
Health Care Spending in the United Statesand Other High-Income CountriesIrene Papanicolas, PhD; Liana R. Woskie, MSc; Ashish K. Jha, MD, MPH
IMPORTANCE Health care spending in the United States is a major concern and is higher thanin other high-income countries, but there is little evidence that efforts to reform US healthcare delivery have had a meaningful influence on controlling health care spending and costs.
OBJECTIVE To compare potential drivers of spending, such as structural capacity andutilization, in the United States with those of 10 of the highest-income countries (UnitedKingdom, Canada, Germany, Australia, Japan, Sweden, France, the Netherlands, Switzerland,and Denmark) to gain insight into what the United States can learn from these nations.
EVIDENCE Analysis of data primarily from 2013-2016 from key international organizationsincluding the Organisation for Economic Co-operation and Development (OECD), comparingunderlying differences in structural features, types of health care and social spending, andperformance between the United States and 10 high-income countries. When data were notavailable for a given country or more accurate country-level estimates were available fromsources other than the OECD, country-specific data sources were used.
FINDINGS In 2016, the US spent 17.8% of its gross domestic product on health care, andspending in the other countries ranged from 9.6% (Australia) to 12.4% (Switzerland). Theproportion of the population with health insurance was 90% in the US, lower than the othercountries (range, 99%-100%), and the US had the highest proportion of private healthinsurance (55.3%). For some determinants of health such as smoking, the US ranked secondlowest of the countries (11.4% of the US population �15 years smokes daily; mean of all 11countries, 16.6%), but the US had the highest percentage of adults who were overweight orobese at 70.1% (range for other countries, 23.8%-63.4%; mean of all 11 countries, 55.6%).Life expectancy in the US was the lowest of the 11 countries at 78.8 years (range for othercountries, 80.7-83.9 years; mean of all 11 countries, 81.7 years), and infant mortality was thehighest (5.8 deaths per 1000 live births in the US; 3.6 per 1000 for all 11 countries). The USdid not differ substantially from the other countries in physician workforce (2.6 physicians per1000; 43% primary care physicians), or nursing workforce (11.1 nurses per 1000). The US hadcomparable numbers of hospital beds (2.8 per 1000) but higher utilization of magneticresonance imaging (118 per 1000) and computed tomography (245 per 1000) vs othercountries. The US had similar rates of utilization (US discharges per 100 000 were 192 foracute myocardial infarction, 365 for pneumonia, 230 for chronic obstructive pulmonarydisease; procedures per 100 000 were 204 for hip replacement, 226 for knee replacement,and 79 for coronary artery bypass graft surgery). Administrative costs of care (activitiesrelating to planning, regulating, and managing health systems and services) accounted for 8%in the US vs a range of 1% to 3% in the other countries. For pharmaceutical costs, spendingper capita was $1443 in the US vs a range of $466 to $939 in other countries. Salaries ofphysicians and nurses were higher in the US; for example, generalist physicians salaries were$218 173 in the US compared with a range of $86 607 to $154 126 in the other countries.
CONCLUSIONS AND RELEVANCE The United States spent approximately twice as much asother high-income countries on medical care, yet utilization rates in the United States werelargely similar to those in other nations. Prices of labor and goods, including pharmaceuticals,and administrative costs appeared to be the major drivers of the difference in overall costbetween the United States and other high-income countries. As patients, physicians, policymakers, and legislators actively debate the future of the US health system, data such as theseare needed to inform policy decisions.
JAMA. 2018;319(10):1024-1039. doi:10.1001/jama.2018.1150
Viewpoint page 977 andEditorials pages 983, 986,988, and 990
Animated Summary Video
Supplemental content andAudio
CME Quiz atjamanetwork.com/learning
Author Affiliations: Department ofHealth Policy and Management,Harvard T. H. Chan School of PublicHealth, Boston, Massachusetts(Papanicolas, Woskie, Jha); HarvardGlobal Health Institute, Cambridge,Massachusetts (Papanicolas, Woskie,Jha); Department of Health Policy,London School of Economics andPolitical Science, London, England(Papanicolas, Woskie).
Corresponding Author: IrenePapanicolas, PhD, Department ofHealth Policy, London School ofEconomics and Political Science,Houghton Street, London WC2A2AE, England ([email protected]).
Clinical Review & Education
JAMA | Special Communication
1024 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

T he United States spends more per capita on health carethan any other nation, substantially outpacing even othervery high-income countries.1,2 However, despite its
higher spending, the United States performs poorly in areas suchas health care coverage and health outcomes.3-5 Higher spendingwithout commensurate improved health outcomes at the popula-tion level has been a strong impetus for health care reform in theUnited States.6
Although it is well known that the United States spendsmore on health care than other countries, less is known aboutwhat explains these differences. The consensus has been thatthe US fee-for-service system is a primary factor,7 leading to
fragmentation, overuse, andan underinvestment in socialdeterminants of health,8-10
dr iv ing high uti l izat ion ofhealth care services and pooroutcomes. Older studies havefound that the United Statesmay underinve st in socia lservices,11 although other datasuggest that higher pricesin the United States, especiallyfor pharmaceuticals, may bea contributor to spending dif-ferences.12,13 One study sug-
gested that increasing rates of outpatient spending and remu-neration of clinicians is a major contributor to the cost differencebetween the United States and other countries.14 Given thatother high-income countries are able to spend less and achievebetter health outcomes, a more nuanced, data-driven under-standing of all aspects of health care cost are needed to assist inreform of the US health care system.
The Organisation for Economic Co-operation and Develop-ment (OECD) and the Commonwealth Fund have recently col-lected and made available increasingly comparable data on inputsand performance of the health care systems across high-incomecountries. Using these and related data, we compared perfor-mance of the United States with 10 other high-income countries onkey metrics that underpin health care spending. By examininggranular data, we sought to understand why US health care costsare so much higher and where policy makers might target theirefforts to encourage a more efficient system.
MethodsSelection of Comparison CountriesTen high-income countries were selected for comparison. Thesecountries were chosen because they were among the highest-income countries in the world, had relatively high health carespending, and had populations with similar demographic character-istics that have similar burdens of illness.3,15 Based on these criteria,the United Kingdom (consisting of England, Scotland, Wales, andNorthern Ireland), Canada, Germany, Australia, Japan, Sweden,France, Denmark, the Netherlands, and Switzerland were chosenfor comparison. These 10 selected countries represent differentgeographic areas and diverse health system structures.
Conceptual Framework and Indicator SelectionTo better understand the higher US health care costs relative toother high-income countries, a range of outcomes were explored.We first analyzed comparative data on general health systemspending, including spending by function. Next, comparativeinputs, including labor costs and structural capacity (which,aside from contributing to direct costs, may also influence mainte-nance costs or influence the price to use equipment) were ex-amined. Because many of the leading explanations relating tohigher health care costs involve the transformation of health caredollars to health care outcomes,16 we extended the analysis toexamine a range of intermediate outputs—namely, access, utiliza-tion (inpatient, outpatient, major procedures), pharmaceuticalspending and utilization, patient experience, and quality of care—aswell as valued health system outcomes, such as population health.To provide a broader context of overall factors that can contributeto differences in health care spending, we also examined socialspending, as well as demographic differences, risk factors, andprevalence of disease. In line with previous international compari-sons, the health care system included all groups whose primaryintent is to improve health.5,17
This approach resulted in the presentation of a total of 98 indi-cators across 7 domains: (1) general spending; (2) populationhealth; (3) structural capacity; (4) utilization; (5) pharmaceuticals;(6) access and quality; and (7) equity. In each domain, measureswere selected that were available across the majority of the coun-tries in the analysis. We were unable to find comparable pricingdata for most areas, such as for diagnostic procedures and treat-ments, except for workforce remuneration and pharmaceuticals.In the area of quality, the focus was on indicators that capturedquality of prevention, primary care, and inpatient care across theareas of appropriateness, effectiveness, experience, and safety. Inthe area of access to care, variations related to financial costs aswell as waiting times were explored. In addition, reflecting equity,variations related to service availability, quality of care, and costwere assessed.
Data SourcesData were extracted from a range of databases compiled by inter-national organizations, with the majority coming from the OECD.
JAMA.COM +
Animated Summary VideoHealth Care Spending in theUnited States and OtherHigh-Income Countries
Key PointsQuestion Why is health care spending in the United States somuch greater than in other high-income countries?
Findings In 2016, the United States spent nearly twice as much as10 high-income countries on medical care and performed less wellon many population health outcomes. Contrary to someexplanations for high spending, social spending and health careutilization in the United States did not differ substantially fromother high-income nations. Prices of labor and goods, includingpharmaceuticals and devices, and administrative costs appearedto be the main drivers of the differences in spending.
Meaning Efforts targeting utilization alone are unlikely to reducethe growth in health care spending in the United States; a moreconcerted effort to reduce prices and administrative costsis likely needed.
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1025
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

Data on structural equipment, workforce, utilization, pharmaceuti-cal spending, access, and quality were accessed from OECD.statand the OECD 2015 Health Care at a Glance report. Additionaldata on health spending, health system, and country characteris-tics were obtained from the World Bank International Bank forReconstruction and Development–International DevelopmentAssociation database and the 2016 OECD Health Systems Charac-teristics Survey.
Data on retail pharmaceutical spending per capita wereobtained from the OECD for all countries. Data on total pharmaceu-tical spending per capita were obtained from IntercontinentalMarketing Services or the International Federation of Pharmaceuti-cal Manufacturers and Associations. Pharmaceutical data oncountry-level output of new chemical entities was taken fromDaemmrich.18 Population perceptions of the health system andselect access measures were obtained from the 2016 Common-wealth Fund Survey of Consumers.15
All data on per capita spending, gross domestic product (GDP),and remuneration were translated into US dollar equivalents, withexchange rates based on purchasing power parities of national cur-rencies. Remuneration data were then converted to 2017 dollarsusing the US Consumer Price Index in line with Laugesen andGlied.19 Data on health spending are presented by function of careas a percentage of the country’s total spending on health consis-tent with System of Health Accounts categorization, with adapta-tions for outpatient spending to address issues of comparabilitywith the United States’ National Health Expenditure Accounts(eTable 2 in Supplement 1). When OECD data were not availablefor a given country or more accurate country-level estimates wereavailable, country-specific data sources were used. The focus wason indicators from 2013 onward with an occasional exception. Forexample, for the United States, data for the horizontal index, neo-natal mortality by low birth weight, and antibiotic prescribing werefrom 2009, 2004, and 2004, respectively.
