A Report from ASCO GI 2008
Up-to-Date Review of the Treatment of Metastatic Colorectal Cancer
Edward Chu, MDProfessor of Internal Medicine and Pharmacology
Chief, Section of Medical Oncology
Yale Cancer CenterYale University School of Medicine
New Haven, CT

Outline
• Cytotoxic chemotherapy
• FOLFOX and neurotoxicity
• FOLFOX versus XELOX
• Integration of biologics with cytotoxic chemotherapy
• Bevacizumab
• Bevacizumab plus panitumumab
• Biomarker development for anti-EGFR antibodies
Abstract 280
Hochster HS, Grothey A, Shpilsky A, Childs BH
Effect of Intravenous Calcium and Magnesium vs Placebo on Response to
FOLFOX+bevacizumab in theCONcePT Trial
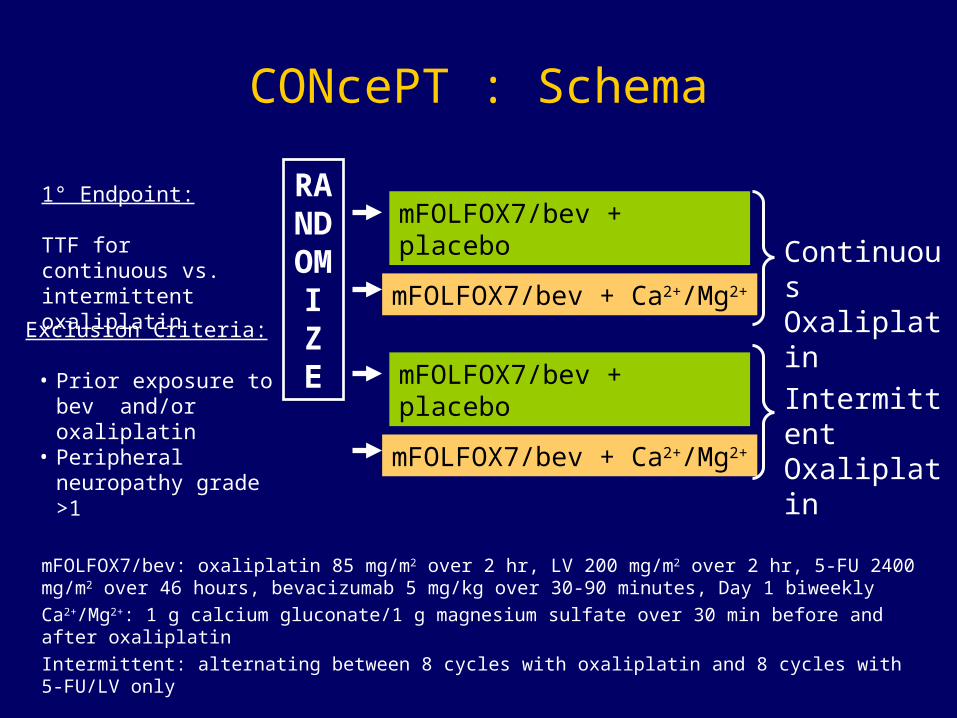
CONcePT : Schema
mFOLFOX7/bev: oxaliplatin 85 mg/m2 over 2 hr, LV 200 mg/m2 over 2 hr, 5-FU 2400 mg/m2 over 46 hours, bevacizumab 5 mg/kg over 30-90 minutes, Day 1 biweekly
Ca2+/Mg2+: 1 g calcium gluconate/1 g magnesium sulfate over 30 min before and after oxaliplatin
Intermittent: alternating between 8 cycles with oxaliplatin and 8 cycles with 5-FU/LV only
RANDOMIZE
mFOLFOX7/bev + placebo
mFOLFOX7/bev + Ca2+/Mg2+
mFOLFOX7/bev + placebo
mFOLFOX7/bev + Ca2+/Mg2+
Continuous Oxaliplatin
Intermittent Oxaliplatin
1° Endpoint:
TTF for continuous vs. intermittent oxaliplatin
Exclusion Criteria:
• Prior exposure to bev and/or oxaliplatin
• Peripheral neuropathy grade >1
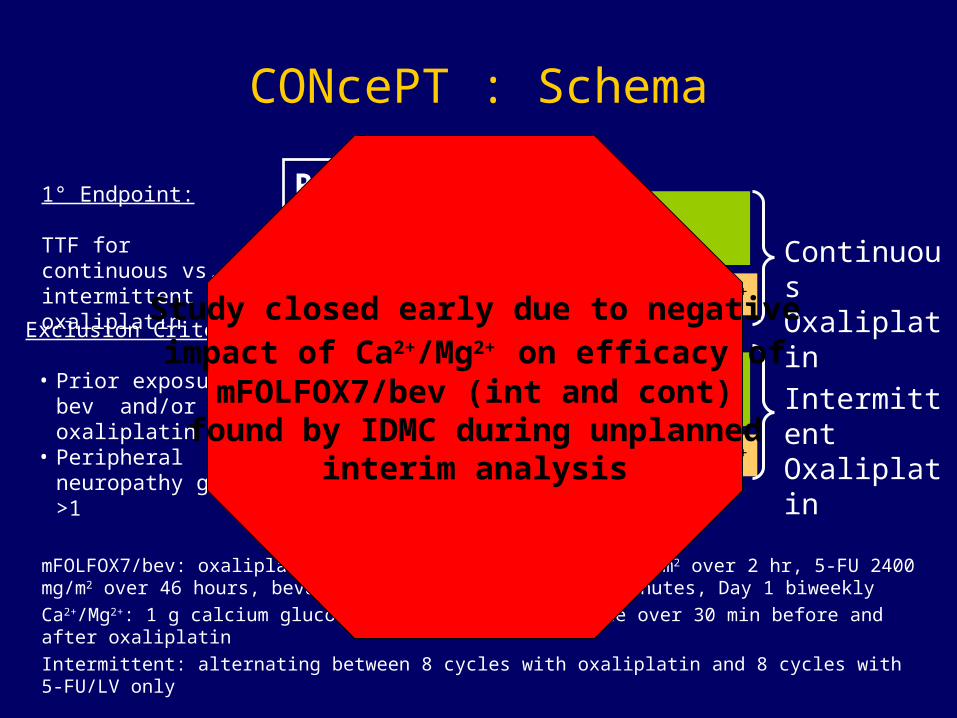
CONcePT : Schema
mFOLFOX7/bev: oxaliplatin 85 mg/m2 over 2 hr, LV 200 mg/m2 over 2 hr, 5-FU 2400 mg/m2 over 46 hours, bevacizumab 5 mg/kg over 30-90 minutes, Day 1 biweekly
Ca2+/Mg2+: 1 g calcium gluconate/1 g magnesium sulfate over 30 min before and after oxaliplatin
Intermittent: alternating between 8 cycles with oxaliplatin and 8 cycles with 5-FU/LV only
RANDOMIZE
mFOLFOX7/bev + placebo
mFOLFOX7/bev + Ca2+/Mg2+
mFOLFOX7/bev + placebo
mFOLFOX7/bev + Ca2+/Mg2+
Continuous Oxaliplatin
Intermittent Oxaliplatin
1° Endpoint:
TTF for continuous vs. intermittent oxaliplatin
Exclusion Criteria:
• Prior exposure to bev and/or oxaliplatin
• Peripheral neuropathy grade >1
Study closed early due to negative impact of Ca2+/Mg2+ on efficacy of
mFOLFOX7/bev (int and cont)found by IDMC during unplanned
interim analysis

