ADVANCED PALLIATIVE CARECASE PRESENTATION
Prepared by: Amani AbdullahSupervised by: Dr. Ruqayya Al Zeilani
CHIEF COMPLAIN
Mr. Kh.O is a 77-year-old male patient, a case of metastatic colorectal carcinoma, Mets to liver, lymph nodes and peritoneum
on 10/10/2013 admitted via ER due to increasing abdominal pain (NRS=8/10), vomiting and constipation of two days duration prior to admission.
BIOGRAPHIC DATA
Name of patient: Mr. Kh.O Age: 77 years old Gender: male Place of birth: Palestine Address: Al- Zarqa District Religion: Muslim Nationality: Jordanian Civil status: Married Occupation: A Carpenter. Educational attainment: Intermediate Level
2011 started to complain of severe abdominal pain,7days of constipation associated with nausea and vomiting.
Attended the general hospital emergency department; but had difficulty to get early appointment to follow up with his investigations CT scan and colonoscopy was postponed many times
PATIENT’S STORY
PATIENT’S STORY
Mr. Kh.O underwent a surgical procedure of
colectomy and colostomy on may/2013
Had used the medication “Irinotecan" on 1st/
Sept/2013 which is a drug used for the treatment
of cancer.
His complain at that time was relieved by using enema and laxatives
Continued to have on/off constipation On Oct / 2012 diagnosed as a colorectal
carcinoma of stage 2
On may/2013 confirmed diagnosis of CRC with METs to liver, lymph nodes and peritoneum
PATIENT’S STORY
PATIENT’S HX
Past Medical and Family Hx: No history of hypertension or diabetes mellitus.
Past Surgical Hx: only the surgical intervention for the resection of the carcinoma in addition to chemotherapy.
Patient was informed by his oncologist that further chemotherapy was unlikely to be effective
Mr. Kh.O is Married with two wives Has one son Had his own shop watched by his nephew but
with low income Mr. Kh.O is an ex-smoker, quit age (40), used
to smoke two packets per/day. Insured Own a house His 2nd wife is the one taking care about him
and the for their child who is cp and blind and caring for the other wife as she is an aged one.
SOCIAL HX:

ASSESSMENT
Lifestyle: Personal habits: Early in the morning, drinks
a cup of coffee and three cigarettes
Diet: before hospitalization: Mr. Kh.O claimed that
he eats one meal a day. He loves to eat meat and salty food. He drinks very little amount of water per day and only after meals then follow it with three pieces of cigarettes.
During hospitalization: Has difficulty in having food related to his
obstructed bowels although no limitations needed
Has poor appetite yet likes to have a piece of (kaak) and a cup of tea with meramia
Sleep and rest Pattern:Before hospitalization The patient normally sleeps at 9:00 pm but
often a hard time to get a good sleep, he usually wakes up at 6:00 am and starts his work cycle
During hospitalization: The patient stated that he usually sleeps at
10:00 pm and wakes up around 6:00 “due to sleeping pills” as he stated. (Xanax)
Elimination Pattern:
Before Hospitalization: Mr. Kh.O voids yellow colored urine 6 times a day,
he also claimed that he had not experienced any difficulties in urination he also claimed that he used to defecate once every 3-5 days with brown, formed or semi-solid stool and used to have laxatives
During hospitalization: Mr. Kh.O urinates using condom catheter, with
yellow colored urine, total output in 24 hrs = 3000cc.
Can’t defecate as of his total bowel obstruction, a phosphate enema trials done but failed to help and was of no use..

Activities of daily living:Before hospitalization: The patient had no difficulties in performing
the basic activities such as grooming, dressing and toileting.
During hospitalization: The patient can perform few of the basic
activities specifically grooming, dressing and toileting and needed the assistance of his wife.
PSYCHOSOCIAL ASSESSMENT
Social Data:Family Relationship/Friendship Assessment: Mr. Kh.O lives at his own house with his two
wives and his sick son at the same building
His second wife is the only one to care for his family and extremely exhausted for they don’t have money to afford a servant
Mr. Kh.O stated “ I thank my wife because she is taking care of me day and night and she never leaves me, although she get’s tired all the time and she never sleeps well because of the noisy hospital environment but she never complained”.
Occupational Hx: Mr. Kh.O was a carpenter at his own place and after being sick he delegated his nephew for taking care of his shop
Socioeconomic status: securely covered by the health insurance
He stated that his major stressor aside from his condition is the issue of leaving his family alone with no support even the house he owns has a court case and the only son he has is already sick.
He always pray every day and asks for guidance from Allah. He has the ability to verbalize appropriate emotions and uses non verbal communications such as eye movements, gestures and interacts clearly during an interview.
Mr. Kh.O is very attached to his family presence during his disease, he expressed that they were the only supporter for him during his treatments..
SPIRITUAL ASSESSMENT
“ I feel guilty about one thing in my life, that I was putting myself last on everything, I should have taken care of myself much better than that” he stated. Patient looked really sad and he also added “am not afraid of death”.
“Its just that I will miss my family, but that’s what Allah wants, Thank Allah for everything”.