Figure 1. Spending
General
Overall population (in millions)
Rank (highest to lowest) 1 2 3 4 5 6 7 8 9 10 11
Denmark6
CHE8
Sweden10
NLD17
Australia24
Canada36
France64
UK66
Germany83
Japan127
US323
69
Mean
Population ≥65 y, % US14.5
Australia14.7
Canada15.7
NLD17.3
UK17.3
CHE17.5
Denmark18.1
France18.2
Sweden19.9
Germany21.4
Japan25.1
18.2
GDP per capita, US $(in thousands)
Japan37.50
UK38.50
France41.00
Canada42.40
Germany42.90
Australia45.10
NLD46.30
Sweden51.60
US52.10
Denmark53.40
CHE54.00
45.90
Land area (× 1000 sq km) CHE42
NLD42
Denmark43
UK244
Germany357
Japan378
Sweden450
France549
Australia7741
US9834
Canada9985
2697
Poverty rate, % below povertyline of 60%
Denmark12
NLD15
France15
Germany16
CHE17
Sweden17
UK18
Australia20
Canada21
Japan22
US24
18
Total spending on health, % of total national GDP
Australia9.6
UK9.7
Canada10.3
NLD10.5
Denmark10.8
Japan10.9
France11
Germany11.3
Sweden11.9
CHE12.4
US17.8
11.5
Health spending
Public spending on health,% of total national GDP
Australia6.3
Canada7.4
UK7.6
CHE7.7
US8.3
Japan8.6
France8.7
Germany8.7
Denmark9.2
NLD9.5
Sweden10
8.4
Inpatient care Canada17
US19
Sweden21
UK24
Japan27
Germany27
Denmark28
CHE28
France30
Australia31
NLD32
26
Outpatient care NLD22
France23
Germany23
Japan27
UK30
Sweden31
CHE33
Denmark34
Canada36
Australia39
US42
31
Mean spending on healthper capita, US $
UK3377
France3661
Japan3727
Australia4357
Canada4641
Germany5182
NLD5202
Denmark6463
CHE6787
Sweden6808
US9403
5419
Long-term care Australia2
US5
France11
Canada14
Germany16
UK18
Japan19
CHE19
Denmark24
NLD26
Sweden26
16
Medical goods Denmark10
NLD12
Sweden12
CHE13
US14
UK15
Australia17
Japan20
Canada20
France20
Germany20
16
Governance andadministration
Japan1
France1
Denmark2
Sweden2
UK2
Australia3
Canada3
CHE4
NLD4
Germany5
US8
3
Home-based care DenmarkNA
CHENA
Australia0
Canada0
NLD0
Sweden0
Germany1
Japan3
UK3
US3
France4
2
Preventive care Australia2
CHE2
France2
Japan3
Denmark3
Sweden3
Germany3
US3
NLD4
UK5
Canada6
3
Other Denmark0
NLD0
Japan1
CHE1
UK3
Canada4
Sweden5
Germany5
Australia6
US6
France9
4
Health expenditure by function of care as a % of total national health expenditure
Population with health carecoverage, %
Australia100
Japan100
Canada100
Denmark100
CHE100
NLD99.9
France99.9
Sweden100
Germany99.8
UK100
US90
99
GDP indicates gross domestic product; NA, not applicable. CHE indicates Switzerland; NLD, the Netherlands. See eTable 1 in Supplement 2 for data ordered by country.
Clinical Review & Education Special Communication Health Care Spending in the United States and Other High-Income Countries
1026 JAMA March 13, 2018 Volume 319, Number 10 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

Supplement 1 includes tables that provide a breakdown ofsources and methods for the data reported herein. In these tables,we note issues of comparability and timeliness for each indicator,such as workforce. In figures describing data for each of the 7 do-mains, a simple mean of the data for each indicator across all 11 coun-tries is presented in the final column. Throughout the Results sec-tion in the text, all comparative findings are presented descriptively.
ResultsDemographic Characteristics and Health Care SpendingIn 2016, the US population was significantly larger than allcomparison countries at 323 million (Figure 1 and eTable 1 inSupplement 2). Japan had the next largest population with 127 mil-lion. The US system also covered the second largest geographicalarea (9 834 000 sq km), following Canada (9 985 000 sq km). Theother countries other than Australia had much smaller land mass.In 2016, the United States spent 17.8% of its GDP on health care(range of the other countries, 9.6%-12.4%; mean of all 11 countries,11.5%) (Figure 1 and Figure 2) and had almost double the healthspending per capita (mean, $9403) compared with the other coun-tries (range, $3377-$6808; mean of all 11 countries, $5419).Although the United States spent more, the percentage of thepopulation with health insurance in the United States was 90%,lower than in all of the other countries (range, 99%-100%).
All systems had relatively similar levels of public spending as apercentage of GDP (defined as spending from government and/orsocial or compulsory insurance funds), with the United States spend-ing at about the mean level (8.3%) of all the countries, although, un-like the other countries, this spending covered only about 37% ofthe population. By expenditure as a function of care, the UnitedStates spent only 19% of its health spending on inpatient care, whichexcludes same-day hospital care. This proportion was less than thatof all other countries, with Australia (31%) and the Netherlands (32%)spending the most (Figure 1). The United States spent a greater pro-portion than the other countries on outpatient care (44% com-pared with a mean of 31%) and governance and administration, whichincludes activities relating to planning, regulating, and managinghealth systems and services (8% compared with a mean of 3%).
Across the 11 countries, the United States had the lowest per-centage of the population older than 65 years (14.5% compared witha mean of 18.2%) and also had the highest rate of poverty, with 24%of the population living below the poverty line, followed by Japan(22%) and Canada (21%). The United States ranked below the meanbut was not an outlier with regard to total social spending (spend-ing on old age, incapacity, labor market, education, family, and hous-ing [Figure 3]) at 16.7% of GDP (compared with a mean of 19.4% ofGDP in all 11 countries). This reflected public social spending, whichwas, at 11.3% of GDP, below the mean of all 11 countries (15.3% ofGDP). The United States ranked fourth with regard to private socialspending at 5.4% of GDP (compared with a mean of 4.1%) and wassimilar to the United Kingdom (5.6%) and ranked behindthe Netherlands (7.1%) and Switzerland (6.0%), reflecting mostlyprivate pension payments.20
Insurance System CharacteristicsThe structural characteristics of the health care system are de-tailed in the Table. Three countries, the United Kingdom, Sweden,and Denmark, have national health care systems, whereasCanada and Australia have regionally administered universal insur-ance programs. Germany, France, the Netherlands, and Switzerlandhave statutory/mandatory health insurance systems. Only theUnited States has a voluntary, private employer-based andindividual-based system. All of the countries except the UnitedStates have an automatic or compulsory enrollment process.Private insurance as the primary form of insurance is highest in theUnited States at 55.3%, followed by Germany at 10.8%. The major-ity of the countries do not have private insurance as the primaryform of insurance.
Population HealthAmong important determinants of health, the United States had thehighest percentage of overweight or obese adults (70.1% com-pared with a mean of 55.6%) but had relatively low smoking rates(11.4% of the population compared with a mean of 16.6%) (Figure 4and eTable 2 in Supplement 2). The drinking rate (8.8 L per capita)and unemployment rate (4.4%) in the United States are bothclose to the mean values of all 11 countries at 9.1 L per capita and5.4%, respectively.
Figure 2. Health Spending as a Percentage of Gross Domestic Product
20
8
10
12
14
16
18
6
4
2
0
Spen
ding
on
Hea
lth
as a
% o
f GDP
UnitedStates
UnitedKingdom
CanadaGermany AustraliaJapanSweden France TheNetherlands
Switzerland Denmark
Total health spending Government health spending Private health spendingMean Mean Mean
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1027
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

The United States consistently had the poorest populationhealth outcomes (Figure 4). The United States had the lowest lifeexpectancy (78.8 years compared with a mean of 81.7 years) andthe lowest health-adjusted life expectancy (69.1 years comparedwith a mean of 72.0 years). The variability of life expectancy acrossthe United States (ranging from 81.3 years in Hawaii to 75 years inMississippi) (eTable 3 in Supplement 1) was similar to that of the lifeexpectancy across all countries in the study.
The United States had the highest infant mortality (5.8 deathsper 1000 live births compared with a mean of 3.6), neonatal mor-tality (4.0 deaths per 1000 live births compared with a mean of 2.6),and maternal mortality (26.4 deaths per 100 000 live births com-pared with a mean of 8.4) (Figure 4). The United States also had thesecond highest percentage of infants with low birth weight (8.1%compared with a mean of 6.6%). Japan had the highest low birthweight (9.5%). When adjusting neonatal mortality to exclude deathsof infants born weighing less than 1000 g, the United States rankedfifth relative to the other countries, with 1.61 deaths per 1000 livebirths, compared with a mean of 1.70 for all 11 countries.
Workforce and Structural CapacityThe physician workforce in the United States was lower than themean of all 11 countries at 2.6 per 1000 population compared with3.3 per 1000 population (Figure 5 and eTable 3 in Supplement 2).The proportion of US physicians who were primary care physicians(43%) was the same as the mean of all 11 countries. Using a func-tionality-based approach to identifying primary care physicians,US general internists provided a significant amount of primary care,whereas internists in Canada almost exclusively provided acutehospital-based care (Figure 6). Compared with countries withcomparable data, mean remuneration of generalists, special-
ists, and nurses was higher in the United States. When adjustingfor purchasing power parity, the mean US remuneration for gener-alists was $218 173, nearly double the mean remuneration in all 11countries, which ranged from $86 607 in Sweden to $154 126 inGermany. The remuneration for specialists was higher in the UnitedStates at $316 000 compared with other countries, ranging from$98 452 in Sweden to $202 291 in Australia). The remuneration ofnurses was also higher in the United States ($74 160) than in othercountries, where it ranged from $42 492 in France to $65 082 in theNetherlands. The remuneration of health care professionals as a ra-tio to the mean national wage was highest in the United States forspecialists (5.3 compared with a mean of 3.7), generalists (3.6 com-pared with a mean of 2.7), and nurses (1.23 compared witha mean of 1.1).
There was notable variation between countries in the supply ofmedical equipment, such as magnetic resonance imaging (MRI) units,computed tomography (CT) machines, and mammography ma-chines. Japan had the highest number of MRI units and CT scannersper population (approximately 52 and 107 per 1 million population, re-spectively), and the United States had the second highest for MRI(38 per 1 million population) and third highest for CT (41 per 1 millionpopulation). The lowest per capita rate for both MRI units and CT scan-ners was in the United Kingdom, with 7.2 MRI units and 9.5 CT scan-ners per 1 million population. The United States had fewer hospitalbeds per 1000 population (2.8) than Japan (13.2) and Germany (8.2)and fewer long-term beds per 1000 population older than 65 years(38.8) compared with the mean of the study countries (54.2).
