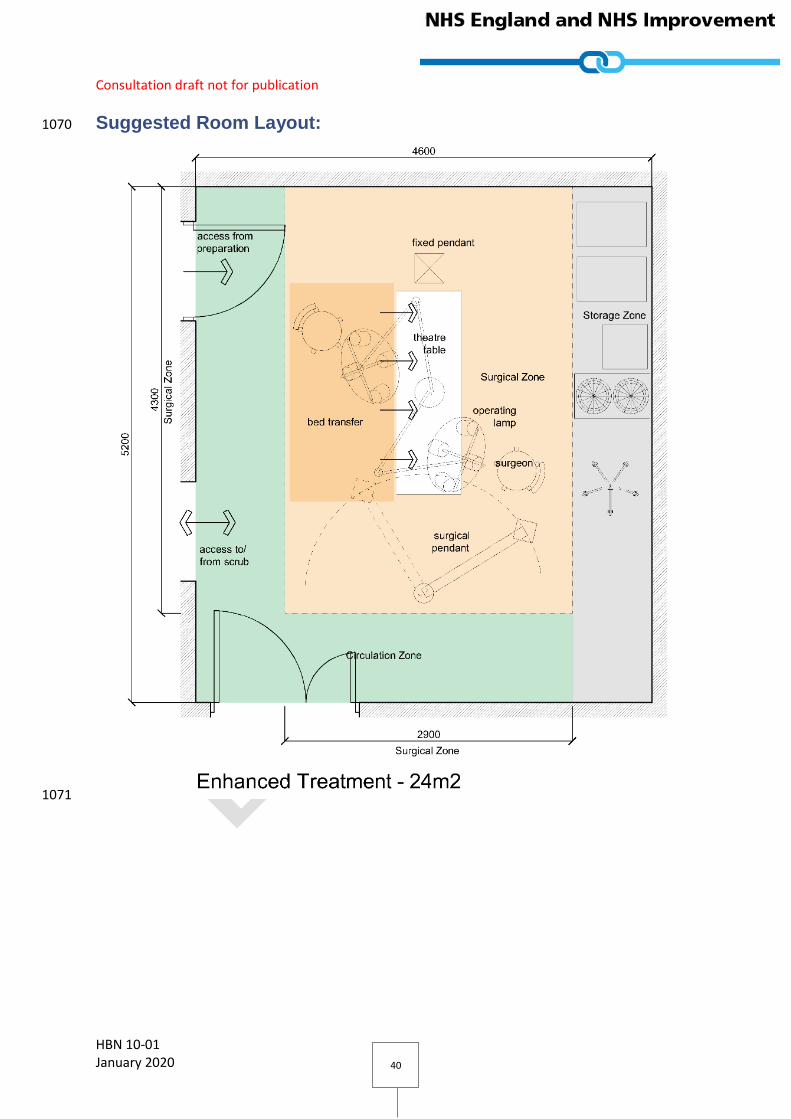
Consultation draft not for publication
HBN 10-01 January 2020 40
Suggested Room Layout: 1070
1071

Consultation draft not for publication
HBN 10-01 January 2020 41
Anaesthetic Room 1072
3.38 Dedicated anaesthetic rooms are often provided in the UK, however elsewhere 1073 in the world the patient is often anaesthetised within the operating theatre. The 1074 requirement for dedicated anaesthetic rooms will be a project decision. 1075
3.39 Initial clinical procedures, for example monitoring and the insertion of 1076 intravenous infusions, will commence in the anaesthetic room. 1077
3.40 In most circumstances a patient will be transferred to the anaesthetic room from 1078 either the in-patient ward or the admissions lounge accompanied by a nurse 1079
escort, parent or carer. 1080
3.41 It is essential to be able to access the patient from all sides. 1081
3.42 Privacy, and the maintenance of an undisturbed environment, is of great 1082 importance. 1083
3.43 The recommended size for an anaesthetic room is 19m2. 1084
The space will be used by: 1085
The patient; 1086
Up to two staff, including: 1087
o Anaesthetist & assistant; 1088
1 other (i.e. Patient escort). 1089
Activities: 1090
Anaesthetic accessories 1091
and equipment are stored. 1092
Controlled and scheduled 1093
drugs are stored securely. 1094
Holding/storing sterile 1095
equipment. 1096
Holding/storing stock of 1097
infusion fluids. 1098
Refrigerated storage of 1099
drugs/medicines. 1100
Operating lists may be 1101
displayed. 1102
Recording patient 1103
data/notes. 1104
Collecting used anaesthetic 1105
accessories for 1106
reprocessing. 1107
Collecting waste materials 1108
for disposal. 1109
Clinical wash-hand basin 1110
will be used. 1111
Administration of 1112
intravenous analgesia 1113
Administration of general 1114
anaesthesia 1115
Maintenance of general 1116
anaesthesia. 1117
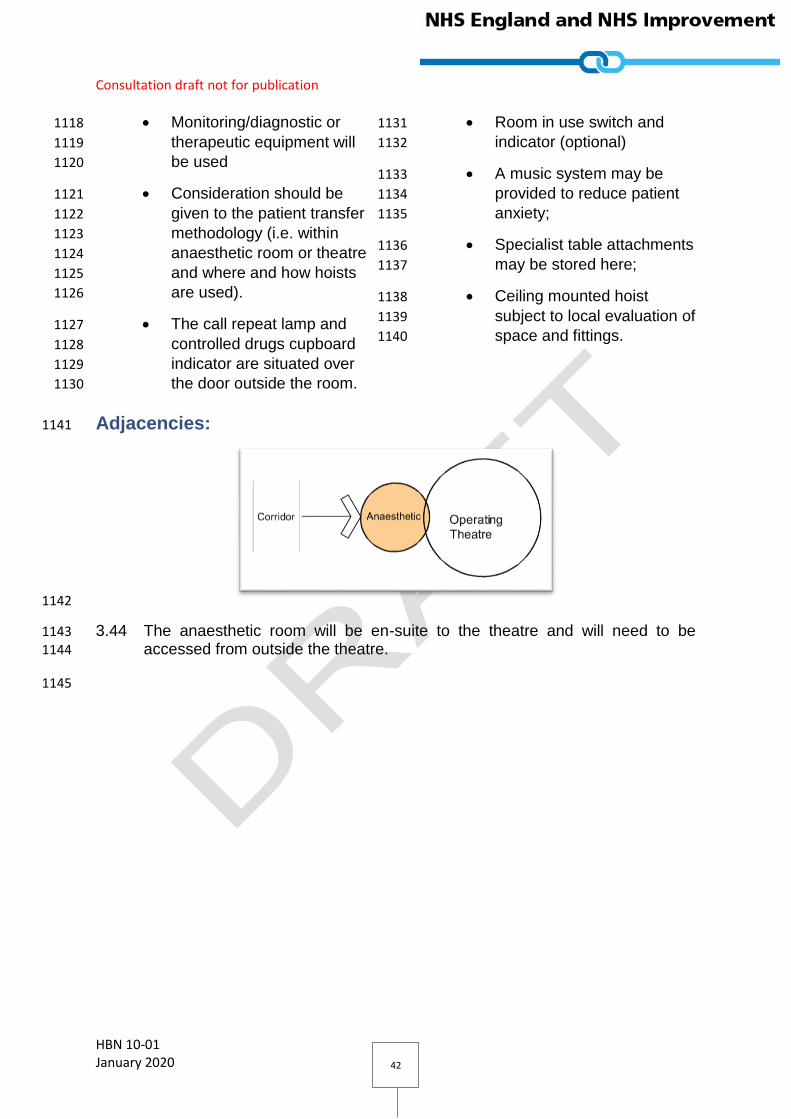
Consultation draft not for publication
HBN 10-01 January 2020 42
Monitoring/diagnostic or 1118
therapeutic equipment will 1119
be used 1120
Consideration should be 1121
given to the patient transfer 1122
methodology (i.e. within 1123
anaesthetic room or theatre 1124
and where and how hoists 1125
are used). 1126
The call repeat lamp and 1127
controlled drugs cupboard 1128
indicator are situated over 1129
the door outside the room. 1130
Room in use switch and 1131
indicator (optional) 1132
A music system may be 1133
provided to reduce patient 1134
anxiety; 1135
Specialist table attachments 1136
may be stored here; 1137
Ceiling mounted hoist 1138
subject to local evaluation of 1139
space and fittings. 1140
Adjacencies: 1141
1142
3.44 The anaesthetic room will be en-suite to the theatre and will need to be 1143
accessed from outside the theatre. 1144
1145
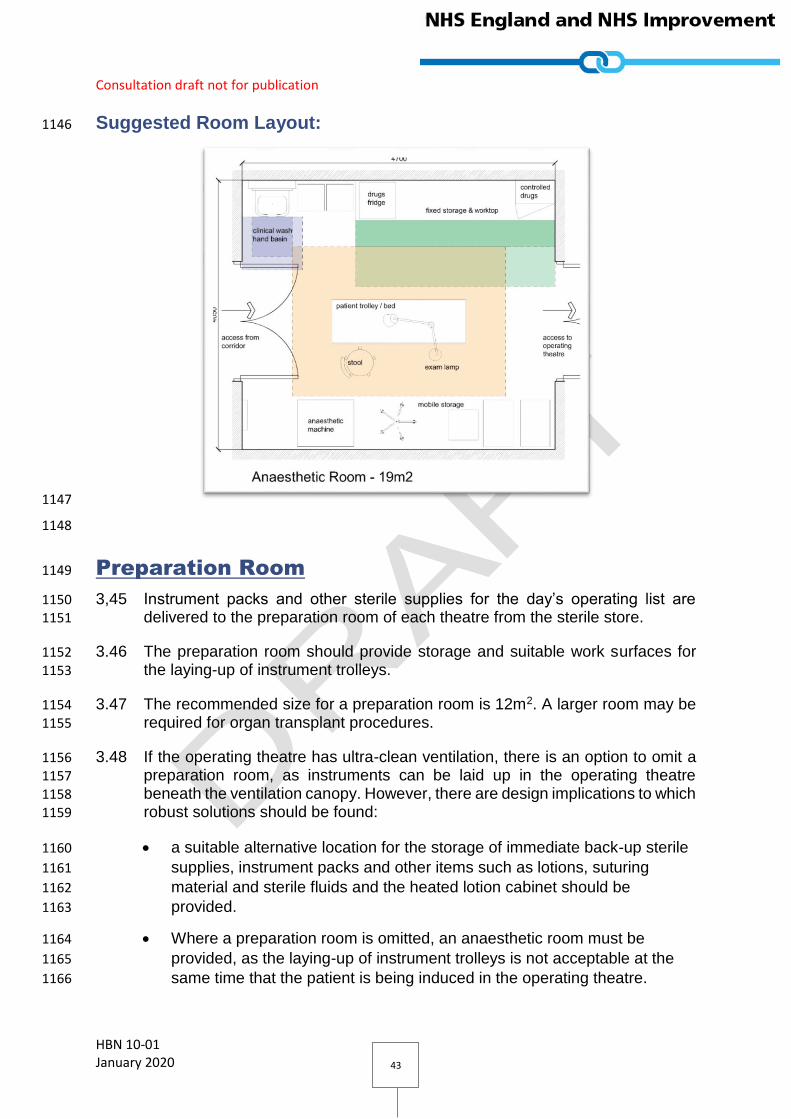
Consultation draft not for publication
HBN 10-01 January 2020 43
Suggested Room Layout: 1146
1147
1148
Preparation Room 1149
3,45 Instrument packs and other sterile supplies for the day’s operating list are 1150 delivered to the preparation room of each theatre from the sterile store. 1151
3.46 The preparation room should provide storage and suitable work surfaces for 1152
the laying-up of instrument trolleys. 1153
3.47 The recommended size for a preparation room is 12m2. A larger room may be 1154 required for organ transplant procedures. 1155
3.48 If the operating theatre has ultra-clean ventilation, there is an option to omit a 1156 preparation room, as instruments can be laid up in the operating theatre 1157 beneath the ventilation canopy. However, there are design implications to which 1158 robust solutions should be found: 1159
a suitable alternative location for the storage of immediate back-up sterile 1160
supplies, instrument packs and other items such as lotions, suturing 1161
material and sterile fluids and the heated lotion cabinet should be 1162
provided. 1163
Where a preparation room is omitted, an anaesthetic room must be 1164
provided, as the laying-up of instrument trolleys is not acceptable at the 1165
same time that the patient is being induced in the operating theatre. 1166

Consultation draft not for publication
HBN 10-01 January 2020 44
The space will be used by: 1167
A minimum of two members of staff. 1168
Activities: 1169
Instrument trollies and 1170
equipment are stored. 1171
Temporarily holding/storing 1172
sterile equipment and 1173
consumables sufficient for 1174
the operating list planned 1175
A small supply of common 1176
consumables to be stored 1177
(e.g. sutures and dressing 1178
materials). 1179
A heated lotion cabinet is 1180
sited in this room. 1181
Holding/storing stock of 1182
warmed irrigation fluids. 1183
Operating lists may be 1184
displayed. 1185
Sterile instrument trolleys 1186
for the operation procedure 1187
at hand will be prepared by 1188
a scrubbed instrument 1189
technician/nurse with the 1190
assistance of at least one 1191
circulating nurse. 1192
Prepared instrument trolleys 1193
will be transferred into 1194
theatre at the appropriate 1195
time without contaminating 1196
the instruments or drapes. 1197
Collecting waste materials 1198
for disposal. 1199
Separate data and voice 1200
outlets may be used where 1201
structured cabling solutions 1202
are not available1203
1204
Adjacencies: 1205
1206
3.49 The preparation room will be en-suite to the theatre and will need to be 1207
accessed from outside the theatre to allow for the delivery of clean supplies. 1208

Consultation draft not for publication
HBN 10-01 January 2020 45
Suggested Room Layout: 1209
1210
Scrub up & Gowning 1211
3.50 The scrub up and gowning area is used by surgical staff to scrub their hands 1212
and arms before surgery, and to put on their surgical gown (assisted by a 1213 circulating nurse). In some instances, the scrub nurse will gown and glove the 1214
surgeon and surgical assistants). 1215
3.51 The recommended size for a scrub room is 9.5m2 to allow for 3 people to use 1216 the scrub sink. A project option is to instead provide a recessed scrub bay within 1217 the theatre. 1218
3.52 One scrub and gowning room can be shared between two operating theatres, 1219 both of which should be directly accessible with sufficient space for six people, 1220
with three people scrubbing back to back. In this situation, the mechanical 1221 engineer should be consulted, as it will have an impact on the air pressure 1222 regime. 1223
The space will be used by: 1224
Up to three surgical staff (six in a shared room); 1225
Scrub/circulating nurse. 1226
Activities: 1227

Consultation draft not for publication
HBN 10-01 January 2020 46
Staff will scrub for the 1228
appropriate period at a 1229
suitable trough 1230
Staff will be able to view a 1231
clock to time their scrub 1232
Provision of medicated 1233
scrub solution and medical 1234
hand sanitizer is made to 1235
suit the number of people 1236
scrubbing 1237
Provision of sterile 1238
scrubbing brushes 1239
Provision of paper towels 1240
Sterile Gown Packs are 1241
stored away from the area 1242
of possible splash-back 1243
A selection of different sizes 1244
of Sterile Gloves is stored 1245
away from the possible area 1246
of splash-back (potentially 1247
in a purpose built glove 1248
dispenser container. 1249
A gowning trolley for 1250
opening sterile packs is 1251
located at a safe distance 1252
from the trough 1253
Used paper towels and 1254
opened gown packaging is 1255
discarded into appropriately 1256
sized waste bins. 1257
A circulating nurse is 1258
available to tie gowns for 1259
the scrubbed personnel 1260
Project option to configure 1261
this as a six-person room 1262
serving two theatres 1263
Adjacencies: 1264
3.53 The scrub room will be en-suite to the theatre and will need to be accessed 1265 from outside the theatre. 1266
1267
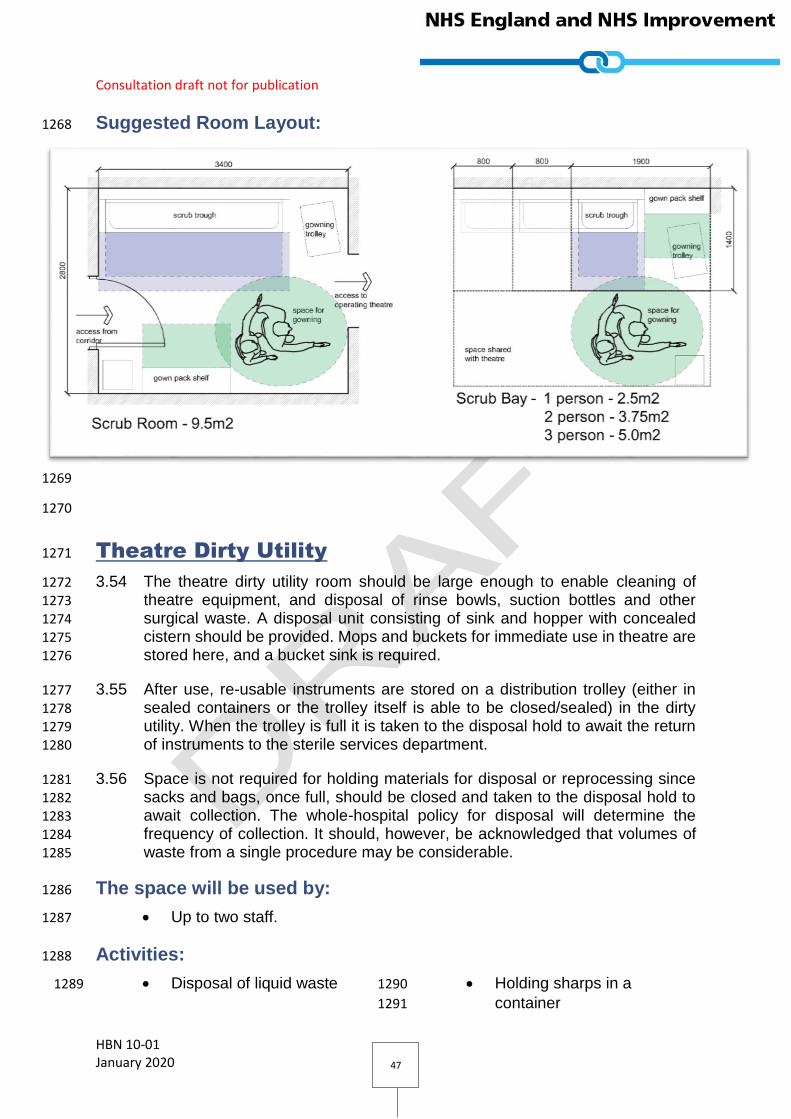
Consultation draft not for publication
HBN 10-01 January 2020 47
Suggested Room Layout: 1268
1269
1270
Theatre Dirty Utility 1271
3.54 The theatre dirty utility room should be large enough to enable cleaning of 1272
theatre equipment, and disposal of rinse bowls, suction bottles and other 1273 surgical waste. A disposal unit consisting of sink and hopper with concealed 1274 cistern should be provided. Mops and buckets for immediate use in theatre are 1275
stored here, and a bucket sink is required. 1276
3.55 After use, re-usable instruments are stored on a distribution trolley (either in 1277 sealed containers or the trolley itself is able to be closed/sealed) in the dirty 1278 utility. When the trolley is full it is taken to the disposal hold to await the return 1279
of instruments to the sterile services department. 1280
3.56 Space is not required for holding materials for disposal or reprocessing since 1281 sacks and bags, once full, should be closed and taken to the disposal hold to 1282 await collection. The whole-hospital policy for disposal will determine the 1283
frequency of collection. It should, however, be acknowledged that volumes of 1284 waste from a single procedure may be considerable. 1285
The space will be used by: 1286
Up to two staff. 1287
Activities: 1288
Disposal of liquid waste 1289 Holding sharps in a 1290
container 1291
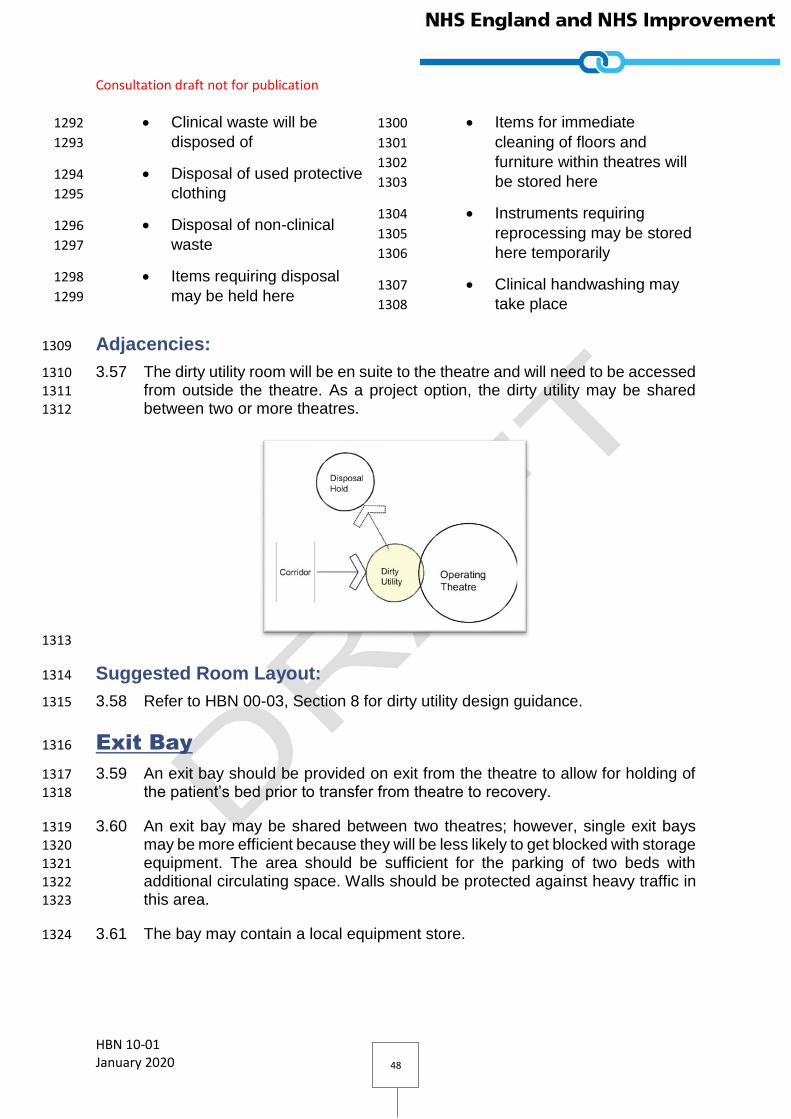
Consultation draft not for publication
HBN 10-01 January 2020 48
Clinical waste will be 1292
disposed of 1293
Disposal of used protective 1294
clothing 1295
Disposal of non-clinical 1296
waste 1297
Items requiring disposal 1298
may be held here 1299
Items for immediate 1300
cleaning of floors and 1301
furniture within theatres will 1302
be stored here 1303
Instruments requiring 1304
reprocessing may be stored 1305
here temporarily 1306
Clinical handwashing may 1307
take place 1308
Adjacencies: 1309
3.57 The dirty utility room will be en suite to the theatre and will need to be accessed 1310 from outside the theatre. As a project option, the dirty utility may be shared 1311 between two or more theatres. 1312
1313
Suggested Room Layout: 1314
3.58 Refer to HBN 00-03, Section 8 for dirty utility design guidance. 1315
Exit Bay 1316
3.59 An exit bay should be provided on exit from the theatre to allow for holding of 1317 the patient’s bed prior to transfer from theatre to recovery. 1318
3.60 An exit bay may be shared between two theatres; however, single exit bays 1319 may be more efficient because they will be less likely to get blocked with storage 1320 equipment. The area should be sufficient for the parking of two beds with 1321 additional circulating space. Walls should be protected against heavy traffic in 1322 this area. 1323
3.61 The bay may contain a local equipment store. 1324
Consultation draft not for publication
HBN 10-01 January 2020 49
Alternative Theatre Suite Model 1325
3.62 For large operating departments, the amount of space required for en-suite 1326 ancillary rooms can be significant, with large cost implications. 1327
3.63 An alternative model is one that eliminates the need for individual rooms by 1328 treating the department as a whole. This has been employed to great success 1329 at Erasmus Medical Centre in Rotterdam. Each theatre still has an en-suite 1330
preparation room and exit bay, but that is the extent of the en-suite provision. 1331
3.64 [DN: Erasmus layout to follow] 1332
3.65 This model provides a significant saving in floor area requirements and, 1333 therefore, capital costs. 1334
General Department Arrangement: 1335
3.66 [DN: diagrams to follow] 1336
Sedation within the theatre: 1337
3.67 The use of separate anaesthetic rooms is used widely in the UK but is less 1338
common elsewhere in the World. It is common practice in the US and some 1339 European countries to exclude the traditional anaesthetic room from the 1340
operating department layout. 1341
3.68 Patients are prepared for their operation in the operating theatre, avoiding the 1342 need for dedicated anaesthetic rooms, and the duplication of anaesthetic 1343
equipment. 1344
3.69 The omission of dedicated anaesthetic rooms should be treated as a radical 1345
departure from common UK practice, and should only be considered with the 1346 full support and participation of the clinical team. 1347
3.70 Dedicated anaesthetic rooms should always be provided to operating theatres 1348 that are used for children, as it provides a much calmer environment than the 1349
theatre itself and allows for parents to accompany their children prior to 1350 sedation. 1351
Scrub on entry to the department: 1352
3.71 In this model, scrub facilities are provided at the point of entry to the department 1353
for staff, ideally close to staff welfare facilities. Staff scrub at the start of their 1354 shift, with the whole department past the scrub point being treated as clean. 1355
Dirty items bagged and taken to disposal hold: 1356
3.72 To omit the need for a dedicated dirty utility, items must be bagged and taken 1357
to the disposal hold immediately after surgery. Capacity and management of 1358 the disposal hold will need to be considered. 1359