SPIRITUAL ASSESSMENT
He prays 5 times a day although sometimes it seems very hard for him to move, he prays while he’s sitting on her bed because he can’t stand for praying and that makes him feel sad because he used to perform it well when he was healthy but now all he could do is doing” the minimal things” as he expressed.
He reads Qur’an whenever he’s able to; also he stated that he likes the spiritual advisor to visit him frequently and pray for him as that comforts him a lot as he said, because he can ventilate what he feels to him and makes him think that he is getting closer to Allah.
PHYSICAL EXAMINATION
General Survey: Assessed/received patient lying on bed
comfortably, awake, conscious, responsive, and coherent with ongoing IVF NS 0.9 at 60 ml/hr with the following VS
Temperature: 37.3 C Heart Rate: 90 bpm Respiratory Rate: 18 rpm Blood Pressure 100/70 mmHg Oxygen Saturation: 95% (room air)
Skin, Hair and Nails Presence of bruises noted on the upper limbs
at site of (clexane) injections, no pallor is noted, cool and clammy to touch, fair skin turgor in both upper and lower extremities.
Bed sore at the sacral region stage2 pen skin Hair is white and not evenly distributed. Nails are trimmed convex shaped, smooth in
texture, intact epidermal lining around the nails, capillary refill test less than 3 seconds.

Skull and Face Rounded (normocephalic and symmetrical with
frontal parietal and occipital prominences), no nodules or masses upon palpation.
Eyes and vision: Eyelids are intact, sclera appears white, pale
conjunctiva and no discharges.
Ears and Hearing Ears are symmetrical in size, able to hear.
Nose and Sinuses Symmetric, has a good sense of smelling (can
smell orange fruit) no tenderness or pain noted.
Oropharynx (Mouth and Throat) Dry and cracked tongue and lips, able to
move freely has difficulty to swallow foods, needs good oral hygiene.
Neck Lymph nodes are noted and palpable at RT
side of the neck. Cardiovascular, Peripheral Systems and
Respiratory System No abnormalities found or observed.

Breast and Axillae With Rt lymph nodes enlarged.
Abdomen Presence of colostomy intact ,no infection
bruises, distended abdomen no audible bowel sound upon auscultation, had X-ray with fluid collection into abdominal cavity, had a trial of enemas for supportive measures no effect.
Musculoskeletal Unable to stand straight, difficulty to stand
can’t walk alone.

