MANAGEMENT
LIVER ABSCESS
dr. Samuel Sampetoding, SpB-KBD
Department of Surgery Faculty of Medicine, Universitas Hasanuddin,
Wahidin Sudirohusodo Hospital, Makassar

LIVER ABSCESS?
is an encapsulated collection of suppurative
material within the liver parenchyma,
infected by bacterial, fungal, and/or
parasite
pyogenic liver
abscess
(PLA)
amebic liver
abscess
(ALA)
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
Figure 1. Liver Abscess Huston CD. Sleisenger and Fordtran's Gastrointestinal and Liver Disease (2016)|133

LIVER ABSCESS?
Abses Hepar
Pyogenik
(PLA)
Abses Hepar
Amoebik
(ALA)
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
10th
century
20th
century over the past 100 years has
seen fairly dramatic changes
in demographics, etiology,
diagnosis, and treatment.
↑ immunosuppression
↑ Liver Abscess
incidence
2.3 - 275.4 cases per 100.000

TYPES OF ABSCESS
Fig. 1. The gray areas. Depicts a comparison of the sub-groups of HA and also delineates the areas of overlap between them. Journal of
Clinical and Translational Hepatology 2016 vol. 4 | 158–168

ETIOPATHOGENESIS
Fig. 2. Routes of infection. Journal of Clinical and Translational Hepatology 2016 vol. 4 | 158–168
PLA ALA Pathogen:
• Escherichia coli
• Klebsiella pneumonia DM
• Streptococcus constellatus
immunocompetent
Pathogen:
• Entamoeba hystolitica
• Related to nutritional
status & poor sanitation
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445

Infectious Abscess
Figure 2. Organisms isolated from all positive cultures.
Serraino et al. Medicine (2018) 97:19

ETIOPATHOGENESIS
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
Tabel 1 Etiology of PLA

RISK FACTORS Table 1. Risk factors for development of hepatic abscess (HA) and
increased mortality from HA
Increased risk of
developing HA
Increased mortality
from HA
Diabetes mellitus Malignancy
Liver cirrhosis Diabetes mellitus
Immune-compromised
state Liver cirrhosis
Use of PPI Male gender
Advanced age19 Multiorgan failure16
Male gender*16 Sepsis
Infection with mixed
organisms
HA rupture
Abscess size > 5 cm
Respiratory distress
Hypotension
Jaundice
Extrahepatic involvement16
*Diabetes mellitus, liver cirrhosis and male gender are risk factors for both
development and increased mortality of HA.
Journal of Clinical and Translational
Hepatology 2016 vol. 4 | 158–168

CLINICAL PRESENTATION
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
1
Early presentation non spesific
predormal symptomps: weight
loss, fever, fatigue, malaise, anorexia, and myalgia.
2
Classic triad
• right upper quadrant pain
• fever or chills
• generalized malaise
3 Others
• hepatomegaly • jaundice
1 Asymptomatic >>>
2
Sub-acute
• mild diarrhea to severy dystery
• abdominal pain
3 Others
• high grade fever • RUQ pain
• History of gastroenteritis
• Jaundice (uncommon)
PLA ALA