Consultation draft not for publication
HBN 10-01 January 2020 50
Disposal Hold 1360
3.73 In an operating department a considerable quantity of material for disposal is 1361 generated, and a central disposal hold is required. Bagged refuse, clinical 1362 waste, soiled linen and materials for recycling are held here safely and securely 1363 while awaiting collection. This lockable room should be accessible from the 1364 hospital street. Collections may then be made without the need to enter into the 1365
main circulation space. 1366
3.74 Full “sharps” containers from the anaesthetic rooms, operating theatres and 1367 recovery unit will also be stored in the disposal hold. 1368
3.75 Project teams should also refer to the DHSC current decontamination policy to 1369 ensure that medical devices are stored and reprocessed or disposed of in a 1370 safe manner. 1371
3.76 Instruments that have been used on a possible CJD or vCJD patient should not 1372
be re-used but may be quarantined by securely storing in a rigid sealed 1373 container after use, until the diagnosis is confirmed. For further guidance see 1374
‘Advisory Committee on Dangerous Pathogens Spongiform Encephalopathy: 1375 Transmissible spongiform encephalopathy agents: safe working and the 1376
prevention of infection’ (DH, 2003). 1377
3.77 Other distribution trolleys will be stored in the hold while awaiting collection by 1378
the SSD. These trolleys can be extremely large (1500 mm x 750 mm). When 1379 planning the size of the hold, the approximate number of trolleys to be stored 1380
following an operating session and frequency of collection should be taken into 1381 consideration. 1382
1383
Suggested Room Layout: 1384
3.78 Refer to HBN 00-03, Section 9 for disposal hold design guidance. 1385
1386
Consultation draft not for publication
HBN 10-01 January 2020 51
Storage 1387
3.80 It cannot be overstated how important it is to ensure that theatre departments 1388 have the correct allowance for storage. Theatres need ready access to a large 1389 amount of equipment and consumables. 1390
3.81 The type of storage to be considered includes: 1391
Bulk Store: 1392
3.82 Packaged instrument trays and supplies are delivered from the SSD on a daily 1393
basis. Additional sterile instruments and equipment are also kept in this room. 1394 Bench-top sterilizers should not be installed, as the protocols are difficult and 1395 time-consuming to complete. Adequate instruments and an agreed turnaround 1396 time for these will obviate the need for benchtop sterilizers and reprocessing of 1397
instruments in clinical areas. 1398
3.83 Non-sterile items are also stored here. 1399
3.84 See HFN 29 – ‘Materials management (supply, storage and distribution) in 1400 healthcare facilities’ and HTM 71 – ‘Materials management modular storage’ 1401
for further details. 1402
Clinical Equipment Store: 1403
3.85 Floor space within this store is needed for a variety of equipment including drip 1404 stands, monitoring equipment, ultrasound machines and haemodialysis 1405
equipment. Where possible, clinical equipment should be stored off the floor to 1406 help maintain a dust-free environment. Shelf space is needed for smaller items 1407
such as infusion pumps, ventilator accessories, monitoring equipment and 1408 suction apparatus. Electrical socket-outlets are required for charging 1409 equipment. Under-provision of storage for equipment may lead to unused 1410 equipment being kept in patient areas. This store should be located within easy 1411
access of the recovery unit and adjacent to the equipment service room. 1412
8.86 There is also a need for storage of operating table accessories such as arm 1413
boards (for the anaesthetist or surgeon), lithotomy poles (where required) head 1414 rests (for ENT. Ophthalmology and neurosurgery) and in some instances for a 1415 specialist operating table (for orthopaedics or neurosurgery) Many table 1416 accessories are stored on a purpose provided mobile frame, some hospitals 1417 incorporate a small storage room at the main doors to theatres off the exit bay 1418
specifically for this purpose. 1419
Linen Store: 1420
3.87 Storage is required for clean linen supplies, either in a linen store or on a linen 1421 exchange trolley. The amount of linen storage required depends on the linen 1422
supplies policy, the number of deliveries per day and the number of patients. 1423

Consultation draft not for publication
HBN 10-01 January 2020 52
Ready-use Store: 1424
3.88 A dedicated, easily accessible store for gas cylinders is required for the 1425 operating theatre. It should conform with the requirements of HTM 2022 – 1426
‘Medical gas pipeline systems’. 1427
Blood Storage: 1428
3.89 At least one blood storage refrigerator is required in the operating department. 1429 This should be located within easy access from operating theatres and the 1430 recovery unit. Personnel from the transfusion laboratories require easy access 1431 for supply and top-up purposes. 1432
3.90 Larger departments may prefer to have two blood refrigerators, one of which 1433 could be located in the recovery unit. 1434
3.91 The refrigerator should be wired in with central alarms and, possibly, barcode 1435
locks. 1436
3.92 Use of these refrigerators is governed by national and local blood transfusion 1437
service regulations. 1438
Storage Requirement Calculator: 1439
3.93 [DN: QUESTON FOR REVIEWERS: if we can devise a metric to help project 1440 teams decide how much storage is required, would this be useful?] 1441
1442
Recovery Unit 1443
3.94 A dedicated recovery unit is required. This should be located centrally in the 1444
operating theatre department. For a department with eight operating theatres, 1445 it is recommended that a minimum of 16 recovery beds are provided. However, 1446
the final number will depend on local knowledge of the clinical specialties and 1447
the number of patients/procedures undertaken. 1448
Suggested General Arrangement: 1449
3.95 [DN: Diagrams to follow.] 1450
3.96 The recovery suite consists of the following rooms: 1451
Recovery Room / Bays 1452
Staff Base 1453
Clean Utility 1454
Dirty Utility 1455
Consultation draft not for publication
HBN 10-01 January 2020 53
Recovery Room / Bays: 1456
3.97 Most patients are admitted to the unit for postoperative care. Understandably, 1457 many patients are disoriented when they are waking from sedation. It is 1458
therefore essential that the environment reflect a therapeutic atmosphere whilst 1459 continuing to meet the clinical requirements. Natural daylight enhances the 1460 feeling of well-being and is desirable. 1461
3.98 Hospital protocols will determine how long the patient is to remain in recovery 1462 before being discharged back to their post-operative ward or in the case of a 1463
day case patient, to the second stage recovery area. 1464
3.99 Staff will need 360º access to a patient, therefore an island solution is required 1465
in each bed space. The main overhead lighting should be dimmable. A wall 1466 mounted clock with a sweep seconds hand is required, visible from all bed 1467 spaces. 1468
3.100 For best practice and to ensure the patient’s privacy and dignity, every bed 1469
space should be separated by radiation protected partitions or curtains, with a 1470 curtain at the foot end of each bed space. 1471
3.101 25% of the recovery spaces should be single cubicles, each of which can be 1472 utilised as a normal recovery bed but is suitably equipped for caring for Critical 1473
Care patients. Further guidance on requirements for critical care bed spaces 1474 can be found in HBN 04-02. 1475
3.102 Consideration should be given to the use of hoists in the recovery unit. A 1476 number of options are available. For maximum flexibility, a hoist in every bed 1477 space is the ideal solution for new facilities or a major refurbishment. 1478
3.103 Clinical hand-wash basins are required are required at the foot of the bed 1479 spaces. A minimum of one basin between two beds is required. 1480
3.104 Refer to HBN 00-03, Section 5 for typical recovery space design guidance. 1481
Recovery Staff Base 1482
3.105 The recovery unit requires a dedicated communications base serving as a focal 1483 point and observation post within the clinical area. It should be enclosed in a 1484 glazed partition to reduce noise levels. The base will require a minimum of three 1485 telephone lines plus data access, computer facilities and white message board, 1486 and direct access to the clean and dirty utility rooms. A number of designs have 1487
been reviewed. Some units have a large, raised central station, enclosed by 1488 partition walls of wired fireproof double-glazed glass, from which all bed spaces 1489 are visible. Advantages of this arrangement are that people can have 1490 conversations on the telephone or face-to face, while limiting the noise levels 1491 in the clinical area. All incoming information from the operating theatres, via 1492
computer links, arrives at this central point. 1493
3.106 Refer to HBN 00-03, Section 12 for general staff base design guidance. 1494

Consultation draft not for publication
HBN 10-01 January 2020 54
Recovery Clean Utility 1495
3.107 The clean utility provides storage for clean disposable items and equipment. It 1496 may also accommodate: 1497
lockable controlled drugs cupboard; 1498
drugs refrigerator; 1499
warm blanket storage facility. 1500
3.108 Shelf space is needed for items of equipment such as infusion pumps, ventilator 1501
accessories, monitoring equipment and suction apparatus. Electrical socket-1502 outlets are required for charging equipment. 1503
3.109 One anaesthetic machine and a cardiac arrest trolley with defibrillator should 1504 also be located here. 1505
3.110 Refer to HBN 00-03, Section 8 for clean utility design guidance. 1506
Recovery Dirty Utility 1507
3.111 The equipment in this dirty utility room will be identical to that described in the 1508
theatre dirty utility room (described in section X of this document) with the 1509
exception that if disposable bedpans, vomit bowls etc are used, a macerator is 1510
required. If re-usable bedpans etc are used, a steam washer/sterilizer is 1511 necessary. 1512
3.112 Refer to HBN 00-03, Section 8 for dirty utility design guidance. 1513
Staff Accommodation 1514
3.113 [DN: QUESTION FOR REVIEWERS: are there any HBN 10-01-specific 1515 requirements for staff accommodation that should be included here?] 1516
[DN: See HBNs XX] 1517
Rest Facilities: 1518
Beverage Bay: 1519
Changing Facilities: 1520
Offices: 1521
1522
Hybrid Operating Theatres 1523
3.114 Dedicated medical imaging rooms can be located within the Operating 1524 department as part of the theatre suite. 1525
Consultation draft not for publication
HBN 10-01 January 2020 55
3.115 Two models for the use of these imaging rooms are available. Either the theatre 1526 itself is equipped with imaging equipment that is moved via tracks to the patient 1527 within the operating room, or the patient is moved to an adjacent imaging room. 1528 In both cases the option of accessing the imaging room at other times, e.g. for 1529 use by intensive care patients is desirable so the location within the complex 1530
may need to consider this requirement. In either case, there will be a 1531 requirement for a control room. 1532
The space will be used by: 1533
The Patient; 1534
Up to 8 staff, including: 1535
o Surgical team & assisting staff; 1536
o Radiology team; 1537
o Anaesthetist & assisting staff; 1538
o Circulating support staff. 1539
Activities: 1540
Patient may be connected 1541
to anaesthetic machine. 1542
Maintenance of general 1543
anaesthesia 1544
Monitoring/diagnostic or 1545
therapeutic equipment may 1546
be used. 1547
Assembling and connecting 1548
mobile equipment. 1549
Surgical instruments on 1550
instrument trolley may be 1551
used. 1552
Surgical procedures may be 1553
performed under local or 1554
general anaesthetic. 1555
Patient undergoes 1556
interventional diagnostic 1557
procedures 1558
Computer generated 1559
images are viewed using 1560
ceiling or wall mounted 1561
screens. 1562
Used swabs may be 1563
checked, weighed and 1564
recorded. 1565
Operating lists may be 1566
displayed. 1567
Recording patient 1568
data/notes. 1569
Electronic patient records 1570
(EPRs) may be accessed 1571
and updated. 1572
Patient is transferred from 1573
operating table to 1574
bed/trolley. 1575
Storage of small items of 1576
equipment or consumables 1577
as required 1578
"IN USE" sign sited outside 1579
the doorway of the room. 1580
Contrast media may be 1581
administered. 1582
Disposal of waste. 1583
1584
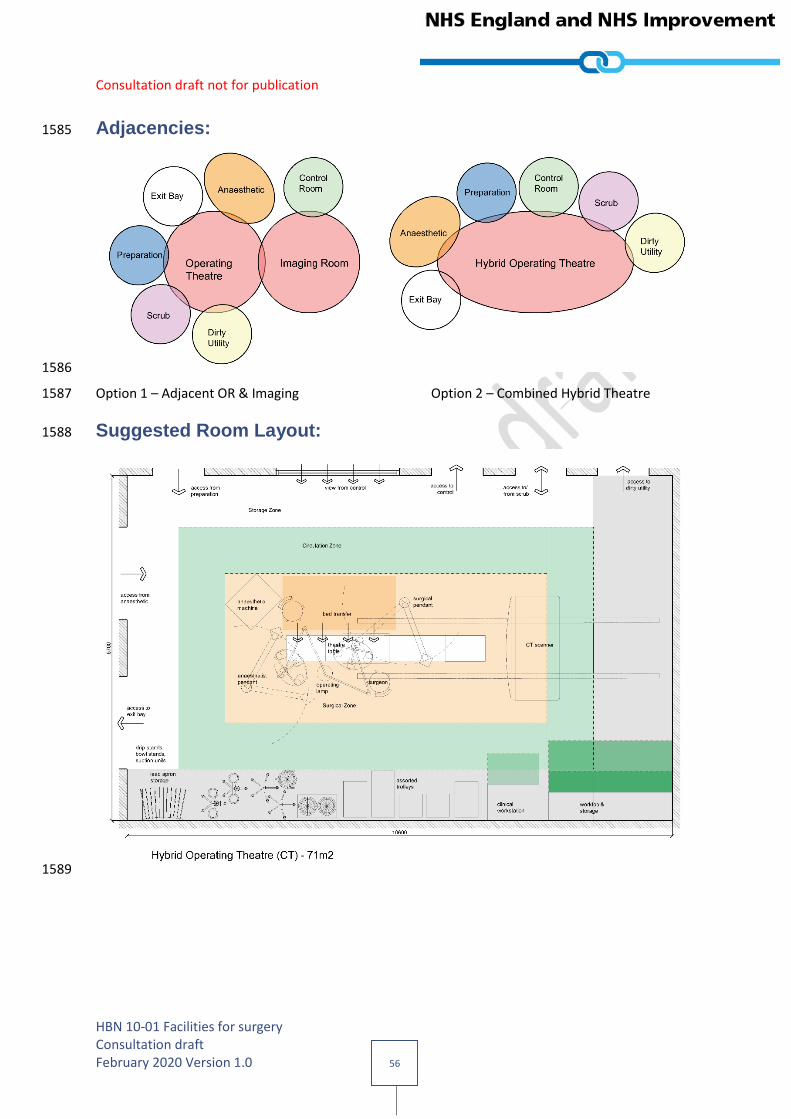
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 56
Adjacencies: 1585
1586
Option 1 – Adjacent OR & Imaging Option 2 – Combined Hybrid Theatre 1587
Suggested Room Layout: 1588
1589

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 57
1590
Support/utility 1591
Storage 1592
3.116 [DN: Consider provision and storage of ultrasound machine - an ultrasound 1593 machine is a good diagnostic tool; it can be used at the patient’s side (therefore 1594
not having to move the patient). It depends on demand and sharing with ED. 1595 Which option is more efficient and less costly?] 1596
3.117 [DN: Would need a small storage room for bulk stores (e.g. IV fluids/oxygen 1597 tubing/masks etc.) Medium size? 1598
3.118 This will depend on supply and delivery and FM frequency of delivery. With 1599 clever design, these could be stored within Gratnell-type trolleys. It will vary with 1600
demand. Site visits will possibly show how they solve the supply issues.] 1601
3.119 [DN: mention medicines storage – cross-reference the new HBN 14-02.] 1602
3.120 [DN: Other storage requirements? May need to use carts as much as possible, 1603 and have a top-up system. FM-dependent, e.g linen.] 1604
Dirty utility 1605
3.121 [DN: Provision of small dirty utility with bedpan washer/macerator.] 1606

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 58
4.0 Engineering requirements 1607
Introduction 1608
4.1 This section sets out the engineering services recommendations for the 1609
specialist day surgery rooms contained within the department. 1610
4.2 It does not cover any areas outside of the rooms or infrastructure. Reference 1611 should be made to the associated HTM’s to which the designer must be familiar 1612 with. 1613
4.3 This guidance will inform the designers with the criteria and materials 1614 specification needed to meet the functional requirements. Specific 1615 requirements should be formulated in discussion with both end-users, such as 1616
clinicians as well as electrical and water safety groups and manufacturers of 1617 specialist equipment. Some issues particularly those related to the use of lasers 1618 will require specific and detailed discussion with other professional consultants. 1619
4.4 Where lasers are to be used, safety precautions in accordance with the relevant 1620
standards should be employed, including the provision of warning lights, door 1621 interlocks and pressure stabiliser shielding. 1622
Environmental requirements 1623
4.5 An increasing number of patients undergo surgery without a general 1624 anaesthetic and hence remain aware of their surroundings, even in theatres. 1625
4.6 Designers should aim to create an environment that is conducive to making 1626 patients feel at ease and giving them confidence, thus aiding the healing 1627 process. At the same time, it should facilitate efficient working and contribute to 1628 positive staff morale. 1629
4.7 Detailed environmental requirements for specialist equipment should be 1630
obtained from the manufacturers for the specific equipment to be installed. The 1631
comfort of patients and staff are an essential consideration in respect of 1632 temperature stability. Humidity and temperature control will frequently be a key 1633 feature of successful design. 1634
4.8 Centralised cooling and air conditioning units should be considered in 1635 preference to local stand-alone units. 1636
4.9 Recommended minimum environmental criteria is identified under each specific 1637 room type that follow. 1638
Energy 1639
4.10 Metering of all major plant and equipment serving the rooms should be in 1640 accordance with CIBSE recommendations and reflect Building Regulations 1641
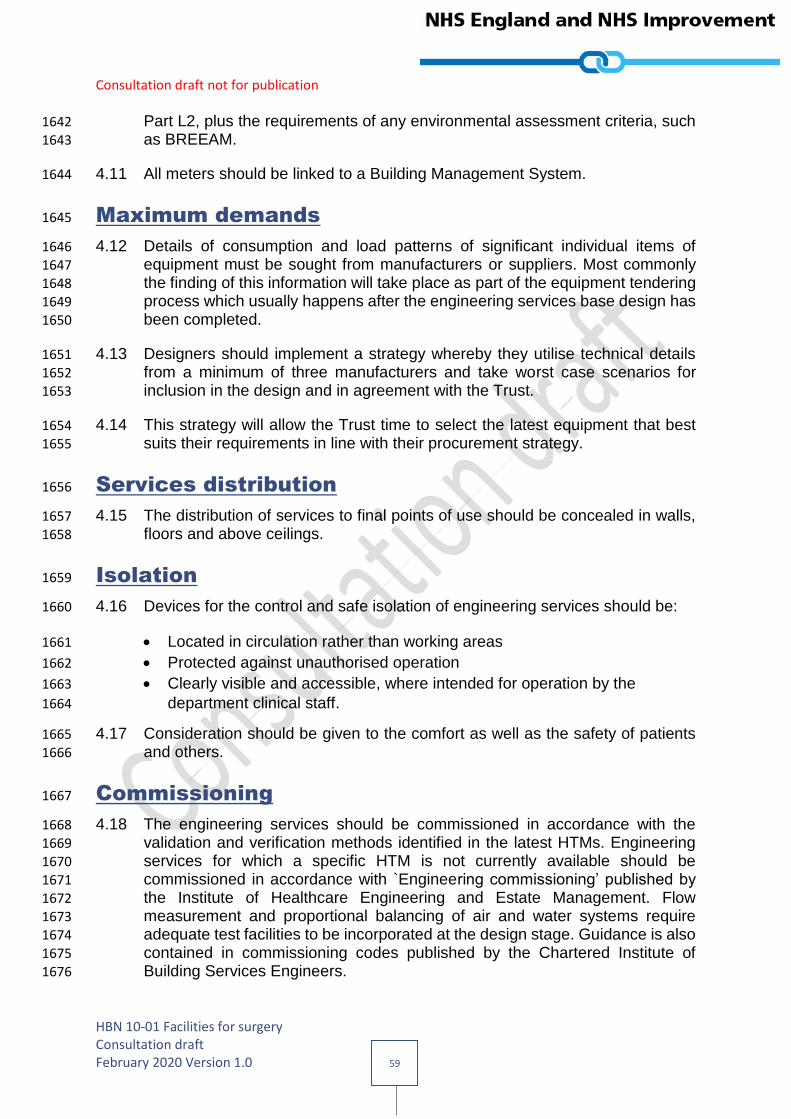
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 59
Part L2, plus the requirements of any environmental assessment criteria, such 1642 as BREEAM. 1643
4.11 All meters should be linked to a Building Management System. 1644
Maximum demands 1645
4.12 Details of consumption and load patterns of significant individual items of 1646 equipment must be sought from manufacturers or suppliers. Most commonly 1647
the finding of this information will take place as part of the equipment tendering 1648 process which usually happens after the engineering services base design has 1649
been completed. 1650
4.13 Designers should implement a strategy whereby they utilise technical details 1651 from a minimum of three manufacturers and take worst case scenarios for 1652 inclusion in the design and in agreement with the Trust. 1653
4.14 This strategy will allow the Trust time to select the latest equipment that best 1654
suits their requirements in line with their procurement strategy. 1655
Services distribution 1656
4.15 The distribution of services to final points of use should be concealed in walls, 1657
floors and above ceilings. 1658
Isolation 1659
4.16 Devices for the control and safe isolation of engineering services should be: 1660
Located in circulation rather than working areas 1661
Protected against unauthorised operation 1662
Clearly visible and accessible, where intended for operation by the 1663
department clinical staff. 1664
4.17 Consideration should be given to the comfort as well as the safety of patients 1665 and others. 1666
Commissioning 1667
4.18 The engineering services should be commissioned in accordance with the 1668 validation and verification methods identified in the latest HTMs. Engineering 1669 services for which a specific HTM is not currently available should be 1670 commissioned in accordance with `Engineering commissioning’ published by 1671
the Institute of Healthcare Engineering and Estate Management. Flow 1672 measurement and proportional balancing of air and water systems require 1673 adequate test facilities to be incorporated at the design stage. Guidance is also 1674
contained in commissioning codes published by the Chartered Institute of 1675 Building Services Engineers. 1676

