
2012 Performance Assessment and Improvement Report 1
Pullman Regional Hospital
2012 Annual Performance
Assessment & Improvement Report

2012 Performance Assessment and Improvement Report 2
Values:
personal integrity and commitment to provide compassionate, responsible, quality ser-
vices to our community
an environment that allows individuality, team work, and communication to flourish
the enriching nature of diversity, creativity, and innovation
honesty and leadership in an atmosphere of mutual respect and trust.
Vision:
Pullman Regional Hospital is a community leader of integrated health and healing activities
where our values guide and inspire, and science and technology quietly enable people to
comfort, encourage, and heal.
Mission:
Pullman Regional Hospital exists to nurture and facilitate a healthier quality of life for our
community.
Customer Service Philosophy:
Each of us at Pullman Regional Hospital is sincerely interested in exceeding the expecta-
tions of others in a courteous, respectful, and friendly manner. We accept personal respon-
sibility to understand each person’s needs and provide individualized service.
Patient Care Philosophy:
It is our belief that all individuals are active partners in their own health and healing activi-
ties. This is supported by a flexible care environment where information is shared while
participation and personal choice are encouraged.

2012 Performance Assessment and Improvement Report 3
Page
Organizational Responsibility 6-13
Strategic Planning
Community Health 2020 and “Generosity Inspires”
Governing Board Committee Activities
Regulatory Compliance
Corporate Compliance
Occupational Safety and Health
Healthcare Portability and Accountability Act
Joint Commission Accreditation
Centers for Medicare and Medicaid Validation Survey
Medical Staff
Recruitment and Retention
Electronic Focused and Ongoing Professional Performance Evaluation
Physician Leadership Council
Organizational Ethics
Superior Clinical Outcomes 14-23
Culture of Safety : “Just Culture”
National Patient Safety Goals
Medication Safety
Influenza Prevention Program
Infection Prevention
At Pullman Regional Hospital, our Strategic Focus Areas provide
direction for our efforts in supporting our mission, moving to-
ward our vision, and being consistent with our values. Strategic
objectives and organizational initiatives offer the operational
roadmap for ongoing progress towards our future within a cul-
ture of performance measurement and continuous improve-
ment.
2012 — Continuing the Quest for Quality

2012 Performance Assessment and Improvement Report 4
Page
Unexpected Outcomes Management
Elective Deliveries
Fall Prevention
Communication of Critical Values
CO2 Monitoring
Medical Staff PI
Customer Loyalty and Satisfaction 24-26
Inpatient and Outpatient Satisfaction
Customer Satisfaction Assessment
Community Engagement
Community Education — Washington State Libraries
Volunteers and Auxiliary
Pet Partnerships
Employee Engagement 27-31
New Employee Orientation
Employee Retention and Turnover
“Specialty Certification
“Passport to Growth”
Crisis Prevention Institute Training
Staff and Physician Recognition
Leadership and Skills Development
Financial Effectiveness 32-35
2012 Year-End Recap
Statement of Operations
Vital Signs

2012 Performance Assessment and Improvement Report 5
Page
Productivity Standards
Utilization Management
Partnerships and Collaboration 36-40
Clinical Informatics
Computerized Provider Order Entry
Physician Documentation
Nursing Documentation
“Meaningful Use”
Health Information Management Systems (HIMSS 13)
Achievement Award
Information Technology
Medical Office EMR Implementation
“Most Wired” Awards
WSHA Partnerships for Patients
Nutrition Counseling
INBC Blood Center
Electronic Learning/Education Programming
New and Improved Services and Products 41
Magnetic Resonance Imaging (MRI) Upgrade
da Vinci Robotic Surgical System
Electroconvulsive Therapy
Evaluation of the 2012 Performance Assessment and Improvement Program 42
2012 Performance Assessment and Improvement Report 6
Strategic Planning Process
Our overall strategy is to create outcomes that, over time, will reflect the following attributes:
We are regarded as a healthcare leader in our region.
The services available in our region are integrated and collaborative and address health and healing en-deavors.
There is a comprehensive care community on Bishop Boulevard.
We are considered a preferred healthcare organization by physicians, staff, and patients by assuring that:
The values we espouse as an organization truly serve as an inspiration for everyone that associates with the hospital;
We continually upgrade our science and technology which further promotes a quiet, healing envi-ronment;
The people providing the care and services sincerely feel they are supported and trained to com-fort, encourage, and heal;
The quality of life in our community is healthier.
In order to connect our overall strategy with our operating activities, we have adopted three imperatives that guide our efforts:
Continuing emphasis on our quality improvement culture;
Strengthening market share in the region;
Recruiting and retaining high quality physicians, hospital staff, and other providers.
The following six Strategic Focus Areas will sharpen our strategic planning:
Developing and/or changing, and implementing precise and rigorous systems to produce superior clinical outcomes;
Assessing and improving the level of customer loyalty across all customer groups on an ongoing basis;
Developing processes to enhance employee engagement;
Improving the efficiency and financial performance of the hospital;
Developing partnerships and seeking collaborative opportunities that improve our capacity to better serve our community;
Creating and implementing new and/or improved services and products.
In June, the annual planning session was facilitated by Leanne Kaiser Carlson, who is one of the principle own-ers of the Kaiser Philanthropy Institute. Our efforts for this session identified the inclusion of generosity and its many facets as a core focus for developing a new model in healthcare delivery. We continued these efforts throughout 2012 (see page 8).
Organizational Responsibility

2012 Performance Assessment and Improvement Report 7
Strategic Planning Process
Organizational Responsibility

2012 Performance Assessment and Improvement Report 8
Strategic Planning
Community Health 2020 and Generosity Inspires
In 2012, considerable focus and attention went to planning for COMMUNITY HEALTH 2020 and Generosity In-spires efforts. Community Health 2020 is the plan by which Pullman Regional Hospital aspires to be the most successful small community hospital in the Pacific Northwest. The central goal is to create a self-sustaining, self-determining, inclusive model for healthcare in our community. We want to serve as an inspiration for transformational leadership, leading edge facilities and technology, and healthcare innovation. We want to create a new model of healthcare that builds upon our quality acute care and medical services by incorpo-rating the principles of “population health” and an integrated model of care. Population health focuses on prevention, health management and care coordination. By doing this we will improve individual health status and raise the level of community wellness, assure that medical facilities, technology, and expertise remain at the forefront of care, and that each person touched through their relationship with Pullman Regional Hospital will feel a positive impact in their life.
Creating a self-sustaining, self-determining, inclusive model for healthcare captures the foundational compo-nent of COMMUNITY HEALTH 2020. In order to assure a self-sustaining future a hospital must have a positive margin in order to maintain essential public services upon which all communities depend. Without alternative funding sources in the future, and with a dwindling financial margin, Pullman Regional Hospital will face the dire prospect of dramatically reducing or eliminating essential services for our community. Our plan is to build an Endowment for Quality and Access which will enable us to continue providing the high quality medical ser-vices we now deliver along with building a Community Health & Leadership Pavilion. The Pavilion would house two centers: The Center for Learning & Innovation and The Center for Women’s & Children’s Health. These centers will be developed to address our goal of improving the health of large populations through innovation, health management and prevention.
We spent 2012 preparing for this endeavor with an investment in building the Pullman Regional Hospital Foun-dation infrastructure. This began with the recruitment and appointment of Rueben Mayes as the Chief Devel-opment Officer for Pullman Regional Hospital. He and his staff will be tasked with raising private and grant funding to achieve Community Health 2020. Equally as important is the cultural shift the hospital must make in contributing to our goal. Generosity Inspires is a way that employees and the community can see how gener-ous acts fuel the organization’s philanthropic and transformational goals and to actively participate in this work. Megan Guido was appointed to carry out Generosity efforts in concert with the Community Health 2020 work. This will include story-telling, building cultural awareness of the role of philanthropy and giving in our work with patients and the community, and growing our hospital volunteer program as well as volunteerism in the community to improve health and wellness. Additionally, she will work spearheading pilot programs in healthcare innovation and strategic planning.
Organizational Responsibility
2012 Performance Assessment and Improvement Report 9
Governing Board Committee Activities
Quality Improvement Committee (QIC):
The QIC provided oversight for performance assessment and improvement activities. It monitored the Supe-
rior Clinical Outcomes Dashboard, Medical Staff Report, and Customer Service Dashboard quarterly. The Uti-
lization Review Dashboard was introduced in 2012. Areas of focus continued to be patient safety with an em-
phasis on the timely communication of critical tests and values, immunizations, infection prevention, evi-
dence-based clinical management, and patients with respiratory compromise.
Strategic Planning Committee:
The Strategic Planning Committee provided support and guidance in the hospital’s strategic initiatives, in-
cluding the expansion of Palouse Surgeons into a broader Palouse Specialties organization which would in-
corporate other medical specialties in the planning for future hospital and community needs. Areas of focus
included physician recruitment, long term care considerations, property acquisition feasibility, and the annu-
al strategic planning session. The committee received an update on the Critical Access Hospital Coalition,
which was formed to address the concerns regarding federal legislature proposals relating to Critical Access
Hospitals within 10 miles of another hospital, and the Circle of Care efforts to re-establish adult day health
services in the region.
Governance Committee:
The Governance Committee of the Board of Commissioners continued their work in a variety of are-
as. Ongoing efforts focused on the Board’s self-evaluation process and education activities, CEO evaluation,
bylaws and policies, committee structure, compliance and HIPAA updates, and succession planning.
Organizational Responsibility

2012 Performance Assessment and Improvement Report 10
Governing Board Committee Activities
Finance Committee:
The Finance Committee’s primary purpose is the ongoing re-
view and discussion of the financial operation of the Hospital
District. Monthly, the committee discusses the financial analy-
sis of the hospital, clinic network, and joint ventures. Along
with this review, the Finance Committee undertook several
other key focuses in 2012. Below is a brief summary of a few
of those efforts:
Review and discussion of U.S. Bank covenant require-
ments, action plan, and refunding of the bonds in 2015 at
call-date.
Reviewed various future bond financing options.
Reviewed property insurance bids and selection of vendor to cover the District’s assets.
Reviewed professional liability bids and selection.
Discussed funding options and priority for Imaging Services regarding CT versus MRI.
Analysis of historical review of the District’s collection process and recap of claims filed for the prior year.
The committee reviewed the previously discussed information on ratios and benchmarking, recommend-
ing to the Board that they establish certain ratio goals for the next couple years.
Developed budget goals for ensuing year.
Evaluated the impact on the facility should the loss of CAH occur at the Federal level and established a
recommendation to join a CAH 10-mile coalition.
Reviewed new services that were established in 2011 (e.g., new Nuclear Medicine machine, Genetic
Counseling Services, daVinci Robotic Assisted Surgery)
Analyzed the impact of the 2012 price study.
Pullman Regional Hospital recognizes and appreciates all of the
Commissioners for their commitment, time, and effort.
Organizational Responsibility