UtilizationThe United States’ utilization of health care services was similarto the other countries (Figure 7 and eTable 4 in Supplement 2),
Figure 3. Social Spending as a Percentage of Gross Domestic Product
30
20
25
15
10
5
0
Soci
al S
pend
ing
as a
% o
f GDP
UnitedStates
UnitedKingdom
Germany Sweden France TheNetherlands
Switzerland Denmark Canada Japan Australia
Total social spendingMean
Public social spendingMean
Private social spendingMean
Social spending is the provision by public (and private) institutions of benefits toand financial contributions targeted at households and individuals to providesupport during circumstances that adversely affect their welfare, provided thatthe provision of the benefits and financial contributions constitutes neither adirect payment for a particular good or service nor an individual contract ortransfer. Such benefits can be cash transfers or can be direct (in-kind) provisionof goods and services. Main spending areas include old age, health, family,incapacity, labor market, and housing (Organisation for Economic Co-operationand Development). Private social spending is functionally the same as publicsocial spending but provided through a private mechanism. Social benefits
delivered through the private sector (not transfers between individuals) involvean element of compulsion and/or interpersonal redistribution; for example,through pooling of contributions and risk sharing. This may include old-agepensions and support services for older adults, survivor benefits, disability andsickness cash benefits, family support, unemployment benefits, housingsupport (eg, rent subsidies), and other social policy areas excluding healthspending. Pensions constitute an important part of private social spending inthe United States and can be mandatory or voluntary. Independent,out-of-pocket spending on social services is not included.
Clinical Review & Education Special Communication Health Care Spending in the United States and Other High-Income Countries
1028 JAMA March 13, 2018 Volume 319, Number 10 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

Tabl
e.In
sura
nce
Syst
emCh
arac
teris
tics
Char
acte
ristic
s
Coun
try
Unite
dSt
ates
Unite
dKi
ngdo
ma
Germ
any
Swed
enFr
ance
The
Net
herl
ands
Switz
erla
ndDe
nmar
kCa
nada
Japa
nAu
stra
lia
Gene
ral
Mai
nso
urce
ofba
sic
care
cove
rage
sb
Priv
ate
empl
oyer
-bas
edan
din
divi
dual
insu
ranc
e
Nat
iona
lhea
lthca
resy
stem
Stat
utor
yhe
alth
insu
ranc
esy
stem
Nat
iona
lhea
lth
care
syst
emSt
atut
ory
heal
thin
sura
nce
syst
em
Man
dato
ryhe
alth
insu
ranc
esy
stem
Man
dato
ryhe
alth
insu
ranc
esy
stem
Nat
iona
lhea
lthca
resy
stem
Regi
onal
lyad
min
iste
red
univ
ersa
lpub
licin
sura
nce
prog
ram
Stat
utor
yhe
alth
insu
ranc
esy
stem
Regi
onal
lyad
min
iste
red
univ
ersa
lpub
licin
sura
nce
prog
ram
Enro
llmen
tpro
cess
forb
asic
care
cove
rage
c
Volu
ntar
yAu
tom
atic
Com
puls
ory
Auto
mat
icCo
mpu
lsor
yCo
mpu
lsor
y;un
iver
sally
man
date
dpr
ivat
ein
sura
nce
Com
puls
ory;
univ
ersa
llym
anda
ted
priv
ate
insu
ranc
e
Auto
mat
icAu
tom
atic
Com
puls
ory
Auto
mat
ic
No.
ofin
sure
rsfo
rin
sura
nce-
type
syst
emsd
880
Firm
s;53
79es
tabl
ishm
ents
NA
118
Sick
ness
fund
sN
A3 N
onco
mpe
ting
insu
ranc
esc
hem
es
60In
sura
nce
plan
s52
Insu
ranc
epl
ans
NA
NA
>340
0N
onco
mpe
ting
publ
ic,q
uasi
-pub
lic,
and
empl
oyer
-bas
edin
sure
rs
NA
Priv
ate
byty
pe,%
ofto
talp
opul
atio
ne
Priv
ate
aspr
imar
yfo
rmof
insu
ranc
e55
.30
10.8
NA
00
00
NA
NA
0
Dupl
icat
ive,
supp
lem
enta
ry,o
rco
mpl
imen
tary
insu
ranc
e
7.7
10.6
23.1
1095
.584
.127
.936
.567
NA
32.0
Abbr
evia
tion:
NA,
nota
pplic
able
.a
The
info
rmat
ion
inth
issp
ecifi
ctab
lere
fers
only
toEn
glan
d,no
tthe
entir
eU
nite
dKi
ngdo
m.
bU
nite
dSt
ates
:pub
lic(M
edic
are)
fora
ges�
65;s
tate
-adm
inist
ered
publ
ic(M
edic
aid)
forl
owin
com
e.c
Uni
ted
Stat
es:c
ompu
lsory
from
2014
to20
17.
dU
nite
dSt
ates
:an
esta
blish
men
tisd
efin
edas
asin
gle
phys
ical
loca
tion
whe
rebu
sines
sisc
ondu
cted
orw
here
serv
ices
orin
dust
rialo
pera
tions
are
perf
orm
ed.
eD
uplic
ate:
priv
ate
insu
ranc
eth
atof
fers
cove
rage
forh
ealth
serv
ices
alre
ady
incl
uded
unde
rpub
liche
alth
insu
ranc
e.D
uplic
ate
heal
thin
sura
nce
can
bem
arke
ted
asan
optio
nto
the
publ
icse
ctor
beca
use,
whi
leit
offe
rsac
cess
toth
esa
me
med
ical
serv
ices
asth
epu
blic
sche
me,
ital
soof
fers
acce
ssto
diffe
rent
prov
ider
sorl
evel
sofs
ervi
ce,s
uch
as(1
)acc
esst
opr
ivat
ehe
alth
faci
litie
stha
tare
nota
cces
sible
thro
ugh
publ
icin
sura
nce
whe
nth
efu
llcos
toft
hese
rvic
eis
paid
bypr
ivat
ein
sura
nce;
(2)a
cces
sto
fast
/priv
ilege
dco
vera
geby
bypa
ssin
gqu
eues
inpu
blic
syst
em;(
3)ac
cess
toca
rein
depe
nden
tofr
efer
rala
ndga
teke
eper
syst
ems;
(4)c
hoic
eof
phys
icia
n,ho
spita
l,or
othe
rhea
lthca
repr
ovid
er.I
tdoe
snot
exem
ptin
divi
dual
sfro
mco
ntrib
utin
gto
publ
iche
alth
insu
ranc
e.Su
pple
men
tary
:priv
ate
heal
thin
sura
nce
that
prov
ides
cove
rage
fora
dditi
onal
heal
thse
rvic
esno
tcov
ered
byth
epu
blic
sche
me.
Dep
endi
ngon
the
coun
try,
itm
ayin
clud
ese
rvic
esth
atar
eun
cove
red
byth
epu
blic
syst
emsu
chas
luxu
ryca
re,e
lect
ive
care
,lon
g-te
rmca
re,d
enta
lcar
e,ph
arm
aceu
tical
s,re
habi
litat
ion,
alte
rnat
ive
orco
mpl
emen
tary
med
icin
e,et
c,or
supe
riorh
otel
and
amen
ityho
spita
lser
vice
s(e
ven
whe
not
herp
ortio
nsof
the
serv
ice,
such
asth
em
edic
alco
mpo
nent
,are
cove
red
byth
epu
blic
syst
em).
Com
plim
enta
ry:p
rivat
ein
sura
nce
that
com
plem
ents
cove
rage
ofpu
blic
lyin
sure
dse
rvic
esor
serv
ices
with
inpr
inci
pal/s
ubst
itute
heal
thin
sura
nce,
whi
chis
inte
nded
topa
yon
lya
prop
ortio
nof
qual
ifyin
gca
reco
sts,
byco
verin
gal
lorp
arto
fthe
resid
ualc
osts
noto
ther
wise
reim
burs
ed(e
g,co
-pay
men
ts).
May
bere
ferr
edto
as“s
uppl
emen
tary
”in
US
liter
atur
e.
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1029
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

except for imaging. The United States performed the second high-est number of MRI scans and the highest number of CT scans (118MRIs per 1000 population compared with a mean in all 11 countriesof 82 per 1000 population; 245 CTs per 1000 population com-pared with a mean of 151 per 1000 population).
Annual hospital discharges in the United States, at 125 per 1000population, were just below the middle of the distribution (rangingfrom 84 per 1000 in Canada to 255 per 1000 in Germany, with amean of 150 per 1000 in all 11 countries) (Figure 8). Discharges forcommon conditions in the United States such as acute myocardialinfarction (192 per 100 000 population compared with a mean of190 per 100 000 population), pneumonia (365 per 100 000 popu-lation compared with a mean of 352 per 100 000 population), andchronic obstructive pulmonary disease (230 per 100 000 popula-tion compared with a mean of 206 per 100 000 population) weresimilar to the means of all 11 countries. For discharges for mental andbehavioral conditions, the United States was below the mean of all11 countries (679 per 100 000 population compared with a meanof 736 per 100 000 population) (Figure 7). Consultation levels in theUnited States were below the mean at 4 visits per person per yearcompared with a mean of 6.6 (Figure 8).
The United States had somewhat higher levels of some com-mon surgical procedures, such as revascularization procedures (forcoronary artery bypass procedures, 79 per 100 000 population com-pared with a mean of 54 per 100 000 population), knee replace-ments (226 per 100 000 population compared with a mean of 163
per 100 000 population), cesarean deliveries (33 per 100 live birthscompared with a mean of 25 per 100 live births), coronary angio-plasties (248 per 100 000 population compared with a mean of 217per 100 000 population), and cataract surgeries (1110 per 100 000population compared with a mean of 971 per 100 000 popula-tion). For a few procedures, the United States had comparable orlower rates vs the other 10 countries, such as for hip replacements(204 per 100 000 population compared with a mean in all 11 coun-tries of 207 per 100 000 population).
Length of stay had less variation across countries with the ex-ception of Japan, which had a mean all-cause length of stay of 16.9days, far longer than in the other countries (Figure 8). The UnitedStates had relatively fewer days in the hospital compared with themean for 3 different length-of-stay measures (all-cause hospitaliza-tion, normal neonatal delivery hospitalization, and acute myocar-dial infarction hospitalization) (Figure 7).