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 60
4.19 The services for some diagnostic imaging equipment may need to be 1677 commissioned before the final completion of the engineering contract 1678 programme, to allow the imaging equipment commissioning to be completed 1679 prior to the first patient. Parts of this commissioning are concerned with 1680 radiation safety and the approval of the RPA must be obtained for the imaging 1681
processes and schedules proposed. 1682
The operating theatre 1683
4.20 A control panel to accommodate environmental controls, alarms and 1684 instrumentation, clocks, medical viewing screens, door locks and lighting 1685
controls should be provided. 1686
4.21 The control panel should be fully recessed and ideally accessed for 1687 maintenance outside of the theatre itself. 1688
Mechanical services 1689
Environmental criteria 1690
4.22 The environmental criteria should be in accordance with HTM 03-01. 1691
Ventilation 1692
4.23 The ventilation central system should be designed in accordance with HTM 03-1693
01 including design of air-movement control schemes for operating theatres. 1694
Heating 1695
4.24 The heating distribution system should be designed in accordance with HTM 1696 03-01. 1697
4.25 The heating provision in the operating suite should be achieved via the 1698 ventilation system. 1699
4.26 A low temperature all air system is to be provided with duct mounted heater 1700 batteries. The batteries should be located in the ceiling void, ideally in corridors 1701 or ancillary rooms, to ensure they are fully accessible. 1702
Cooling 1703
4.27 The cooling distribution system should be designed in accordance with HTM 1704 03-01. 1705
4.28 The cooling provision in the operating suite should be achieved via the 1706
ventilation system. 1707
4.29 As a low temperature all air system is provided, the main cooling coils on the 1708 air handling units should be utilised. The heater batteries should be utilised to 1709 adjust the room temperatures to meet individual user requirements. 1710

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 61
Medical gas 1711
4.30 Medical gas services should be designed in accordance with HTM 02-01. Outlet 1712 quantities identified should form the starting point for discussions with the users 1713 and inclusion in project room data sheets. 1714
Domestic water services 1715
4.31 Domestic water services should be designed in accordance with HTM 04-01 1716 and agreed with the Water Safety Group. 1717
Humidification 1718
4.32 Humidification is not a general requirement of HTM 03-01. 1719
Building Management System 1720
4.33 The operating suite should be connected to the central BMS network. 1721
4.34 Each room should be provided with wall mounted temperature controllers to 1722 enable user control within the temperature parameters set out 2.1.1 above 1723
Electrical services 1724
Electrical power distribution 1725
4.35 The primary objective is to deliver designs that are both safe for staff, patient 1726
and visitors and available when they need to use it. HTM 06-01 provides 1727
excellent guidance on electrical distribution within a healthcare estate, 1728
addressing both of these issues and forms the basis upon which design 1729 proposals should be assessed. 1730
4.36 As required by HTM 06-01, these recommendations need to be considered, 1731 reviewed and expanded upon in conjunction with the Trust Electrical Safety 1732 Group (ESG), to finalise the brief and include but not limited to the following: 1733
Normal electrical supplies (dual path) 1734
Emergency electrical supplies 1735
Electrical interference 1736
Uninterruptable supply units (UPS) 1737
Isolated power supplies (IPS) 1738
4.37 Risk is addressed from two different viewpoints, the effect on the patient 1739 (clinical risk, life safety) and continuity of service (business continuity), i.e. whilst 1740
a patient may be safe the loss of a facility such as IT servers over a prolonged 1741 period will prevent the functioning of the hospital. 1742
4.38 The designer should lead this process in terms of clinical risk, obtaining 1743 guidance from the Trust in terms of business continuity. 1744
4.39 For operating theatres, a minimum of clinical risk A should be adopted for all 1745
patient zones and clinical risk B to all other areas. 1746
4.40 Electrical supply connections to all medical electrical equipment should comply 1747
with BS 7671 and associated guidance notes. 1748

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 62
4.41 Designers must ensure that the electrical loads are balanced across the infra 1749 structure network and that there is sufficient capacity to meet current and 1750 potential future demands. 1751
4.42 Where laminar flow hoods are provided, dual supplies to each controller should 1752 be considered. 1753
Lighting 1754
4.43 Natural light is of particular importance to the well-being of patients and staff. 1755 All surgical facilities, where possible, should have natural daylight directly from 1756 windows, or by means of borrowed light. Where natural light is not available 1757
through conventional means, consideration should be given to technologies 1758 such as artificial skylights etc. 1759
4.44 Artificial lighting should be provided to supplement as required, and achieve the 1760 desired light levels and environment conditions whilst considering energy 1761
consumption. Its positioning should be carefully considered. 1762
4.45 Where this is the case, proposals should reflect the guidance set out in CIBSE 1763 Lighting guides with particular reference to LG2 ‘Hospitals and Healthcare 1764
Buildings’. 1765
4.46 At each entrance of the theatre, a safety sign and warning lamp must be 1766
provided in order to warn people that they are entering a controlled area and to 1767 comply with the statutory requirements. 1768
4.47 The warning lamp must provide clear indication in red when it is energised and 1769 may incorporate the legend ‘Do Not Enter’, visible only when illuminated. ‘Laser 1770 in Use’ signs should also be provided where equipment is present. 1771
4.48 Signs should be switched by the surgeon’s panel or appropriate devices 1772 interlocked with the operation of the equipment and operating suite doors. 1773
Call systems 1774
4.49 Addressable call systems should be designed in accordance with HTM 08-01. 1775
Outlet quantities identified should form the starting point for discussions with 1776
the users and should be included in project room data sheets. 1777
Security 1778
4.50 Local security policies should determine at the planning stage the level of 1779
security to be provided. 1780
4.51 Closed circuit television (CCTV) should be provided, where required, in 1781 consultation with the users, to monitor patients undergoing treatment in 1782 restricted areas and where left unattended. The interference to which such 1783 equipment may be subjected should be considered when specified to ensure 1784
acceptable electromagnetic compatibility. Care should be taken in the 1785
positioning of monitors in order to preserve patient privacy. 1786
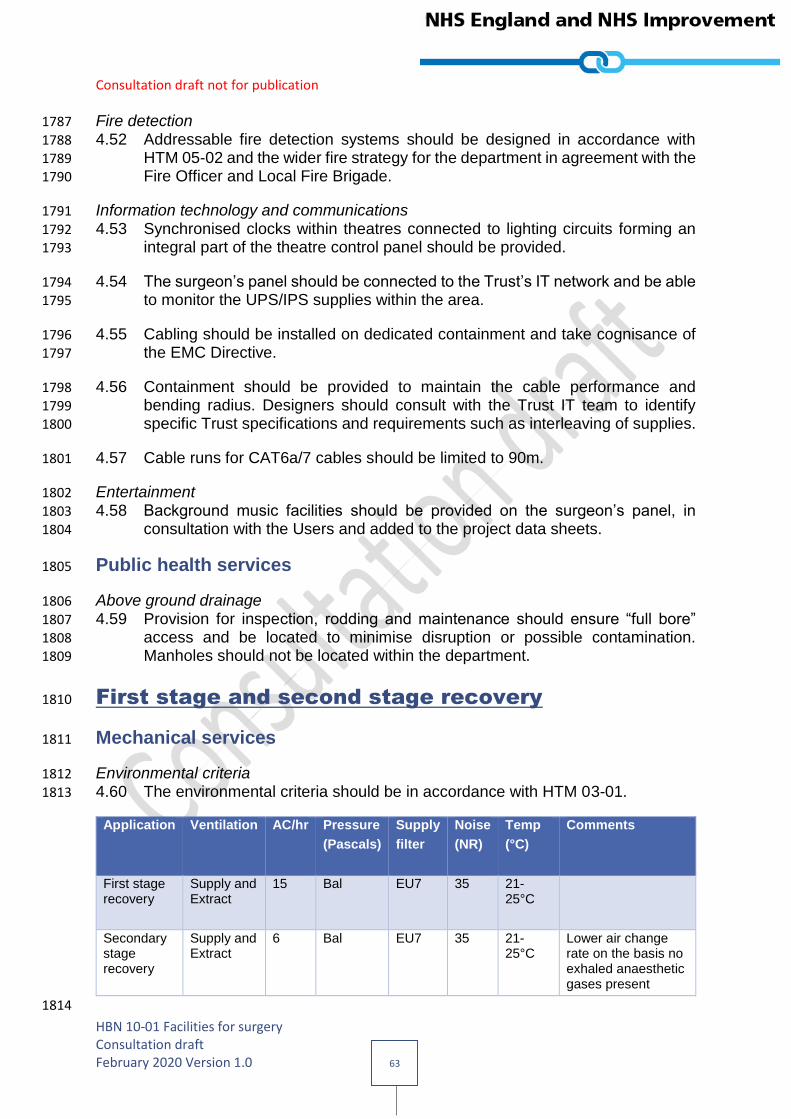
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 63
Fire detection 1787
4.52 Addressable fire detection systems should be designed in accordance with 1788 HTM 05-02 and the wider fire strategy for the department in agreement with the 1789 Fire Officer and Local Fire Brigade. 1790
Information technology and communications 1791
4.53 Synchronised clocks within theatres connected to lighting circuits forming an 1792 integral part of the theatre control panel should be provided. 1793
4.54 The surgeon’s panel should be connected to the Trust’s IT network and be able 1794 to monitor the UPS/IPS supplies within the area. 1795
4.55 Cabling should be installed on dedicated containment and take cognisance of 1796 the EMC Directive. 1797
4.56 Containment should be provided to maintain the cable performance and 1798 bending radius. Designers should consult with the Trust IT team to identify 1799
specific Trust specifications and requirements such as interleaving of supplies. 1800
4.57 Cable runs for CAT6a/7 cables should be limited to 90m. 1801
Entertainment 1802
4.58 Background music facilities should be provided on the surgeon’s panel, in 1803
consultation with the Users and added to the project data sheets. 1804
Public health services 1805
Above ground drainage 1806
4.59 Provision for inspection, rodding and maintenance should ensure “full bore” 1807 access and be located to minimise disruption or possible contamination. 1808 Manholes should not be located within the department. 1809
First stage and second stage recovery 1810
Mechanical services 1811
Environmental criteria 1812
4.60 The environmental criteria should be in accordance with HTM 03-01. 1813
Application Ventilation AC/hr Pressure
(Pascals)
Supply
filter
Noise
(NR)
Temp
(°C)
Comments
First stage recovery
Supply and Extract
15 Bal EU7 35 21-25°C
Secondary stage recovery
Supply and Extract
6 Bal EU7 35 21-25°C
Lower air change rate on the basis no exhaled anaesthetic gases present
1814
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 64
1815
Ventilation 1816
4.61 The ventilation central system should be designed in accordance with HTM 03-1817
01. 1818
Heating 1819
4.62 The heating distribution system should be designed in accordance with HTM 1820 03-01. 1821
4.63 The heating provision in the recovery room should be achieved via the 1822
ventilation system. 1823
4.64 A low temperature all air system is to be provided with duct mounted heater 1824
batteries. The batteries should be located in the ceiling void, ideally in corridors 1825 or ancillary rooms, to ensure they are fully accessible. 1826
Cooling 1827
4.65 The cooling distribution system should be designed in accordance with HTM 1828
03-01. 1829
4.66 The cooling provision in the recovery room should be achieved via the 1830
ventilation system. 1831
4.67 As a low temperature all air system is provided, the main cooling coils on the 1832
air handling units should be utilised. The heater batteries should be utilised to 1833 adjust the room temperatures to meet individual user requirements. 1834
Medical gas 1835
4.68 Medical gas services should be designed in accordance with HTM 02-01. Outlet 1836 quantities identified should form the starting point for discussions with the users 1837
and inclusion in project room data sheets. 1838
Domestic water services 1839
4.69 Domestic water services should be designed in accordance with HTM 04-01 1840
and agreed with the Water Safety Group. 1841
Humidification 1842
4.70 Humidification is not a general requirement of HTM 03-01. 1843
Building Management System 1844
4.71 All recovery rooms should be connected to the central BMS network. 1845
4.72 Each room should be provided with wall mounted temperature controllers to 1846 enable user control within the temperature parameters set out 3.1.1 above 1847

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 65
Electrical services 1848
Electrical power distribution 1849
4.73 The primary objective is to deliver designs that are both safe for staff, patient 1850
and visitors and available when they need to use it. HTM 06-01 provides 1851 excellent guidance on electrical distribution within a healthcare estate, 1852 addressing both of these issues and forms the basis upon which design 1853 proposals should be assessed. 1854
4.74 As required by HTM 06-01, these recommendations need to be considered, 1855
reviewed and expanded upon in conjunction with the Trust Electrical Safety 1856
Group (ESG), to finalise the brief and include but not limited to the following: 1857
Normal electrical supplies (dual path) 1858
Emergency electrical supplies 1859
Electrical interference 1860
Uninterruptable supply units (UPS) 1861
Isolated power supplies (IPS) 1862
4.75 Risk is addressed from two different viewpoints, the effect on the patient 1863 (clinical risk, life safety) and continuity of service (business continuity), i.e. whilst 1864 a patient may be safe the loss of a facility such as IT servers over a prolonged 1865
period will prevent the functioning of the hospital. 1866
4.76 The designer should lead this process in terms of clinical risk, obtaining 1867 guidance from the Trust in terms of business continuity. 1868
4.77 For 1st stage recovery areas a minimum of clinical risk A should be adopted, 1869
with category B for 2nd stage recovery. 1870
4.78 Electrical supply connections to all medical electrical equipment should comply 1871
with BS 7671 and associated guidance notes. 1872
4.79 Designers must ensure that the electrical loads are balanced across the infra 1873
structure network and that there is sufficient capacity to meet current and 1874
potential future demands. 1875
Lighting 1876
4.80 Natural light is of particular importance to the well-being of patients and staff. 1877
All surgical facilities, where possible, should have natural daylight directly from 1878 windows, or by means of borrowed light. Where natural light is not available 1879 through conventional means, consideration should be given to technologies 1880 such as artificial skylights etc. 1881
4.81 Artificial lighting should be provided to supplement as required, and achieve the 1882
desired light levels and environment conditions whilst considering energy 1883
consumption. Its positioning should be carefully considered. 1884
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 66
4.82 Where this is the case, proposals should reflect the guidance set out in CIBSE 1885 Lighting guides with particular reference to LG2 ‘Hospitals and Healthcare 1886 Buildings’. 1887
4.83 Clinical task lighting at each bed space is essential for the continuous clinical 1888 assessment of a patients colour and general physical status. 1889
Call systems 1890
4.84 Addressable call systems should be designed in accordance with HTM 08-01. 1891 Outlet quantities identified should form the starting point for discussions with 1892 the users and should be included in project room data sheets. 1893
Security 1894
4.85 Local security policies should determine at the planning stage the level of 1895 security to be provided. 1896
4.86 Closed circuit television (CCTV) should be provided, where required, in 1897
consultation with the users, to monitor patients undergoing treatment in 1898 restricted areas and where left unattended. The interference to which such 1899 equipment may be subjected should be considered when specified to ensure 1900
acceptable electromagnetic compatibility. Care should be taken in the 1901 positioning of monitors in order to preserve patient privacy. 1902
Fire detection 1903
4.87 Addressable fire detection systems should be designed in accordance with 1904
HTM 05-02 and the wider fire strategy for the department in agreement with the 1905 Fire Officer and Local Fire Brigade. 1906
Information technology and communications 1907
4.88 Cabling should be installed on dedicated containment and take cognisance of 1908 the EMC Directive. 1909
4.89 Containment should be provided to maintain the cable performance and 1910 bending radius. Designers should consult with the Trust IT team to identify 1911 specific Trust specifications and requirements such as interleaving of supplies. 1912
4.90 Cable runs for CAT6a/7 cables should be limited to 90m. 1913
Entertainment 1914
4.91 HTM 08-03 recommends that entertainment facilities will enhance patient well-1915
being and experience, and identifies various systems to be considered. These 1916 being: 1917
Television 1918
Internet services (Wi-Fi) 1919
Music 1920
IT and Communications (also see section above) 1921
Healthcare information 1922