CONcePT : Clinical Efficacy
ContPlacebo(N = 34)
Cont Ca2+Mg2+
(N = 35)
IntPlacebo(N = 36)
IntCa2+Mg2+
(N = 35)
Median Duration of Treatment
15.1 17.1 28.1 18.1
ORR (evaluable), % 21 36 45 43
Discontinuation of Treatment, N
Adverse Event 16 13 8 12
Progression 9 5 8 8
Physician/Pt Decision 8 14 10 11
Other 1 2 10 4
• Two-factor logistic regression exploratory model of response data revealed no significant relationship between use of Ca2+/Mg2+ and response
• Future reports of neuroprophylaxis await pending data
CONcePT: Conclusions
Abstract 347
Ramanathan RK, André T, Rothenberg ML, de Gramont A,
Tournigand C, Goldberg RM, Gupta S
Diabetes Mellitus and the Incidence and Time to Onset of Oxaliplatin-Induced
Peripheral Sensory Neuropathy (PSN) in Patients with Colorectal Cancer: A Pooled
Analysis of Three Randomized Studies

Pooled Analysis
• Conducted pooled analysis of data from randomized clinical trials including FOLFOX4 treatment arm
– EFC3313 (MOSAIC): 5-FU and LV (LV5–FU2) + oxaliplatin as adjuvant therapy in CRC
– EFC4584: Three-arm study of LV5–FU2, LV5–FU2 with oxaliplatin, or oxaliplatin alone as second-line therapy of metastatic CRC
– EFC2962: Phase II/III study of LV5–FU2 + oxaliplatin
• PSN data from the overall study population with or without diabetes were analyzed for:
– Incidence and time to onset of PSN (Kaplan-Meier)
– Trends indicating clinically relevant differences in the incidence and severity of PSN (Kaplan-Meier)
Ramanathan et al, ASCO GI 2008, abstract 347.