CLINICAL PRESENTATION
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
Tabel 2 Clinical Presentation of PLA
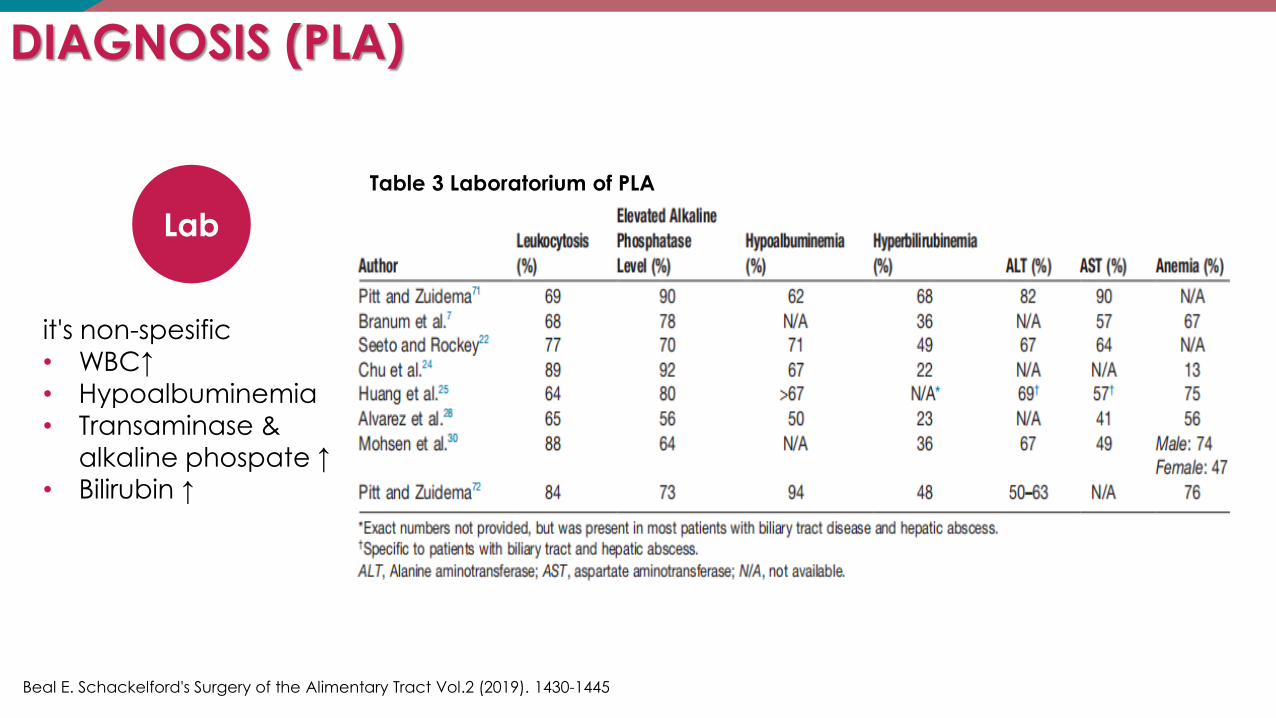
DIAGNOSIS (PLA)
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
it's non-spesific • WBC↑
• Hypoalbuminemia
• Transaminase &
alkaline phospate ↑ • Bilirubin ↑
Lab
Table 3 Laboratorium of PLA

DIAGNOSIS
Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
• elevated right
diaphgrama
• air fluid level w/ gas
forming
subdiaphragmatica
• pleular effusion
• athelectasis
CXR
2
USG
3
• hypoechoic and
varying degrees of
internal echogenicity
• low opacity, reveal rim
and internal
septations
enhancement
CT
Scan
3
MRI
4
• hyperintense on T2-
weighted images and
hypointense on
noncontrast T1-
weighed images, by
gadolinium
demonstrate similar
enhancement on CT
RADIOLOGIC

DIAGNOSIS
Journal of Clinical and Translational Hepatology 2016
vol. 4 | 158–168
3.
4.
Figure 3. Ultrasound (US). A. US demonstrates a hypoechoic abscess with heterogeneous echogenicity centrally consistent with
septations and internal debris (blue arrow). B. Color Doppler US demonstrates peripheral hypervascularity surrounding the abscess
cavity.

DIAGNOSIS
Journal of Clinical and Translational Hepatology
2016 vol. 4 | 158–168 4.
Figure 4 Dynamic contrast-enhanced computed tomography (CT). A. Late arterial phase CT demonstrates hypervascular, peripheral enhancement of the abscess seen in Figure 4 (blue arrow). B. Portal venous phase CT demonstrates conspicuity of internally enhancing septations (blue star), likely representing intervening hepatic
parenchyma. Note the multilocular nature of the abscess, which has implications for potential treatments (blue arrows).