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 67
4.92 It is important that designers consider the inclusion of entertainment systems 1923 from the outset within 2nd stage recovery areas in conjunction with the user’s, 1924 as integral systems are the preferred option. 1925
Public health services 1926
Above ground drainage 1927
4.93 Provision for inspection, rodding and maintenance should ensure “full bore” 1928 access and be located to minimise disruption or possible contamination. 1929 Manholes should not be located within the department. 1930
4.94 [DN: Links to the relevant HTMs will be provided.] 1931
1932
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 68
References 1933
HBNs 1934
[DN: List will be inserted (see list in introduction which will be updated for new titles to 1935 be published this year)] 1936
HTMs 1937
[DN: List will be inserted (see list in introduction which will be updated for new titles to 1938 be published this year)] 1939
Acts and Regulations 1940
[DN: list will be inserted] 1941
Standards 1942
[DN: List will be inserted] 1943
NHS national policies 1944
NHS Improvement (2017). National priorities for acute hospitals 2017 – good 1945
practice guide: focus on improving patient flow. 1946
https://improvement.nhs.uk/resources/good-practice-guide-focus-on-improving-1947 patient-flow/ 1948
NHS Improvement (2017). National priorities for acute hospitals 2017 – case studies: 1949
focus on improving patient flow. 1950
https://improvement.nhs.uk/resources/case-studies-focus-improving-patient-flow/ 1951
[DN: Additional references will be inserted] 1952
1953
Other 1954
Royal College of Physicians (2013). Future hospital: Caring for Medical Patients – a 1955 Report from the Future Hospital Commission to the Royal College of Physicians. 1956 RCP, London. 1957
[DN: Additional references will be inserted] 1958
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 69
Wider sources of healthcare planning information, 1959
tools and support 1960
NHS England & NHS Improvement’s Model Hospital Portal 1961
The Model Hospital25 is a digital information service designed to help NHS providers 1962
improve their productivity and efficiency. The Model Hospital is a web tool that can be 1963 used by anyone in the NHS from board to ward to explore and compare productivity, 1964 quality and responsiveness data to identify opportunities to improve. Model 1965 Ambulance, Model Mental Health and Model Community Health Services have also 1966
recently been developed for trusts which provide these services. Trusts can use the 1967 tools to dive deeper into their data and compare with peers to understand “what good 1968 looks like” and thus identify areas for improvement. 1969
The ProCure22 Framework 1970
The ProCure22 Framework is the recommended procurement method for publicly-1971
funded capital projects over £1 million. 1972
The Principal Supply Chain Partners (PSCPs) have developed a number of repeatable 1973
room arrangements26 for use in NHS Acute and Mental Health facilities, all of which 1974 are fully compliant with HBNs and HTMs. 1975
The P22 Training Academy has created a suite of e-modules which are freely available 1976 for use.27 1977
A number of P22 toolkits are also available (including the Clinical Design 1978 Requirements Toolkit [DN: this may be included as an appendix]. The P22 Framework 1979 encourages users to test its toolkits and provide feedback to inform continuous 1980
improvement. 1981
Miscellaneous sources including professional membership 1982
organisations 1983
DN: QUESTION FOR REVIEWERS: What organisations should we include here? The 1984
criteria for inclusion need to be defined. 1985
IHEEM
Institute of Healthcare Engineering and Estates Management
An International Professional Engineering Institute specialising in the Healthcare Estates Sector.
https://www.iheem.org.uk/
Knowledge Portal and Technical Advisory Platforms: https://www.iheem.org.uk/Knowledge-Portal
Health Estate Journal:
https://www.iheem.org.uk/Health-Estate-Journal
HefmA https://www.hefma.co.uk
Hefma Pulse magazine:
25 See https://improvement.nhs.uk/resources/model-hospital/ 26 See http://www.procure21plus.nhs.uk/repeatable_rooms/ 27 See INSERT LINK
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 70
Health Estates and Facilities Management Association
A branch-based network of Estates and Facilities Professionals working in the NHS.
https://www.hefma.co.uk/our-magazine
AfH
Architects for Health
A network of like-minded people who share ideas, experiences and best practices in healthcare design.
https://www.architectsforhealth.com/
ABHI
Association of British Healthcare Industries
The UK’s leading industry association for health technology.
https://www.abhi.org.uk/
Resource Hub:
https://www.abhi.org.uk/resource-hub/
DiMHN
Design in Mental Health Network
A not-for-profit, social enterprise company with charitable aims and is open to anyone with an interest in the design of mental health facilities.
https://www.dimhn.org/
The Network magazine:
https://www.dimhn.org/the-network/
IPS
Infection Prevention Society
Infection prevention best practice.
https://www.ips.uk.net/
Journal of Infection Prevention:
https://www.ips.uk.net/professional-practice/journal-infection-prevention-jip/#.XlMhiGj7Q2w
EuHPN
European Health Property Network
A membership of professionals from a wide range of disciplines that meets annually for a workshop.
https://euhpn.eu/
Salus
An online knowledge community dedicated to designing a healthier society.
https://www.salus.global/
EFPC
European Forum for Primary Care
The aim of the forum is to improve the health of the population by promoting strong Primary Care. This is done by advocating for Primary Care, by generating data and evidence on Primary Care and by exchanging information between its members.
http://euprimarycare.org/
The King’s Fund
Strategic priorities are to work with people in the health and care system to:
drive improvements in health and wellbeing across places and communities
https://www.kingsfund.org.uk/
Integrated care topic:
https://www.kingsfund.org.uk/topics/integrated-care
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 71
improve health and care for people with the worst health outcomes
support people and leaders working in health and care.
SCIE
Social Care Institute for Excellence
Resources, consultancy and training on integrating health, care and related services.
https://www.scie.org.uk/integrated-care
LGA
Local Government Association
Health and care systems across the country are joining up services to improve the health, wellbeing and experiences of individuals, through both national and local transformation programmes.
Integration and the Better Care Fund:
https://www.local.gov.uk/our-support/our-improvement-offer/care-and-health-improvement/integration-and-better-care-fund
BIM4Health
Building Information Modelling for Health
A community of practice to help raise awareness of BIM and build capacity and capability.
http://www.bim4health.org/bim4health/index.html
1986
1987
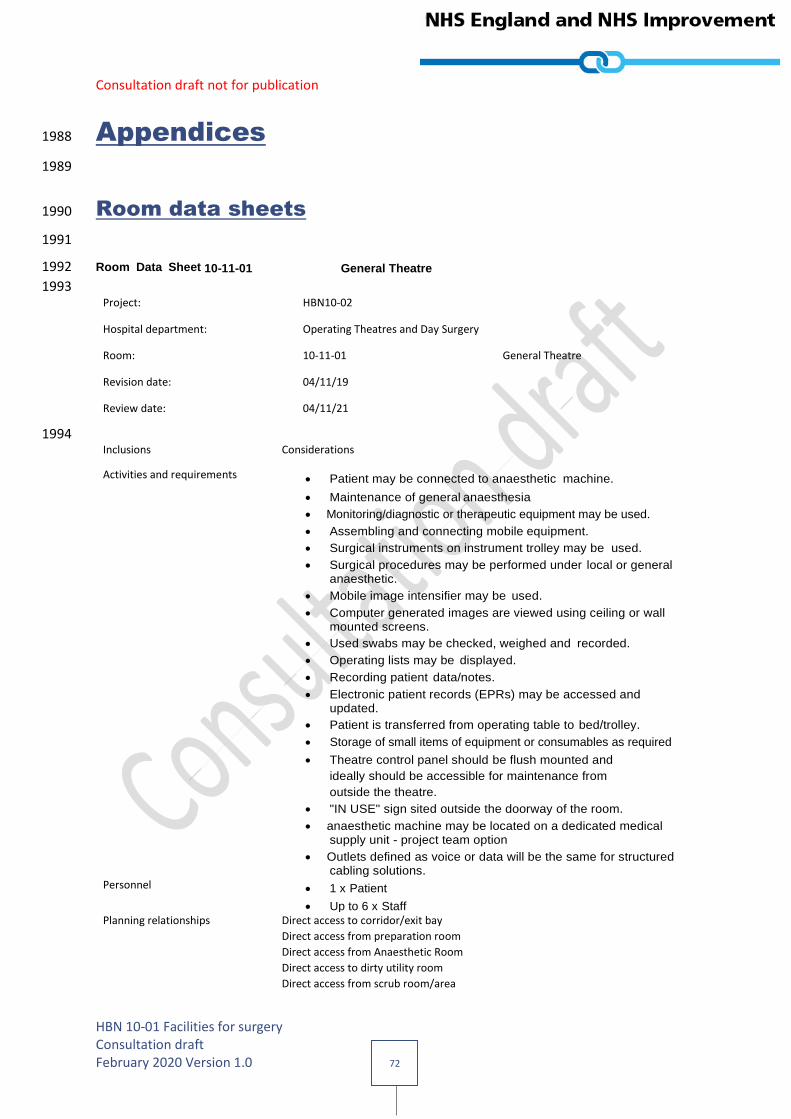
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 72
Appendices 1988
1989
Room data sheets 1990
1991
Room Data Sheet 10-11-01 General Theatre 1992
1993 Project: HBN10-02
Hospital department: Operating Theatres and Day Surgery
Room: 10-11-01 General Theatre
Revision date: 04/11/19
Review date: 04/11/21
1994 Inclusions Considerations
Activities and requirements Patient may be connected to anaesthetic machine.
Maintenance of general anaesthesia
Monitoring/diagnostic or therapeutic equipment may be used.
Assembling and connecting mobile equipment.
Surgical instruments on instrument trolley may be used.
Surgical procedures may be performed under local or general anaesthetic.
Mobile image intensifier may be used.
Computer generated images are viewed using ceiling or wall mounted screens.
Used swabs may be checked, weighed and recorded.
Operating lists may be displayed.
Recording patient data/notes.
Electronic patient records (EPRs) may be accessed and updated.
Patient is transferred from operating table to bed/trolley.
Storage of small items of equipment or consumables as required
Theatre control panel should be flush mounted and
ideally should be accessible for maintenance from
outside the theatre.
"IN USE" sign sited outside the doorway of the room.
anaesthetic machine may be located on a dedicated medical supply unit - project team option
Outlets defined as voice or data will be the same for structured cabling solutions.
Personnel 1 x Patient
Up to 6 x Staff Planning relationships Direct access to corridor/exit bay
Direct access from preparation room
Direct access from Anaesthetic Room
Direct access to dirty utility room
Direct access from scrub room/area
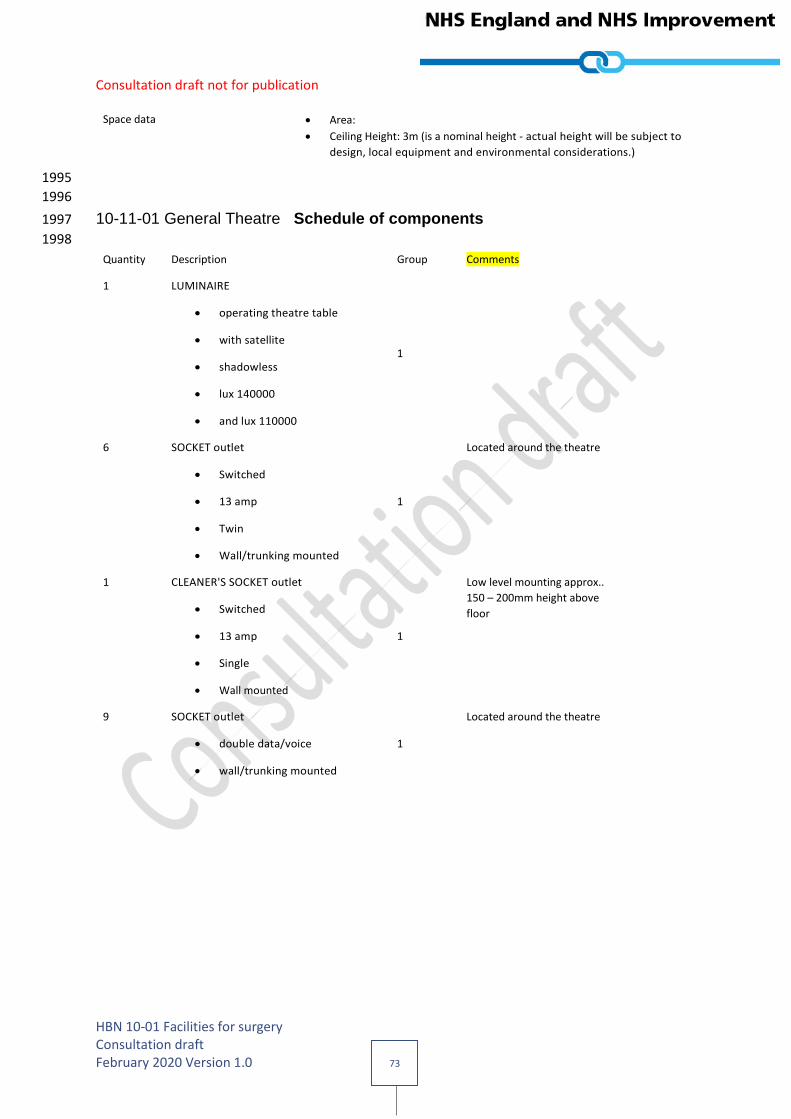
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 73
Space data Area:
Ceiling Height: 3m (is a nominal height - actual height will be subject to
design, local equipment and environmental considerations.)
1995
1996
10-11-01 General Theatre Schedule of components 1997
1998
Quantity Description Group Comments
1 LUMINAIRE
operating theatre table
with satellite
shadowless
lux 140000
and lux 110000
1
6 SOCKET outlet
Switched
13 amp
Twin
Wall/trunking mounted
1
Located around the theatre
1 CLEANER'S SOCKET outlet
Switched
13 amp
Single
Wall mounted
1
Low level mounting approx..
150 – 200mm height above
floor
9 SOCKET outlet
double data/voice
wall/trunking mounted
1
Located around the theatre
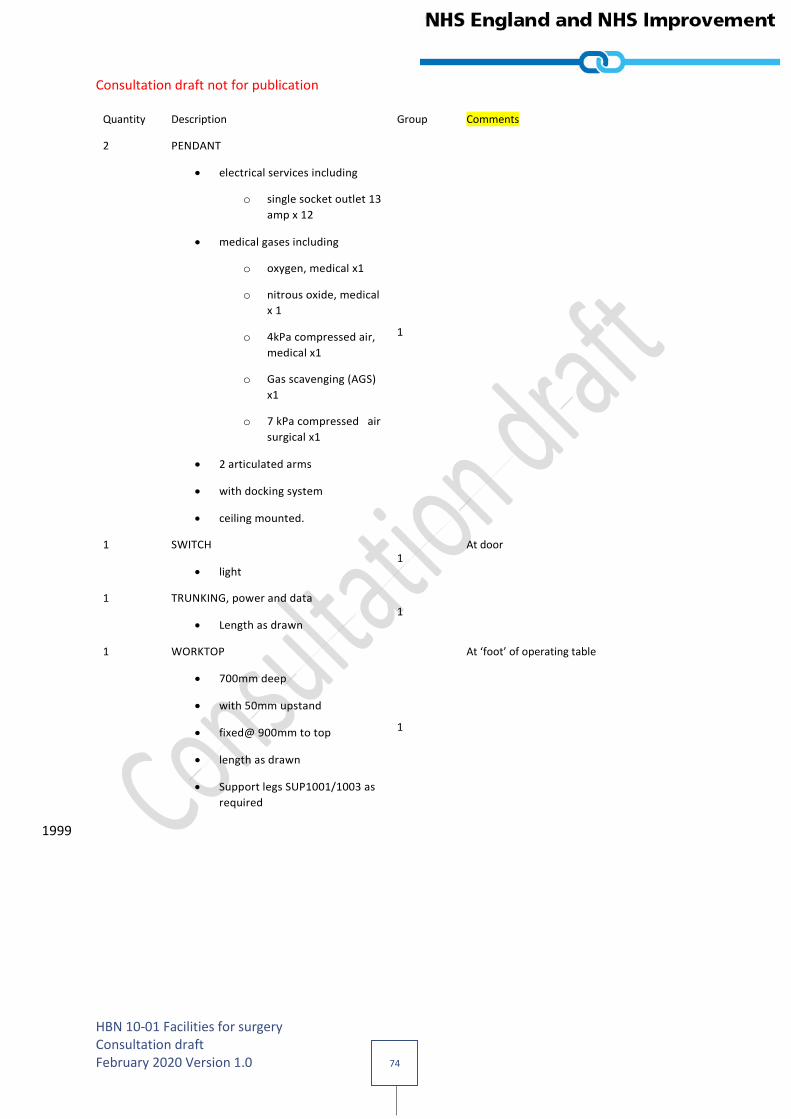
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 74
Quantity Description Group Comments
2 PENDANT
electrical services including
o single socket outlet 13
amp x 12
medical gases including
o oxygen, medical x1
o nitrous oxide, medical
x 1
o 4kPa compressed air,
medical x1
o Gas scavenging (AGS)
x1
o 7 kPa compressed air
surgical x1
2 articulated arms
with docking system
ceiling mounted.
1
1 SWITCH
light 1
At door
1 TRUNKING, power and data
Length as drawn 1
1 WORKTOP
700mm deep
with 50mm upstand
fixed@ 900mm to top
length as drawn
Support legs SUP1001/1003 as
required
1
At ‘foot’ of operating table
1999
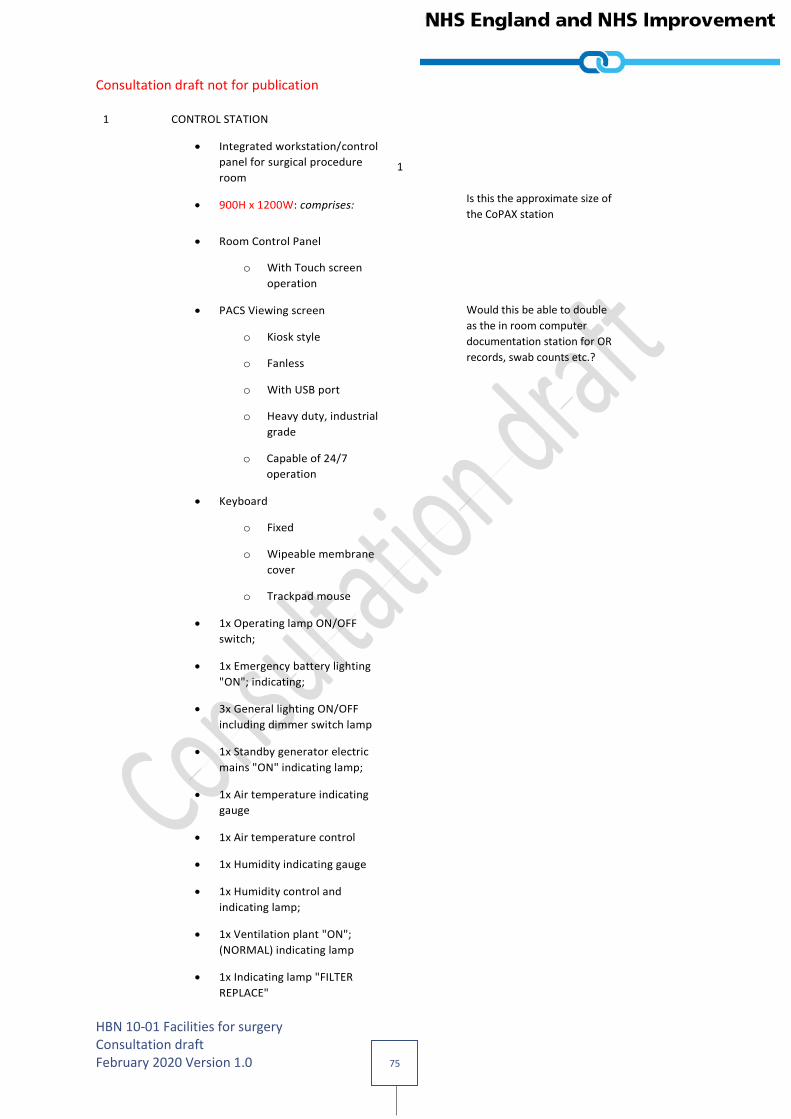
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 75
1 CONTROL STATION
Integrated workstation/control
panel for surgical procedure
room
900H x 1200W: comprises:
1
Is this the approximate size of
the CoPAX station
Room Control Panel
o With Touch screen
operation
PACS Viewing screen
o Kiosk style
o Fanless
o With USB port
o Heavy duty, industrial
grade
o Capable of 24/7
operation
Would this be able to double
as the in room computer
documentation station for OR
records, swab counts etc.?
Keyboard
o Fixed
o Wipeable membrane
cover
o Trackpad mouse
1x Operating lamp ON/OFF
switch;
1x Emergency battery lighting
"ON"; indicating;
3x General lighting ON/OFF
including dimmer switch lamp
1x Standby generator electric
mains "ON" indicating lamp;
1x Air temperature indicating
gauge
1x Air temperature control
1x Humidity indicating gauge
1x Humidity control and
indicating lamp;
1x Ventilation plant "ON";
(NORMAL) indicating lamp
1x Indicating lamp "FILTER
REPLACE"

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 76
1x Indicating lamp "LOW AIR
FLOW';
1x Indicating lamp "MEDICAL
GAS FAILURE"
1 x Clock time elapsed
1x Clock synchronous (time of
day)
1x Room "IN USE"; light,
ON/OFF switch
2 SCREEN, COMPUTER
ceiling/wall mounted 2
For ease of viewing from
surgeon’s operating position
2 BRACKET
Computer monitor
Ceiling/wall mounted
2
1 BOARD
Marker
Whiteboard
dry-wipe
with pen holder
wall mounted
600H 900W
2
Above worktop
1 ANAESTHETIC MACHINE/WORKSTATION
with ventilator
with accessories
mobile
1580H 565W 695D
3
2 SUCTION UNIT
Pipeline
high pressure
theatre
3
1 CHAIR
Anaesthetist
Wipeable
height adjustable
3

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 77
1 COMPUTER
complete with keyboard
screen
and telephone
wall mounted
3
At worktop
1 DIATHERMY APPARATUS
Surgical
monopolar and bipolar
operation
portable
190H 400W 330D
3
2 HOLDER
Sack
with lid
foot operated
large
capacity 120 litres
mobile
3
At ‘foot’ of table
2 KICKABOUT
bowl stand
stainless steel
360mm dia.
3
1 PLATFORM
step-stand
stackable
portable
130H 480W 330D
3
1 SCALE
Swab
includes Mains adaptor
3
At worktop
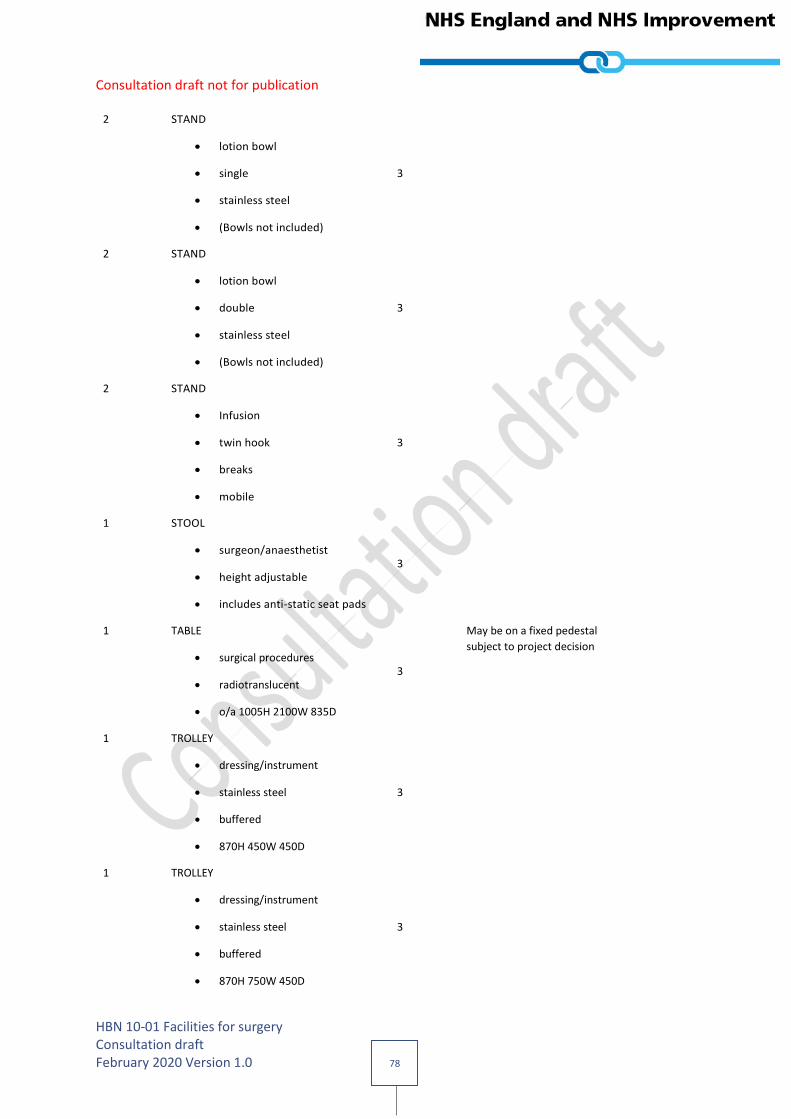
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 78
2 STAND
lotion bowl
single
stainless steel
(Bowls not included)
3
2 STAND
lotion bowl
double
stainless steel
(Bowls not included)
3
2 STAND
Infusion
twin hook
breaks
mobile
3
1 STOOL
surgeon/anaesthetist
height adjustable
includes anti-static seat pads
3
1 TABLE
surgical procedures
radiotranslucent
o/a 1005H 2100W 835D
3
May be on a fixed pedestal
subject to project decision
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 450W 450D
3
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 750W 450D
3

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 79
1 TROLLEY
Instruments
stainless steel
buffered
870H 920W 620D
3
1 TROLLEY
instrument tray
MAYO
Height adjustable
650W 450D
3
2000
2001