2012 Performance Assessment and Improvement Report 11
Corporate Compliance
In 2012 the Corporate Compliance Committee continued its efforts to ensure that Pullman Regional Hospital
was in compliance with federal and state laws. The committee continued to focus upon
priority areas including clarification of appropriate admission status, nursing and physi-
cian documentation, education, and billing practices.
In addition, the Utilization Review (UR) Committee provided leadership for all utilization
management efforts (see page 37). Milliman Care Guidelines are continuing to be used
for clinical management and guidance in terms of goal-setting for patients. The Rural
Healthcare Quality Network physician advisor reviews charts on a quarterly basis and
offers feedback to the physicians regarding utilization of services as well as clinical man-
agement.
A Chargemaster review was conducted, and in response to recommendation, all charge sheets were re-
viewed and revised in terms of “level charges”. In addition, a Medicare/Medicaid audit was conducted. The
hospital is still awaiting final results.
Planned areas of focus for 2013 include:
Organizational Responsibility
Occupational Safety and Health
In 2012, the Safe Patient Handling Team, with the assistance of Donna Haynes, updated our educational method to be used in 2013 and future years. All equipment videos have been placed on Healthstream as well as a Safe Patient Handling course to be viewed by all employees who handle patients. They will also be required to do a return demonstration. In 2012, the training was primarily done one-on-one with staff mem-bers and had moderate success.
The Hovermatt was added to our patient handling equipment in the ED and we initiated the use of a dispos-able transfer and repositioning sheet called the Z-slider on the units. These are kept in the nurse pass-throughs. The ED also obtained a new stretcher that can hold up to 700 lbs. for use in caring for bariatric patients. A bariatric shower bench that holds 500 lbs. was obtained in MSU.
The nurse managers were educated in doing root cause analysis (RCA) for employee injuries and patient falls as we are required by our workers’ comp trust to conduct these RCA’s. For those incidents of employee injuries that had occurred prior to this training, Bernadette Berney and Connie Koal completed the RCA’s in conjunction with information obtained from the managers. RCA information on employee injuries and pa-tient injuries was reported to the Safe Patient Handling Committee and input was sought on prevention strategies.
In October 2012, the Environment of Care/Safety Committee announced that Pullman Regional Hospital was the recipient of a Top Performer Award from our Workers’ Compensation Program. The award is in recogni-tion of our dedication to the safety and health of our employees. The hospital received a plaque and $5000 to be used to enhance our continued efforts to provide a safe work environment for our employees.
Lengths of Stay exceeding 4 days Outpatient observation services
Swing bed utilization Information patients of observation service
Inpatient and outpatient payments Sleep studies
2012 Performance Assessment and Improvement Report 12
Joint Commission Accreditation
Centers for Medicare and Medicaid Validation Survey
In May 2012, the Department of Health conducted an unannounced validation survey of the hospital’s Criti-
cal Access designation following the Joint Commission survey. Hospitals are chosen at random to undergo
this survey in order to validate findings from the Joint Commission. Additional findings may also be identi-
fied. All findings have been corrected and no additional action is required.
The Joint Commission conducted its triennial unannounced survey in March 2012.
Pullman Regional Hospital achieved full accreditation requirements for improvement
in the areas of safety and life safety, documentation, and medication management.
Process improvements were implemented and all requirements have been removed
from the hospital’s accreditation status. The Joint Commission lab survey is expected
in 2013.
Healthcare Insurance Portability & Accountability Act (HIPAA)
In 2012, the HIPAA Committee continued its efforts to ensure compliance with federal regulations relating to
patient privacy and confidentiality. Education was provided to staff at New Employee Orientation, which in-
cluded review of regulations associated with HIPAA and the Hi-Tech Rule, areas of potential risk, mitigation
strategies to manage the risk, hospital resources and the breach investigation process. Software to “detect”
potential breaches was also purchased and system administrators were trained. The hospital is required to
conduct proactive audits on a regular basis as part of the Hi-Tech Rule. Implementation is scheduled for ear-
ly 2013.
Organizational Responsibility

2012 Performance Assessment and Improvement Report 13
2012 Medical Staff Activities
Medical Staff Recruitment and Retention:
In continuing our efforts to identify and respond to community needs for healthcare, 2012 was very success-
ful for recruitment efforts. Dr. Geoff Stiller returned to the Palouse and established a practice in general and
cosmetic surgery. In addition, Dr. Nigel Campbell joined the obstetrics/gynecology practice. Two new emer-
gency physicians also joined the physician group at Pullman Regional Hospital. In 2013, recruitment efforts
will continue to be focused upon internal medicine and orthopedic surgery.
Electronic Focused and Ongoing Professional Performance Evaluation:
In 2012, the Family Medicine Committee piloted a process for ongoing chart review and professional perfor-
mance review through the electronic medical record. Findings and recommendations were also completed
and submitted electronically. It will be introduced to the other medical staff committees in 2013.
Physician Leadership Council (PLC):
A Physician Leadership Council was organized in 2011, with initial efforts focused upon developing their role
and areas of focus in better serving the medical community and supporting Pullman Regional Hospital. The
membership has expanded to nine physicians and they have recently identified several areas that merit their
ongoing energy in order to further develop medical services in the community. In 2012, strategic objectives
were established:
Community: Clinics/services offered to the community (i.e. Medical Neighborhood) may include public fo-rums by the PLC.
Hospital: Act as sounding board for providers and the community, may include prioritizing capital purchases and consideration of ways to share services to increase efficiencies.
Physician Practices: Influence/resolve issues within the medical community including how to support local practices/providers.
Organizational Responsibility
Ethics Committee: This interagency/interdisciplinary committee is a resource for hospital employees, physi-
cians, and patients and their families to assist in dealing with ethical and moral issues. As a member of the
committee, Bill Kabasenche, PhD., a WSU bioethics professor, has provided expertise and facilitation of case
reviews in the consideration of actual and potential issues relating to informed consent, end-of-life decisions,
power of attorney and other topics.
The committee has four areas of focus:
Identification of potential and actual ethical issues and providing recommendations;
Education for staff and medical staff regarding ethical issues;
Policy development;
Consultation concurrently and retrospectively to offer clarity in dealing with specific situations. Decision-making is the responsibility of the individual(s) involved.
Organizational Ethics

2012 Performance Assessment and Improvement Report 14
Commitment to Patient Safety : Pullman Regional Hospital is committed to creating and sustaining a work
environment where patient safety is consistently a top priority. This environment demonstrates a commit-
ment to designing policies and processes to prevent errors, providing appropriate numbers of qualified staff,
encourage event reporting, learning from errors, and commitment to continuous improvement. The core
principles include: maintaining a safe reporting environment; identifying individual and leadership respon-
sibilities; understanding errors and effectively responding; and the timely and effective response in the
event of a significant error.
In 2011, a second Culture of Safety survey was conducted with hospital and medical staff. Two areas of fo-
cus were identified: creating a safe environment for reporting errors and creating a non-punitive response to
errors (see below). In addition to identifying areas of focus for 2012, four areas of strength were also identi-
fied: overall perception of patient safety, teamwork within departments, supervisors promoting patient safe-
ty, and appropriate staffing levels. In all of these areas, Pullman Regional Hospital ranks at or above the 90th
percentile as compared with the national database.
In order to address these two focus areas identified for improvement, the Patient Safety Team developed a
“Commitment to Patient Safety” and refined the “Just Culture” algorithm for responding to errors and unex-
pected events. Hospital staff were included in the development of these tools. In addition, the Patient Safety
Team utilized the revised algorithm in reviewing cases in order to become more consistent in the application
in distinguishing between systems vs. human issues and the appropriate response.
Culture of Safety
Superior Clinical Outcomes Superior Clinical Outcomes
Safety Culture Composites
Pullman Regional
Hospital 2009 (n=74)
Pullman Regional
Hospital 2011
(n=314)
90th Percentile 2011
National Database
(1032 hospitals)
Overall Perceptions of Safety 74% 78% 76%
Frequency of Events Reported 53% 60% 72%
Manager Actions Promoting Safety 83% 80% 83%
Organizational Learning 71% 73% 82%
Teamwork w/in Departments 85% 86% 87%
Communication Openness 73% 69% 71%
Feedback and Communication About Error 63% 65% 75%
Nonpunitive Response to Error 49% 52% 55%
Staffing 71% 78% 68%
Hospital Management Support for Safety 78% 86% 84%
Teamwork Across Hospital Departments 64% 75% 72%
Hospital Handoffs and Transitions 52% 59% 60%