The United States had high levels of administrative burden; thiswas notable in particular for administrative spending, for which theUnited States was an outlier (8% of GDP spent on administration andgovernance compared with a mean of 3% of GDP) (eTable 1 inSupplement 1). Physicians in the United States also reported hav-ing a higher level of administrative burden than the mean of all 11countries in 3 areas; however, this burden was high in all insurance-based systems. Fifty-four percent of surveyed physicians in theUnited States identified time spent on administrative issues re-lated to insurance or claims as a major problem, 33% reported that
Figure 4. Population Health
Smoking, % of populationaged ≥15 y who smoke daily
1 2 3 4 5 6 7 8 9 10 11
Sweden11.2
US11.4
Australia12.4
Canada14
UK16.1
Denmark17
Japan18.2
NLD19
CHE20.4
Germany20.9
France22.4
16.6
Mean
Alcohol consumption, L percapita in population aged ≥15 y
Japan7.2
Sweden7.2
NLD8
Canada8.1
US8.8
Denmark9.4
CHE9.5
UK9.5
Australia9.7
Germany11
France11.9
9.1
Obese or overweight, % ofpopulation aged ≥15 y
Japan23.8
France49
Germany60
Canada60.3
UK62.9
Australia63.4
US70.1
CHE41a
Denmark47.4a
NLD47.4a
Sweden48.3a
55.6
Rank (highest to lowest)Determinants of health
Life expectancy in totalpopulation at birth, mean, y
US78.8
Germany80.7
Denmark80.8
UK81
NLD81.6
Canada81.7
Sweden82.3
France82.4
Australia82.5
CHE83
Japan83.9
81.7
Health-adjusted lifeexpectancy, mean, y
US69.1
Denmark71.2
Germany71.3
UK71.4
Australia71.9
Sweden72
NLD72.2
Canada72.3
France72.6
CHE73.1
Japan74.9
72
Life expectancy for womenaged ≥40 y, mean, y
US42.6
Denmark43.4
UK43.7
NLD43.9
Germany43.9
Canada44.8
Sweden44.8
Australia45.4
CHE45.8
France46.4
Japan47.7
44.8
Life expectancy for menaged ≥40 y, mean, y
US38.7
Germany39.4
Denmark39.8
UK40.5
France40.6
NLD40.8
Canada41.1
Sweden41.5
Australia41.7
Japan41.8
CHE42
40.7
Life expectancy
Infant mortality, deaths per1000 live births
Japan2.1
NLD2.5
Sweden2.5
Australia3.2
Germany3.3
Denmark3.7
France3.8
CHE3.9
UK3.9
Canada5.1
US5.8
3.6
Neonatal mortality, deaths per1000 live births
Japan0.9
Sweden1.7
Australia2.3
Germany2.3
NLD2.5
France2.6
UK2.7
Denmark3
CHE3.1
Canada3.2
US4
2.6
Maternal mortality, deaths per100 000 live births
Denmark4.2
Sweden4.4
Australia5.5
CHE5.8
Japan6.4
NLD6.7
Canada7.3
France7.8
Germany9
UK9.2
US26.4
8.4
Neonatal mortality, deaths per1000 live births excluding <1000 g
AustraliaNA
JapanNA
CHENA
FranceNA
Germany1.49
Sweden1.56
US1.61
Canada1.63
UK1.77
NLD1.96
Denmark2.09
1.7
Low birth weight, % of totallive births
CHENA
Sweden4.4
Denmark5
France6.2
Canada6.3
Australia6.4
NLD6.5
Germany6.6
UK6.9
US8.1
Japan9.5
6.6
Maternal and infant health
NA indicates not applicable. CHE indicates Switzerland; NLD, the Netherlands. See eTable 2 in Supplement 2 for data ordered by country.a Patient self-reported data.
Clinical Review & Education Special Communication Health Care Spending in the United States and Other High-Income Countries
1030 JAMA March 13, 2018 Volume 319, Number 10 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

“time spent on administrative issues related to reporting clinical orquality data to government or other agencies is a major problem,”and 16% reported having spent “a lot of time on paperwork or dis-putes related to medical bills.”
PharmaceuticalsAmong the 11 countries, the United States had the highest pharma-ceutical spending per capita at $1443, with Switzerland following at$939 and a mean of $749 for all 11 countries (Figure 9 and eTable 5in Supplement 2). Retail spending per capita was also highest in theUnited States at $1026, representing about 71% of the total, whichwas consistent with the group mean at 72% (Figure 9). For 4 phar-maceuticals (Crestor, Lantus, Advair, and Humira) used for com-mon conditions, the United States had higher prices than all other
countries; for 3 of these, the US price was more than double thenext highest price. With respect to a measure of innovation, theUnited States and Switzerland had the highest number of newchemical entities at 111 and 26, respectively. The United Statesaccounted for 57% of total global production of new chemical enti-ties. No estimates were available for Canada, Australia, Sweden,the Netherlands, and Denmark. The United States also had highgeneric penetration at 84% of the total pharmaceutical market,which was comparable with markets in the United Kingdom andGermany. Australia and the Netherlands had low generic penetra-tion at 30% and 17%, respectively. Despite having the highest rateof generic penetration, the amount that the United States spenton generic products as a percentage of total pharmaceutical spend-ing was similar to other countries, suggesting that brand-name
Figure 5. Workforce and Structural Capacity
Magnetic resonanceimaging units
DenmarkNA
CHENA
SwedenNA
UK7.2
Canada8.9
France12.6
NLD12.9
Australia14.7
Germany30.5
US38.1
Japan51.7
22
Computed tomographyunits
SwedenNA
UK9.5
Canada12.7
NLD13.3
France16.6
Germany35.3
CHE36.1
Denmark37.1
US41
Australia56.1
Japan107.2
36.5
Mammography machineunits
NLDNA
SwedenNA
GermanyNA
France7.5
Denmark14.2
Canada17.3
UK21
Australia23
CHE28.3
Japan33
US43.3
23.5
Overall physicians per1000 population
Rank (highest to lowest)Practicing workforce
1 2 3 4 5 6 7 8 9 10 11
UK2.1
Japan2.4
Canada2.6
US2.6
France3.1
Australia3.5
NLD3.5
Denmark3.6
Germany4.1
Sweden4.2
CHE4.3
3.3
Mean
Primary care physicians,% of total
Denmark22
Sweden33
Japan43
US43
Australia45
Germany45
UK45
NLD47
Canada48
CHE48
France54
43
Specialists, % of total France46
Canada52
CHE52
NLD53
Australia55
Germany55
UK55
Japan57
US57
Sweden67
Denmark78
57
Nurses per 1000 population UK8.2
France9.4
Canada9.5
Japan10.5
US11.1
Sweden11.2
Australia11.5
NLD12.1
Germany13
Denmark16.3
CHE17.4
11.8
Generalist physicians DenmarkNA
CHENA
Sweden86 607
Australia108 564
NLD109 586
France111 769
Japan124 558a
UK134 671
Canada146 286
Germany154 126
US218 173
133 723
Specialist physicians CHENA
Sweden98 452
JapanaDenmark140 505
France153 180
UK171 987
Germany181 243
Canada188 260
NLD191 995
Australia202 291
US316 000
182 657
Nurses SwedenNA
CHENA
France42 492
Japan44 712
UK49 894
Germany53 668
Canada55 349
Denmark58 891
Australia64 357
NLD65 082
US74 160
51 795
Ratio of generalistremuneration to mean wage
JapanNA
DenmarkNA
CHENA
Sweden2
Australia2.1
NLD2.1
France2.6
Canada3.0
UK3.1
Germany3.3
US3.6
2.7
Ratio of specialistsremuneration to mean wage
JapanNA
CHENA
Sweden2.3
Denmark2.6
UK3.4
NLD3.6
France3.6
Australia3.8
Canada3.9
Germany3.9
US5.3
3.7
Non–health-specific annualwage, meanb
Japan39 113
Sweden42 816
UK42 835
France42 992
Germany46 389
Canada48 403
Australia52 063
Denmark52 580
NLD52 833
CHE60 124
US60 154
49 118
Ratio of nurse remunerationto mean wage
CHENA
SwedenNA
France0.99
Denmark1.12
Japan1.14
Canada1.14
Germany1.16
UK1.16
NLD1.23
US1.23
Australia1.24
1.1
Hospital beds per 1000population
Sweden2.5
Canada2.7
Denmark2.7
UK2.7
US2.8
NLD3.3
Australia3.8
CHE4.6
France6.1
Germany8.2
Japan13.2
4.8
Long-term beds per 1000population aged ≥65 y
Japan35.1
US38.8
Denmark48.9
UK49.5
Germany53.1
Canada53.7
Australia54
France59
NLD65.5
CHE67.6
Sweden70.6
54.2
Equipment per 1 million population
Workforce remuneration, US $
Beds
NA indicates not applicable. CHE indicates Switzerland; NLD, the Netherlands.See eTable 3 in Supplement 2 for data ordered by country. Generalist physiciansare defined as any practicing physician registered in his or her country asa generalist physician or a specialist in the field of family medicine, pediatrics,geriatrics, or internal medicine and excludes students, interns, andnonpracticing physicians. Remuneration numbers may be an underestimate insome countries (eg, Canada) because they do not account for practice expenses
for self-employed physicians. Japan is excluded from remuneration means withthe exception of nursing. Definitions of specialist and generalist physiciansin regard to remuneration were taken from the Organisation for EconomicCo-operation and Development.a The number for Japan, 124 558, is a combined total of generalists and specialists.b In 2016 constant prices at 2016 US dollar purchasing power parities.
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1031
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

pharmaceuticals were largely responsible for high overall spending.These countries have notably different ways in how they financepharmaceuticals; there is considerable variation in both the sharecovered by private insurance and the percentage covered by pri-vate out-of-pocket spending. The United States had high levels ofprivate spending (36% compared with a mean of 8%), althoughsimilar to Canada (30%), and was below the mean for out-of-pocket spending at 30% (compared with a mean of 36%). Withregard to antibiotic prescriptions, which are often considered ameasure of inappropriate treatment, the United States was abovethe mean, with a defined daily dose (average maintenance doseper day for a drug used for its main indication in adults) of 24 com-pared with a mean of 20.2.
Access and QualityRelative to comparison countries, US performance varied on qual-ity and access measures (Figure 10 and eTable 6 in Supplement 2).Of the other countries examined, the United States was the only onein which a sizeable minority (approximately 10%) of individualslacked coverage for basic health care services (Figure 1). For the 3access measures (ability to get same- or next-day care when sick,2-month wait time to see a specialist, and adequate time spent withregular physician) the United States generally performed better thanthe other countries. In the United States, 51% were able to get same-or next-day care compared with a mean of 57% in all 11 countries. Inthe United States, 6% had a wait time of 2 months or more to see aspecialist compared with mean of 13% in all 11 countries. Waitingtimes to see a specialist were longer for national health serviceand single-payer systems (ie, percentage with wait times longerthan 2 months: Canada, 39%; United Kingdom, 19%; Sweden, 19%)compared with insurance-based systems (Netherlands, 7%;Switzerland, 9%; Germany, 3%; France, 4%), with a mean of 13%.The United States ranked near the mean for patients reporting hav-
ing spent adequate time with their regular physician (81% com-pared with a mean of 83% in all 11 countries).