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 80
Room Data Sheet 10-11-03 Enhanced Treatment Room 2002
2003 Project: HBN10-02
Hospital department: Operating Theatres and Day Surgery
Room: 10-11-03 Enhanced Treatment Room
Revision date: 04/11/19
Review date: 04/11/21
2004 Inclusions Considerations
Activities and requirements Patient may be connected to anaesthetic machine.
Maintenance of general anaesthesia
Monitoring/diagnostic or therapeutic equipment may be used.
Assembling and connecting mobile equipment.
Surgical instruments on instrument trolley may be used.
Surgical procedures may be performed under local or general anaesthetic.
Mobile image intensifier may be used.
Computer generated images are viewed using ceiling or wall mounted screens
Used swabs may be checked, weighed and recorded.
Operating lists may be displayed.
Recording patient data/notes..
Electronic patient records (EPRs) may be accessed and updated.
Patient is transferred from operating table to bed/trolley.
Storage of small items of equipment or consumables as required
Theatre control panel should be flush mounted and
ideally should be accessible for maintenance from
outside the theatre.
"IN USE" sign sited outside the doorway of the room.
anaesthetic machine may be located on a dedicated medical supply unit - project team option
Outlets defined as voice or data will be the same for structured cabling solutions.
Personnel 1 x Patient
Up to 3 x Staff
Planning relationships Direct access to corridor/exit bay
Direct access from preparation room
Direct access to dirty utility room
Direct access from scrub room/area
Space data Area:
Ceiling Height: 3m (is a nominal height - actual height will be subject to
design, local equipment and environmental considerations.)
2005
2006
2007
2008
2009
2010
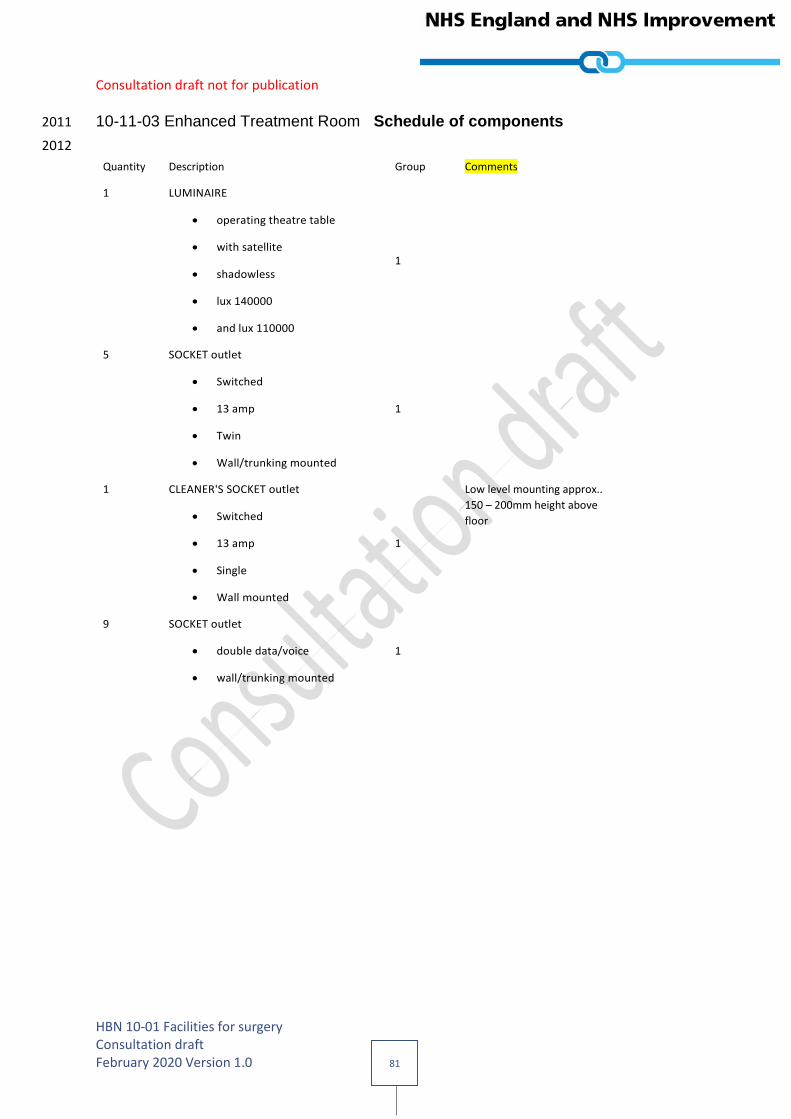
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 81
10-11-03 Enhanced Treatment Room Schedule of components 2011
2012
Quantity Description Group Comments
1 LUMINAIRE
operating theatre table
with satellite
shadowless
lux 140000
and lux 110000
1
5 SOCKET outlet
Switched
13 amp
Twin
Wall/trunking mounted
1
1 CLEANER'S SOCKET outlet
Switched
13 amp
Single
Wall mounted
1
Low level mounting approx..
150 – 200mm height above
floor
9 SOCKET outlet
double data/voice
wall/trunking mounted
1
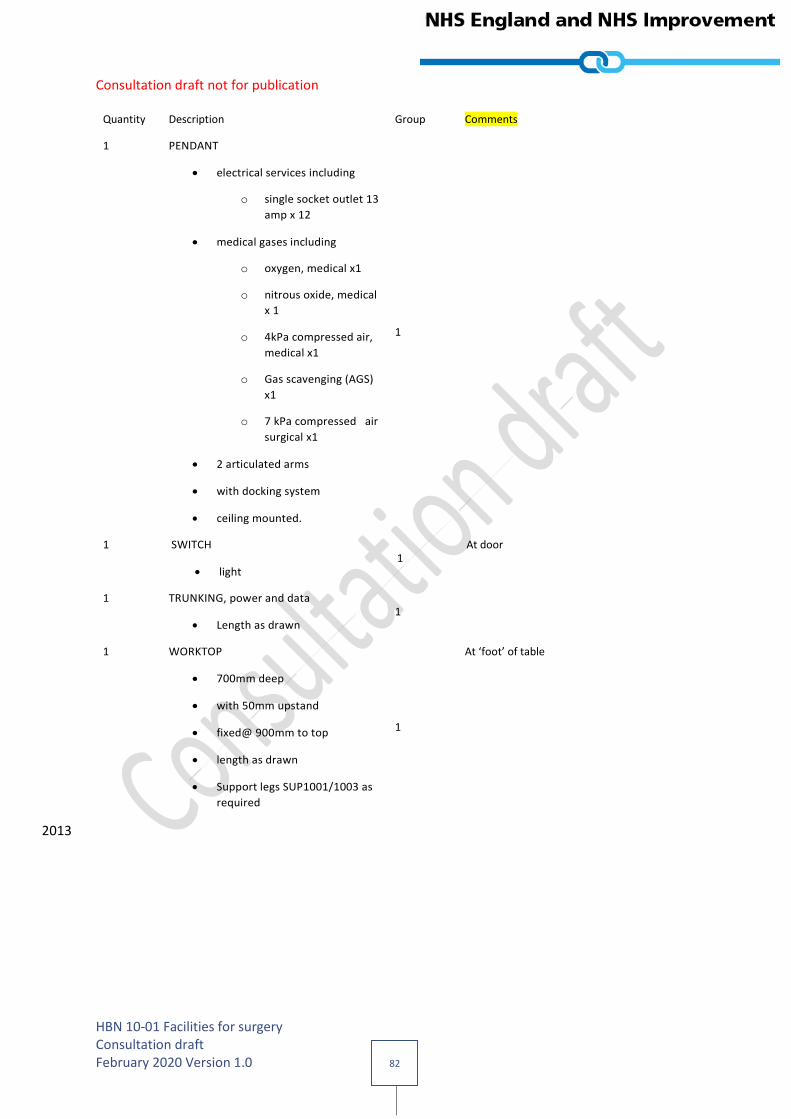
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 82
Quantity Description Group Comments
1 PENDANT
electrical services including
o single socket outlet 13
amp x 12
medical gases including
o oxygen, medical x1
o nitrous oxide, medical
x 1
o 4kPa compressed air,
medical x1
o Gas scavenging (AGS)
x1
o 7 kPa compressed air
surgical x1
2 articulated arms
with docking system
ceiling mounted.
1
1 SWITCH
light 1
At door
1 TRUNKING, power and data
Length as drawn 1
1 WORKTOP
700mm deep
with 50mm upstand
fixed@ 900mm to top
length as drawn
Support legs SUP1001/1003 as
required
1
At ‘foot’ of table
2013
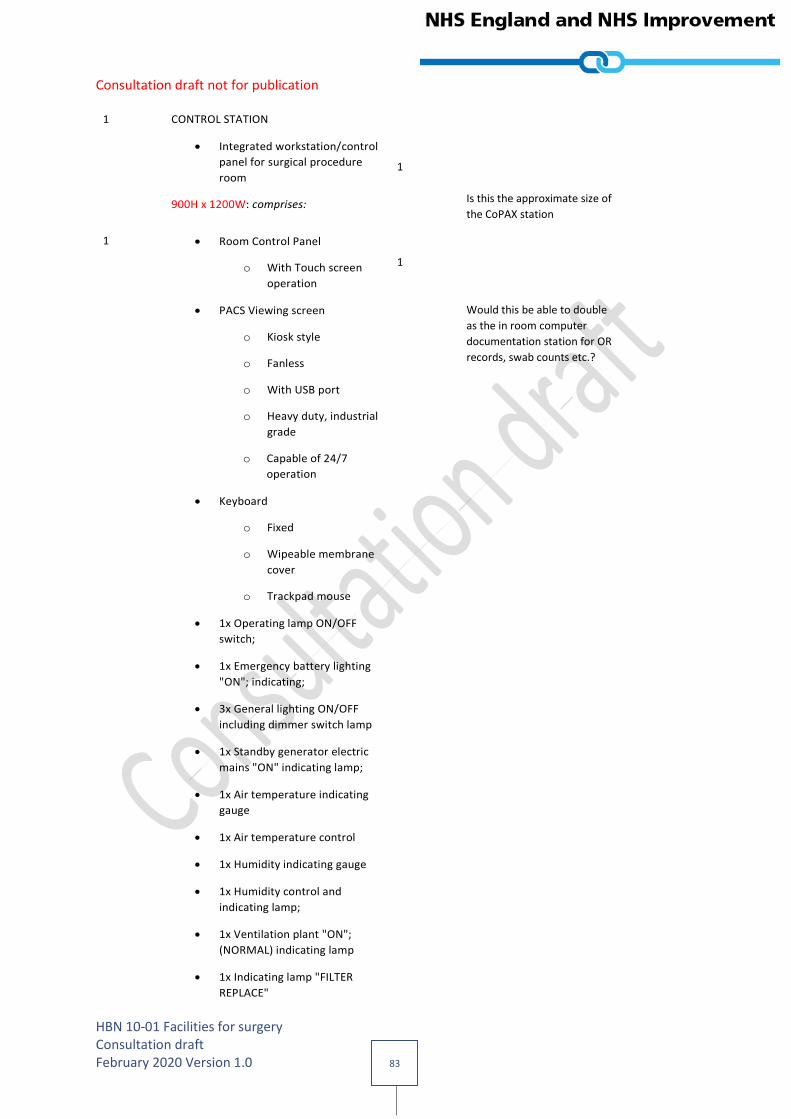
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 83
1 CONTROL STATION
Integrated workstation/control
panel for surgical procedure
room
900H x 1200W: comprises:
1
Is this the approximate size of
the CoPAX station
1 Room Control Panel
o With Touch screen
operation
1
PACS Viewing screen
o Kiosk style
o Fanless
o With USB port
o Heavy duty, industrial
grade
o Capable of 24/7
operation
Would this be able to double
as the in room computer
documentation station for OR
records, swab counts etc.?
Keyboard
o Fixed
o Wipeable membrane
cover
o Trackpad mouse
1x Operating lamp ON/OFF
switch;
1x Emergency battery lighting
"ON"; indicating;
3x General lighting ON/OFF
including dimmer switch lamp
1x Standby generator electric
mains "ON" indicating lamp;
1x Air temperature indicating
gauge
1x Air temperature control
1x Humidity indicating gauge
1x Humidity control and
indicating lamp;
1x Ventilation plant "ON";
(NORMAL) indicating lamp
1x Indicating lamp "FILTER
REPLACE"
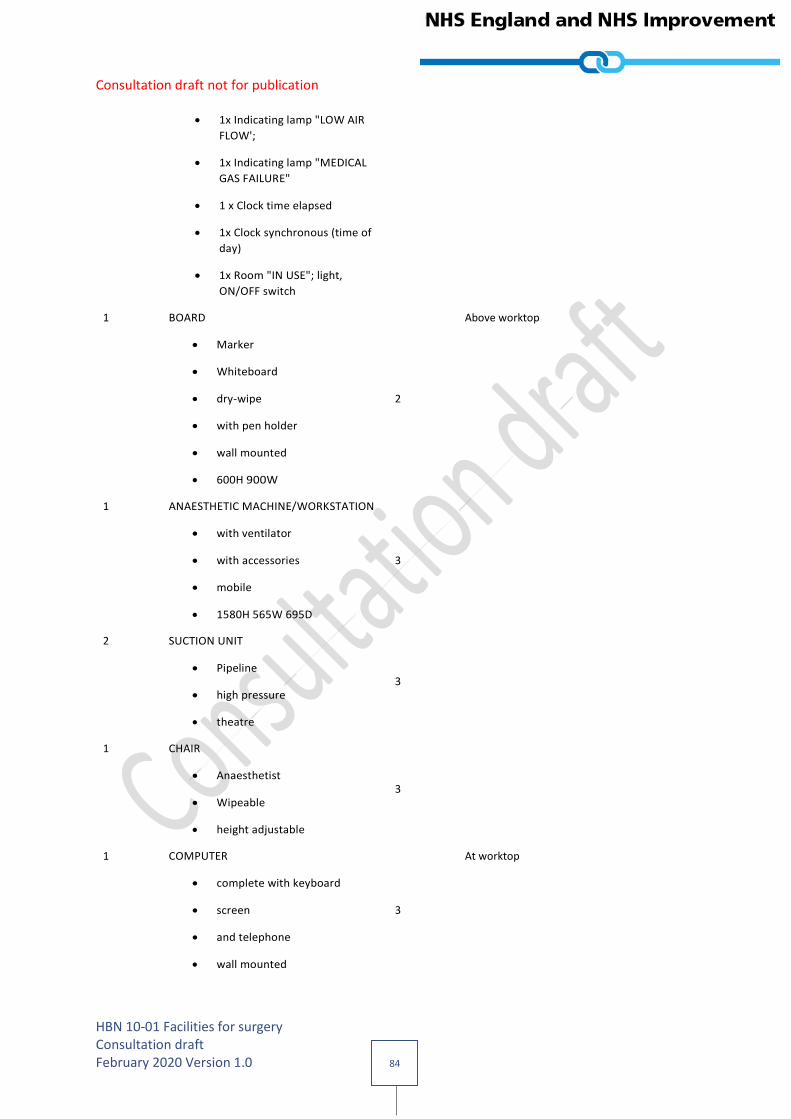
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 84
1x Indicating lamp "LOW AIR
FLOW';
1x Indicating lamp "MEDICAL
GAS FAILURE"
1 x Clock time elapsed
1x Clock synchronous (time of
day)
1x Room "IN USE"; light,
ON/OFF switch
1 BOARD
Marker
Whiteboard
dry-wipe
with pen holder
wall mounted
600H 900W
2
Above worktop
1 ANAESTHETIC MACHINE/WORKSTATION
with ventilator
with accessories
mobile
1580H 565W 695D
3
2 SUCTION UNIT
Pipeline
high pressure
theatre
3
1 CHAIR
Anaesthetist
Wipeable
height adjustable
3
1 COMPUTER
complete with keyboard
screen
and telephone
wall mounted
3
At worktop

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 85
1 DIATHERMY APPARATUS
Surgical
monopolar and bipolar
operation
portable
190H 400W 330D
3
2 HOLDER
Sack
with lid
foot operated
large
capacity 120 litres
mobile
3
At ‘foot’ of table
2 KICKABOUT
bowl stand
stainless steel
360mm dia.
3
1 PLATFORM
step-stand
stackable
portable
130H 480W 330D
3
1 SCALE
Swab
includes Mains adaptor
3
At worktop
2 STAND
lotion bowl
single
stainless steel
(Bowls not included)
3
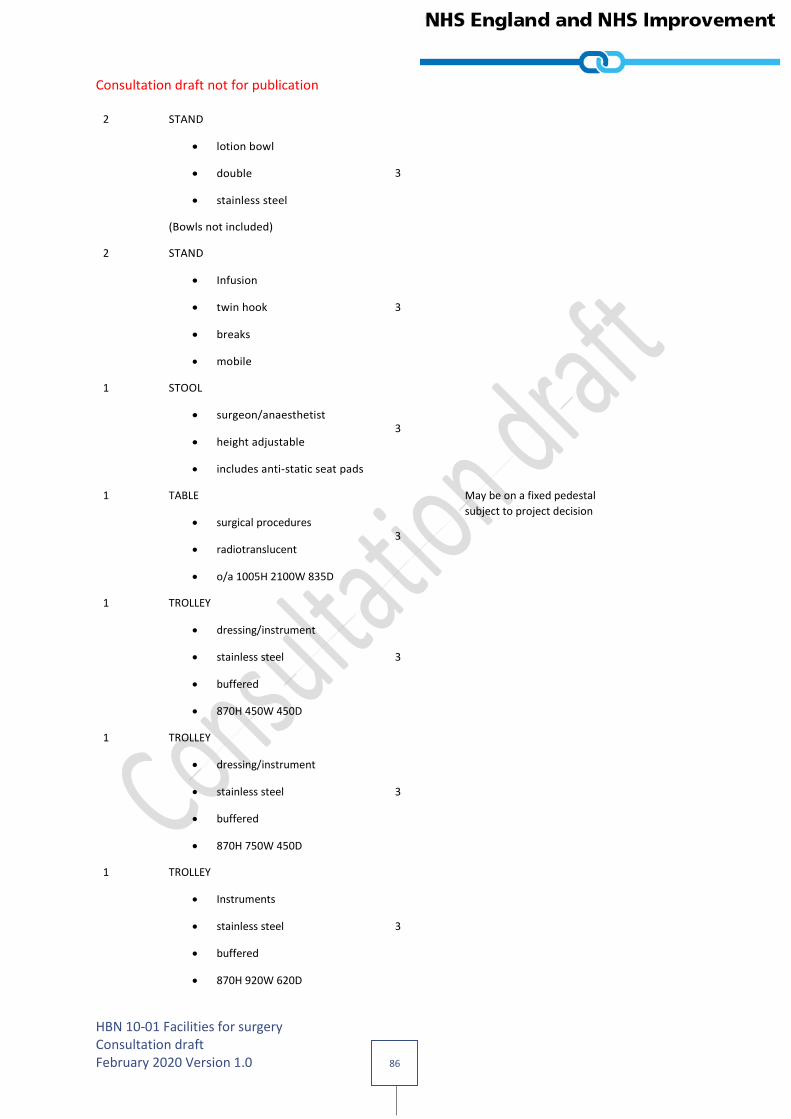
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 86
2 STAND
lotion bowl
double
stainless steel
(Bowls not included)
3
2 STAND
Infusion
twin hook
breaks
mobile
3
1 STOOL
surgeon/anaesthetist
height adjustable
includes anti-static seat pads
3
1 TABLE
surgical procedures
radiotranslucent
o/a 1005H 2100W 835D
3
May be on a fixed pedestal
subject to project decision
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 450W 450D
3
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 750W 450D
3
1 TROLLEY
Instruments
stainless steel
buffered
870H 920W 620D
3

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 87
1 TROLLEY
instrument tray
MAYO
Height adjustable
650W 450D
3
2014
2015

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 88
Room Data Sheet: 10-11-04 Hybrid Operating Theatre (CT) 2016
2017 Project: HBN10-02
Hospital department: Operating Theatres and Day Surgery
Room: 10-11-04 Hybrid Operating Theatre (CT)
Revision date: 04/11/19
Review date: 04/11/21
2018 Inclusions Considerations
Activities and requirements Patient may be connected to anaesthetic machine.
Maintenance of general anaesthesia
Monitoring/diagnostic or therapeutic equipment may be used.
Assembling and connecting mobile equipment.
Surgical instruments on instrument trolley may be used.
Surgical procedures may be performed under local or general anaesthetic.
Patient undergoes interventional procedures under CT scan
Computer generated images are viewed using ceiling or wall mounted screens.
Used swabs may be checked, weighed and recorded.
Operating lists may be displayed.
Recording patient data/notes.
Electronic patient records (EPRs) may be accessed and updated.
Patient is transferred from operating table to bed/trolley.
Storage of small items of equipment or consumables as required
Theatre control panel should be flush mounted and
ideally should be accessible for maintenance from
outside the theatre.
"IN USE" sign sited outside the doorway of the room.
anaesthetic machine may be located on a dedicated medical supply unit - project team option
Outlets defined as voice or data will be the same for structured cabling solutions.
Contrast media may be administered.
Disposal of waste.
Personnel 1 x Patient
Up to 8 x Staff
Planning relationships Direct access to corridor/exit bay
Direct access from preparation room
Direct access from Anaesthetic Room
Direct access to dirty utility room
Direct access from scrub room/area
Direct access of CT scanner from ‘parked’ position.
Direct line of sight from control room to surgeon
Space data Area:
Ceiling Height: 3m (is a nominal height - actual height will be subject to
design, local equipment and environmental considerations.)
2019
2020
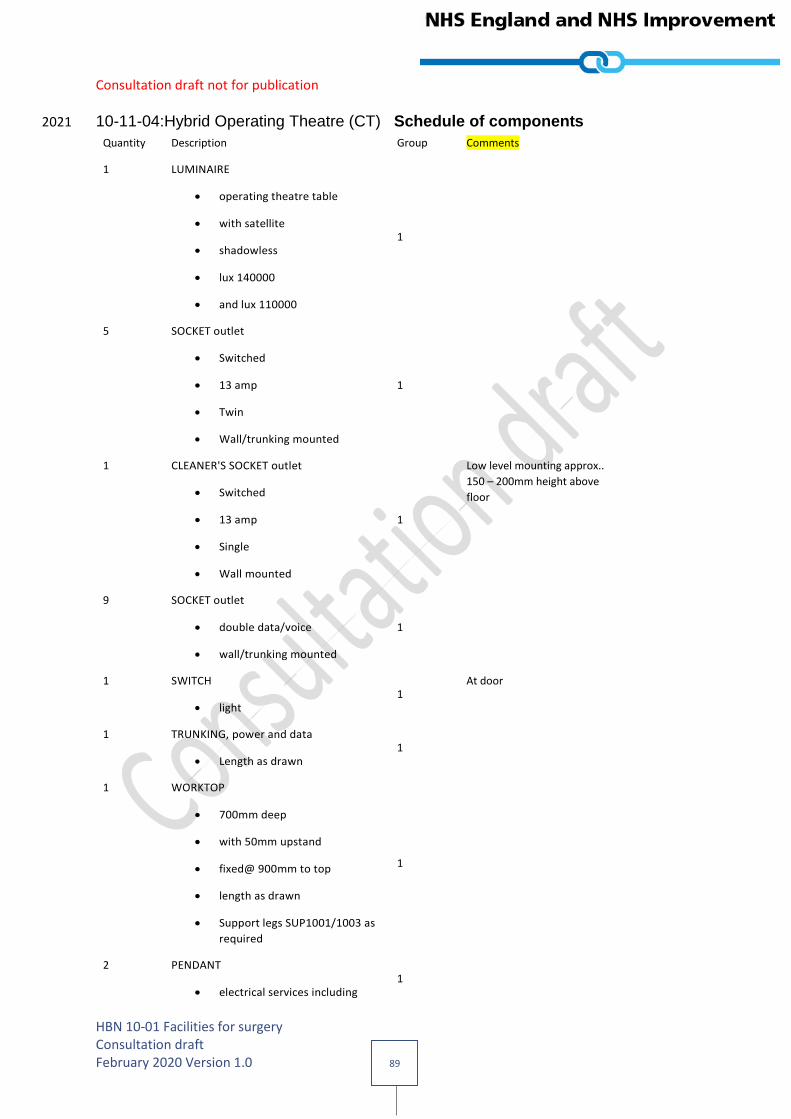
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 89
10-11-04:Hybrid Operating Theatre (CT) Schedule of components 2021
Quantity Description Group Comments
1 LUMINAIRE
operating theatre table
with satellite
shadowless
lux 140000
and lux 110000
1
5 SOCKET outlet
Switched
13 amp
Twin
Wall/trunking mounted
1
1 CLEANER'S SOCKET outlet
Switched
13 amp
Single
Wall mounted
1
Low level mounting approx..
150 – 200mm height above
floor
9 SOCKET outlet
double data/voice
wall/trunking mounted
1
1 SWITCH
light 1
At door
1 TRUNKING, power and data
Length as drawn 1
1 WORKTOP
700mm deep
with 50mm upstand
fixed@ 900mm to top
length as drawn
Support legs SUP1001/1003 as
required
1
2 PENDANT
electrical services including 1