2012 Performance Assessment and Improvement Report 15
Superior Clinical Outcomes
Knowledge Deficit Barriers Identified Failure to adhere to
policy/procedure
Problem Identified
Educate Remove Barriers
Management
intervention
Consider which human behavior
category is appropriate
Yes Yes Yes
No No
First time occurrence;
inadvertently doing other than
what should have been done:
Lapse in judgment or a mistake
Repeated occurrence(s); a
choice that increases risk
where risk is not recognized or
is mistakenly believed to be
justified
Risk-taking with conscious
disregard of a substantial or
unjustified risk
Manage through changes
in process, procedures,
design, and environment.
Set clear expectations for
performance.
Accountable Discipline
– performance
improvement plan or
reminder 1
Accountable Discipline –
Reminder 1, 2, Day of
Decision or Termination
Coach; Educate
Console if appropriate
Coach; Educate
Performance improvement or reminder 1
Discipline
Human Error
At-Risk Behavior
Reckless Behavior
Human Behavior Categories
Problem Algorithm
2012 Performance Assessment and Improvement Report 16
National Patient Safety Goals
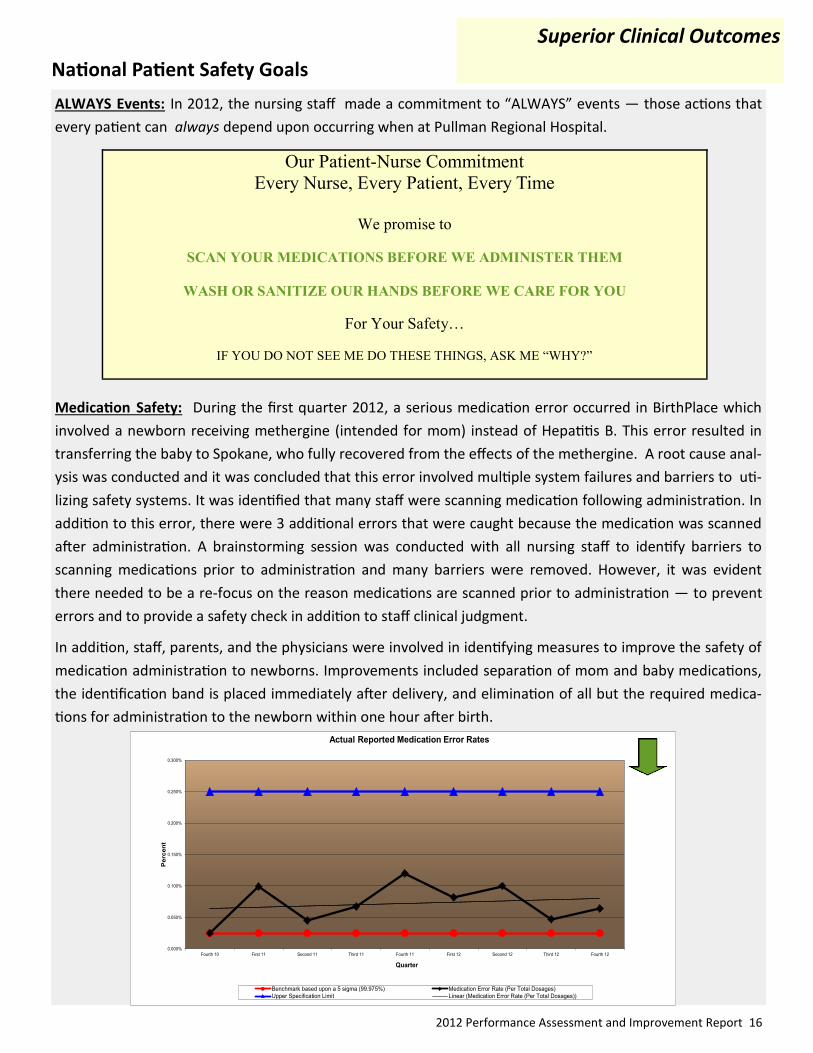
ALWAYS Events: In 2012, the nursing staff made a commitment to “ALWAYS” events — those actions that
every patient can always depend upon occurring when at Pullman Regional Hospital.
Medication Safety: During the first quarter 2012, a serious medication error occurred in BirthPlace which
involved a newborn receiving methergine (intended for mom) instead of Hepatitis B. This error resulted in
transferring the baby to Spokane, who fully recovered from the effects of the methergine. A root cause anal-
ysis was conducted and it was concluded that this error involved multiple system failures and barriers to uti-
lizing safety systems. It was identified that many staff were scanning medication following administration. In
addition to this error, there were 3 additional errors that were caught because the medication was scanned
after administration. A brainstorming session was conducted with all nursing staff to identify barriers to
scanning medications prior to administration and many barriers were removed. However, it was evident
there needed to be a re-focus on the reason medications are scanned prior to administration — to prevent
errors and to provide a safety check in addition to staff clinical judgment.
In addition, staff, parents, and the physicians were involved in identifying measures to improve the safety of
medication administration to newborns. Improvements included separation of mom and baby medications,
the identification band is placed immediately after delivery, and elimination of all but the required medica-
tions for administration to the newborn within one hour after birth.
Superior Clinical Outcomes
Our Patient-Nurse Commitment
Every Nurse, Every Patient, Every Time
We promise to
SCAN YOUR MEDICATIONS BEFORE WE ADMINISTER THEM
WASH OR SANITIZE OUR HANDS BEFORE WE CARE FOR YOU
For Your Safety…
IF YOU DO NOT SEE ME DO THESE THINGS, ASK ME “WHY?”
0.000%
0.050%
0.100%
0.150%
0.200%
0.250%
0.300%
Fourth 10 First 11 Second 11 Third 11 Fourth 11 First 12 Second 12 Third 12 Fourth 12
Perc
en
t
Quarter
Actual Reported Medication Error Rates
Benchmark based upon a 5 sigma (99.975%) Medication Error Rate (Per Total Dosages)
Upper Specification Limit Linear (Medication Error Rate (Per Total Dosages))

2012 Performance Assessment and Improvement Report 17
National Patient Safety Goals
Reporting of Medication Errors: The Agency for Healthcare Research and Quality (AHRQ) has defined one of
the important elements of creating a culture of safety is staff’s willingness to report errors. Research has
shown that most medical errors are due to process and systems issues, and the identification of potential
(not reaching patient) and actual errors allows the hospital to make the necessary improvements in the sys-
tem to avoid future errors. Since 2009, Pullman Regional Hospital has had a focused effort to increase the
reporting of these errors. These include efforts to create a non-punitive culture maintaining and improving
the incident reporting system, and reinforcing the importance of reporting to hospital staff by department
leaders.
Patient’s Involvement in Care: Patients are encouraged to be active participants in their care at Pullman Re-
gional Hospital. Our Philosophy of Patient Care supports these efforts by encouraging patients to be
“partners” in their patient care processes.
Superior Clinical Outcomes
80.0
85.0
90.0
95.0
100.0
4th2010
1st2011
2nd2011
3rd2011
4th2011
1st2012
2nd2012
3rd2012
4th2012
Mea
n
Patient Satisfaction with Involvement in Care
Patient Satisfaction with Involvement in Care
Target
Linear (Patient Satisfaction with Involvement in Care)
1st 10 2nd 10 3rd 10 4th 10 1st 11 2bd 11 3rd 11 4th 11 1st 12 2nd 12 3rd 12 4th 12
No impact on Patient; Severity Index A-C 36 27 21 25 55 45 19 22 43 36 24 29
Impact on Patient (Treatement and/orMonitoring); Severity Index D - H
6 1 2 0 2 0 0 1 4 2 0 1
0
10
20
30
40
50
60
Num
ber
Med Errors: Impact on Patients

2012 Performance Assessment and Improvement Report 18
National Patient Safety Goals
Influenza Prevention Program
In a continuing effort to increase the rate of voluntary employee participation, a minimum goal of 90% was
established by the Board of Commissioners. The hospital was again divided into teams (“herds”) by work
areas. Each employee who participated in the program was entered into a weekly drawing for prizes. There
was also a team competition to achieve 100% participation and eligibility for the grand prize of a $500.00
Visa Card which was awarded at the Anniversary Party.
In addition, an event was conducted called “Shotoberfest” which combined an emergency preparedness drill
for “Point of Distribution” with administration of influenza vaccinations to employees and adult family mem-
bers. Over 300 vaccinations were administered. All participants received a German-themed lunch (with root
beer).
An on-line education program was required for employees who planned to decline the vaccine. These em-
ployees were required to have an “Informed Declination” meeting with the medical director for Employee
Health or his designee. All employees were either required to have the vaccine, sign a medical declination,
or complete the educational module and meet with the medical director.
Infection Prevention
Tdap Immunizations: In response to the epidemic of Pertussis in Washington State, an emphasis on immuniz-
ing our staff with Tdap resulted in an increase in overall vaccinations. This immunization became a condition
of employment for all new employees in July 2012. We have achieved a participation rate of 80% as com-
pared with 46% in 2011. The Board of Commissioners established a goal of 100% participation.
TB Screening: 100% of new employees were screened for TB using the Quanti-FERON TB Gold test.
Antibiotic Stewardship: In October, an educational session was provided to physicians by Dr. Timothy Dellit
from Harborview Medical Center. The focus of the presentation was appropriate use of antibiotics with a
goal of decreasing resistance to antibiotics as well as decreasing the incidence Clostridium difficile.
Superior Clinical Outcomes
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
2007 2008 2009 2010 2011 2012
Staff Receiving Influenza Immunization
Percent Immunized

2012 Performance Assessment and Improvement Report 19
National Patient Safety Goals
Infection Prevention
Superior Clinical Outcomes
ICU/MSU Patients at risk for central line associated bloodstream infections: There was one case of cen-
tral line associated bloodstream infections in 2012. We continue to use the “central line bundle” and
emphasize appropriate hand hygiene. In collaboration with the lab and ICU, new central line blood cul-
ture policy was developed that will more definitively identify a blood stream infection related to a cen-
tral line. In addition, a new central/PICC line dressing kit was implemented which has a “stat lock” se-
curement device and replaces sutures for skin closure around the line. Another improvement was the
use of the MicroClave Clear IV valve which has a small residual volume, a straight, clear fluid pathway,
and is neutral displacement. We also added the use of the Curos port protector with an alcohol swab
cap which disinfects and protects the IV ports. In addition, in 2012 we added daily baths with Chlorhex-
adine Gluconate (CHG).
Clostridium difficile Testing: In 2012, utilizing the enhanced testing methods improved overall accuracy
of results.
Hand Hygiene: In 2012, we continued to have an emphasis on hand hygiene. In addition to tent cards
located in patient rooms, nursing staff are now instructing patients to ask staff if they have cleansed
their hands when they come into the room (see page 16 ALWAYS events).
Infection Prevention Risk Assessments: Annually, a risk assessment is conducted to evaluate service areas, patient populations, and procedures which have the potential for causing infections. We identify the strategies for prevention as well as the method for evaluating results. Areas of focus in 2012 were prioritized and included the following:
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
HAI 1.70% 1.34% 2.12% 2.77% 2.06% 1.98% 1.44% 1.88% 1.25% 1.24% 1.77%
HAI Nat. Aver. 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50% 4.50%
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
4.00%
4.50%
5.00%
Pe
rce
nt
Hospital-Acquired Infections
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
SSI 0.70% 0.29% 0.97% 1.24% 1.23% 1.31% 0.75% 0.91% 0.75% 0.39% 0.71%
SSI Nat. Aver. 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00% 2.00%
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
4.00%
4.50%
5.00%
Pe
rce
nt
Surgical Site Infections
1. Central line associated bloodstream infections* 5. Catheter-associated urinary tract infections*
2. Hospital-acquired pneumonia 6. Influenza/Tdap vaccinations
3. Multi-drug resistant organisms 7. Compliance with isolation procedures
4. Surgical site infections* 8. TB Screening
* Required by CMS
2012 Priorities for Infection Prevention