The United States had relatively high screening rates for breastcancer (81% compared with a mean of 67% in all 11 countries) butlower rates of measles immunization (92% compared with a meanof 94%) (Figure 10). The United States had considerably lower ratesof all 4 clinical outcome measures than the other countries. Thirty-day mortality for ischemic stroke was 4.2 per 100 patients in theUnited States compared with a mean of 7.9 per 100 patients in all 11countries. For obstetric trauma without instrument, the United Stateshad 1.5 cases per 100 deliveries, whereas the mean was 2.3 per 100deliveries in all 11 countries. The United States had high avoidablehospitalizations for diabetes and asthma relative to comparisoncountries (191.0 per 100 000 population compared with a mean of125.6 per 100 000 population for diabetes, and 89.7 per 100 000population compared with a mean of 42.4 per 100 000 popula-tion for asthma). When accounting for disease prevalence, the rateof US hospitalizations for diabetes was similar to that of other coun-tries, although hospitalizations for asthma were highest in the UnitedStates, closely followed by the United Kingdom. Relative to the othercountries, the US public reported the lowest satisfaction with theirhealth system, with only 19% reporting that the system works well.
US Disaggregated DataWhen access and quality measures were disaggregated by payer,the United States performed slightly worse for those covered byMedicaid, but performance was uneven across insurance groups(eTable 4 in Supplement 1). Nine percent of both privately insuredindividuals and those insured by Medicaid reported a 2-month waittime to see a specialist; this was lower than rates for Medicarepatients (11%) but higher than for uninsured individuals (8%). Onselected prevention measures, such as measles immunization, pri-vately insured individuals had the highest rate of coverage at 95%,
Figure 6. Practicing Physicians by Primary Care Specialization
100
80
60
40
20
0
Phys
icia
ns, %
Specialist
Obstetrics andgynecology
Geriatrics
Pediatrics
Internal medicine
Family medicine
Generalist, notfurther specified
AustraliaJapanCanadaDenmarkSwitzerlandNetherlandsFranceSwedenGermanyUnitedKingdom
UnitedStates
The total number of physicians, or 100%, differs for each country. Data are 2017or closest available year. A functionality-based definition to identify primarycare was used to identify physicians as those who provide a set of activitieswhose functions define the boundaries of primary care. This included chronic,preventive, and acute care in both inpatient and outpatient settings irrespectiveof disease: disease prevention, early detection and diagnosis, treatment andmanagement, care coordination and integration, and health maintenance,counseling, and/or patient education. The clinicians were often a patient’s first
point of contact for the health system with some degree of longitudinalresponsibility for the patient. This definition was used to reach out to countryexperts and identify who is considered a primary care clinician in eachrespective country. National workforce data or Eurostat data, where available,was then categorized according to expert responses. Physicians specializing inobstetrics and gynecology are categorized as specialists for all countries buthave their own category in this figure.
Clinical Review & Education Special Communication Health Care Spending in the United States and Other High-Income Countries
1032 JAMA March 13, 2018 Volume 319, Number 10 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

whereas for breast screening, Medicare beneficiaries had the high-est rates (82%). Conversely, Medicare beneficiaries had the highestrates of mortality for both ischemic stroke and acute myocardialinfarction. There was also variability in avoidable admissions:patients with Medicaid insurance had the highest number ofasthma-related admissions and Medicare beneficiaries had thehighest number of admissions for diabetes. When disaggregatedby income or race, life expectancy was significantly differentamong US groups, with nonwhite and poorer populations havingshorter life expectancies (eTables 3 and 4 in Supplement 1).
EquityThe United States had the highest horizontal inequity, indicatingthe most inequitable access to physicians when adjusted for need. TheUnited States had an 11% rate of out-of-pocket spending as a percent-age of total national health spending (compared with a mean of13% in all 11 countries) and a 2.6% rate as a percentage of house-hold consumption (compared with a mean of 2.4%) (Figure 11 andeTable 7 in Supplement 2). However, the United States had a higherproportion of unmet need in the population, with 22.3% of the popu-
lation reporting that they missed a consultation because of cost com-pared with the mean of 9.4% for all 11 study countries. Given that thesystem has free access at the point of entry, the United Kingdom re-ported one of the lowest levels of barriers to accessing health ser-vices, but the level was higher than in both Germany and Sweden.
DiscussionIn this study based on data primarily from 2013-2016, the UnitedStates spent approximately twice as much as other high-incomecountries on medical care and fared worse on common populationhealth outcomes such as life expectancy and infant mortality. How-ever, the main findings of this comparison were that, contrary tosome explanations for high spending, US social spending and healthcare utilization were relatively similar to other high-income na-tions. Although utilization of some surgical procedures (such as coro-nary angioplasty, total knee replacement, and cesarean delivery) washigher in the United States, this utilization did not appear to ex-plain a large part of the higher spending in the United States.
Figure 7. Utilization
Discharges per 100 000 population
Acute myocardial infarction
Rank (highest to lowest) 1 2 3 4 5 6 7 8 9 10 11
Japan89
France124
UK160
Denmark174
NLD175
US192
Canada193
Australia196
CHE223
Sweden273
Germany287
190
Mean
Mental and behavioral NLD119
UK269
Japan319
France368
Canada629
US679
Australia856
Denmark892
Sweden1068
CHE1182
Germany1719
736
Pneumonia Canada187
NLD224
CHE269
France271
Australia338
US365
Japan378
Germany380
Sweden432
UK459
Denmark567
352
Chronic obstructivepulmonary disease
Japan45
France138
CHE142
NLD161
Sweden186
US230
Denmark234
Canada241
UK251
Australia286
Germany352
206
Magnetic resonance imaging SwedenNA
Australia41
NLD52
UK53
Canada56
CHE70
Denmark82
France105
Japan112
US118
Germany131
82
Examinations per 1000 population
Computed tomography SwedenNA
UK79
NLD81
CHE100
Australia120
Germany144
Canada153
Denmark162
France197
Japan231
US245
151
Total hip replacementper 100 000 population
Japan90
Canada136
Australia171
UK183
US204
NLD216
Sweden234
France236
Denmark237
Germany283
CHE292
207
Total knee replacementper 100 000 population
JapanNA
NLD118
Sweden124
UK141
France145
Canada166
Denmark168
CHE176
Australia180
Germany190
US226
163
Hysterectomy per 100 000women
JapanNA
UK161
NLD167
France182
Sweden186
Denmark197
Canada232
Australia262
US266
CHE291
Germany301
225
Cesarean delivery per100 live births
NLD16
Sweden17
Japan18
Denmark21
France21
UK23
Canada26
Germany31
Australia32
CHE33
US33
25
Cataract surgery per 100 000population
JapanNA
CHE438
UK736
NLD1005
Germany1027
Sweden1029
Denmark1037
Australia1060
Canada1060
US1110
France1207
971
Coronary artery bypass graftsurgery
JapanNA
CHENA
UK26
France29
Sweden31
Australia54
Canada58
Germany64
NLD69
Denmark73
US79
54
Coronary angioplasty CHENA
UK128
Canada157
Australia172
Denmark190
Japan193
Sweden205
France237
NLD248
US248
France393
217
Surgical procedures
Normal delivery UK1.5
Canada1.6
NLD1.9
US2
Sweden2.3
Australia2.7
Denmark2.7
Germany2.9
CHE3.6
France4.1
Japan5.7
2.8
Length of stay per capita, mean, d
Cardiovascular procedures per 100 000 population
Acute myocardial infarction JapanNA
Denmark3.9
Sweden4.7
Australia5.4
US5.4
Canada5.5
NLD5.6
France6
UK7.1
CHE7.3
Germany10.3
6.1
NA indicates not applicable. CHE indicates Switzerland; NLD, the Netherlands. See eTable 4 in Supplement 2 for data ordered by country.
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1033
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

The data also suggest that some of the more common explana-tions about higher health care spending in the United States,such as underinvestment in social programs, the low primarycare/specialist mix, the fee-for-service system encouraging highvolumes of care, or defensive medicine leading to overutilization,did not appear to be major drivers of the substantially higher UShealth care spending compared with other high-income countries.Instead, the data suggest that the main driving factors werelikely related to prices, including prices of physician and hospitalservices, pharmaceuticals, and diagnostic tests, which likely alsoaffected access to care. In addition, administrative costs appearedmuch higher in the United States. These findings indicate thatefforts targeting utilization alone are unlikely to reduce the gap inspending between the United States and other high-income coun-tries, and a more concerted effort to reduce prices and administra-tive costs is likely needed.
Several findings in this report may be surprising to policy mak-ers. There is broad consensus among US policy makers that theUnited States spends too much on health services and too little onsocial services. This analysis showed that US social spending ap-pears to be similar to that in other high-income OECD countries. This
finding calls into question the belief that higher health care spend-ing is due to a lack of investment in social determinants. In particu-lar, given that the United States did not appear to be an outlier withregard to utilization of services, it is unlikely that a lack of social spend-ing results in higher health care spending due to a misallocation ofresources that results in greater need (and overutilization).
Another common perception among policy makers is that theUS system is often perceived to be disproportionately driven byspecialist care. However, the number of specialist practitioners inthe US system, both as an absolute number and a percentage, wasnot considerably different from comparison countries. One expla-nation may be differences in the way primary care services aredelivered in other countries. In many other countries, nurses andallied health professionals may make up a higher proportion of thehealth care workforce,21 although we did not find substantiallyhigher numbers of nurses in the other countries. The extent towhich this explains variation in numbers of physicians across sys-tems is unclear, but it is unlikely to fully account for why the UnitedStates is not an outlier.