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 90
Quantity Description Group Comments
o single socket outlet 13
amp x 12
medical gases including
o oxygen, medical x1
o nitrous oxide, medical
x 1
o 4kPa compressed air,
medical x1
o Gas scavenging (AGS)
x1
o 7 kPa compressed air
surgical x1
2 articulated arms
with docking system
ceiling mounted.
2022
2023
2024
1 CONTROL STATION
Integrated workstation/control
panel for surgical procedure
room
900H x 1200W: comprises:
1
Is this the approximate size of
the CoPAX station
Room Control Panel
o With Touch screen
operation
1
PACS Viewing screen
o Kiosk style
o Fanless
o With USB port
o Heavy duty, industrial
grade
o Capable of 24/7
operation
Would this be able to double
as the in room computer
documentation station for OR
records, swab counts etc.?
Keyboard
o Fixed
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 91
o Wipeable membrane
cover
o Trackpad mouse
1x Operating lamp ON/OFF
switch;
1x Emergency battery lighting
"ON"; indicating;
3x General lighting ON/OFF
including dimmer switch lamp
1x Standby generator electric
mains "ON" indicating lamp;
1x Air temperature indicating
gauge
1x Air temperature control
1x Humidity indicating gauge
1x Humidity control and
indicating lamp;
1x Ventilation plant "ON";
(NORMAL) indicating lamp
1x Indicating lamp "FILTER
REPLACE"
1x Indicating lamp "LOW AIR
FLOW';
1x Indicating lamp "MEDICAL
GAS FAILURE"
1 x Clock time elapsed
1x Clock synchronous (time of
day)
1x Room "IN USE"; light,
ON/OFF switch
2025
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 92
1 IMAGER, COMPUTER TOMOGRAPHY (CT)
128 slice unit 2
1 IMAGER, COMPUTER TOMOGRAPHY (CT)
heat exchanger
1800H 900W 750D
2
1 IMAGER, COMPUTER TOMOGRAPHY (CT)
imaging cabinet
1800H 900W 750D
2
1 RACK, x-ray lead apron
3 hangers
hinged
wall mounted
2
2 SCREEN, COMPUTER
ceiling/wall mounted 2
2 BRACKET
Computer monitor
Ceiling/wall mounted
2
1 BOARD
Marker
Whiteboard
dry-wipe
with pen holder
wall mounted
600H 900W
2
Above worktop
1 ANAESTHETIC MACHINE/WORKSTATION
with ventilator
with accessories
mobile
1580H 565W 695D
3
2 SUCTION UNIT
Pipeline
high pressure
theatre
3
1 CHAIR 3
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 93
Anaesthetist
Wipeable
height adjustable
1 COMPUTER
complete with keyboard
screen
and telephone
wall mounted
3
at worktop
1 DIATHERMY APPARATUS
Surgical
monopolar and bipolar
operation
portable
190H 400W 330D
3
2 HOLDER
Sack
with lid
foot operated
large
capacity 120 litres
mobile
3
by worktop
2 KICKABOUT
bowl stand
stainless steel
360mm dia.
3
1 PLATFORM
step-stand
stackable
portable
130H 480W 330D
3
1 SCALE
Swab
includes Mains adaptor
3
at worktop

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 94
2 STAND
lotion bowl
single
stainless steel
(Bowls not included)
3
2 STAND
lotion bowl
double
stainless steel
(Bowls not included)
3
2 STAND
Infusion
twin hook
breaks
mobile
3
1 STOOL
surgeon/anaesthetist
height adjustable
includes anti-static seat pads
3
1 TABLE
surgical procedures
radiotranslucent
o/a 1005H 2100W 835D
3
Will be on a fixed pedestal,
commensurate with type and
make of CT Scanner
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 450W 450D
3
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 750W 450D
3
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 95
1 TROLLEY
Instruments
stainless steel
buffered
870H 920W 620D
3
1 TROLLEY
instrument tray
MAYO
Height adjustable
650W 450D
3
2026
2027
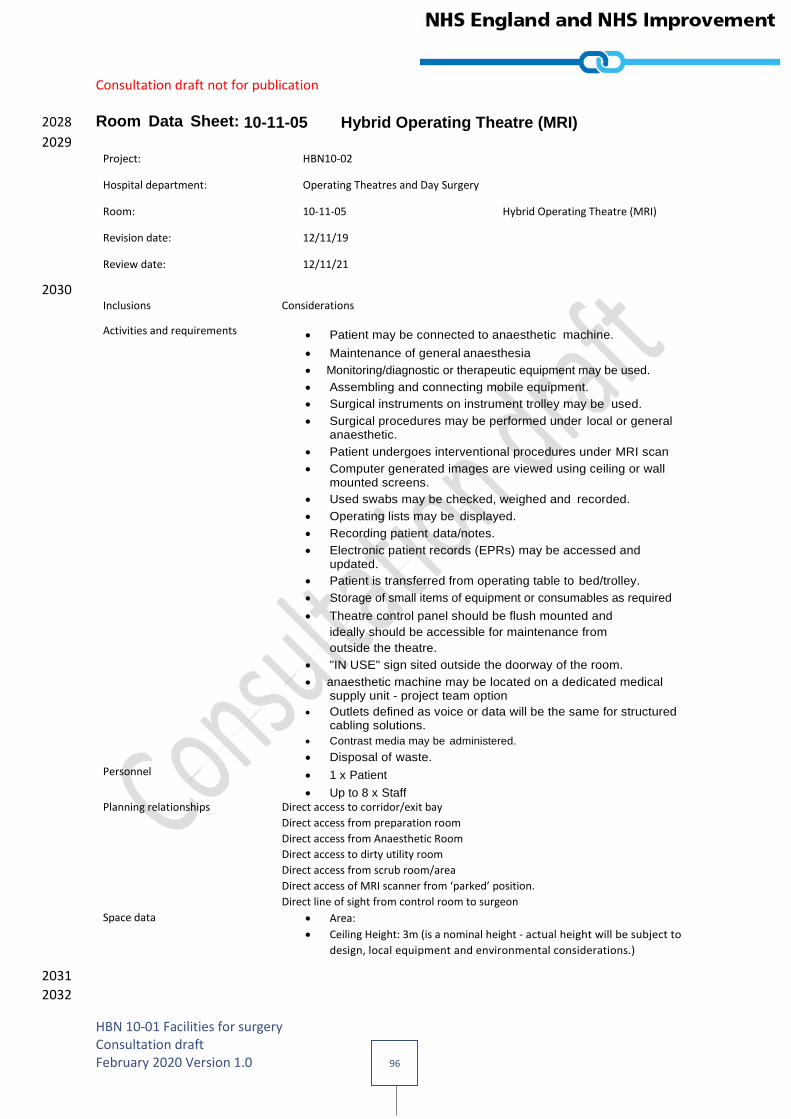
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 96
Room Data Sheet: 10-11-05 Hybrid Operating Theatre (MRI) 2028
2029 Project: HBN10-02
Hospital department: Operating Theatres and Day Surgery
Room: 10-11-05 Hybrid Operating Theatre (MRI)
Revision date: 12/11/19
Review date: 12/11/21
2030 Inclusions Considerations
Activities and requirements Patient may be connected to anaesthetic machine.
Maintenance of general anaesthesia
Monitoring/diagnostic or therapeutic equipment may be used.
Assembling and connecting mobile equipment.
Surgical instruments on instrument trolley may be used.
Surgical procedures may be performed under local or general anaesthetic.
Patient undergoes interventional procedures under MRI scan
Computer generated images are viewed using ceiling or wall mounted screens.
Used swabs may be checked, weighed and recorded.
Operating lists may be displayed.
Recording patient data/notes.
Electronic patient records (EPRs) may be accessed and updated.
Patient is transferred from operating table to bed/trolley.
Storage of small items of equipment or consumables as required
Theatre control panel should be flush mounted and
ideally should be accessible for maintenance from
outside the theatre.
"IN USE" sign sited outside the doorway of the room.
anaesthetic machine may be located on a dedicated medical supply unit - project team option
Outlets defined as voice or data will be the same for structured cabling solutions.
Contrast media may be administered.
Disposal of waste.
Personnel 1 x Patient
Up to 8 x Staff
Planning relationships Direct access to corridor/exit bay
Direct access from preparation room
Direct access from Anaesthetic Room
Direct access to dirty utility room
Direct access from scrub room/area
Direct access of MRI scanner from ‘parked’ position.
Direct line of sight from control room to surgeon
Space data Area:
Ceiling Height: 3m (is a nominal height - actual height will be subject to
design, local equipment and environmental considerations.)
2031
2032
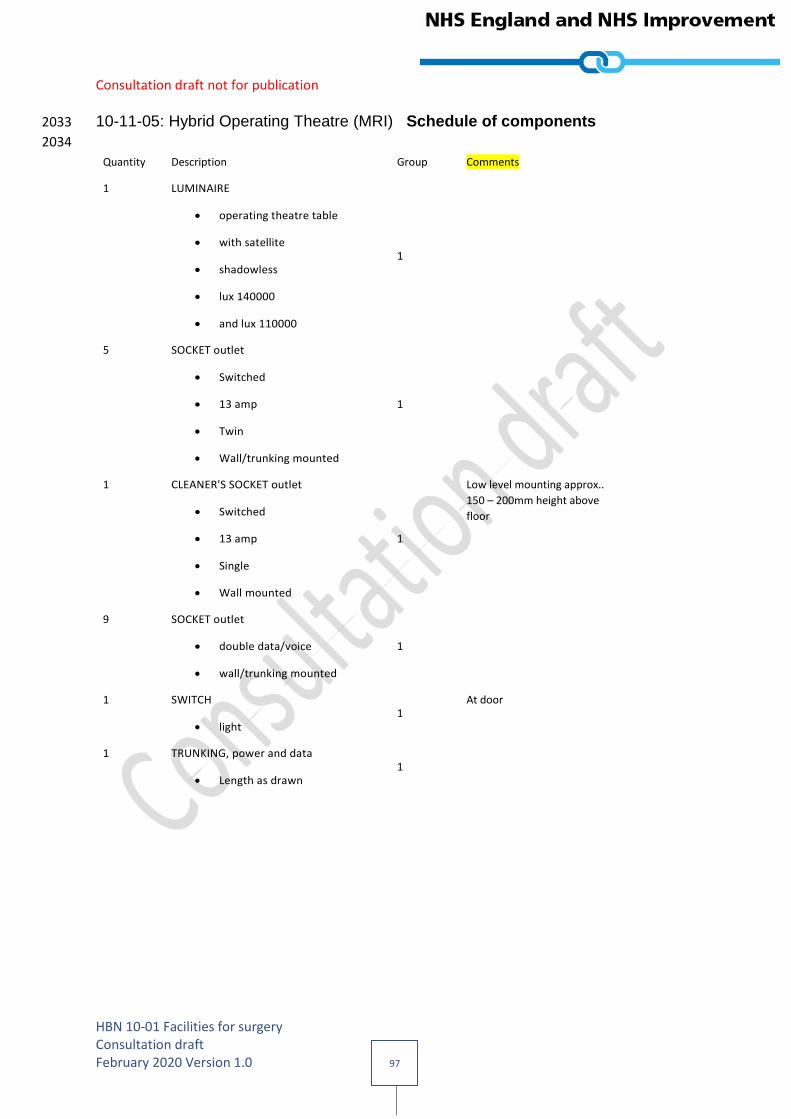
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 97
10-11-05: Hybrid Operating Theatre (MRI) Schedule of components 2033
2034
Quantity Description Group Comments
1 LUMINAIRE
operating theatre table
with satellite
shadowless
lux 140000
and lux 110000
1
5 SOCKET outlet
Switched
13 amp
Twin
Wall/trunking mounted
1
1 CLEANER'S SOCKET outlet
Switched
13 amp
Single
Wall mounted
1
Low level mounting approx..
150 – 200mm height above
floor
9 SOCKET outlet
double data/voice
wall/trunking mounted
1
1 SWITCH
light 1
At door
1 TRUNKING, power and data
Length as drawn 1

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 98
Quantity Description Group Comments
2 PENDANT
electrical services including
o single socket outlet 13
amp x 12
medical gases including
o oxygen, medical x1
o nitrous oxide, medical
x 1
o 4kPa compressed air,
medical x1
o Gas scavenging (AGS)
x1
o 7 kPa compressed air
surgical x1
2 articulated arms
with docking system
ceiling mounted.
1
1 WORKTOP
700mm deep
with 50mm upstand
fixed@ 900mm to top
length as drawn
Support legs SUP1001/1003 as required
1
2035
2036
2037
1 CONTROL STATION
Integrated workstation/control
panel for surgical procedure
room
900H x 1200W: comprises:
1
Is this the approximate size of
the CoPAX station
Room Control Panel
o With Touch screen
operation
PACS Viewing screen Would this be able to double
as the in room computer
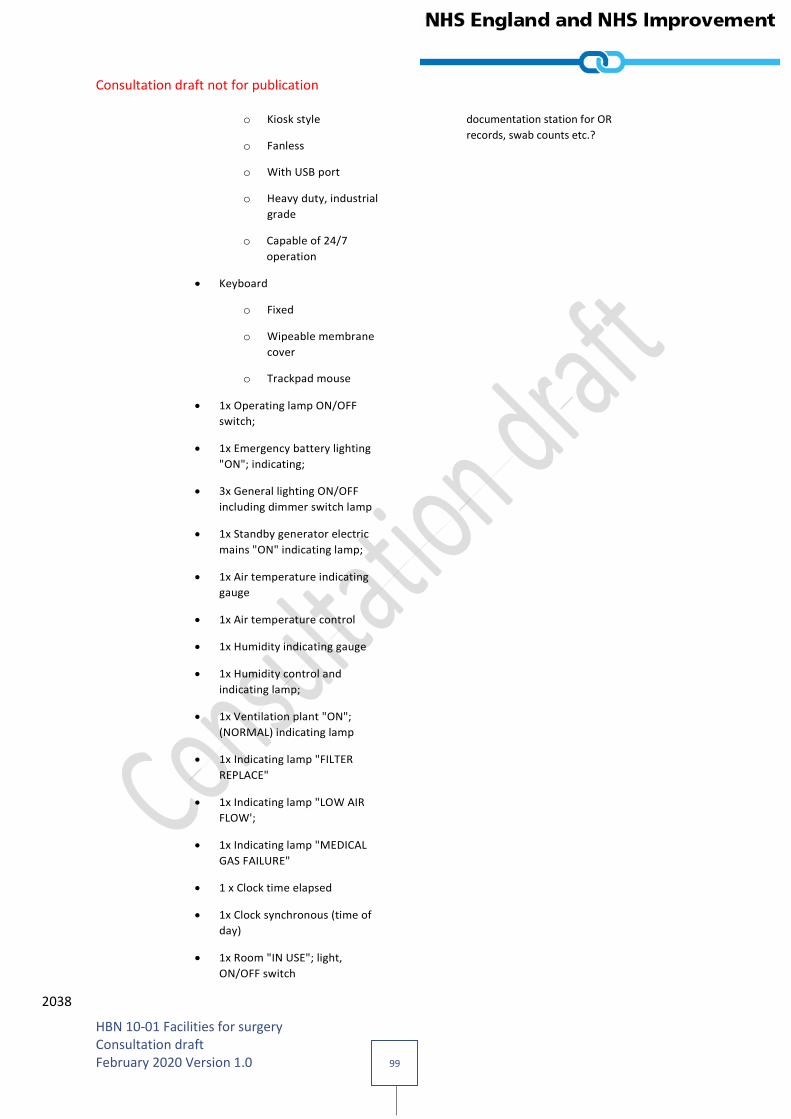
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 99
o Kiosk style
o Fanless
o With USB port
o Heavy duty, industrial
grade
o Capable of 24/7
operation
documentation station for OR
records, swab counts etc.?
Keyboard
o Fixed
o Wipeable membrane
cover
o Trackpad mouse
1x Operating lamp ON/OFF
switch;
1x Emergency battery lighting
"ON"; indicating;
3x General lighting ON/OFF
including dimmer switch lamp
1x Standby generator electric
mains "ON" indicating lamp;
1x Air temperature indicating
gauge
1x Air temperature control
1x Humidity indicating gauge
1x Humidity control and
indicating lamp;
1x Ventilation plant "ON";
(NORMAL) indicating lamp
1x Indicating lamp "FILTER
REPLACE"
1x Indicating lamp "LOW AIR
FLOW';
1x Indicating lamp "MEDICAL
GAS FAILURE"
1 x Clock time elapsed
1x Clock synchronous (time of
day)
1x Room "IN USE"; light,
ON/OFF switch
2038
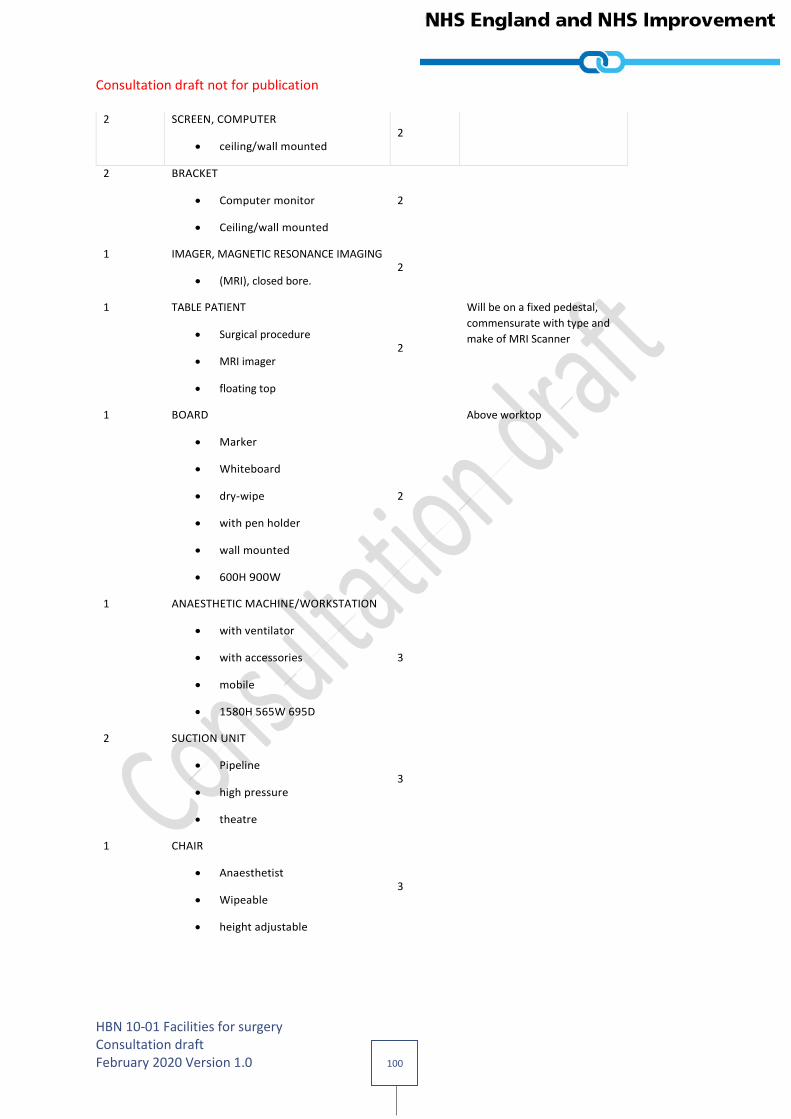
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 100
2 SCREEN, COMPUTER
ceiling/wall mounted 2
2 BRACKET
Computer monitor
Ceiling/wall mounted
2
1 IMAGER, MAGNETIC RESONANCE IMAGING
(MRI), closed bore. 2
1 TABLE PATIENT
Surgical procedure
MRI imager
floating top
2
Will be on a fixed pedestal,
commensurate with type and
make of MRI Scanner
1 BOARD
Marker
Whiteboard
dry-wipe
with pen holder
wall mounted
600H 900W
2
Above worktop
1 ANAESTHETIC MACHINE/WORKSTATION
with ventilator
with accessories
mobile
1580H 565W 695D
3
2 SUCTION UNIT
Pipeline
high pressure
theatre
3
1 CHAIR
Anaesthetist
Wipeable
height adjustable
3
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 101
1 COMPUTER
complete with keyboard
screen
and telephone
wall mounted
3
at worktop
1 DIATHERMY APPARATUS
Surgical
monopolar and bipolar
operation
portable
190H 400W 330D
3
2 HOLDER
Sack
with lid
foot operated
large
capacity 120 litres
mobile
3
by worktop
2 KICKABOUT
bowl stand
stainless steel
360mm dia.
3
1 PLATFORM
step-stand
stackable
portable
130H 480W 330D
3
1 SCALE
Swab
includes Mains adaptor
3
at worktop