2012 Performance Assessment and Improvement Report 20
Additional Patient Safety Performance Improvement Initiatives
Elective Deliveries: In response to the American
College of Gynecology’s recommendations that
no elective deliveries (inductions and C-sections)
take place prior to 39 week gestation, the OB-
Peds Committee and the Quality Improvement
Committee (QIC) continued to track progress in
meeting this target. While induction rates have
improved significantly, the hospital continues to
be challenged by scheduling issues for C-sections.
The OB-Peds Committee continues to discuss pos-
sible options; in the meantime, it has recom-
mended that a gestational age of at least 38
weeks plus 5 days be maintained.
Unexpected Outcomes Management: The Unex-
pected Event Response Team (UERT) responded
to 12 reported events in 2012 as compared with
17 in 2011. Surgical events accounted for the ma-
jority of events reported.
Fall Prevention: In 2012, in response to an increase in fall rates, additional efforts were undertaken to identify
trends through root cause analysis and improve processes related to fall prevention. These efforts included:
Signage in rooms reminding nursing about using bed alarms;
Standing with the patient when using the bath-room, and signage placed to remind patient to wait for assistance;
Requiring two people to walk post-operative to-tal knee replacement patients;
Trialing a walking lift that has a seat sling to catch the patient while ambulating.
Superior Clinical Outcomes
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
4th2010
1st2011
2nd2011
3rd2011
4th2011
1st2012
2nd2012
3rd2012
4th2012
Elective Deliveries
Repeat C-sections meeting criteria of 39 weeks or greater.
Elective inductions meeting criteria of 39 weeks gestation or greater
Surgical
IT
Security/Psychiatric
Neonatal/Pediatric
2012 Unexpected Events Reported
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
9.00
10.00
Fourth 10 First 11 Second 11 Third 11 Fourth 11 First 12 Second 12 Third 12 Fourth 12
Nu
mb
er
Inpatient Falls per 1000 Patient Days
Inpatient falls per 1000 patient days Upper Specification Limit
2012 Performance Assessment and Improvement Report 21
Communication of Critical Values: In 2011, communication of critical values continued to be the focus for
the Respiratory Care Department, ICU, MSU, Laboratory, and Imaging. During the last two years, perfor-
mance overall has improved in all areas. However, efforts continue to improve performance in terms of doc-
umentation.
Carbon Dioxide Monitoring: Standards of care for patients at high risk for respira-
tory compromise postoperatively were implemented in July 2011 and 2012. This
improved service involves patients being assessed preoperatively with the
“Epworth Sleepiness Scale” and other evidence-based criteria that have been
found to put patients at risk for having respiratory complications postoperatively.
Patients that are found to be at low, moderate, or high risk for respiratory com-
plications have specific care interventions to monitor them closely postoperative-
ly. One of the specific interventions that Pullman Regional Hospital has initiated is the use of End-Tidal CO2
monitoring, which has the ability to recognize respiratory compromise much earlier than any other assess-
ment or diagnostic tools by measuring the amount of exhaled CO2. Beginning in January 2013, Respiratory
Care will begin tracking the inter-
ventions that patients required
based upon the monitoring.
Superior Clinical Outcomes
Critical Values 1st
2010
2nd
2010
3rd
2010
4th
2010
1st
2011
2nd
2011
3rd
2011
4th
2011
1st
2012
2nd
2012
3rd
2012
4th
2012
Target Goal
Radiology report turnaround time <24
hours
97.4% 97.6% 96.3% 97.5% 97.6% 97.4% 95.8% 97.9% 97.9% 98.4% 98.0% 98.2% 95.0% 100.0%
Percent of imaging critical results reported
within 1 hour.
NA NA 88.1% 90.6% 90.4% 94.0% 89.8% 100.0% 100.0% 100.0% 100.0% 100.0% 95.0% 100.0%
Stat lab turnaround time for the ED <1 hour 99.1% 98.7% 96.9% 98.6% 94.3% 96.9% 96.7% 98.0% 98.0% 98.0% 97.0% 97.5% 95.0% 100.0%
Critical lab value called to the provider by
the RN within the specified time frame
NA NA 34.8% 70.0% NA 66.2% 72.2% 77.0% 77.0% 85.6% 89.3% 81.8% 95.0% 100.0%
80.0%
85.0%
90.0%
95.0%
100.0%
105.0%
4th 2011 1st 2012 2md 2012 3rd 2012 4th 2012
Capnography
Percent of patient assessed pre-operatively for possible respiratorycomplications
Percent of patients meeting indications for end tidal CO2 monitoringand received it

2012 Performance Assessment and Improvement Report 22
2012 Medical Staff Performance
Improvement Activities
OB/Peds Committee
The committee reviewed 109 charts and provided physicians with copies of review worksheets for feedback.
In some cases the physician was invited to the committee to participate in the review. No actions were tak-
en.
Other activities included a recommendation for the discontinuation of Vaginal Births After C-sections
(VBACs), a discussion of the use of pulse oximetry for newborns, and review/development of Neonatal Re-
suscitation Providers (NRP) protocols, and the Safe Sleep Policy, the Respiratory Distress Policy, and the Cy-
togenic Policy.
Critical Care/Medicine Committee
The committee reviewed 33 charts and provided general reminders regarding documentation issues and
one verbal consultation with a physician regarding protocol adherence. The committee also developed the
Radiology Assistant privilege form, and revised the Transfusion Reaction Policy. Following a massive transfu-
sion, a Root Cause Analysis was conducted and several process changes identified; a drill was conducted and
additional changes were made.
Surgery Committee
The committee reviewed 67 charts; one case was referred by the Critical Care Medicine Committee with no
further action required. One case was reviewed per request of the physician reviewer for the Rural
Healthcare Quality Network with no further action required.
Anesthesia
The committee reviewed 108 charts with feedback to the providers for documentation issues. The com-
mittee also developed MRI anesthesia protocols and processes.
Credentials
The committee reviewed and recommended 14 initial appointments, 41 reappointments, and performed five
Focused Professional Performance Review (FPPE) evaluations and two additional privilege requests. In addi-
tion, the committee recommended the Radiology Assistant privilege form, developed a medical staff catego-
ry matrix, and revised the Credentialing Procedure Manual to address requirements for low volume provid-
ers.
Superior Clinical Outcomes

2012 Performance Assessment and Improvement Report 23
2012 Medical Staff Performance
Improvement Activities
Family Medicine
The committee reviewed 23 charts with no action required. In addition, the committee completed its pilot of
the electronic chart review system (OPPE and FPPE).
Psychiatry Committee
The committee reviewed 1 chart with no action required. Other case reviews resulted in reminders to use
the Suicide Precautions protocol, and clarification of the referral process. Other activities included revising
the chart review indicators and development of a Hopelessness Screening tool for all patients.
Emergency Medicine Trauma
The committee reviewed 29 emergency medicine charts and 46 trauma charts. It was concluded from these
reviews that medical management was appropriate. In addition, the committee developed a policy for the
administration of nitrous oxide in the ED, a pre-oxygenation protocol for elective intubations in the ED, and
an order set for pediatric diabetic ketoacidosis patients.
Pharmacy, Therapeutics, and Infection Control
The committee continued to monitor adverse drug reactions, medication errors, hospital-acquired infec-
tions, DVT prophylaxis, and immunizations. It reviewed the
Influenza Plan and infection prevention expectations.
Medical Executive Committee
The committee recommended Credentialing Procedure manual revisions, and the Radiologist Assistant privi-
lege form. It revised the documentation policy to be consistent with Joint Commission requirements. The
committee also completed the annual policy review.
Superior Clinical Outcomes
I think they were all very good — nurses, CNAs
and doctors. I think they did a wonderful job.”
2012 Performance Assessment and Improvement Report 24
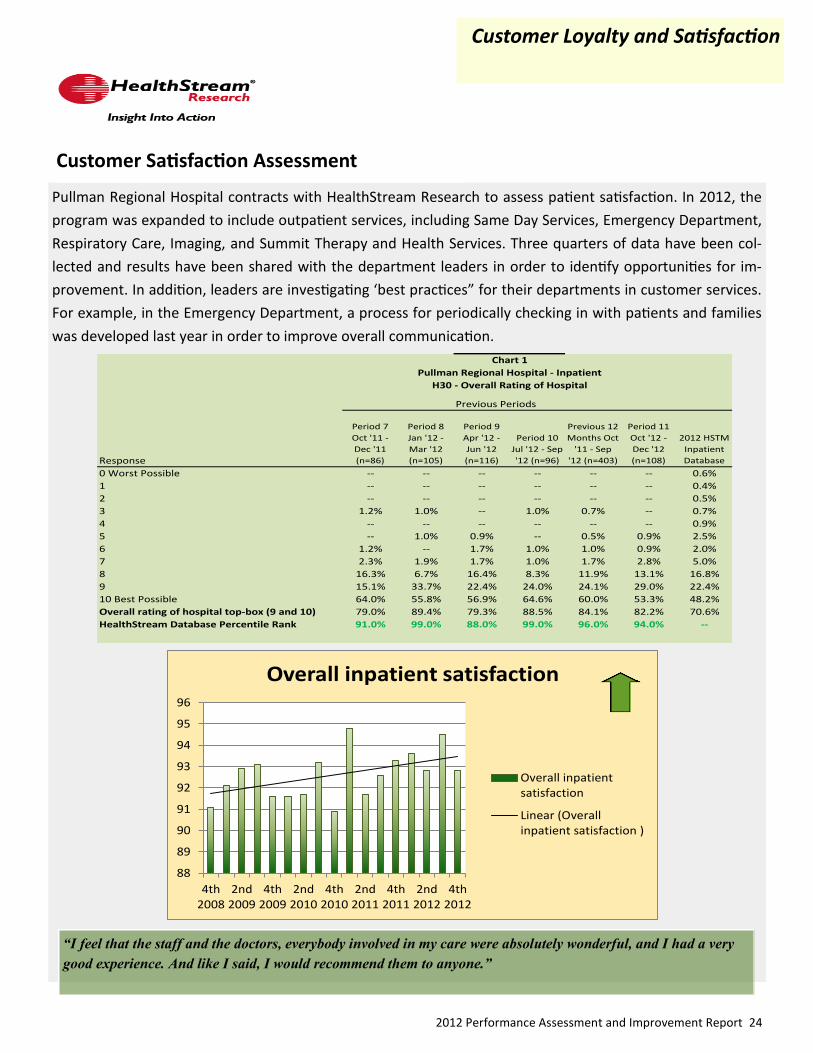
Pullman Regional Hospital contracts with HealthStream Research to assess patient satisfaction. In 2012, the
program was expanded to include outpatient services, including Same Day Services, Emergency Department,
Respiratory Care, Imaging, and Summit Therapy and Health Services. Three quarters of data have been col-
lected and results have been shared with the department leaders in order to identify opportunities for im-
provement. In addition, leaders are investigating ‘best practices” for their departments in customer services.
For example, in the Emergency Department, a process for periodically checking in with patients and families
was developed last year in order to improve overall communication.
Customer Satisfaction Assessment
Customer Loyalty and Satisfaction
“I feel that the staff and the doctors, everybody involved in my care were absolutely wonderful, and I had a very
good experience. And like I said, I would recommend them to anyone.”
88
89
90
91
92
93
94
95
96
4th2008
2nd2009
4th2009
2nd2010
4th2010
2nd2011
4th2011
2nd2012
4th2012
Overall inpatient satisfaction
Overall inpatientsatisfaction
Linear (Overallinpatient satisfaction )
Previous Periods
Response
Period 7
Oct '11 -
Dec '11
(n=86)
Period 8
Jan '12 -
Mar '12
(n=105)
Period 9
Apr '12 -
Jun '12
(n=116)
Period 10
Jul '12 - Sep
'12 (n=96)
Previous 12
Months Oct
'11 - Sep
'12 (n=403)
Period 11
Oct '12 -
Dec '12
(n=108)
2012 HSTM
Inpatient
Database
0 Worst Possible -- -- -- -- -- -- 0.6%
1 -- -- -- -- -- -- 0.4%
2 -- -- -- -- -- -- 0.5%
3 1.2% 1.0% -- 1.0% 0.7% -- 0.7%
4 -- -- -- -- -- -- 0.9%
5 -- 1.0% 0.9% -- 0.5% 0.9% 2.5%
6 1.2% -- 1.7% 1.0% 1.0% 0.9% 2.0%
7 2.3% 1.9% 1.7% 1.0% 1.7% 2.8% 5.0%
8 16.3% 6.7% 16.4% 8.3% 11.9% 13.1% 16.8%
9 15.1% 33.7% 22.4% 24.0% 24.1% 29.0% 22.4%
10 Best Possible 64.0% 55.8% 56.9% 64.6% 60.0% 53.3% 48.2%
Overall rating of hospital top-box (9 and 10) 79.0% 89.4% 79.3% 88.5% 84.1% 82.2% 70.6%
HealthStream Database Percentile Rank 91.0% 99.0% 88.0% 99.0% 96.0% 94.0% --
Pullman Regional Hospital - Inpatient
H30 - Overall Rating of Hospital
Chart 1