DIAGNOSIS
Journal of Clinical and Translational Hepatology 2016 vol. 4 | 158–
168
4.
Figure 5. Magnetic resonance imaging (MRI).
A. T2-weighted image demonstrates multiple (at least six) small hyperintense abscess cavities
in the right hepatic lobe (blue arrows). Note the hyperintense, edematous hepatic
parenchyma (blue star). B. Noncontrast T1-weighted fat-sat image demonstrates varying
degrees of T1 hyperintensity in the abscess cavities consistent with proteinaceous debris.
C. Postcontrast T1- weighted fat-sat image demonstrates peripheral or rim enhancement
around each of the abscesses.

TREATMENT
4.
Fig. 10. Treatment strategies*. *Adapted from Hope WW, Vrochides DV, Newcomb WL, Mayo-Smith WW, Iannitti DA. Optimal treatment of hepatic abscess. Am Surg
2008;74:178-182.
Journal of Clinical and Translational Hepatology 2016 vol. 4 | 158–168

DRUG THERAPY FOR PLA
4. Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
1 Effective for small abscesses, < 3–5 cm in diameter and smaller abscesses in
difficult anatomical positions
2 Soon as blood obtained for identification of organisms, usually
accomplished a third-generation cephalosporin plus metronidazole or
piperacillin/tazobactam
3 Recommendation: empiric coverage for gram-negative bacilli, gram-
positive cocci, as well as anaerobic
• 3 weeks IV followed 1–2 months PO, or
• 2–3 weeks IV followed 1–2 weeks PO
4 Treatment duration depends on response, as determined by repeat US, and
resolution of fever and leukocytosis

DRUG THERAPY FOR ALA
4. Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
1 Effective for uncomplicated amebic hepatic abscess
2
3
Both amebic colitis and liver abscess—nitroimidazole derivatives (e.g., metronidazole)
Amebic colitis—luminal agents such as paromomycin, diloxanide furoate,
iodoquino

PERCUTANEOUS DRAINAGE
4. Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
1 PD is most common first-line treatment by 16-18 Ga needle aspiration or insertion of 8-14 F pigtail catheter drain under US or CT guidance
2 Benefits: minimally invasive procedure, no need for GA, lower risk of
adhesion formation, contamination, and lower cost in comparing with surgical
3 Failures: multiloculated, catheter blockage by viscous fluid and necrotic
tissue, hypoalbuminemia significant risk
4 Complications: haemorrhage and biliary fistula
5 PD indication for ALA: deterioration in clinical condition despite adequate
treatment, bacterial superinfection, abscess with high risk of rupture

CURRENT UNIT PROTOCOL FOR THE MANAGMENT OF DRAINS PLACED
Liver abscess: contemporary presentation and management in a Western population 23rd February 2018, Volume 131 Number 1470

SURGICAL
4. Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
1 Indication:
• rupture peritonitis difficult access
• co-existing pathology requiring surgery
• larger abscesses (> 3–5 cm)
2
3
Approach: controversy
Type: surgical drainage or resection
(hepatectomy)
Fig. 9. Large solid-cystic multiloculate septate liver abscess in the right lobe
Pais-Costa SR, Araujo SLM, Figueiredo VN. Hepatectomy for pyogenic liver
abscess treatment: exception approach? ABCD Arq Bras Cir Dig.
2018;31(3):e1394.

COMPLICATION
4. Beal E. Schackelford's Surgery of the Alimentary Tract Vol.2 (2019). 1430-1445
Developed
in
15.7% of patients
Septic metastasis leading to extrahepatic complications:
endopthalmitis, septic
pulmonary embolism, infection
of lungs, CNS, and eyes
Abscess rupture: spontaneous
(6.1%), incidence of abscesses by Klebsiella > other bacteria
Erode diaphragm:
causing pleural effusion,
empyema, pneumonia,
pericarditis,
bronchopleural fistulas, or duodenobronchofistulas
MOF

THANKS FOR WATCHING