Although the ratio of primary care physicians to specialists wassimilar between the United States and other high-income countries,
Figure 8. Performance on Key Measures of Utilization
0.5 1.0 1.5 2.00
No. of Hospital Bed Days per Inpatient
Japan
Germany
France
Switzerland
Sweden
Australia
United Kingdom
The Netherlands
United States
Denmark
Canada
Hospital bed daysC
2.5 2 4 6 8 10 12 14 160
Length of Stay per Inpatient, d
Japan
Germany
France
Switzerland
Sweden
Australia
United Kingdom
The Netherlands
United States
Denmark
Canada
All-cause length of stayD
18
15050 100 2502000
Hospital Discharges per 1000 Population
Japan
Germany
France
Switzerland
Sweden
Australia
United Kingdom
The Netherlands
United States
Denmark
Canada
Hospital dischargesA
300 102 4 6 8 120
Physician Visits per Capita in a Given Year
Japan
Germany
France
Switzerland
Sweden
Australia
United Kingdom
The Netherlands
United States
Denmark
Canada
ConsultationsaB
14
The vertical dashed lines indicate mean values.a Consultations is the mean number of consultations or visits with a physician per person per year in all care delivery settings.
Clinical Review & Education Special Communication Health Care Spending in the United States and Other High-Income Countries
1034 JAMA March 13, 2018 Volume 319, Number 10 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

the salaries paid to both generalist and specialist physicians weremarkedly higher in the United States, where specialists were paidtwice as much as those in the United Kingdom or Germany and pri-mary care physicians and nurses also had substantially higher sala-ries. However, it can be difficult to compare salaries of workers fromvarious countries. In general, salaries for professionals are higher inthe United States than in other countries, and in addition, workersin the United States bear higher costs in some areas, such as for healthcare insurance, higher education, or planning for retirement, thanworkers in other countries. Some of these issues are accounted forin the ratio of national average wage, but US physicians and nursesstill had the highest ratio.
Some of the differential observed in cost between physiciansand nurses in the United States and in the other countries may re-flect differences in productivity or the extent to which training costsare borne by the individual, although in either case it is unlikely toaccount for the magnitude of the difference. In 2011, Laugesen andGlied19 estimated that the investment repayment cost for private
education in the United States would amount to about $21 300 peryear for a primary care physician and about $24 400 for an ortho-pedic surgeon over a 35-year period.
Taking this investment into account, however, does not explainthe more than $200 000 difference in compensation observed forphysicians between countries. Although remuneration varies widelyacross systems, the optimal level of compensation remains unclear.Salaries in the United States may be high, but recent debates on re-muneration of medical staff in the United Kingdom and France, forexample, suggest that salaries in other countries may be too low.22
Other indicators, such as average wages for competitive nonhealthprofessions or retention of medical graduates, may help inform ap-propriate salaries of health care professionals in a given country.
Prices of services were not examined directly, but US healthcare spending was found to be higher than in other countriesdespite similar utilization patterns, suggesting that higher priceswere the primary cause of high health care spending in the UnitedStates relative to other nations. This is consistent with prior work
Figure 9. Pharmaceuticals
Rank (highest to lowest) 1 2 3 4 5 6 7 8 9 10 11 Mean
Retail pharmaceutical spendingper capita, US $
Denmark573
NLD292
Sweden501
UK383
Australia346
France541
CHE776
Germany480
Canada587
Japan443
US1026
541
Crestor (cholesterol)
Lantus (diabetes) DenmarkNA
CHENA
NLDNA
SwedenNA
France47
Australia54
Germany61
Japan64
UK64
Canada67
US186
78
Prices, US $ per moa
Advair (asthma) DenmarkNA
CHENA
NLDNA
SwedenNA
UKNA
Australia29
France35
Germany38
Japan51
Canada74
US155
64
Humira (rheumatoid arthritis) DenmarkNA
CHENA
NLDNA
SwedenNA
Japan980
France982
UK1158
Canada1164
Australia1243
Germany1749
US2505
1436
AustraliaNA
CanadaNA
DenmarkNA
NLDNA
SwedenNA
France11
Germany12
UK16
Japan18
CHE26
US111
NANew chemical entities, No.b
Public spending US34
Canada36
Denmark43
CHE43
Australia49
Sweden52
NLD65
UK66
Japan71
Germany75
France80
56
Private insurance
Private out-of-pocket spending Germany18
France19
Japan28
US30
NLD33
Canada34
UK36
Sweden48
Australia50
Denmark51
CHE51
36
Pharmaceutical expenditure by financing type, % of total spending
Australia0
Sweden0
UK0
Japan1
France1
NLD2
Germany7
Denmark8
CHE8
Canada30
US36
8
Volume NLD17
Australia30
Sweden44
Denmark54
CHE54
Japan56
Canada70
France70
Germany80
UK83
US84
58
Value
Share of generics, % of totalc
Denmark14
CHE14
Australia15
Sweden15
NLD16
France16
US28
Canada29
Japan33
UK33
Germany37
23
JapanNA
NLD10.7
Sweden12.9
Germany14.4
Denmark16.6
UK20.1
US24
Canada25
Australia28.3
France29.9
CHENA
20.2Antibiotic prescribing, defineddaily doses per 1000 populationd
DenmarkNA
CHENA
NLDNA
SwedenNA
Australia9
France20
UK26
Japan29
Canada32
Germany41
US86
35
NLD466
Total spending per capita, US $ Denmark675
CHE939
Sweden566
Australia560
France697
UK779
Japan837
Canada613
Germany667
US1443
749
NA indicates not applicable. CHE indicates Switzerland; NLD, the Netherlands.See eTable 5 in Supplement 2 for data ordered by country.a US discounted prices are listed; nondiscounted prices are $216.00 for Crestor,
$372.75 for long-acting insulin, $309.60 for Advair, and $3430.82 for Humira.b A new chemical entity is a compound without any precedent among the
regulated and approved drug products.c Volume is most often the proportion of total prescriptions that were for
generic brands. Volumes can be expressed in defined daily doses or as anumber of packages/boxes or standard units. Value is most often the
proportion of total cost (ie, government and patient expenditure) that was forgeneric brands. Values can be, for instance, the turnover of pharmaceuticalcompanies, the amount paid for pharmaceuticals by third-party payers, or theamount paid by all payers (third-party and consumers). Market value is mostoften at ex-factory prices, while amounts paid by third-party payers andconsumers are in general at retail prices.
d Defined daily dose is the assumed mean maintenance dose per day for a drugused for its main indication in adults. Data shown here are actual mean defineddaily doses for each country.
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1035
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

by Anderson et al,23 which also illustrated higher health carespending in the United States despite similar inputs and levels ofcare utilization, and more recent work by Dieleman et al.13 In addi-tion to differential prices for physician services and pharmaceuti-cals, these results suggest that prices for nonphysician services andprocedures also appeared to be markedly higher in the UnitedStates. For the select procedures for which comparable data wereavailable, the United States paid considerably more than its coun-terparts. In 2013, the International Federation of Health Plans24
reported that the average cost in the United States was $75 345for a coronary artery bypass graft surgery, whereas the costsin the Netherlands and Switzerland were $15 742 and $36 509,respectively. Computed tomography was also much higher in the
United States, with an average payment of $896 per scan com-pared with $97 in Canada, $279 in the Netherlands, $432 in Swit-zerland, and $500 in Australia in 2013. Similarly, the mean paymentfor an MRI in the United States was $1145 compared with $350 inAustralia and $461 in the Netherlands.
Of particular interest to US health policy makers is the role ofthe pharmaceutical market and its influence on health care spend-ing. Not surprisingly, US spending on pharmaceuticals was almostdouble the spending in comparison countries. Previous work sug-gests that this is driven by high prices for brand-name drugs ratherthan by utilization, which is comparable with other high-incomecountries.24-27 Across comparison countries, the United States hadthe highest volume of generics, accounting for more than 80% of
Figure 10. Access and Quality
Access, %
Able to get same- or next-day appointmenta
Rank (highest to lowest) 1 2 3 4 5 6 7 8 9 10 11
JapanNA
DenmarkNA
CHENA
Canada43
Sweden49
US51
Germany53
France56
UK57
Australia67
NLD77
57
Mean
2-mo Wait time to see specialist JapanNA
DenmarkNA
Germany3
France4
US6
NLD7
CHE9
Australia13
Sweden19
UK19
Canada39
13
Adequate time with regular(primary) physician
JapanNA
DenmarkNA
FranceNA
Sweden78
Canada79
US81
Australia83
CHE84
NLD85
UK86
Germany88
83
System works well JapanNA
DenmarkNA
NLDNA
US19
Canada35
Australia44
Sweden44
UK44
France54
CHE58
Germany60
45
Fundamental changes needed JapanNA
DenmarkNA
NLDNA
CHE37
Germany37
France41
Australia46
Sweden46
UK46
US53
Canada55
45
Measles immunization, %of children
Canada90
Denmark91
France91
US92
Australia93
CHE93
UK93
NLD96
Germany97
Japan98
Sweden98
94
Breast cancer screening, %of women aged 50-69 yb
Japan41
CHE47
France52
Australia55
Germany71
Canada72
Sweden75
UK76
NLD79
US81
Denmark84
67
Complete rebuild of healthsystem needed
JapanNA
DenmarkNA
NLDNA
CHE3
Germany3
Australia4
France4
UK7
Canada9
Sweden10
US23
8
Clinical outcomes
30-d Stroke mortality per1000 patientsc
JapanNA
DenmarkNA
NLDNA
US4.2
Germany6.4
CHE6.9
France7.9
UK9.2
Australia9.3
Sweden9.6
Canada10
7.9
30-d Mortality per 1000 patientswith acute myocardial infarction
JapanNA
DenmarkNA
NLDNA
Australia4.1
US5.5
Canada6.7
France7.2
UK7.6
CHE7.7
Sweden8.3
Germany8.7
7
Foreign body left per100 000 discharges
JapanNA
DenmarkNA
NLDNA
US4.1
Sweden4.6
Germany5.5
UK6.1
France6.2
Australia8.6
Canada8.6
CHE12.3
7
Obstetric trauma withoutinstrument per 100 deliveries
JapanNA
France0.6
US1.5
Germany2.1
Australia2.4
NLD2.5
Denmark2.6
CHE2.6
Sweden2.8
UK2.8
Canada3.1
2.3
Diabetes hospitalizations per100 000 populationd
NLD69.8
CHE72.6
UK72.8
Canada93.7
Sweden96
Denmark113.4
Australia141.1
France150.6
Japan162.3
US191
Germany218.3
125.6
Diabetes hospitalizations as aratio of population with diabetese
CHE1.20
NLD1.20
France1.20
Canada1.30
UK1.70
Denmark1.80
Sweden1.90
US2
Germany2.40
Australia2.80
Japan2.80
2.00
Asthma hospitalizations as aratio of population with asthmag
Canada0.20
Japan0.30
Sweden0.30
CHE0.40
Australia0.60
NLD0.70
Germany0.70
Denmark0.80
UK1.00
US1.20
0.70
Asthma hospitalizations per100 000 populationf
Canada14.6
Sweden19
CHE27.5
Germany28.7
France29.6
Japan34.7
NLD36
Denmark50.6
Australia64.8
France0.80
UK71
US89.7
42.4
Avoidable hospitalizations
Prevention
Perceptions, %
NA indicates not applicable. CHE indicates Switzerland; NLD, the Netherlands.See eTable 6 in Supplement 2 for data ordered by country.a Able to get same- or next-day appointment when sick, excluding those who
did not need to see a physician or nurse.b Women aged 40 to 49 years in Sweden.c Thirty-day stroke mortality after hospital admission for ischemic stroke.
d Limited to a primary diagnosis of diabetes.e Diabetes hospitalizations are limited to persons aged 15 years or older, whereas
the denominator (population with diabetes) is both adult and pediatric.f Limited to a primary diagnosis of asthma.g Asthma hospitalizations are limited to persons aged 15 years or older, whereas
the denominator (population with asthma) is both adult and pediatric.