2012 Performance Assessment and Improvement Report 25
Community Education
Community Service and Education:
Prepared Childbirth Classes
Refresher Childbirth Classes
Sibling Classes
New Parent Classes
Fitness Program
Monthly EMS Rounds
ACLS/CPR Classes
Nutrition Education
Diabetes Support Group
Breast Cancer Support Group
Prostate Cancer Support Group
Lupus/Fibromyalgia Support Group
Type I Diabetes Family Support Group
Prostate Screening Program
Senior Citizen Luncheon Presentations
WSU Class Instruction by Physical Therapists
Alcohol Awareness Education
Community “Compass” Resource Guide
Pediatric Advanced Life Support classes
Neonatal Resuscitation classes
Meals on Wheels
Co-sponsorship of an educational series on
Alzheimer’s and related illnesses
“We Care” Senior Fair
Palouse Area Cancer Coalition
Community Events:
Schweitzer Engineering Health Fair
Sunnyside Elementary Career Day
Palouse Mall Baby Fair
Inland NW Blood Drives
Family Fair
Lentil Festival
Relay for Life
Women ‘s Works
Summit Therapy and Health Services Open House
Pumpkin Dash
Student Programs:
WWAMI Medical Student Preceptor Program
Interns in Pharmacy and Education
LCSC C.N.A., Nursing, and Radiology student clinical
education
Walla Walla Community College nursing students
Intercollegiate College of Nursing students
Student volunteers in the Pharmacy and Emergency
Department
Spokane Community College Health Information Man-
agement Interns
MEDEX NW Physician Assistant Training at U of W
Pullman Regional Hospital is a “community leader of integrated health and healing activities.” The hospital
demonstrated this commitment through its community events and educational offerings.
Customer Loyalty and Satisfaction

2012 Performance Assessment and Improvement Report 26
Community Engagement
Community Volunteers: One-hundred and seven community volunteers donated a total of 8,773 hours. These hours were donated at the Information Desk, Gift Garden, Same Day Services, Oncology Department, serving as hospital chaplains and at various Auxiliary events.
Student Volunteers: Seventy-nine WSU student volunteers served in the Pharmacy, Med-Surg, ICU and Sur-gery departments and at the Information Desk contributing 2,690 hours.
Auxiliary:
In 2012, eight departmental projects were fund-ed by the Auxiliary totaling $18,939. Since 1968, the Auxiliary has donated more than $437,325 to the hospital. On Saturday, December 8th, the Auxiliary hosted its annual Holiday Tea at Ban-yan’s on the Ridge. Over $2,500 was raised in donations at the tea. The Christmas Tree Raffle was also held in December. Sixteen businesses and individuals donated decorated trees and $4,235 was raised. The Gift Garden continues to be the major source of funding for the Auxiliary. Other fundraisers included sales of See’s Candy, Have-A-Heart, and Books-R-Fun book sales.
Volunteer/Auxiliary Recognition Luncheon:
The volunteers and auxiliary members were honored during the Annual Volunteer-Auxiliary Recognition Luncheon on April 5th at Banyan’s on the Ridge Pavilion. Carol Smawley was honored as the Auxilian of the Year and Kelma Short as the Volunteer of the Year.
Pet Partnership Program: Pullman Regional Hospital’s Pet Partnership Program coordinates Pet Partnership teams to volunteer at sites across the Palouse to share the healing capacity of pets with the community, in-cluding long term care facilities, senior living centers, daycares, etc. There are currently eight pet partners that participate in providing this animal-assisted support to promote physical and emotional well-being.
Customer Loyalty and Satisfaction
Our volunteers are an invaluable and welcomed complement to the care we provide and an indispensable
part of Pullman Regional Hospital. The benefits of giving time to help others include a greater under-
standing of yourself, the development of life-long friends, and the joy of giving.
50
55
60
65
70
75
80
85
90
95
100
2007 2008 2009 2010 2011 2012
Volunteer Satisfaction
Mean Score

2012 Performance Assessment and Improvement Report 27
In 2012, Pullman Regional Hospital conducted seven New Employee Orientations for 70 new hires. The orien-
tation included philosophy and culture of the hospital, Color Code, performance improvement, and regulato-
ry requirements. Evaluation of the orientation process showed that 88.9% of respondents indicated “Strongly
Agree” or “Agree” on the 90 day survey (see below) as compared with 84.3% in 2011.
New Employee Orientation
Employee Engagement
Pullman Regional Hospital 90 Day Survey Response Data for 2012
Strongly
Agree/
Agree
Strongly
Agree/
Agree
Recruitment Process Department Orientation
My job interview was scheduled amazingly quickly! 87.5%
My department orientation provided me the exact tools and knowledge
I needed to perform my new job responsibilities. 90.0%
I felt really good about the time between my interview and my job offer. 92.5%
My preceptor is an excellent role model of the knowledge, skills, and
attitudes expected of the staff members in my department. 95.0%
The interview included a great description of my job responsibilities. 82.5%
My preceptor did an amazing job of assisting me to know what is
expected of me at work in my job and in the department. 95.0%I received an astounding packet of information about the hospital and the generous benefits
offered to the employees of PRH. 92.5%
PRH has done a super job in providing me the materials and equipment
I need to do my work right. 95.0%It was easy to accept the job offer as it also included my competitive rate of pay. 90.0% Employee Engagement
New Employee Orientation At work, I have the opportunity to do what I do best every day. 85.0%I absolutely enjoyed attending New Employee Orientation. 82.5% In the last 7 days, I have received recognition or praise for doing good 82.5%The information provide to me in New Employee Orientation was what I needed to begin my new
job. 82.5%
I believe that my department leader and/or someone else at the
hospital seems to care about me as a person. 90.0%What is totally awesome is that I see the information presented and discussed in New Employee
Orientation about the vision, mission, and philosophy of PRH lived out in my department 87.5% There is someone at the hospital who encourages my development. 87.5%I definitely feel as if I am a member of the PRH team. 95.0%
Employee Turnover
Employee turnover has continued to trend
downward. This was the first year since 2005
that the number of departures exceeded the
number of hires. In addition, the total num-
ber of employees went from 416 at the be-
ginning of the year and fell to 408 at the end
of the year.
0
5
10
15
20
25
30
35
40
2005 2006 2007 2008 2009 2010 2011 2012
Employee Turnover
% Overall Turnover % Full-time Turnover % Part-time Turnover
0
20
40
60
80
100
120
2005 2006 2007 2008 2009 2010 2011 2012
Employee Hires and Departures
Hires Departures

2012 Performance Assessment and Improvement Report 28
Specialty Certifications
All medical staff members are required to be board-eligible or board certified in a specialty in
order to obtain privileges at Pullman Regional Hospital. Currently, of the 62 active medical staff
61 are board certified (the remaining physician was a medical staff member prior to the imple-
mentation of this requirement). In 2012, three physicians achieved certification or re-
certification — Dr. Aaron Scott in Emergency Medicine, Dr. Steven Pennington in Orthopedic
Surgery and Dr. Stephen Bergmann in Emergency Medicine.
Pullman Regional Hospital Employees
Pullman Regional Hospital Medical Staff
Employee Engagement
Key:
FACHEFellow American College of Healthcare
ExecutivesMRI MRI registry in Imaging CNE
RNC Registered Nurse Certified CMSRNCertified Medical Surgical
Registered NurseM
CCRN Certified Critical Care Registered Nurse CNMTCertified Nuclear Medicine
TechnologistCT
CNOR Certified Nurse Operating Room CRCSTCertified Registered Central
Sterlizing TechnicianCEN
ServSafe Advanced Food Handling Certification CAPACertified Ambulatory
Perianesthesia NursePNBC
CMSRN Certified Medical Surgical RN CNE Certified Nurse Educator ARRTAmerican Registry of
Radiology Technologists
ASHAAmerican Speec andHearing
AssociationARDMS
American Registry ofDiagnostic
Medical SonographyCDE Certified Diabetes Educator
MNTCBNuclear Medicine Technology
Certification Board
Certified Nurse Educator
Mammography registry in
Imaging
CT registry in Imaging
Certified Emergency Nurse
Pedicatric Nurse Board
Certified
Scott Adams FACHE Lisa Cordodor CNOR Dorcas Hirzel Trainer Darin Porter ARRT(CT)(RRA)
Stacey Agggabao CEN Tyson Cranston ARRT(CT) Angie Hoener ARDMS Garrett Quarve ServSafe
Hawa Al-Hassan RNC Anna Engle RNC Kai Johnson CEN Linda Rauch RNC
Jennifer Anderson ARRT(CT) Linda Fisher CNOR Keri Jones ASHA Amber Roberts RNC
Kellsi Ausman RNC Marcy Fisher CCRN Julie Keller CDE Lynn Sakamoto CNOR
Jennifer Becker RNC Rachel Gabby PNCB Laura Keogh RNC Helen Scheibe ARRT(M)(CT)
Nicoline Blaker RNC Andi Gallagher ARRT(M)(MR) Laure' Larsen CCRN Kelly Sebold ASHA
Jonna Bobeck CEN Jami Gilkey ARDMS Dawn Libey RNC Jason Sondgeroth CEN
Johanna Bounous CCRN Kelly Goertzen CCRN Lyle Lowder NMTCB Eileen Taylor CEN
Charles Butler CEN Ginny Gosse CCRN Steffen Ludwig ServSafe Nicole Weiss RNC
April Cane ServSafe Charles Gunkle RNC Cathy Murphy CAPA Cathy Wilkins CEN
Brenda Champoux ARRT(M) Donna Haynes CNE Peggy Myers ARDMS Betsy Wilson ASHA
Lynne Cooper CEN Laurie Heimbigner RNC Carol Owings RNC Dianna Wise RNC
Ambyr Henderson ASHA Jamie Peters CNOR Melissa Wolf RNC