Neurologic Patient is oriented to time, person and place.
He was able to state where he lives. Patient was able to answer well when asked
of his complete name, birth and age, GCS = 15/15.
Reproductive System: Not done.
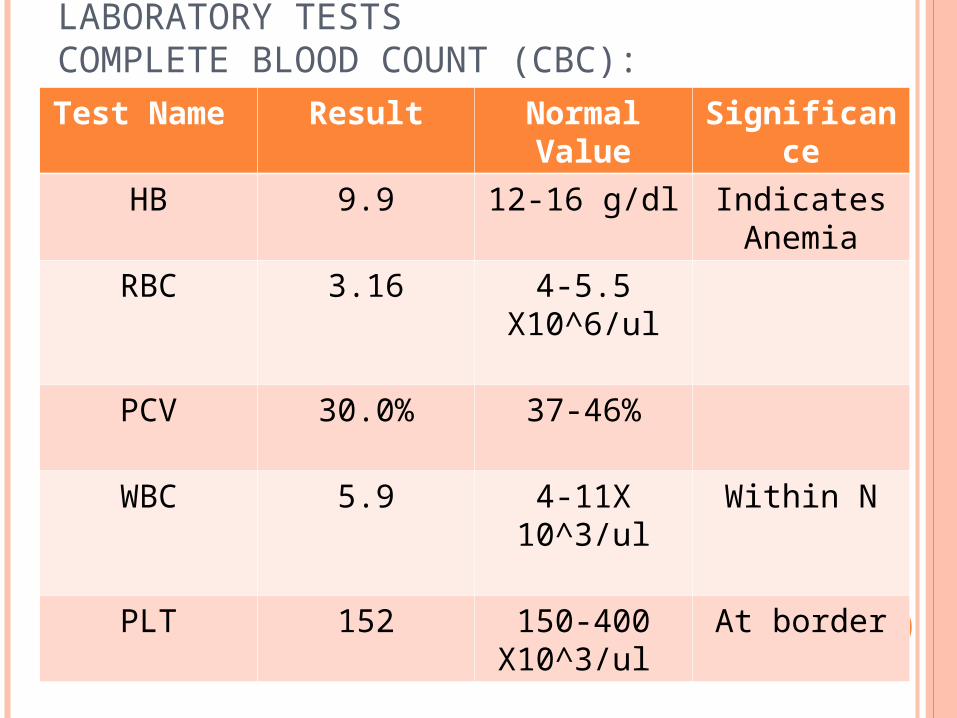
LABORATORY TESTS COMPLETE BLOOD COUNT (CBC):Test Name Result Normal
ValueSignificanc
e
HB 9.9 12-16 g/dl Indicates Anemia
RBC 3.16 4-5.5 X10^6/ul
PCV 30.0% 37-46%
WBC 5.9 4-11X 10^3/ul
Within N
PLT 152 150-400 X10^3/ul
At border
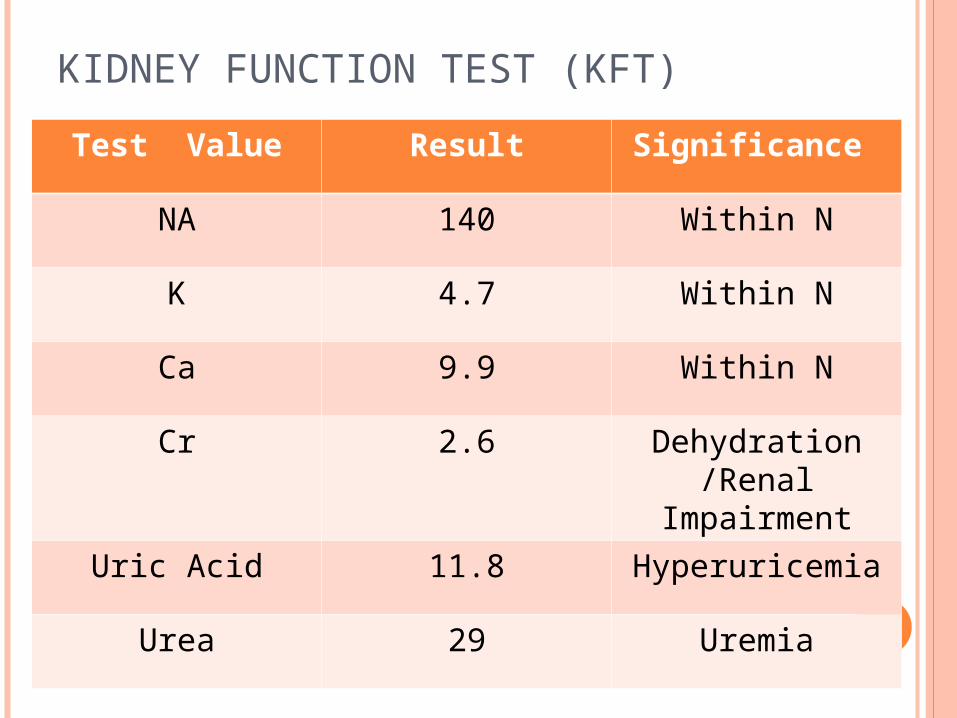
KIDNEY FUNCTION TEST (KFT)
Test Value Result Significance
NA 140 Within N
K 4.7 Within N
Ca 9.9 Within N
Cr 2.6 Dehydration /Renal
Impairment
Uric Acid 11.8 Hyperuricemia
Urea 29 Uremia
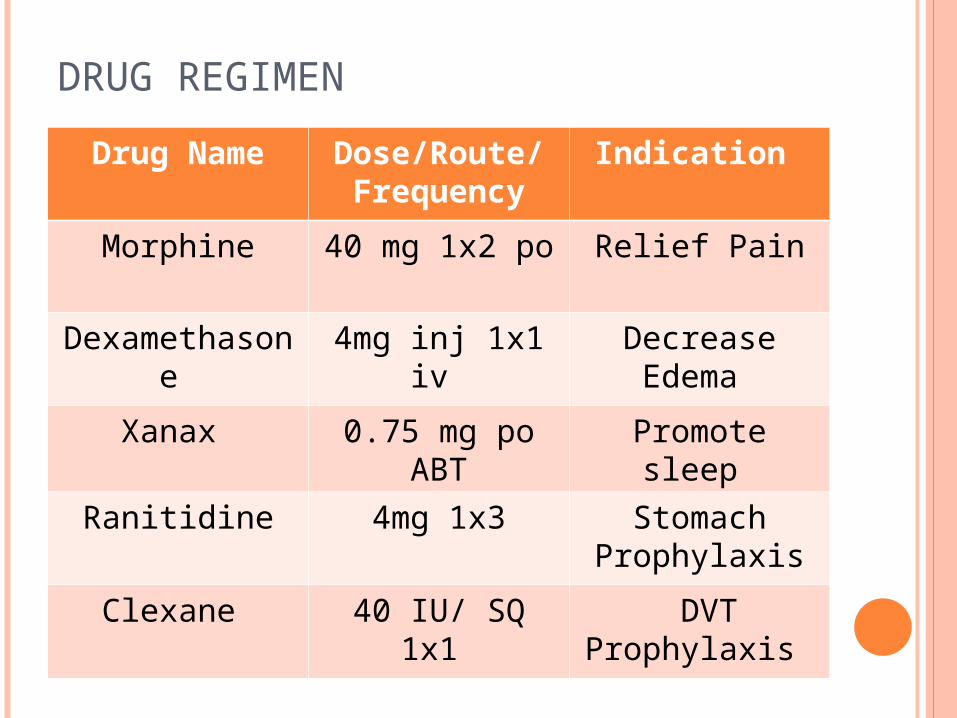
DRUG REGIMEN
Drug Name Dose/Route/Frequency
Indication
Morphine 40 mg 1x2 po Relief Pain
Dexamethasone
4mg inj 1x1 iv Decrease Edema
Xanax 0.75 mg po ABT
Promote sleep
Ranitidine 4mg 1x3 Stomach Prophylaxis
Clexane 40 IU/ SQ 1x1 DVT Prophylaxis
NURSING CARE PLAN PHYSICAL DIMENSION
Nursing DiagnosisPain related to total bowel obstruction secondary to
metastatic liver, lymphnodes and peritoneum evidenced by patient verbalization by NRS (8/10) , facial grimace and restlessness.
Goal Within 35 mints of giving appropriate nursing
interventions, patient will be able to verbalize reduction of pain from 8/10 to (1-3)/10
Nursing interventionsProvided non-pharmacologic comfort measures and
diversional activities.Evaluate pain relief/ control at regular intervals. Adjust
medication regimen as necessary. Noted and investigated changes from previous reports. Provided comfort measures and quiet environment Instructed and encouraged used of relaxation technique such
as focus breathing. Administered analgesic as indicated by the physician Evaluation After 35 mints of giving appropriate nursing interventions and
pain medications goal partially met, Patient verbalized reduction of pain from 8/10 to 4/10