Clinical Review & Education Special Communication Health Care Spending in the United States and Other High-Income Countries
1036 JAMA March 13, 2018 Volume 319, Number 10 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

total pharmaceuticals used by US residents yet just under 30% ofthe United States’ total spending on pharmaceuticals. Australia andFrance had much smaller generic market penetration rates, presum-ably because brand-name drugs are comparatively affordable.25
Although the United States’ high prices of pharmaceuticals arecontroversial, these prices have been viewed as critical to innova-tion, including US production of new chemical entities.18,28 Whetherinnovation justifies high levels of spending is not clear.
Performance on access is also a central concern to policy mak-ers. These data indicated that the United States had the lowest rateof insurance coverage. However, the percentage of the populationwith health insurance is at a historical high and has continued to in-crease since the passage of the Affordable Care Act. Out-of-pocketspending was also surprisingly low in the United States, which maybe explained in part by the relatively high proportion of patients whodo not seek care or who skip consultations because of high costs.Prior work has shown that out-of-pocket spending is more concen-trated among the poor.29 Other factors influencing access to carein the United States aside from affordability likely include the coun-try’s considerable landmass (and correspondingly large rural popu-lation). Personal choice is an additional albeit contentious factor. Forexample, the Kaiser Family Foundation has found that approxi-mately 20% of uninsured US residents have incomes of 400% ormore of the federal poverty level and have largely chosen to forgo
insurance.30 In the other countries in this study with similar healthinsurance designs (the Netherlands and Switzerland), the propor-tion of the population choosing to forego coverage is considerablyless.31,32 Still, a substantial proportion of people would benefit fromcoverage but remain uninsured in the United States, and increas-ing coverage for these individuals remains a policy priority.
A central concern in the United States is the extent to whichgreater health care spending translates to better outcomes. Com-paring intermediate country-level health care outcomes across arange of health care services showed that the United States doesperform favorably on certain acute care outcomes but less so forprimary care measures. Notably, the United States had among thehighest breast cancer screening rates and the lowest 30-day mor-tality rates for acute myocardial infarction and stroke. Although therates of avoidable hospitalizations in the United States, such as fordiabetes and asthma, are well above those of most of the countriesin the analysis, accounting for the United States’ higher prevalenceof both diseases reduced this gap considerably. The United Stateshas relatively poor population health outcomes, which likely repre-sents a combination of factors including issues with the affordabil-ity of care. However, the United States average, in comparisonto averages of much smaller, more homogeneous countries, maylead to erroneous conclusions. For example, the life expectancy ofMinnesota, a state comparable in size and demographics to
Figure 11. Distribution and Equity
Out-of-pocket spending
Rank (highest to lowest) 1 2 3 4 5 6 7 8 9 10 11 Mean
As % of total health expenditure NLD5.2
France6.3
UK9.7
US11
Germany13.2
Denmark13.4
Canada13.6
Japan13.9
Sweden14.1
Australia18.8
CHE26.8
13.3
As % of household consumption
Equity
Horizontal inequity index, %a AustraliaNA
JapanNA
DenmarkNA
CHENA
NLDNA
SwedenNA
UK0.40
Germany1.00
France1.30
Canada1.90
US6
2.10
NLD1.3
France1.4
UK1.4
Germany1.8
Japan2.2
Canada2.3
Denmark2.6
US2.6
Australia3.2
Sweden3.4
CHE4.5
2.4
Consultation skippedbecause of cost
JapanNA
DenmarkNA
Germany2.6
Sweden3.9
UK4.2
Canada6.6
CHE7
France9
NLD12.5
Australia16.2
US22.3
9.4
% Unmet need, below-averageincome
% Unmet need, above-averageincome
JapanNA
DenmarkNA
Germany6
Sweden7
UK7
Australia13
Canada13
France14
NLD16
CHE22
US32
14.4
Unmet needb
JapanNA
DenmarkNA
UK8
Sweden16
Germany16
Australia24
NLD29
Canada30
France30
CHE31
US43
25.2
Rural population, % oftotal population
Japan6
NLD9
Australia10
Denmark12
Sweden14
UK17
Canada18
Germany18
US18
France20
CHE26
15
Population density per sq mile
Geographic breakdown
Australia3
Canada4
Sweden24
US35
France122
Denmark136
CHE212
Germany237
UK271
Japan348
NLD505
173
Urban physicians per1000 population
DenmarkNA
NLDNA
UKNA
Germany2
Australia2.6
CHE2.8
Japan2.9
US3.2
Canada4.1
France4.1
Sweden4.5
3.3
2.1Rural physicians per1000 population
DenmarkNA
NLDNA
UKNA
Canada0.4
Germany1.3
Japan1.4
US1.4
Australia1.7
France2.5
Sweden3.5
CHE4.4
NA indicates not applicable. CHE indicates Switzerland; NLD, the Netherlands.See eTable 7 in Supplement 2 for data ordered by country.a The horizontal inequity index is the percentage probability of a physician visit
in the past 12 months by wealth. If the index is greater than 0, thenhigh-income groups access physicians more than low-income groups afteradjustment for relative need.
b Regarding unmet need, the Commonwealth Fund International Health Policy
Survey poses a number of questions to a representative sample from eachcountry. For this indicator, it was analyzed whether a respondent did notconsult with or visit a physician because of cost, skipped a medical test,treatment, or follow-up that was recommended by a physician because ofcost, or did not fill or collect a prescription for medicine or skipped dosesof medicine because of cost. Low income is defined as household incomeless than 50% of the country median.
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1037
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018

Sweden or Denmark, has more similar population health outcomesto these countries than Minnesota has in comparison to Mississippi.
This analysis extends to a body of work that has explored UShealth care spending33 by revisiting comparisons following the pas-sage of the Affordable Care Act, which has both increased cover-age and spurred health care delivery reform toward the delivery ofhigh-value care.9,13 Similar to previous work by Garber and Skinner,10
Reinhardt et al,12 and Anderson et al23 that examined US health carespending relative to other OECD countries, we found that the UnitedStates spent significantly more on health care despite having simi-lar levels of utilization. However, from 2010 onward it appeared thatthe United States had similar levels of public social spending com-pared with other high-income countries. While public social spend-ing has increased since 2010 (from 15.6% of GDP in 2005 to 19.3%of GDP in 2010), utilization rates have remained relativelyunchanged.20,23 This finding suggests that differences in socialspending are less likely to be the main driver of differences in healthcare spending than previous works have suggested.34 This is a simi-lar conclusion to recent work by Dieleman et al,13 which identifiedprices and intensity of care to be largely related to increases in healthcare spending over the past 15 years and negatively associated withdisease prevalence or incidence.
This study has several limitations. First, there was limited avail-ability of comparable data across health systems, which restrictedthe areas of health system performance we were able to compare.In particular, data on prices across systems were lacking, as was thenumber of indicators on quality and coverage. The indicators se-lected thus provide a snapshot of performance in some domains—particularly quality—which may not be representative of quality ofthe entire system or may be limited due to data availability acrossall countries. For instance, 30-day mortality rates reflect only in-hospital rates, which may influence the apparent variations ob-served, particularly given differences in length of stay and dis-charge practices across countries. Second, because of the difficultiesin collecting and standardizing indicators across countries, some of
the data used reflect different years, may be out of date, or may havebeen measured differently based on country-specific definitions ofvariables. Even when data were collected from the same source, is-sues of comparability remain because of fundamental differencesin how systems are organized and, in turn, how care is categorized.Two areas of particular concern are outpatient spending and the pri-mary care workforce. We attempted to address limitations in theworkforce data by utilizing a functionality-based approach to iden-tifying who provides primary care services in each country and bycross-referencing resulting numbers with country experts. Third, thestudy was able to present only descriptive comparative findings, andit is not possible to make any causal inferences. Fourth, the data didnot adjust for factors such as underlying population differences orsystem delivery and organizational factors, which likely influencesome of the observed variation in this space. Fifth, the response rateto some surveys that were the basis for some measures, such as abil-ity to get same- or next-day appointment and 2-month wait time tosee a specialist physician, were not good across all countries. Sixth,we did not consider the actual prices of devices, which, given theincreasing number of hip and knee replacements and use of otherdevices, are emerging as an important consideration in the cost ofcare in the United States.
ConclusionsThe United States spent approximately twice as much as otherhigh-income countries on medical care, yet utilization rates in theUnited States were largely similar to those in other nations. Pricesof labor and goods, including pharmaceuticals, and administrativecosts appeared to be the major drivers of the difference in overallcost between the United States and other high-income countries.As patients, physicians, policy makers, and legislators activelydebate the future of the US health system, data such as these areneeded to inform policy decisions.
ARTICLE INFORMATION
Accepted for Publication: February 2, 2018.
Author Contributions: Dr Papanicolas and MsWoskie had full access to all of the data in the studyand take responsibility for the integrity of the dataand the accuracy of the data analysis.Concept and design: All authors.Acquisition, analysis, or interpretation of data: Allauthors.Drafting of the manuscript: Papanicolas, Woskie.Critical revision of the manuscript for importantintellectual content: All authors.Statistical analysis: Woskie.Administrative, technical, or material support: Allauthors.Supervision: Papanicolas, Jha.
Conflict of Interest Disclosures: All authors havecompleted and submitted the ICMJE Form forDisclosure of Potential Conflicts of Interest andnone were reported.
Additional Contributions: We thank DuncanOrlander, BA, Harvard School of Public HealthDepartment of Health Policy and Management,for research assistance (compensated as partof regular pay).
REFERENCES
1. World Health Organization. Global HealthExpenditure Database. http://apps.who.int/nha/database/Country_Profile/Index/en. AccessedSeptember 22, 2017.