2012 Performance Assessment and Improvement Report 29
Employee Engagement
In September 2010 Pullman Regional Hospital began offering CPI training. This Nonviolent Crisis Intervention
training program is a holistic behavior management system based on the philosophy of providing the best
Care, Welfare, Safety, and Security for staff and those in their care, even during the most violent moments.
The program focuses on preventing disruptive behavior by communicating with individuals respectfully and
with concern for their well-being. The program teaches physical interventions only as a last resort—when
an individual presents an imminent danger to self or others—and all physical interventions taught are de-
signed to be non-harmful, noninvasive, and to maintain the individual’s dignity. Follow-up debriefing strate-
gies are also key components of the training program.
Passport to Growth
Crisis Prevention Institute (CPI) Training
In August 2011, the decision was made to get Passport to Growth re-started after a three-year hiatus. In October 2011, 89 employees entered the program and in October 2012, 73 employees exited the program, 3 employees completed their employment with the hospital before the exit time period, and 13 employees car-ried their program over to the 2012-2013 year.
The decision to offer Passport to Growth for employee participation is made on an annual basis. In September 2012, the decision was made to offer the program for the 2012-2013 program year however, the reward for completion would be a $50 Visa Gift card for all three levels of participation. This was a change from the three different levels of recognition for the completion of one of the three levels. In October 2012, we had 32 employees join the program for the next year.
Department 2010 – Numbers 2011 – Numbers 2012 – Numbers 2013 – Numbers Totals
Emergency Department 3 18 4 0 25
Maintenance/Security 1 5 3 0 9
Clinical Coordinators 1 5 1 1 8
Patient Registration 4 8 4 0 16
Patient Financial Services 1 8 0 0 9
Summit Therapy 1 26 5 2 34
Other Clinical Staff 5 16 13 10 37
Other Support Staff 2 5 10 2 18
Full Class Totals 18 91 40 15 Total 164
Refresher Class Totals 0 9 22 8 Total 39

2012 Performance Assessment and Improvement Report 30
Staff & Physician Recognition
Employee Appreciation: During National Hospital Week, several
events were held in appreciation of our staff. These included a Long-
horn Barbeque and the Summit Therapy and Health Services Open
House. The festivities culminated in a celebration at Zeppoz for all
employees and their families. Everyone enjoyed food, fun and
games, and were recognized for their years of service to the hospi-
tal.
Nurses’ Recognition Day: In recog-
nition of Nurses’ Day, the nursing
staff at Pullman Regional Hospital
held a Mexican Fiesta for all hospital
staff. Staff enjoyed a meal of beef
or chicken burritos, beans, rice and
a salad. Strawberries and whipped
cream served with a cinnamon chip
were served for dessert, and virgin
margaritas topped off the fiesta.
Doctors’ Day: In April, in celebration of Doctors’ Day, awards for
Physician Excellence, Dr. Congeniality (based upon patient satisfac-
tion) and TechnoDoc were given out at the Quarterly Medical Staff
Meeting (see left column). Two physicians were also recognized in
2012 for their years of service: Drs. John Keizur and Mike Frostad
were recognized for 15 and 10 years of service respectively.
Anniversary Celebration: The annu-
al Anniversary Celebration was again
held at Schweitzer Event Center. Ap-
proximately 200 hospital staff, Foun-
dation board members, medical
staff, and volunteers attended the
event. A “Generosity Heals” was es-
tablished to provide resources for
staff members during personal cri-
ses or in time of need. Initial contri-
butions were raised through a Dessert Auction and resulted in ap-
proximately $1100 to establish the fund.
Outstanding Employee Award:
Melissa Kennedy
Nurse Excellence Award:
Boguslawa Szafruga
Physician Excellence Award:
Dr. Benno Mohr
Patient Satisfaction Excellence
Award (Dr. Congeniality):
Dr. Ben Adkins
Dr. Steve Hall
TechnoDoc Award:
Dr. John Keizur
TechnoDoc Honorable Mention:
Dr. Karen Geheb
Employee Engagement
“I had an outstanding experience at
Pullman Regional Hospital and I can’t
think of anything they could have done
better.”

2012 Performance Assessment and Improvement Report 31
ICU Nurse Education: Pullman Regional Hospital facilitated two 4-hour Advanced Education courses in col-
laboration with St. Joseph’s Medical Center, Gritman Medical Center, and Tri-State Memorial Hospital. A to-
tal of 128 nurses in the region participated in these education sessions. In addition, the ICU nurses at Pullman
Regional Hospital participated in a Mock Code Competency using simulation technology (see page 40).
Medical Surgical Nurse Education: Seventeen nurses completed a 14-week review and update; in addition,
staff participated in the Mock Code Competency.
BirthPlace Nurse Education: Staff participated in the biannual Stabilization of the Newborn Prior to Transfer
(STABLE) class which is required every 2 years. In addition, the Newborn Resuscitation Provider class was
provided six times during the year. Four new staff RNs attended Labor and Delivery classes at the Deaconess
Neonatal Center.
Same Day Services Staff Education: Staff are provided with articles or published studies on new procedures,
techniques, medications and points of clinical interest.
Emergency Services Staff Education: in 2012 Jonna Bobeck, RN developed learning modules for the follow-
ing: arterial lines, arterial blood gas analysis, central venous catheters, delirium assessment, Hovermatt, Code
Blue, the Sager Splint, massive transfusion, Nitronox, transvenous pacing, Code Stroke, and Cardiac Level
One. These modules are used to initial orientation and annual education through the HealthStream system.
Leadership Retreat:
In December 2012, the Leadership Retreat focused upon exploring the sources of our leadership. The program was designed to help leaders come away with a renewed understanding of how each can facilitate change, both within the organization and in their personal lives. Using the domains of per-sonal mastery, collaborative inquiry, and the systems perspective applied to sustaining profound change, the program provided opportunities to:
Formulate a coherent picture of the results each person most desired to create individually and collec-tively as well as gain a better understanding of the current reality.
Understand how underlying systemic structures shape behavior and how to recognize and shift those structures.
Explore underlying beliefs and assumptions and their impact on the capacity to lead.
Facilitate conversations that promote learning and collaboration.
Operate from a deeper and more stable sense of purpose.
Leadership Development for Physician Leaders
Two physicians began participation in the University of Washington’s Leadership Development Program for
physicians in 2012. This program focused upon personal awareness, leadership principles, data and statistical
analysis, and interpersonal communication, including coaching skill development. Drs. Stephen Hall and Pe-
ter Mikkelsen are in the process of completing the course.
Leadership and Staff Skills
Employee Engagement

2012 Performance Assessment and Improvement Report 32
Financial Effectiveness
Financial SummaryStatement of People & Programs
We are a community of:
409 Full-time and Part-time Employees
198 Volunteers and Auxilians
150 Medical Staff (62 in active membership)
As a team we served:
1,762 Men, Women, Children, & Newborns as inpatients
66,234 Individual outpatient visits
That Totals:
3,902 Patient Days
453 Babies were delivered
875 Equivalent Observation Patient Days
20,999 Observation hours of care
10,322 Patients entered our Emergency Department
87,898 Laboratory tests were performed
26,893 Diagnostic Imaging studies completed
3,785 Surgical cases, 89% of which were outpatient

2012 Performance Assessment and Improvement Report 33
Financial Effectiveness
CONTRACTUALS38%
CHARITY CARE/BAD DEBT
3%
SALARY, WAGES, & BENEFITS (includes Professional Fees)
38%
SUPPLIES10%
INTEREST EXPENSE1%
DEPRECIATION & AMORTIZATION
3%
OTHER 7%
WHERE THE MONEY GOES

2012 Performance Assessment and Improvement Report 34
Financial Effectiveness
Pullman Regional Hospital Vital Signs
2007 2008 2009 2010 2011 2012
Patient Days 4,248 4,276 4,049 4,299 3,874 3,902
Patient
Admissions
Surgical
Cases
Births 376 361 432 394 392 453
Emergency Visits 8,680 9,633 10,145 9,275 9,706 10,322
FTEs 272 286 294 291 312 317
1,312
3,785
1,290
3,708 3,511 3,486 3,929 3,782
1,461 1,601 1,545 1,443
- 1,000 2,000 3,000 4,000 5,000 6,000
Inptn O/R Cases
SDS Cases
XR / 10
CT
NM
MRI
US
Admits
Patient Days
ED Visits/10
Deliveries
Outpnt Visits/10
De
pa
rtm
en
t V
olu
me
s
Inptn O/RCases
SDS Cases XR / 10 CT NM MRI US Admits Patient Days ED Visits/10 DeliveriesOutpnt
Visits/10
2009 489 2,987 1,485 4,388 456 1,887 4,787 1,545 4,049 1,022 425 5,523
2010 475 3,454 1,415 4,297 342 1,852 4,884 1,443 4,299 928 394 5,585
Last Year 445 3,337 1,428 3,333 325 1,909 5,239 1,290 3,874 971 392 6,035
Current 433 3,352 1,600 3,329 432 1,769 5,359 1,312 3,902 1,032 453 6,623
Volume Review
2009 2010 Last Year Current

2012 Performance Assessment and Improvement Report 35
Productivity Standards
Financial Effectiveness
Utilization Management
The Utilization Management (UM) Department has responsibilities for all functions associated with the appro-priateness of hospital admissions and continued hospital stays as required by applicable statutes and regula-tions for Medicare, Medicaid, and other third party payors. Concurrent review is conducted by hospital staff in order to ensure that these requirements are being met. In addition, ongoing review is also conducted retro-spectively by internal and external reviewers. The department was recently expanded to meet the increasing demands. In addition, Drs. Karen Geheb and Richard Caggiano serve as the physician advisors and review cas-es as needed. External review is conducted quarterly by Dr. Scott Edminster from the Washington State Rural Healthcare Quality Network. Communication and feedback are provided to physicians as appropriate.
The Utilization Review Committee also facilitates UM functions by establishing priorities for ongoing assess-ment and evaluation. Areas of focus in 2012 included patient readmissions. The Director of Utilization Man-agement, the Assistant Director of the Medical Surgical Unit, and a representative from social services attended a WSHA “Safe Table” on readmissions. This collabo-rative has developed a “toolbox” of information to assist hospitals in identifying high risk patients as well as strategies for the reduction of readmissions. The most recent data received from Qualis Health indicated that the readmission rate for Pullman Regional Hospital was approximately 10% as compared with the state average of approximately 16%. The committee has also developed a UR Dash-board which provides data on a quarterly basis in the areas of lengths of stay, re-imbursement, readmissions, and authorizations. This dashboard will also be re-viewed by the Quality Improvement Committee on a quarterly basis.
2012 marked the first full year of utilizing productivity standards. The standard setting was an opportunity to take the historical information review and put into practice a monthly review for each service area. Additionally, the goal of this program is to provide leaders with standards that have been developed by those areas. The labor standards outlined and agreed upon for each department describe what can real-
istically be achieved now. It is important to note, the standards are not intended to alter how work is currently performed. These labor standards work within the cur-rent structure/culture established at Pullman Regional, and do not describe what productivity might be if operations were recast differently. Reaching for a new level of efficiency, one that has never been achieved at Pullman Regional would neces-sarily entail management interventions that change how daily work is performed . A review and training will occur early in 2013 with each area to discuss and develop a deeper understanding, as well as fine tune a leader’s area of oversight.