Nursing interventionsFluid volume deficient related to decreased oral intake
evidenced by physical examination (dry skin) v/s and laboratory tests ( CBC + KFT ).
GoalWithin 3 days of giving appropriate nursing interventions, patient
will be able to maintain fluid volume at a functional level .
Nursing interventionsEstablished rapport to the patient. Assessed V/S Encouraged fluid intake to 3000 ml a day, unless contraindicated. Evaluated CFAC (Color, Frequency, Amount, and Consistency) of
urine.Regulated IVF level (NS 0.9%) accurately EvaluationAfter 3 days of giving appropriate nursing interventions, goal
partially met Patient was able to slightly maintained fluid volume balance

Nursing interventions Constipation related to total bowel obstruction evidenced by
Distended abdomen even with colostomy. GoalWithin 6 hrs. of giving appropriate nursing interventions, patient
will be partially relieved of fullness. Nursing interventionsIdentified areas of stressPalpated abdomen and noting bowel sounds .Provided adequate fluid intake as toleratedAdmisnter laxatives and stool softeners as physician ordered. If
not possible encourage activity and exercise within limits of individual ability
EvaluationAfter 6 hrs. of giving appropriate nursing interventions, goal not
met and Patient was not able to defecate.
Psychosocial dimension
Nursing interventionsAnticipatory grieving related to loss and altered role function
evidenced by patient’s verbalization and expression of guilty feeling as he forms a burden on his family.
Goal: Within 6 hrs. of giving appropriate nursing interventions, patient
will be able to identify and express feelings freely and effectively.
Nursing Interventions: Determined circumstances of current situation Encourage the Chaplin presence to clear out stressors Evaluated patient‘s perception of anticipated situation
Provided open environment and trusting relationship
Nursing Interventions: Be honest when answering questions, providing information Reviewed past life experiences and previous loss, noting
strengths and successes Given information that feelings are accepted and are to be
expressed appropriately Evaluation: After 6 hrs. of giving appropriate nursing interventions, goal
met. Patient was able to accept his situation and express feelings freely.
Spiritual dimension
Nursing interventionsFear and ineffective coping related to patient’s disease
progression and poor prognosis evidenced by patients verbalization of guilt feeling, regrets and helplessness.
Goal:Within 6 hrs. of giving appropriate nursing interventions, patient
will be able to perceive available support system (family support) to assist in coping up from fear .
Interventions: Presented information at patient‘s level of understanding or
acceptance Conveyed acceptance of the patient‘s perception of fear Used calm and reassuring approach. Spent time with patient in each shift
Interventions: Oriented family to patient‘s specific needs, allowing
family members to participate in giving care. Arranged for family member to stay with the patient Used relaxation technique to reduce attention of fear .
Evaluation : After 6 hrs. of giving appropriate nursing interventions,
goal met. Patient was able to perceive available support system (family support) to cope up form fear .
FAMILY CARE PLAN (WIFE) PHYSICAL Nursing interventionsSleep pattern disturbance related to interruptions by health
care professionals on V/S monitoring and care providing evidenced by his wife verbalization of inability to sleep well at night, feeling tired and restless during the day.
Goal: Within 2 days of giving appropriate nursing interventions, the
wife will be able to report good sleep pattern in absence of disturbance.
Interventions: Identified presence of related sleep disturbance factors Recommended restriction of caffeine

Interventions: Assessed her usual sleep pattern Determined her sleep expectations. Provided quiet environment
Evaluation: After 2 days of giving appropriate nursing interventions,
goal met, she was able to sleep within 4-5 hrs. in absence of disturbance
Psychosocial dimension
Nursing interventionsIneffective role performance related to changes in family dynamics
secondary to her husband’s illness evidenced by verbalization of not being able to perform her duty and responsibilities toward her sick son and feeling helpless toward her husband’s condition.
Goal: within 48 hours of nursing interventions the wife will verbalize
increased confidence in ability to deal with her current situation and adjust to possible role limitations.
Interventions: Discuss her perception of how she perceives limitations. Acknowledge and accept feelings of grief, hostility, and
dependency.

Interventions: Discuss meaning of loss or change to her . Ascertain how she views self in usual lifestyle functioning. Set limits on maladaptive behavior. Assist her to identify positive behaviors that will aid in coping.Involve her in planning care and scheduling activities.Evaluation: Goal was met as she could verbalize increased the confidence in ability to deal with her husband’s illness and current health condition.

Spiritual Dimension
Nursing interventionsRisk for spiritual distress related to challenged beliefs and
value systems evidenced by inability to express her personal response toward her dying husband.
Goal: within 48 hours of nursing interventions the wife will be
able to express her acceptance toward her husband’s health status and her personal response toward the dying process.
Interventions: Assess her for signs of depression. Assess her for signs of spiritual pain. Respect her beliefs. Promote the visitation of family and friends.
Be physically present and actively listen to her. Assist her in identifying meaningful experiences. Hold her hand or place hand gently on her arm if she is
comfortable with touch Assist the her in exploring reasons for living and
promote hope Assist her in any religious rites/rituals that she request. Allow her a privacy and a quiet place for prayer. Evaluation: Goal was met with the assistant of the spiritual advisor .
Thank you