2. Health at a Glance 2017. Paris, France: OECDPublishing; 2017. doi:10.1787/health_glance-2017-en.
3. Sorensen N, Reed JD, Bollyky T, et al; GBD 2015Healthcare Access and Quality Collaborators.Healthcare Access and Quality Index based onmortality from causes amenable to personal healthcare in 195 countries and territories, 1990-2015:a novel analysis from the Global Burden of DiseaseStudy 2015. Lancet. 2017;390(10091):231-266.
4. Schneider EC, Sarnak DO, Squires D, Shah A,Doty MM. Mirror, Mirror 2017: InternationalComparison Reflects Flaws and Opportunitiesfor Better US Health Care. July 2017.http://www.commonwealthfund.org/~/media/files/publications/fund-report/2017/jul/schneider_mirror_mirror_2017.pdf. AccessedSeptember 22, 2017.
5. World Health Organization. The World HealthReport 2000: Health Systems, Improving
Performance. 2000. http://www.who.int/entity/whr/2000/en/whr00_en.pdf?ua=1. AccessedJanuary 17, 2018.
6. Obama B. United States health care reform:progress to date and next steps. JAMA. 2016;316(5):525-532.
7. Schroeder SA, Frist W; National Commissionon Physician Payment Reform. Phasing outfee-for-service payment. N Engl J Med. 2013;368(21):2029-2032.
8. For the Public’s Health: Investing in a HealthierFuture: Health and Medicine Division. April 10, 2012.http://www.nationalacademies.org/hmd/Reports/2012/For-the-Publics-Health-Investing-in-a-Healthier-Future.aspx. Accessed January 17, 2018.
9. Berwick DM, Hackbarth AD. Eliminating wastein US health care. JAMA. 2012;307(14):1513-1516.
10. Garber AM, Skinner J. Is American health careuniquely inefficient? J Econ Perspect. 2008;22(4):27-50.
11. Bradley EH, Elkins BR, Herrin J, Elbel B. Healthand social services expenditures: associations withhealth outcomes. BMJ Qual Saf. 2011;20(10):826-831.
Clinical Review & Education Special Communication Health Care Spending in the United States and Other High-Income Countries
1038 JAMA March 13, 2018 Volume 319, Number 10 (Reprinted) jama.com
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018
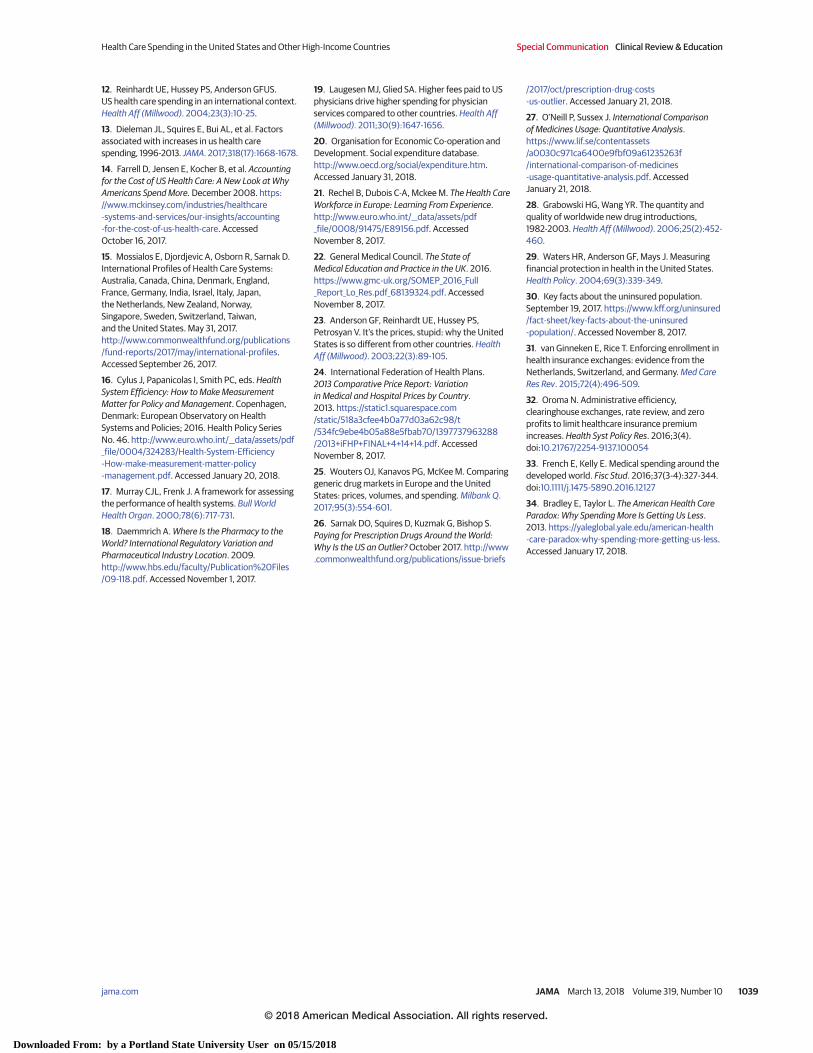
12. Reinhardt UE, Hussey PS, Anderson GFUS.US health care spending in an international context.Health Aff (Millwood). 2004;23(3):10-25.
13. Dieleman JL, Squires E, Bui AL, et al. Factorsassociated with increases in us health carespending, 1996-2013. JAMA. 2017;318(17):1668-1678.
14. Farrell D, Jensen E, Kocher B, et al. Accountingfor the Cost of US Health Care: A New Look at WhyAmericans Spend More. December 2008. https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/accounting-for-the-cost-of-us-health-care. AccessedOctober 16, 2017.
15. Mossialos E, Djordjevic A, Osborn R, Sarnak D.International Profiles of Health Care Systems:Australia, Canada, China, Denmark, England,France, Germany, India, Israel, Italy, Japan,the Netherlands, New Zealand, Norway,Singapore, Sweden, Switzerland, Taiwan,and the United States. May 31, 2017.http://www.commonwealthfund.org/publications/fund-reports/2017/may/international-profiles.Accessed September 26, 2017.
16. Cylus J, Papanicolas I, Smith PC, eds. HealthSystem Efficiency: How to Make MeasurementMatter for Policy and Management. Copenhagen,Denmark: European Observatory on HealthSystems and Policies; 2016. Health Policy SeriesNo. 46. http://www.euro.who.int/__data/assets/pdf_file/0004/324283/Health-System-Efficiency-How-make-measurement-matter-policy-management.pdf. Accessed January 20, 2018.
17. Murray CJL, Frenk J. A framework for assessingthe performance of health systems. Bull WorldHealth Organ. 2000;78(6):717-731.
18. Daemmrich A. Where Is the Pharmacy to theWorld? International Regulatory Variation andPharmaceutical Industry Location. 2009.http://www.hbs.edu/faculty/Publication%20Files/09-118.pdf. Accessed November 1, 2017.
19. Laugesen MJ, Glied SA. Higher fees paid to USphysicians drive higher spending for physicianservices compared to other countries. Health Aff(Millwood). 2011;30(9):1647-1656.
20. Organisation for Economic Co-operation andDevelopment. Social expenditure database.http://www.oecd.org/social/expenditure.htm.Accessed January 31, 2018.
21. Rechel B, Dubois C-A, Mckee M. The Health CareWorkforce in Europe: Learning From Experience.http://www.euro.who.int/__data/assets/pdf_file/0008/91475/E89156.pdf. AccessedNovember 8, 2017.
22. General Medical Council. The State ofMedical Education and Practice in the UK. 2016.https://www.gmc-uk.org/SOMEP_2016_Full_Report_Lo_Res.pdf_68139324.pdf. AccessedNovember 8, 2017.
23. Anderson GF, Reinhardt UE, Hussey PS,Petrosyan V. It’s the prices, stupid: why the UnitedStates is so different from other countries. HealthAff (Millwood). 2003;22(3):89-105.
24. International Federation of Health Plans.2013 Comparative Price Report: Variationin Medical and Hospital Prices by Country.2013. https://static1.squarespace.com/static/518a3cfee4b0a77d03a62c98/t/534fc9ebe4b05a88e5fbab70/1397737963288/2013+iFHP+FINAL+4+14+14.pdf. AccessedNovember 8, 2017.
25. Wouters OJ, Kanavos PG, McKee M. Comparinggeneric drug markets in Europe and the UnitedStates: prices, volumes, and spending. Milbank Q.2017;95(3):554-601.
26. Sarnak DO, Squires D, Kuzmak G, Bishop S.Paying for Prescription Drugs Around the World:Why Is the US an Outlier? October 2017. http://www.commonwealthfund.org/publications/issue-briefs
/2017/oct/prescription-drug-costs-us-outlier. Accessed January 21, 2018.
27. O’Neill P, Sussex J. International Comparisonof Medicines Usage: Quantitative Analysis.https://www.lif.se/contentassets/a0030c971ca6400e9fbf09a61235263f/international-comparison-of-medicines-usage-quantitative-analysis.pdf. AccessedJanuary 21, 2018.
28. Grabowski HG, Wang YR. The quantity andquality of worldwide new drug introductions,1982-2003. Health Aff (Millwood). 2006;25(2):452-460.
29. Waters HR, Anderson GF, Mays J. Measuringfinancial protection in health in the United States.Health Policy. 2004;69(3):339-349.
30. Key facts about the uninsured population.September 19, 2017. https://www.kff.org/uninsured/fact-sheet/key-facts-about-the-uninsured-population/. Accessed November 8, 2017.
31. van Ginneken E, Rice T. Enforcing enrollment inhealth insurance exchanges: evidence from theNetherlands, Switzerland, and Germany. Med CareRes Rev. 2015;72(4):496-509.
32. Oroma N. Administrative efficiency,clearinghouse exchanges, rate review, and zeroprofits to limit healthcare insurance premiumincreases. Health Syst Policy Res. 2016;3(4).doi:10.21767/2254-9137.100054
33. French E, Kelly E. Medical spending around thedeveloped world. Fisc Stud. 2016;37(3-4):327-344.doi:10.1111/j.1475-5890.2016.12127
34. Bradley E, Taylor L. The American Health CareParadox: Why Spending More Is Getting Us Less.2013. https://yaleglobal.yale.edu/american-health-care-paradox-why-spending-more-getting-us-less.Accessed January 17, 2018.
Health Care Spending in the United States and Other High-Income Countries Special Communication Clinical Review & Education
jama.com (Reprinted) JAMA March 13, 2018 Volume 319, Number 10 1039
© 2018 American Medical Association. All rights reserved.
Downloaded From: by a Portland State University User on 05/15/2018