2012 Performance Assessment and Improvement Report 36
Clinical Informatics
Computerized Provider Order Entry (CPOE): In 2012, the focus of efforts was im-
plementation of transition orders for patients admitted from the Emergency De-
partment. In addition, surgical order sets for ophthalmology were implemented.
Training was provided to the ophthalmogists in CPOE. New order sets were also
developed for pediatric patients. Modifications to order sets were ongoing for all
disciplines.
Physician Documentation (PDoc): PDoc templates for newborns and pediatric pa-
tients were implemented. In 2012 there were 29 physicians using PDoc regularly as
compared with 12 providers in 2011.
Nursing Documentation: Additional screens for nursing documentation were de-veloped in 2012 for Close Patient Observation for psychiatric patients, Vaccination screens for documenta-tion of history and assessment, Delirium screens, Sepsis screens in order to assess for early signs and symp-toms of sepsis, and Post-op Respiratory Compromise assessment, and an electronic system for alerting nurs-ing staff for timed assessments and documentation.
Interfaces were also implemented for vital signs and point-of-care testing; values are automatically populat-ed in Clinical Review in the EMR (previously values had to be manually entered). This has resulted in im-proved accuracy of documentation and timeliness.
OBIX System in BirthPlace: In 2011, the OBIX system was implemented for fetal monitoring. In 2012, post-partum nursing assessment and documentation were implemented.
“Meaningful Use”: In 2008, the Office of the National Coordinator and American Recovery and Reinvest-
ment Act created funding sources for implementation of the EMR. The Office of the National Coordinator for
Health Information Technology (ONC) is at the forefront of the administration’s health IT efforts, and is a
resource to the entire health system to support the adoption of health information technology and the pro-
motion of nationwide health information exchange to improve health care. ONC is organizationally located
within the Office of the Secretary for the U.S. Department of Health and Human Services (HHS).
ONC is the principal Federal entity charged with coordination of nationwide efforts to implement and use
the most advanced health information technology and the electronic exchange of health information. The
position of National Coordinator was created in 2004 through an executive order, and legislatively mandat-
ed in the Health Information Technology for Economic and Clinical Health Act (HITECH Act) of 2009.
In 2011, the hospital achieved goals for Stage 1 attestation and received funding from CMS in 2012 as a re-
sult. In addition, work began on Stage 2 in 2012 and will continue through 2013.
Health Information Management Systems (HIMSS 13) Achievement Award: A subdivision of HIMSS is
HIMSS Analytics, which monitors EMR adoption levels of hospitals nationally. There are seven levels (Level
1—7) requiring the achievement of objectives established for each level. In 2012, Pullman Regional Hospital
was recognized for achieving Level 6. At that time, only 7.3% of hospitals had achieved this level.
Partnerships and Collaboration
2012 Performance Assessment and Improvement Report 37
Clinical Informatics
Partnerships and Collaboration
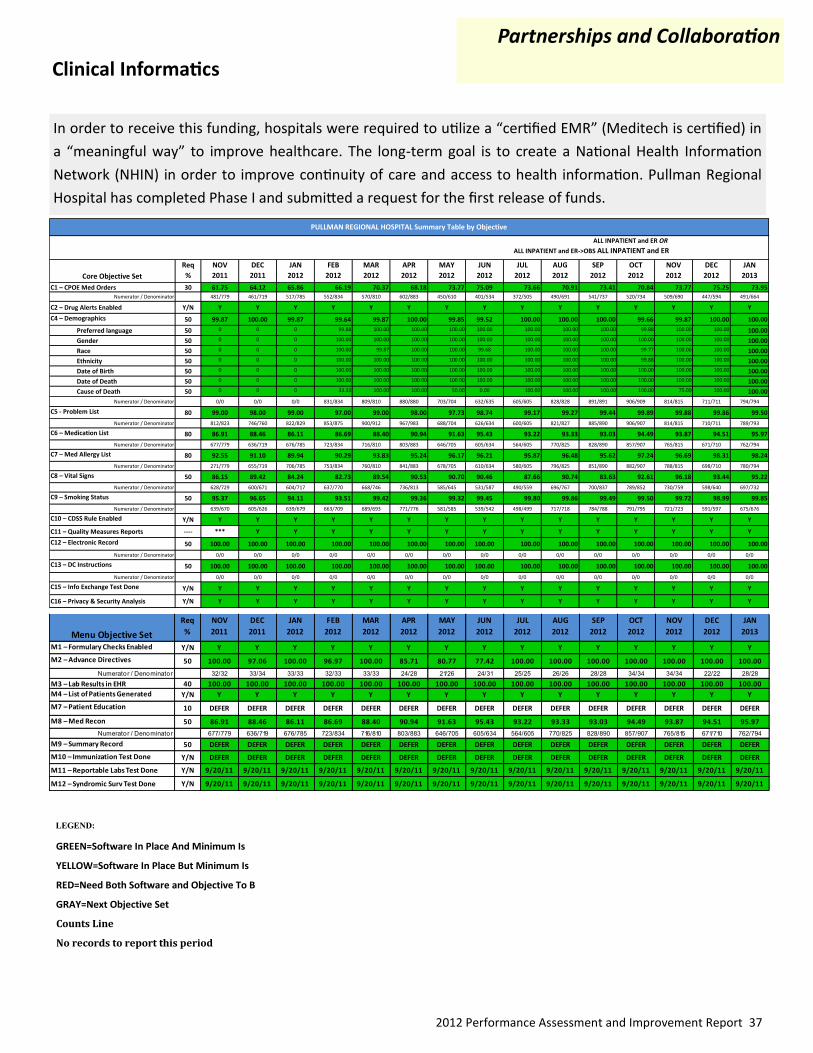
In order to receive this funding, hospitals were required to utilize a “certified EMR” (Meditech is certified) in
a “meaningful way” to improve healthcare. The long-term goal is to create a National Health Information
Network (NHIN) in order to improve continuity of care and access to health information. Pullman Regional
Hospital has completed Phase I and submitted a request for the first release of funds.
LEGEND:
GREEN=Software In Place And Minimum Is
YELLOW=Software In Place But Minimum Is
RED=Need Both Software and Objective To B
GRAY=Next Objective Set
Counts Line
No records to report this period
Core Objective Set
Req
%
NOV
2011
DEC
2011
JAN
2012
FEB
2012
MAR
2012
APR
2012
MAY
2012
JUN
2012
JUL
2012
AUG
2012
SEP
2012
OCT
2012
NOV
2012
DEC
2012
JAN
2013
C1 – CPOE Med Orders 30 61.75 64.12 65.86 66.19 70.37 68.18 73.77 75.09 73.66 70.91 73.41 70.84 73.77 75.25 73.95Numerator / Denominator 481/779 461/719 517/785 552/834 570/810 602/883 450/610 401/534 372/505 490/691 541/737 520/734 509/690 447/594 491/664
C2 – Drug Alerts Enabled Y/N Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
C4 – Demographics 50 99.87 100.00 99.87 99.64 99.87 100.00 99.85 99.52 100.00 100.00 100.00 99.66 99.87 100.00 100.00
Preferred language 50 0 0 0 99.88 100.00 100.00 100.00 100.00 100.00 100.00 100.00 99.88 100.00 100.00 100.00
Gender 50 0 0 0 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00
Race 50 0 0 0 100.00 99.87 100.00 100.00 99.68 100.00 100.00 100.00 99.77 100.00 100.00 100.00
Ethnicity 50 0 0 0 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 99.88 100.00 100.00 100.00
Date of Birth 50 0 0 0 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00
Date of Death 50 0 0 0 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00
Cause of Death 50 0 0 0 33.33 100.00 100.00 50.00 0.00 100.00 100.00 100.00 100.00 75.00 100.00 100.00
Numerator / Denominator 0/0 0/0 0/0 831/834 809/810 880/880 703/704 632/635 605/605 828/828 891/891 906/909 814/815 711/711 794/794
C5 - Problem List 80 99.00 98.00 99.00 97.00 99.00 98.00 97.73 98.74 99.17 99.27 99.44 99.89 99.88 99.86 99.50
Numerator / Denominator 812/823 746/760 822/829 853/875 900/912 967/983 688/704 626/634 600/605 821/827 885/890 906/907 814/815 710/711 789/793
C6 – Medication List 80 86.91 88.46 86.11 86.69 88.40 90.94 91.63 95.43 93.22 93.33 93.03 94.49 93.87 94.51 95.97
Numerator / Denominator 677/779 636/719 676/785 723/834 716/810 803/883 646/705 605/634 564/605 770/825 828/890 857/907 765/815 671/710 762/794
C7 – Med Allergy List 80 92.55 91.10 89.94 90.29 93.83 95.24 96.17 96.21 95.87 96.48 95.62 97.24 96.69 98.31 98.24
Numerator / Denominator 271/779 655/719 706/785 753/834 760/810 841/883 678/705 610/634 580/605 796/825 851/890 882/907 788/815 698/710 780/794
C8 – Vital Signs 50 86.15 89.42 84.24 82.73 89.54 90.53 90.70 90.46 87.66 90.74 83.63 92.61 96.18 93.44 95.22
Numerator / Denominator 628/729 600/671 604/717 637/770 668/746 736/813 585/645 531/587 490/559 696/767 700/837 789/852 730/759 598/640 697/732
C9 – Smoking Status 50 95.37 96.65 94.11 93.51 99.42 99.36 99.32 99.45 99.80 99.86 99.49 99.50 99.72 98.99 99.85
Numerator / Denominator 639/670 605/626 639/679 663/709 689/693 771/776 581/585 539/542 498/499 717/718 784/788 791/795 721/723 591/597 675/676
C10 – CDSS Rule Enabled Y/N Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
C11 – Quality Measures Reports ---- *** Y Y Y Y Y Y Y Y Y Y Y Y Y Y
C12 – Electronic Record 50 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00
Numerator / Denominator 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0
C13 – DC Instructions 50 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00
Numerator / Denominator 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0 0/0
C15 – Info Exchange Test Done Y/N Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
C16 – Privacy & Security Analysis Y/N Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
PULLMAN REGIONAL HOSPITAL Summary Table by Objective
ALL INPATIENT and ER OR
ALL INPATIENT and ER->OBS ALL INPATIENT and ER
Menu Objective Set
Req
%
NOV
2011
DEC
2011
JAN
2012
FEB
2012
MAR
2012
APR
2012
MAY
2012
JUN
2012
JUL
2012
AUG
2012
SEP
2012
OCT
2012
NOV
2012
DEC
2012
JAN
2013
M1 – Formulary Checks Enabled Y/N Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
M2 – Advance Directives 50 100.00 97.06 100.00 96.97 100.00 85.71 80.77 77.42 100.00 100.00 100.00 100.00 100.00 100.00 100.00
Numerator / Denominator 32/32 33/34 33/33 32/33 33/33 24/28 21/26 24/31 25/25 26/26 28/28 34/34 34/34 22/22 28/28
M3 – Lab Results in EHR 40 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00 100.00
M4 – List of Patients Generated Y/N Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y
M7 – Patient Education 10 DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER
M8 – Med Recon 50 86.91 88.46 86.11 86.69 88.40 90.94 91.63 95.43 93.22 93.33 93.03 94.49 93.87 94.51 95.97
Numerator / Denominator 677/779 636/719 676/785 723/834 716/810 803/883 646/705 605/634 564/605 770/825 828/890 857/907 765/815 671/710 762/794
M9 – Summary Record 50 DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER
M10 – Immunization Test Done Y/N DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER DEFER
M11 – Reportable Labs Test Done Y/N 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11
M12 – Syndromic Surv Test Done Y/N 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11 9/20/11