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 102
2 STAND
lotion bowl
single
stainless steel
(Bowls not included)
3
2 STAND
lotion bowl
double
stainless steel
(Bowls not included)
3
2 STAND
Infusion
twin hook
breaks
mobile
3
1 STOOL
surgeon/anaesthetist
height adjustable
includes anti-static seat pads
3
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 450W 450D
3
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 750W 450D
3
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 103
1 TROLLEY
Instruments
stainless steel
buffered
870H 920W 620D
3
1 TROLLEY
instrument tray
MAYO
Height adjustable
650W 450D
3
2039
2040
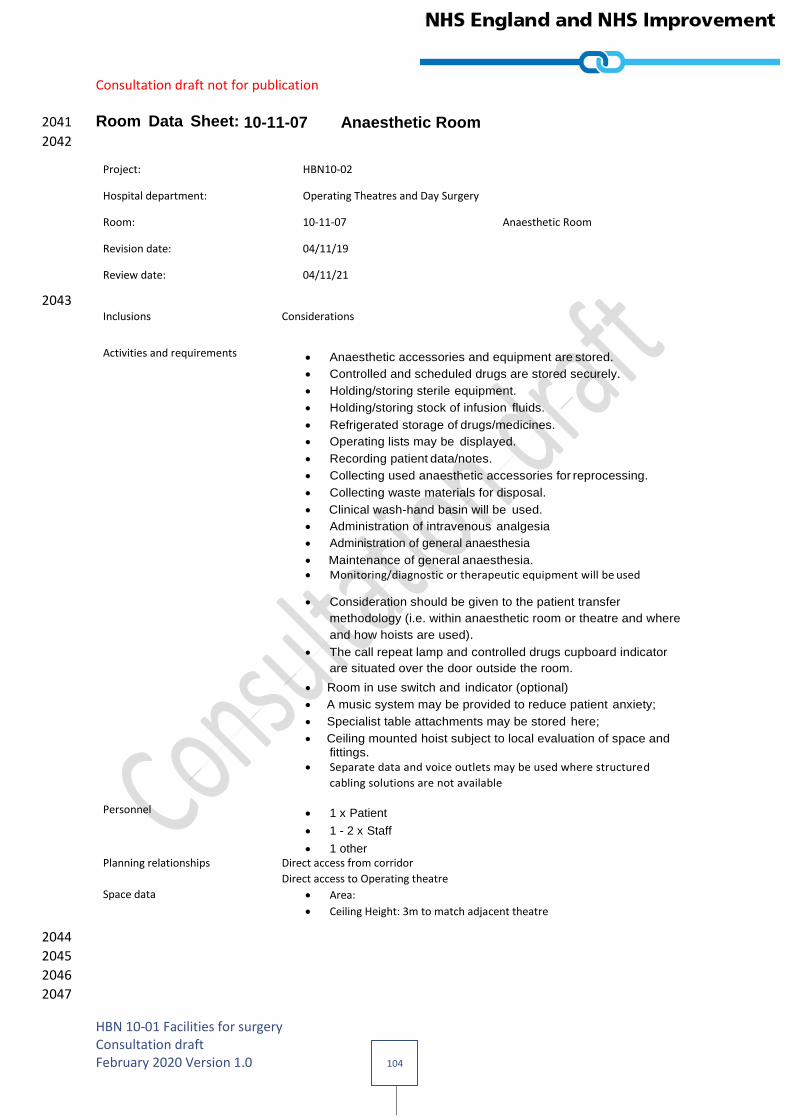
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 104
Room Data Sheet: 10-11-07 Anaesthetic Room 2041
2042
Project: HBN10-02
Hospital department: Operating Theatres and Day Surgery
Room: 10-11-07 Anaesthetic Room
Revision date: 04/11/19
Review date: 04/11/21
2043 Inclusions Considerations
Activities and requirements Anaesthetic accessories and equipment are stored.
Controlled and scheduled drugs are stored securely.
Holding/storing sterile equipment.
Holding/storing stock of infusion fluids.
Refrigerated storage of drugs/medicines.
Operating lists may be displayed.
Recording patient data/notes.
Collecting used anaesthetic accessories for reprocessing.
Collecting waste materials for disposal.
Clinical wash-hand basin will be used.
Administration of intravenous analgesia
Administration of general anaesthesia
Maintenance of general anaesthesia.
Monitoring/diagnostic or therapeutic equipment will be used
Consideration should be given to the patient transfer
methodology (i.e. within anaesthetic room or theatre and where
and how hoists are used).
The call repeat lamp and controlled drugs cupboard indicator
are situated over the door outside the room.
Room in use switch and indicator (optional)
A music system may be provided to reduce patient anxiety;
Specialist table attachments may be stored here;
Ceiling mounted hoist subject to local evaluation of space and fittings.
Separate data and voice outlets may be used where structured
cabling solutions are not available
Personnel 1 x Patient
1 - 2 x Staff
1 other
Planning relationships Direct access from corridor
Direct access to Operating theatre
Space data Area:
Ceiling Height: 3m to match adjacent theatre
2044
2045
2046
2047

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 105
10-11-07: Anaesthetic Room Schedule of components 2048
Quantity Description Group Comments
1 PULL/PUSH BUTTON
staff emergency call, reset
integral/adjacent indicator lamp
wall mounted
1
Above worktop
1 LAMP
repeat call, patient / staff or staff
emergency
or cardiac call
1
At door
1 LUMINAIRE
Examination
Ceiling mounted
Adjustable
1000 lux
1
At head of patient
1 ILLUMINATED SIGN
'Room in use' 1
Outside door
1 LUMINAIRE
indicating controlled drugs
cupboard repeat
1
6 SOCKET outlet
switched
13 amp
twin
wall/trunking mounted
1
1 CONNECTION UNIT
switched
13 amp
flex outlet
indicator light
wall mounted
1
Adjacent to controlled drugs
cupboard
1 CLEANERS’ SOCKET outlet
switched
13 amp
1
Low level mounting approx.
150 – 200mm height above
floor
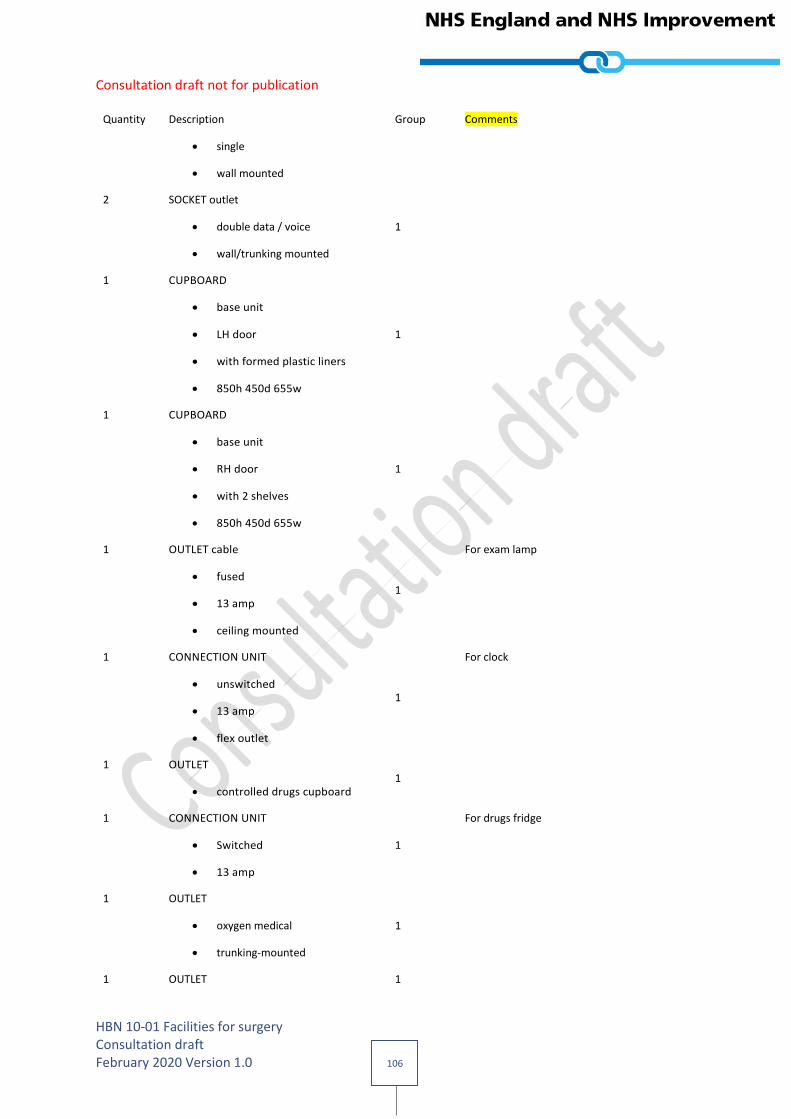
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 106
Quantity Description Group Comments
single
wall mounted
2 SOCKET outlet
double data / voice
wall/trunking mounted
1
1 CUPBOARD
base unit
LH door
with formed plastic liners
850h 450d 655w
1
1 CUPBOARD
base unit
RH door
with 2 shelves
850h 450d 655w
1
1 OUTLET cable
fused
13 amp
ceiling mounted
1
For exam lamp
1 CONNECTION UNIT
unswitched
13 amp
flex outlet
1
For clock
1 OUTLET
controlled drugs cupboard 1
1 CONNECTION UNIT
Switched
13 amp
1
For drugs fridge
1 OUTLET
oxygen medical
trunking-mounted
1
1 OUTLET 1

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 107
Quantity Description Group Comments
vacuum medical
trunking mounted
1 OUTLET
4 kPa compressed air, medical
trunking mounted
1
1 OUTLET
nitrous oxide medical
trunking mounted
1
1 OUTLET
gas scavenging (AGS), medical
trunking mounted
1
1 SWITCH
light 1
At door
1 SWITCH
'Room in use' illuminated sign. 1
At door
1 WORKTOP, Clinical
700mm deep,
with 50mm upstand
fixed@ 900mm to top
length as drawn
Support legs SUP1001/1003 as
required
1
1 WASH BASIN
Clinical
with non touch panel mounted
tap/s.
1
1 TRUNKING for power and data
length as drawn 1
1 TRUNKING for medical services
length as drawn 1
1 CLOCK
synchronous
with second sweep hand
2
Above door to theatre
(out of patient’s line of sight)
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 108
Quantity Description Group Comments
wall mounted
1 BOARD MARKER
Whiteboard
dry wipe
with pen holder
wall mounted
600H 900W
2
1 BRACKET,
holder, suction unit
trunking mounted
2
1 SUCTION UNIT
Pipeline
high/low pressure
rail/wall mounted
use with BRACKET, holder
3
1 CABINET
Metal
controlled drugs
1 door
lockable
with warning light
wall mounted
550H 600W 3000
3
1 DISPENSER
barrier cream
disposable single cartridge
wall mounted
2
1 DISPENSER
paper towel
wall mounted
2
1 DISPENSER
Medical hand sanitizer 2
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 109
Quantity Description Group Comments
lever action
wall mounted
1 DISPENSER
Soap
disposable single cartridge
lever action
wall mounted
2
1 DISPENSER
disposable gloves set of 3
and disposable apron
wall mounted
2
1 ANAESTHETIC MACHINE/WORKSTATION
electrically powered piston
ventilator
mobile
1350H 750W 650D
3
1 COMPUTER
complete with keyboard
and screen
3
1 HOLDER
Sack
with lid
foot operated
medium
freestanding
875H 430W 385D
3
1 HOLDER
sharps box
up to 7 litre capacity
rail/trolley hang or wall
mounted
170H 125W 100D
3
1 MONITOR 3
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 110
Quantity Description Group Comments
vital signs
multi-parameter
with accessories
280H 360W 215D
1 REFRIGERATOR
medical (drug/vaccine)
capacity 160 litre
external temperature gauge
automatic defrost
lockable
underbench
850H 550W 620D
3
1 STAND
Infusion
twin hook
breaks
mobile
3
1 STOOL
surgeon/anaesthetist
height adjustable
includes anti-static seat pads
3
1 SYRINGE pump
anaesthetic use
with diprifusor
115H 400W 180D
3
1 TROLLEY
dressing/instrument
stainless steel
buffered
870H 450W 450D
3
2049
2050
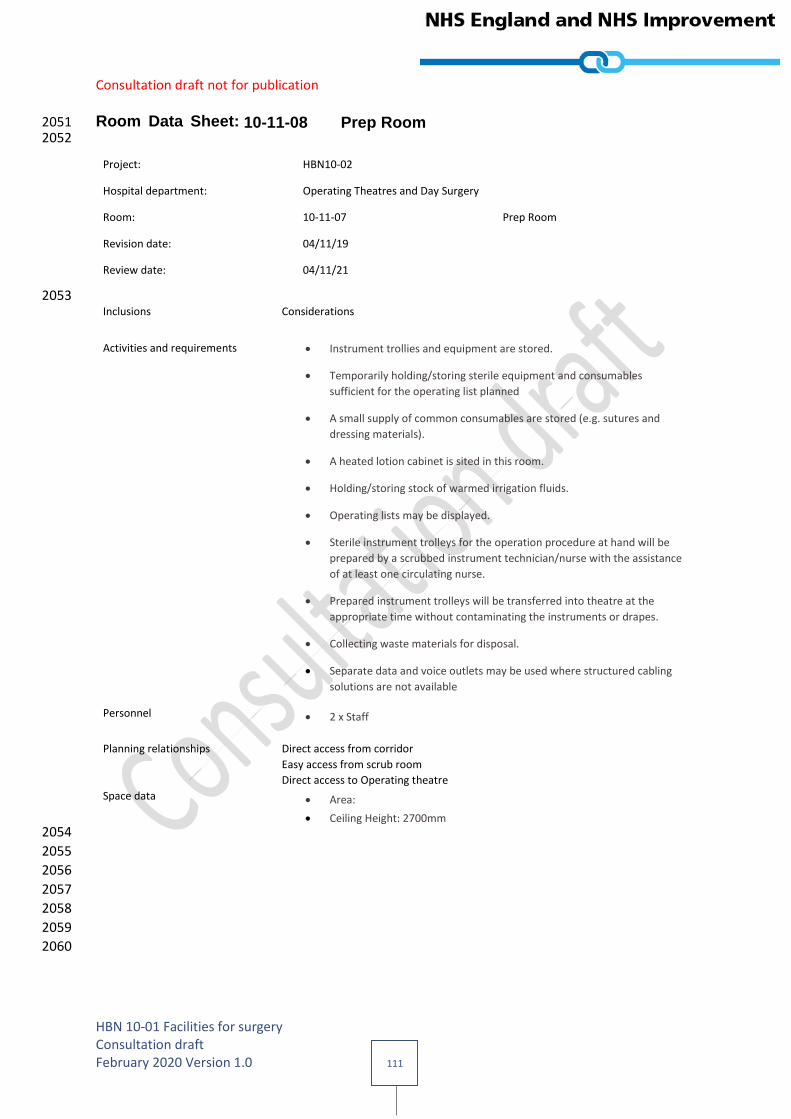
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 111
Room Data Sheet: 10-11-08 Prep Room 2051 2052
Project: HBN10-02
Hospital department: Operating Theatres and Day Surgery
Room: 10-11-07 Prep Room
Revision date: 04/11/19
Review date: 04/11/21
2053 Inclusions Considerations
Activities and requirements Instrument trollies and equipment are stored.
Temporarily holding/storing sterile equipment and consumables
sufficient for the operating list planned
A small supply of common consumables are stored (e.g. sutures and
dressing materials).
A heated lotion cabinet is sited in this room.
Holding/storing stock of warmed irrigation fluids.
Operating lists may be displayed.
Sterile instrument trolleys for the operation procedure at hand will be
prepared by a scrubbed instrument technician/nurse with the assistance
of at least one circulating nurse.
Prepared instrument trolleys will be transferred into theatre at the
appropriate time without contaminating the instruments or drapes.
Collecting waste materials for disposal.
Separate data and voice outlets may be used where structured cabling
solutions are not available
Personnel 2 x Staff
Planning relationships Direct access from corridor
Easy access from scrub room
Direct access to Operating theatre
Space data Area:
Ceiling Height: 2700mm
2054
2055
2056
2057
2058
2059
2060
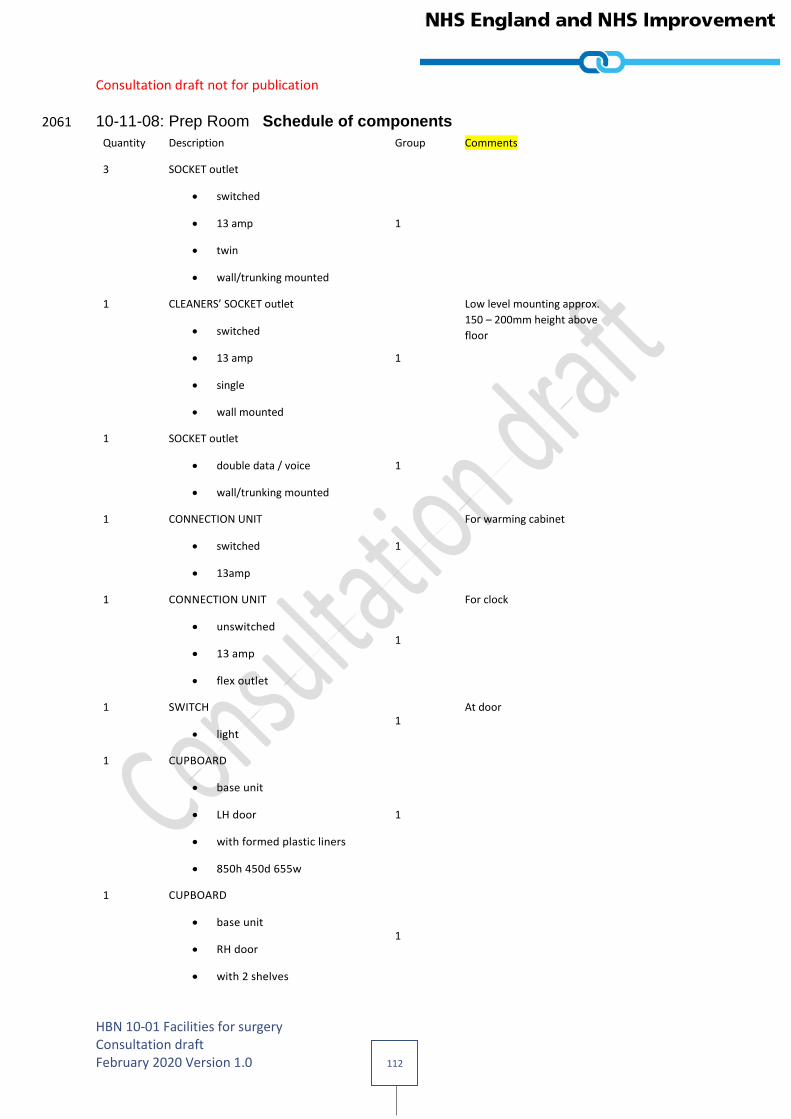
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 112
10-11-08: Prep Room Schedule of components 2061
Quantity Description Group Comments
3 SOCKET outlet
switched
13 amp
twin
wall/trunking mounted
1
1 CLEANERS’ SOCKET outlet
switched
13 amp
single
wall mounted
1
Low level mounting approx.
150 – 200mm height above
floor
1 SOCKET outlet
double data / voice
wall/trunking mounted
1
1 CONNECTION UNIT
switched
13amp
1
For warming cabinet
1 CONNECTION UNIT
unswitched
13 amp
flex outlet
1
For clock
1 SWITCH
light 1
At door
1 CUPBOARD
base unit
LH door
with formed plastic liners
850h 450d 655w
1
1 CUPBOARD
base unit
RH door
with 2 shelves
1

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 113
Quantity Description Group Comments
850h 450d 655w
1 WORKTOP, Clinical
700mm deep,
with 50mm upstand
fixed@ 900mm to top
length as drawn
Support legs SUP1001/1003 as
required
1
1 TRUNKING for power and data
length as drawn 1
Above worktop
1 CLOCK
synchronous
with second sweep hand
wall mounted
2
1 BOARD MARKER
Whiteboard
dry wipe
with pen holder
wall mounted
600H 900W
2
1 CABINET warming,
contrast media and solutions,
stainless steel,
wall mounted
2
1 COMPUTER
complete with keyboard
and screen
3
On worktop
1 READER
Bar Code 3
Connected to PC

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 114
Quantity Description Group Comments
2 HOLDER
Sack
with lid
foot operated
medium
freestanding
875H 430W 385D
3
1 HOLDER
sharps box
up to 7 litre capacity
rail/trolley hang or wall
mounted
170H 125W 100D
3
2 TROLLEY
dressing/instrument
stainless steel
buffered
870H 450W 450D
3
3 TROLLEY
dressing/instrument
stainless steel
buffered
870H 750W 450D
3
1 TROLLEY
instrument tray
MAYO
Height adjustable
650W 450D
3
2 STAND,
lotion bowl,
single,
stainless steel,
(Bowls not included)
3