2012 Performance Assessment and Improvement Report 38
Information Technology
Medical Office Updates:
In 2012, Pullman Regional Hospital’s Information Tech-
nology Department (IT) continued working with Pullman
Family Medicine in upgrading the clinic’s Centricity pro-
gram to 10.0. In addition, interfaces were created with
Inland NW Health Services (INHS) and Child Profile,
which maintains state-wide immunization records.
Wireless Project:
The department upgraded all wireless systems for the
organization and clinic networks, and brought wireless
management in-house. This required rebuilding of the
old wireless network that was administered by INHS and install it on a new platform that is now completely
administered by Pullman Regional Hospital. In 2013, it is anticipated that the wired system will also be
brought under the administration of the hospital.
Radio-Frequency Identification (RFID):
This technology was implemented in the wireless system in the ED in order to perform time studies. It also
required the building of two additional servers. “Exciters” (sensors) were installed in each patient room,
which use ultrasound to track movement in and out of the room. In the future, this technology will be used
for tracking equipment and recording refrigerator temperatures.
Other Projects:
The IT Department completed its project to virtualize all physical servers. In addition, the department also
set up the Moscow office of Palouse Pediatrics.
As a contribution to the Generosity efforts, the department also conducted two food drives in 2012. The
first one raised 970 pounds of food, two large bags of coats for kids, and $175.00 in cash. The second one
raised 203 pounds of food and $135.00 in cash. All were donated to the Pullman Food Bank.
Partnerships and Collaboration
Pullman Regional Hospital was again named as one of the 25 most wired
rural hospitals nationally by Hospital and Health Networks. Based upon
a benchmarking study, hospitals report how they use information tech-
nology to address five key areas: safety and quality, customer service,
business processes, workforce, and public health and safety. Awards are
given to hospitals achieving the highest scores in these areas. This was
the sixth award received by Pullman Regional Hospital.

2012 Performance Assessment and Improvement Report 39
Pullman Regional Hospital joined Partnership for Patients, a nation-wide collaborative effort to reduce the number of hospital-acquired conditions by 40% and hospital readmissions by 20% by the end of 2013. By joining this initiative, hospitals and health care providers across the nation are pledging to make health care safer, more reliable and less costly – ultimately saving thousands of lives and millions of dollars.
Washington State Hospital Association (WSHA) is one of 26 health care organizations in the U.S. to be awarded a Hospital Engagement Net-work (HEN) contract by the U.S. Department of Health And Human Ser-vices in 2011. The Safe Table Collaboratives were focused on the key strategies (see table) and we participated in all of the infection preven-tion, adverse drug events, and preventable readmissions workshops that were offered.
Partnerships and Collaboration
Pullman Regional Hospital hosts a weekly blood drive on Mondays from 1:00 pm to 5:00pm.
Since 2011, Pullman Regional Hospital has partnered with Inland Northwest Blood Center (INBC) to host the weekly blood drives, which has significantly increased donations. INBC also has a “Give Back Program” which pays the hospital $15.00 for each unit donated through the hospital affilia-tion. In 2012, the hospital was given a total of $27,375.
Continuing Partnerships:
Nutrition Therapy at Pullman Regional Hospital has continued our partnership with WSU Health and Well-ness to provide nutrition therapy for WSU students. This partnership began in the fall of 2011 and contin-ues today. Julie Keller, MS, RD, CDE works 16 hours per week during the school year and 4 hours per week in the summer providing this valuable service.
New Partnerships:
In the summer of 2012, Pullman Family Medicine requested that Pullman Regional Hospital Nutrition Thera-py partner with them for diabetes education for their patients. Since Julie Keller, MS, RD, CDE (Certified Dia-betes Educator) has that expertise, she began to see their patients. This resulted in 39 new referrals through the end of the year. Julie sees these patients on Mondays at Pullman Regional Hospital.
In December of 2012, Anne Reed, ARNP at Schweitzer Engineering, inquired about nutrition therapy for their patients. Therefore, in the beginning of 2013, we began receiving referrals from Schweitzer.
Medical Nutrition Therapy Partnerships
Partnerships for Patients
Key Strategies
Adverse Drug EventsCatheter-associated Urinary Tract
Infections (CAUTI)
Central Line-associated Blood
Stream Infections (CLABSI)
Injuries from Falls & Immobility
Safe Deliveries
Pressure Ulcers
Surgical Site Infections
Venous Thromboembolism
Ventilator-associated Pneumonia
Preventable Readmissions
Patient and Family Engagement
2012 Stats Units "Given Back"
1st Quarter 571 $8,565
2nd Quarter 371 $5,565
3rd Quarter 411 $6,165
4th Quarter 472 $7,080

2012 Performance Assessment and Improvement Report 40
Electronic Learning
Partnerships and Collaboration
Electronic Learning System Staff Satisfaction 2012
In 2012, participation in the elec-
tronic learning system continued.
Overall satisfaction increased to
99.0% as compared with 96.6% in
2011.
Indicator BLS ACLS PALS
Number Completed 78 40 9
Overall Satisfaction with the Content of the Program 98.7% 97.5% 100.0%
Applicability to Daily Practice 97.5% 90.9% 100.0%
I will respond in an Emergency because of the Skills I learned in the course. 96.2% 90.0% 100.0%
In 2012, Pullman Regional Hospital continued to offer Pedi-atric Advanced Life Support (PALS), Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS). Participants in-cluded hospital staff and community physicians and staff. The online Neonatal Resuscitation Exam was moved to HealthStream Learning System in order to provide in-creased accessibility to staff.
To support the learning from the HeartCode (ACLS, BLS, PALS) certification, a Mock Code competency was imple-mented. Approximately 100 clinical staff members partici-pated in the event, including nursing and nursing support staff as well as the pharmacists and respiratory therapists. Satisfaction with the blended learning event was 100%, and 88% of evaluations rated the expeience above a 5 on a 1—7 Likert scale; in addition, evaluations also indicated that the staff recommended that it be offered in 2013. Staff comments have validated the use of blended learning approach: “SimMan and SimBaby helped make the situations more realistic.”
“I liked the non-stressful learning environment.”
“I have never been in on a code so now I have a better idea of what to expect.”
In addition, department orientations have continued to be utilized for Surgical Services (which was updated
in July 2012) and the Medical-Surgical Unit for all RNs and CNAs. Improved efficiency has also been achieved
with the enhanced Point-of-Care annual competency assessment and Haz-
ardous Materials Awareness. Effective electronic educational curriculum
includes Safe Patient Handling I and II, Capnography, Hopelessness Risk As-
sessment, Pediatric Update, Preventing Adverse Events in Patients with
Sleep Apnea, Wound Care Management, Delirium ABCDE Assessment, Man-
agement of the Adult Sepsis Patient, and many others.

2012 Performance Assessment and Improvement Report 41
In 2012, Pullman Regional Hospital purchased a new MRI
machine. The installation was completed in December.
This machine has the capacity to perform studies that
could not be done with the prior technology, and provides
the opportunity for members in our community to have
studies done locally. In addition, there are indications that
it will provide improved image quality resulting in the po-
tential for improved outcomes.
Magnetic Resonance Imaging (MRI)
New and Improved Products and Services
daVinci Robotic Surgical System
In 2012 Pullman Regional Hospital continued our experi-
ence with daVinci. Our experience with patient outcomes
has been consistent with the benefits reported by those
providing education about the capabilities of the robot. Pa-
tients have had shorter lengths of stay post-surgically, less
pain, and lower blood loss. There are currently five daVinci-
trained surgeons, Dr. John Keizur, Dr. Ric Minudri, Dr.
Charles Richards, Dr. Nigel Campbell, and Dr. John Visger.
The da Vinci system has been used for urologic, gynecologi-
cal, and general surgery. A total of 143 procedures have
been completed.
“From the time that I entered the hospital for what was my first major surgery, I was treated with
complete professionalism and compassion, and I don’t have a single thing I would change.”
“I have been an x-ray and laboratory technician for over 30
years in the community and my wife and I both feel that I get
excellent care in the hospital every time I’ve been there.”
Electroconvulsive Therapy (ECT)
In 2011, Pullman Regional Hospital expanded its psychiatric complement of services in the community to
include electroconvulsive therapy. This has been shown to be an effective and efficacious treatment in pa-
tients with severe or long-term depression which has failed other treatment options. The team of providers
include nursing, anesthesia, and psychiatry. A core group of nursing staff from Same Day Services began
training in 2010 with the Psychiatric Unit at Sacred Heart Medical Center. Protocols were establish to ad-
dress patient flow and provider roles in this service. In 2012, three patients were served and 14 treatments
were conducted.

2012 Performance Assessment and Improvement Report 42
Evaluation of the Performance Improvement Program
In 2012, patient safety continued to be a focus for our performance assessment and improvement efforts, with particular emphasis on caregiver communication, accuracy of patient identification, and medication rec-onciliation. In 2011, Pullman Regional Hospital addressed all of the National Patient Safety Goals, with imple-mentation and measurement of results through the Superior Clinical Outcomes Dashboard.
In addition, the Dashboards and Balanced Scorecard were revised to establish metrics for the 2012 depart-mental and interdepartmental Strategic Objectives, related to the six Strategic Focus Areas as identified in the 2012 Strategic Plan. Efforts will continue to provide timely, accurate, and relevant information to all staff, medical staff, and board members regarding performance assessment and improvement priorities through All Staff meetings, dashboards, Balanced Scorecards, Leadership Group meetings, Board meetings, and dis-play in the staff hallway.
The Focused and Ongoing Professional Performance Review Process continued as a part of our competency assessment process, with the continued refinement of “report cards” for each specialty and the acquisition of a database for data collection. It is anticipated that in 2013 committees will further delineate the function and intent of the performance review process, as well as develop a complimentary process to provide more consistency and collaboration in the case review and presentation process.
The 2012 Annual PI Report has been accepted by the Quality Improvement Committee, Medical Executive Committee and the Board of Commissioners. The Performance Assessment and Improvement Program has been acknowledged as effective in its scope and direction. Furthermore, it is the goal of Pullman Regional Hospital to continue to identify opportunities to improve the safety and efficacy of patient care, treatments, and services through effective monitoring and evaluation processes.
The following have been identified as areas of focus for 2013:
Superior Clinical Outcomes
Customer Satisfaction
Employee Engagement
Financial Effectiveness
Partnerships and Collaboration
New and Improved Products and Services
__________________________________ ____________________________
Scott Adams, Chairperson Benno Mohr, MD, President
Quality Improvement Committee Medical Staff
———————————
Tricia Grantham, President
Board of Commissioners

2012 Performance Assessment and Improvement Report 43
Pullman Regional Hospital Employees
Redefining Healthcare
Nurses’ Day Mexican Fiesta
Summit Therapy Open House Safety Committee
Anniversary Party Employee Appreciation Family Night at Zeppoz
“Walk for a Cure”