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 115
Quantity Description Group Comments
2 STAND
Lotion bowl
Double
Stainless steel
(bowls not included)
3
2062
2063
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 116
Useful reading 2064
Ahmad, N., Hussein, A.A., Cavuoto, L., Sharif, M., Allers, J.C., Hinata, N., Ahmad, B., Koslowski, J.D., 2065 Hashmi, Z., Bisantz, A. and Guru, K.A. (2016). “Ambulatory movements, team dynamics and 2066 interactions during robot-assisted surgery”. BJU International, Vol. 118, pp. 132–139. Retrieved from 2067 http://onlinelibrary.wiley.com/doi/10.1111/bju.13426/full 2068
Ambulatory Surgery Center Association. (2016). Retrieved from http://www.ascassociation.org 2069
Andersson, A.E., Bergh, I., Karlsson, J., Eriksson, B.I. and Nilsson, K. (2012). “Traffic flow in the 2070 operating room: an explorative and descriptive study on air quality during orthopedic trauma 2071 implant surgery”. American Journal of Infection Control, Vol. 40, pp. 750–755. Retrieved from 2072 https://tinyurl.com/yb7wbuzq 2073
Andersson, A.E., Petzold, M., Bergh, I., Karlsson, J., Eriksson, B.I. and Nilsson, K. (2014). “Comparison 2074 between mixed and laminar airflow systems in operating rooms and the influence of human factors: 2075 experiences from a Swedish orthopedic center”. American journal of infection control, Vol. 42 No. 6, 2076 pp. 665–669. 2077 https://tinyurl.com/yd3az3jv 2078
Assem, M., Ouda, B. K. and Wahed, M.A. (2012). “Improving operating theatre design using facilities 2079 layout planning”. In Biomedical Engineering Conference (CIBEC), 2012 Cairo International, IEEE, pp. 2080 109–113. 2081
Association of periOperative Registered Nurses. (2015). Guideline for a Safe Environment of Care, 2082 Part 2. Guidelines for Perioperative Practice. AORN, Denver, CO. 2083
Australasian Health Facility Guidelines (2017). Operating Room - General, 42m2. Accessed 22 January 2084 2018. 2085 https://healthfacilityguidelines.com.au/component/operating-room-general-42m2-1 2086
Baillie, J. (2010). “Smoothing the path to the theatre”. Health Estates Journal, Vol. 64 No. 22, pp. 33-2087 37. 2088
Baillie, J. (2012). “Premier performers for the theatre”. Health Estates Journal. August, pp. 55–66. 2089
Bayramzadeh, S., Joseph, A., San, D., Khoshkenar, A., Taaffe, K., Jafarifiroozabadi, R. and Neyens, 2090 D.M. (2018). “The impact of operating room layout on circulating nurse’s work patterns and flow 2091 disruptions: a behavioral mapping study”. HERD: Health Environments Research & Design Journal, 2092 https://doi.org/10.1177/1937586717751124. 22 January 2018. 2093
Berg, R.J., Inaba, K., Sullivan, M., Okoye, O., Siboni, S., Minneti, M. and Demetriades, D. (2015). “The 2094 impact of heat stress on operative performance and cognitive function during simulated 2095 laparoscopic operative tasks”. Surgery, Vol. 157, pp. 87–95. Retrieved from 2096 https://tinyurl.com/y8l6lx69 2097
Birnbach, D.J., Rosen, L.F., Fitzpatrick, M., Carling, P. and Munoz-Price, L.S. (2015). “The use of a 2098 novel technology to study dynamics of pathogen transmission in the operating room”. Anesthesia & 2099 Analgesia, Vol. 120, pp. 844–847. 2100
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 117
Bischoff, P., Kubilay, N.Z., Allegranzi, B., Egger, M. and Gastmeier, P. (2017). “Effect of laminar 2101 airflow ventilation on surgical site infections: a systematic review and meta-analysis”. The Lancet 2102 Infectious Diseases, Vol. 17 No. 5, pp. 553-561. 2103
Brandt, C., Hott, U., Sohr, D., Daschner, F., Gastmeier, P. and Rüden, H. (2008). “Operating room 2104 ventilation with laminar airflow shows no protective effect on the surgical site infection rate in 2105 orthopedic and abdominal surgery”. Annals of Surgery, Vol. 248, pp. 695–700. Retrieved from 2106 https://tinyurl.com/ycaeqhj5 2107
Breier, A., Brandt, C., Sohr, D., Geffers, C. and Gastmeier, P. (2011). “Laminar airflow ceiling size: No 2108 impact on infection rates following hip and knee prosthesis”. Infection Control, Vol. 32, pp. 1097–2109 1102. 2110
British Orthopaedic Association (2014). Helping Consultants Get Things Right. The BOA Advisory 2111 Book. Editor J Dias. The Professional Practice Committee, London. 2112
Brogmus, G., Leone, W., Butler, L. and Hernandez, E. (2007). “Best practices in OR suite layout and 2113 equipment choices to reduce slips, trips, and falls”. AORN Journal, Vol. 86, pp. 384–398. Retrieved 2114 from http://onlinelibrary.wiley.com/doi/10.1016/j.aorn.2007.06.003/full 2115
Burlingame, B. (2015). “FGI Guidelines Update # 3: operating room requirements for 2014 and 2116 beyond”. FGI Guidelines Updates. Retrieved from https://www.fgiguidelines.org/wp-2117 content/uploads/2015/07/FGI_Update_ORs_140915.pdf 2118
Cadenhead, C.D., Waggener, L.T. and Goswami, B. (2017). “The role of architecture and physical 2119 environment in hospital safety design”. In Sanchez, J.A., Barach, P., Johnson, J. and Jacobs, J.P. 2120 (Eds.) Surgical Patient Care, Springer International Publishing, London, pp. 159–183. 2121
Chauveaux, D. (2015). “Preventing surgical-site infections: measures other than antibiotics”. 2122 Orthopaedics & Traumatology: Surgery & Research, Vol. 101, S77–S83. Retrieved from 2123 https://www.sciencedirect.com/science/article/pii/S1877056814003272 2124
Conrad, C., Konuk, Y., Werner, P.D., Cao, C.G., Warshaw, A.L., Rattner, D.W. and Miller, D.L. 2125 (2012). “A quality improvement study on avoidable stressors and countermeasures affecting surgical 2126 motor performance and learning”. Annals of Surgery, Vol. 255, p. 1190. Retrieved 2127 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3354736/ 2128
Dascalaki, E.G., Gaglia, A.G., Balaras, C.A. and Lagoudi, A. (2009). “Indoor environmental quality in 2129 Hellenic hospital operating rooms”. Energy and Buildings, Vol. 41, pp. 551–560. Retrieved from 2130 https://tinyurl.com/yb636b2w 2131
Engelmann, C., Neis, J., Kirschbaum, C., Grote, G. and Benno, M. (2014). “A noise-reduction program 2132 in a pediatric operation theatre is associated with surgeon’s benefits and a reduced rate of 2133 complications: a prospective controlled clinical trial”. Annals of Surgery, Vol. 259, pp. 1025–1033. 2134
Evans, R.P. (2011). “Current concepts for clean air and total joint arthroplasty: laminar airflow and 2135 ultraviolet radiation: a systematic review”. Clinical Orthopedics and Related Research, 469, pp. 945–2136 953. doi:10.1007/s11999-010-1688-7. Retrieved 2137 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3048268/ 2138
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 118
Fischer, S., Thieves, M., Hirsch, T., Fischer, K.D., Hubert, H., Bepler, S. and Seipp, H.M. 2139 (2015). “Reduction of airborne bacterial burden in the or by installation of unidirectional 2140 displacement airflow (UDF) systems”. Medical Science Monitor: International Medical Journal of 2141 Experimental and Clinical Research, Vol. 21, pp. 2367–2374. Retrieved from 2142 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4539998/ 2143
Frabetti, A., Vandini, A., Balboni, P., Triolo, F. and Mazzacane, S. (2009). “Experimental evaluation of 2144 the efficacy of sanitation procedures in operating rooms”. American Journal of Infection Control, Vol. 2145 37, 658–664. Retrieved from https://tinyurl.com/ycwnc6wz 2146
Friedrich, M.G., Boos, M., Pagel, M., Thormann, T., Berakdar, A., Russo, S. and Tirilomis, T. (2017). 2147 “New technical solution to minimise noise exposure for surgical staff: the ‘silent operating theatre 2148 optimisation system’”. BMJ Innovations, Vol. 3 No. 4, pp. 196–205. LOOK ON CHC WEBSITE 2149
Fritsch, M.H., Chacko, C.E. and Patterson, E.B. (2010). “Operating room sound level hazards for 2150 patients and physicians”. Otology and Neurotology, Vol. 31, pp. 715–721. 2151 doi:10.1097/MAO.0b013e3181d8d717. 2152
Gurses, A.P., Kim, G., Martinez, E.A., Marsteller, J., Bauer, L., Lubomski, L.H. and Thompson, D. 2153 (2012). “Identifying and categorising patient safety hazards in cardiovascular operating rooms using 2154 an interdisciplinary approach: a multisite study”. BMJ Quality & Safety, Vol. 21, pp. 810–2155 818. Retrieved from http://qualitysafety.bmj.com/content/21/10/810 2156
Hasfeldt, D., Laerkner, E. and Birkelund, R. (2010). “Noise in the operating room – what do we know? 2157 A review of the literature”. Journal of PeriAnesthesia Nursing, Vol. 25, pp. 380–386. 2158 doi:10.1016/j.jopan.2010.10.001. 2159
Hemphälä, H., Johansson, G., Odenrick, P., Åkerman, K. and Larsson, P.A. (2009). “Lighting 2160 recommendations in operating theatres”. In Proceedings of the 17th World Congress on Ergonomics, 2161 International Ergonomics Association, Zurich. 2162
Hirsch, T., Hubert, H., Fischer, S., Lahmer, A., Lehnhardt, M., Steinau, H.-U. and Seipp, H.-M. 2163 (2012). “Bacterial burden in the operating room: impact of airflow systems”. American Journal of 2164 Infection Control, Vol. 40, e228–e232. 2165
Hooper, G.J., Rothwell, A.G., Frampton, C. and Wyatt, M.C. (2011). “Does the use of laminar flow and 2166 space suits reduce early deep infection after total hip and knee replacement?” Bone & Joint Journal, 2167 Vol. 93, pp. 85–90. Retrieved from http://www.boneandjoint.org.uk/content/jbjsbr/93-2168 B/1/85.full.pdf 2169
Hughes, N.L., Nelson, A., Matz, M.W. and Lloyd, J. (2011). “Solutions for prolonged standing in 2170 perioperative settings”. AORN Journal, 93(6), pp. 767–774. 2171
Indian Health Facility Guidelines (2014a). Operating Room – Minor. Health Facility Briefing System, 2172 Version 2. Accessed 22 January 2018. 2173 http://healthfacilityguidelines.com/StdComps/ViewPDF/HFG-India/ORMS-2174 IN/operating_room_minor_rds 2175
Indian Health Facility Guidelines (2014b). Operating Room – X-Ray Hybrid. Health Facility Briefing 2176 System, Version 2. Accessed 22 January 2018. 2177

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 119
http://healthfacilityguidelines.com/StdComps/ViewPDF/HFG-India/ORXR-2178 IN/operating_room_hybrid_x-ray_rds 2179
International Health Facility Guidelines (2011a). Operating Room. Health Facility Briefing System, 2180 Version 2. Accessed 22 January 2018. 2181 http://healthfacilityguidelines.com/StdComps/ViewPDF/iHFG/OR-HY-CT-2182 I/operating_room_hybrid_ct_scanning_room_rds 2183
International Health Facility Guidelines (2011b). Operating Room – Vascular/Cardiac Imaging. Health 2184 Facility Briefing System, Version 2. Accessed 22 January 2018. 2185 http://healthfacilityguidelines.com/StdComps/ViewPDF/iHFG/OR-VC-2186 I/operating_room_vascular_cardiac_imaging_rds 2187
Jeong, S.J., Ann, H.W., Kim, J.K., Choi, H., Kim, C.O., Han, S.H. and Yeom, J.-S. (2013). “Incidence and 2188 risk factors for surgical site infection after gastric surgery: a multicenter prospective cohort study”. 2189 Infection & Chemotherapy, Vol. 45, 422–430. Retrieved from 2190 https://synapse.koreamed.org/search.php?where=aview&id=10.3947/ic.2013.45.4.422&code=0086I2191 C&vmode=FULL 2192
Joseph, A., Bayramzadeh, S., Zamani, Z. and Rostenberg, B. (2017). “Safety, performance, and 2193 satisfaction outcomes in the operating room”. HERD: Health Environments Research & Design 2194 Journal, https://doi.org/10.1177/1937586717705107, 24 April, pp. 1–14. 2195
Katz, J.D. (2014). “Noise in the operating room”. Anesthesiology, Vol. 121, pp. 894–898. 2196 doi:10.1097/ALN.0000000000000319. Retrieved 2197 from http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1921569&resultclick=1 2198
Keller, S., Tschan, F., Beldi, G., Kurmann, A., Candinas, D. and Semmer, N.K. (2016). “Noise peaks 2199 influence communication in the operating room: an observational study”. Ergonomics, Vol. 59, pp. 2200 1541–1552. doi:10.1080/00140139.2016.1159736. 2201
Kelts, G.I., McMains, K.C., Chen, P.G. and Weitzel, E.K. (2015). “Monitor height ergonomics: a 2202 comparison of operating room video display terminals”. Allergy & Rhinology, Vol. 6, e28. Retrieved 2203 from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4388873/ 2204
Knulst, A.J., Mooijweer, R., Jansen, F.W., Stassen, L.P. and Dankelman, J. (2011). “Indicating 2205 shortcomings in surgical lighting systems”. Minimally Invasive Therapy & Allied Technologies, Vol. 2206 20, pp. 267–275. Retrieved from https://tinyurl.com/y84a7tqj 2207
Kracht, J.M., Busch-Vishniac, I.J. and West, J.E. (2007). “Noise in the operating rooms of Johns 2208 Hopkins Hospital”. The Journal of the Acoustical Society of America, Vol. 121, pp. 2673–2209 2680. Retrieved from https://tinyurl.com/yczjxz4x 2210
Kümin, M. and Scarborough, M. (2017). “Laminar flow ventilation during surgery”. The Lancet 2211 Infectious Diseases, Vol. 17 No. 6, p. 581. 2212
Kurmann, A., Peter, M., Tschan, F., Mühlemann, K., Candinas, D. and Beldi, G. (2011). “Adverse effect 2213 of noise in the operating theatre on surgical-site infection”. British Journal of Surgery, Vol. 98, pp. 2214 1021–1025. 2215

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 120
Lee, K. (2015). “Designing the OR of the future”. Healthcare Design. Retrieved from 2216 http://www.healthcaredesignmagazine.com/trends/construction-engineering/designing-or-future/ 2217
Leest, L.V., Kawczynski, R., Lipp, F.E. and Barrientos, R. (2012). “Identifying potential areas of 2218 infectivity on high-touch locations in the OR”. AORN Journal, Vol. 96, pp. 507–512. Retrieved from 2219 http://onlinelibrary.wiley.com/doi/10.1016/j.aorn.2012.07.012/full 2220
Loomans, M.G.L.C., de Visser, I.M., Loogman, J.G.H. and Kort, H.S.M. (2016). “Alternative ventilation 2221 system for operating theaters: parameter study and full-scale assessment of the performance of a 2222 local ventilation system”. Building and Environment, Vol. 102, pp. 26–38. 2223 doi:10.1016/j.buildenv.2016.03.012. Retrieved from 2224 https://pure.tue.nl/ws/files/17124020/LoomansAlternative2016.pdf 2225
Lynch, R.J., Englesbe, M.J., Sturm, L., Bitar, A., Budhiraj, K., Kolla, S. and Campbell, D.A. 2226 (2009). “Measurement of foot traffic in the operating room: implications for infection control”. 2227 American Journal of Medical Quality, Vol. 24, pp. 45–52. doi:10.1177/1062860608326419. Retrieved 2228 from https://tinyurl.com/ya4t6bay 2229
Matern, U. and Koneczny, S. (2007). “Safety, hazards and ergonomics in the operating room”. 2230 Surgical Endoscopy, Vol. 21, pp. 1965–1969. Retrieved from https://tinyurl.com/ydceusw6 2231
McNeer, R.R., Bennett, C.L. and Dudaryk, R. (2016). “Intraoperative noise increases perceived task 2232 load and fatigue in anesthesiology residents: a simulation-based study”. Anesthesia & Analgesia, Vol. 2233 122, pp. 2068–2081. doi:10.1213/ane.0000000000001067. 2234
Memarzadeh, F. and Manning, A.P. (2002). “Comparison of operating room ventilation systems in 2235 the protection of the surgical site”. ASHRAE Transaction: Research, Vol. 108, pp. 3–15. Retrieved 2236 from https://www.orf.od.nih.gov/policiesandguidelines/bioenvironmental/documents/ashrae_final_2237 operating_room_508.pdf 2238
Miner, A.L., Losina, E., Katz, J.N., Fossel, A.H. and Platt, R. (2007). “Deep infection after total knee 2239 replacement: impact of laminar airflow systems and body exhaust suits in the modern operating 2240 room”. Infection Control, Vol. 28, pp. 222–226. 2241
Mousavi, E.S. and Grosskopf, K.R. (2016). “Airflow patterns due to door motion and pressurization in 2242 hospital isolation rooms”. Science and Technology for the Built Environment, Vol. 22, pp. 379–384. 2243 doi:10.1080/23744731.2016.1155959. 2244
Namba, R.S., Inacio, M.C.S. and Paxton, E.W. (2012). “Risk factors associated with surgical site 2245 infection in 30,491 primary total hip replacements”. Journal of Bone & Joint Surgery, British Volume, 2246 Vol. 94-B, pp. 1330–1338. doi:10.1302/0301-620x.94b10.29184. Retrieved from 2247 http://www.boneandjoint.org.uk/content/jbjsbr/94-B/10/1330.full.pdf 2248
National Institute for Health and Clinical Excellence. (2016). Clinical Guideline 65: “Hypothermia: 2249 prevention and management in adults having surgery”. NICE. 2250 https://www.nice.org.uk/guidance/cg65/resources/hypothermia-prevention-and-management-in-2251 adults-having-surgery-pdf-975569636293 2252
Okoro, S.A., Patel, T.H. and Wang, P.T. (2007). “Who needs the surgical headlight?” The Cleft Palate–2253 Craniofacial Journal, Vol. 44, pp. 126–128. 2254

Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 121
Oliver, L. (2017). “Meet the nurse who will soon perform surgery on patients alone”. The Guardian. 2255 30 August. 2256 https://www.theguardian.com/healthcare-network/2017/aug/30/nurse-perform-surgery-patients-2257 alone-surgical-care-practitioner 2258
Palmer, G., Abernathy, J.H., Swinton, G., Allison, D., Greenstein, J., Shappell, S. and Reeves, S.T. 2259 (2013). “Realizing improved patient care through human-centered operating room design: a human 2260 factors methodology for observing flow disruptions in the cardiothoracic operating room”. 2261 Anesthesiology, Vol. 119, pp. 1066–1077. Retrieved from 2262 http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1918091 2263
Patkin, M. (2003). “What surgeons want in operating rooms”. Minimally Invasive Therapy & Allied 2264 Technologies, Vol. 12, pp. 256–262. 2265
Pym, H. (2017, October 24). “How operating theatres are wasting two hours a day”. Retrieved 22 2266 January 2018 from http://www.bbc.co.uk/news/health-41727535 2267
Rostenberg, B. and Barach, P.R. (2011). “Design of cardiovascular operating rooms for tomorrow's 2268 technology and clinical practice – Part one”. Progress in Pediatric Cardiology, 32(2), pp. 121–128. 2269
Rostenberg, B. and Barach, P.R. (2012). “Design of cardiovascular operating rooms for tomorrow's 2270 technology and clinical practice – Part 2”. Progress in Pediatric Cardiology, 33(1), pp. 57–65. 2271
Rostenberg, B. and, Barach, P.R. (2014). “Design of cardiac surgery operating rooms and the impact 2272 of the built environment”. In Barach, P., Jacobs, J., Laussen, P. and Lipshultz, S. (Eds.). Outcomes 2273 Analysis, Quality Improvement, and Patient Safety for Pediatric and Congenital Cardiac Disease. 2274 Springer Books, New York. 2275
Royal College of Surgeons (2007). Delivering surgical services: options for maximising resources. RCS, 2276 London. 2277
Royal College of Surgeons (2016). A Question of Balance: The Extended Surgical Team. RCS, London. 2278
Salassa, T.E. and Swiontkowski, M.F. (2014). “Surgical attire and the operating room: role in infection 2279 prevention”. The Journal of Bone & Joint Surgery, Vol. 96, pp. 1485–1492. 2280
Scaltriti, S., Cencetti, S., Rovesti, S., Marchesi, I., Bargellini, A. and Borella, P. (2007). “Risk factors for 2281 particulate and microbial contamination of air in operating theatres”. Journal of Hospital Infection, 2282 Vol. 66, pp. 320–326. 2283
Shambo, L., Umadhay, T. and Pedoto, A. (2015). “Music in the operating room: is it a safety 2284 hazard?” American Association of Nurse Anesthetists Journal, Vol. 83, pp. 43–48. 2285
Siu, K., Suh, I., Mukherjee, M., Oleynikov, D. and Stergiou, N. (2010). “The impact of environmental 2286 noise on robot-assisted laparoscopic surgical performance”. Surgery, Vol. 147, pp. 107–2287 113. Retrieved from https://tinyurl.com/y78lp6oc 2288
Smyth, E.T M., Humphreys, H., Stacey, A., Taylor, E.W., Hoffman, P. and Bannister, G. (2005). “Survey 2289 of operating theatre ventilation facilities for minimally invasive surgery in Great Britain and Northern 2290 Ireland: current practice and considerations for the future”. Journal of Hospital Infection, Vol. 61 No. 2291 2, pp. 112–122. 2292
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 122
Spagnolo, A.M., Ottria, G., Amicizia, D., Perdelli, F. and Cristina, M.L. (2013). “Operating theatre 2293 quality and prevention of surgical site infections”. Journal of Preventive Medicine and Hygiene, Vol. 2294 54, pp. 131–137. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4718372/ 2295
Stevenson, R.A., Schlesinger, J.J. and Wallace, M.T. (2013). “Effects of divided attention and 2296 operating room noise on perception of pulse oximeter pitch changes: a laboratory study”. 2297 Anesthesiology, Vol. 118, pp. 376–381. doi:10.1097/ALN.0b013e31827d417b. Retrieved from 2298 http://anesthesiology.pubs.asahq.org/article.aspx?articleid=1918694 2299
Stocks, G.W., O’Connor, D.P., Self, S.D., Marcek, G.A. and Thompson, B.L. (2011). “Directed air flow 2300 to reduce airborne particulate and bacterial contamination in the surgical field during total hip 2301 arthroplasty”. The Journal of Arthroplasty, Vol. 26, pp. 771–776. Retrieved from 2302 http://www.s2i.co.jp/product/nimbicsystems/img/reference01.pdf 2303
Thiele, R.H., Huffmyer, J.L. and Nemergut, E.C. (2008). “The ‘six sigma approach’ to the operating 2304 room environment and infection”. Clinical Anaesthesiology, Vol. 22, pp. 537–552. 2305
Tsiou, C., Efthymiatos, G. and Katostaras, T. (2008). “Noise in the operating rooms of Greek 2306 hospitals”. The Journal of the Acoustical Society of America, Vol. 123, pp. 757–765. 2307
Wahr, J., Prager, R., Abernathy, J.H., Martinez, E., Salas, E., Seifert, P. and Nussmeier, N. 2308 (2013). “Patient safety in the cardiac operating room: human factors and teamwork”. Circulation, 2309 Vol. 128, pp. 1139–1169. Retrieved from http://circ.ahajournals.org/content/128/10/1139 2310
Watkins, N., Kobelja, M., Peavey, E., Thomas, S. and Lyon, J. (2011). “An evaluation of operating 2311 room safety and efficiency: pilot utilization of a structured focus group format and three-2312 dimensional video mock-up to inform design decision making”. Health Environments Research & 2313 Design Journal, Vol. 5, pp. 6–22. 2314
Way, T.J., Long, A., Weihing, J., Ritchie, R., Jones, R., Bush, M. and Shinn, J.B. (2013). “Effect of noise 2315 on auditory processing in the operating room”. Journal of the American College of Surgeons, Vol. 2316 216, pp. 933–938. Retrieved from http://www.journalacs.org/article/S1072-7515(13)00044-2317 6/fulltext 2318
Weerakkody, R.A., Cheshire, N.J., Riga, C., Lear, R., Hamady, M.S., Moorthy, K. and Bicknell, C.D. 2319 (2013). “Surgical technology and operating-room safety failures: a systematic review of quantitative 2320 studies”. BMJ Quality & Safety, Vol. 22, pp. 710–718. Retrieved from https://tinyurl.com/y7jxeozl 2321
Wheelock, A., Suliman, A., Wharton, R., Babu, E., Hull, L., Vincent, C. and Arora, S. (2015). “The 2322 impact of operating room distractions on stress, workload, and teamwork”. Annals of Surgery, Vol. 2323 261, pp. 1079–1084. Retrieved from https://tinyurl.com/ya66eb4k 2324
“Why we need new short stay surgery facilities?” (n.d.). Retrieved 22 January 2018 from 2325 https://www.uclh.nhs.uk/aboutus/NewDev/NCF/Pages/Whyweneednewshortstaysurgeryfacilities.as2326 px 2327
Wiegmann, D., ElBardissi, A., Dearani, J., Daly, R. and Sundt, T. (2007). “Disruptions in surgical flow 2328 and their relationship to surgical errors: an exploratory investigation”. Surgery, Vol. 142, pp. 658–2329 665. 2330
Consultation draft not for publication
HBN 10-01 Facilities for surgery Consultation draft February 2020 Version 1.0 123
World Health Organization (2009). WHO Guidelines for Safe Surgery. Safe Surgery Saves Lives. 2331 Retrieved 2332 from http://www.who.int/patientsafety/safesurgery/tools_resources/9789241598552/en/ 2333
Young, R.S. and O’Regan, D.J. (2010). “Cardiac surgical theatre traffic: time for traffic calming 2334 measures?” Interactive Cardiovascular and Thoracic Surgery, Vol. 10, pp. 526–529. Retrieved from 2335 https://pdfs.semanticscholar.org/c40c/d12cfbd4a2169d1ff94715963d935d351c90.pdf 2336
2337