Incidence and Severity of PSN
PSNAll Patients
(N = 1585)
DM Patients (N = 135)
Grade 1 45.2 46.7
Grade 2 28.4 26.7
Grade 3 13.0 12.6
Ramanathan et al, ASCO GI 2008, abstract 347.
Conclusions
• Patients with diabetes mellitus do not have an increased risk of developing cumulative neurotoxicity
Abstract 341
Cassidy J, Clarke S, Diaz-Rubio E, Scheithauer W, A. Figer A,
Wong R, Koski S, Sirzen F, Gilberg F, Saltz L
XELOX vs. FOLFOX-4: Update of Efficacy Results from XELOX-1/NO16966, a
Randomized Phase III Trial of First-Line Treatment for Patients with Metastatic
Colorectal Cancer (MCRC)
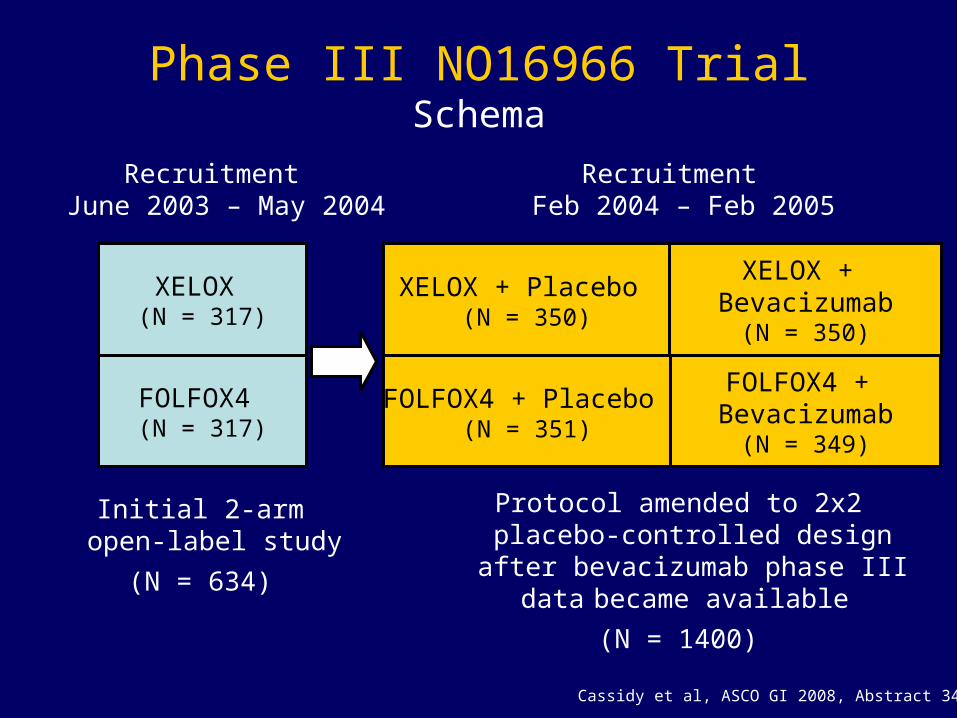
Phase III NO16966 TrialSchema
Cassidy et al, ASCO GI 2008, Abstract 341.
XELOX + Placebo (N = 350)
FOLFOX4 + Placebo (N = 351)
XELOX + Bevacizumab
(N = 350)
FOLFOX4 + Bevacizumab
(N = 349)
XELOX (N = 317)
FOLFOX4 (N = 317)
Initial 2-armopen-label study
(N = 634)
Protocol amended to 2x2 placebo-controlled design after bevacizumab
phase III data became available
(N = 1400)
RecruitmentJune 2003 – May 2004
RecruitmentFeb 2004 – Feb 2005

XELOX-1/NO16966 TrialAdverse Events
Grade 3/4 Adverse Events, %FOLFOX-4 + Placebo
(N = 649)XELOX + Placebo
(N = 655)
Diarrhea <12 20
Nausea 5 5
Stomatitis 2 1
Peripheral Neuropathy 4 4
Peripheral Sensory Neuropathy 3 3
Hand-foot syndrome 1 6
Fatigue <9 <6
Paresthesia 4 5
Neutropenia 43 <7
Febrile neutropenia 5 <2
Thrombocytopenia <4 7
Cassidy et al, ASCO GI 2008, Abstract 341.
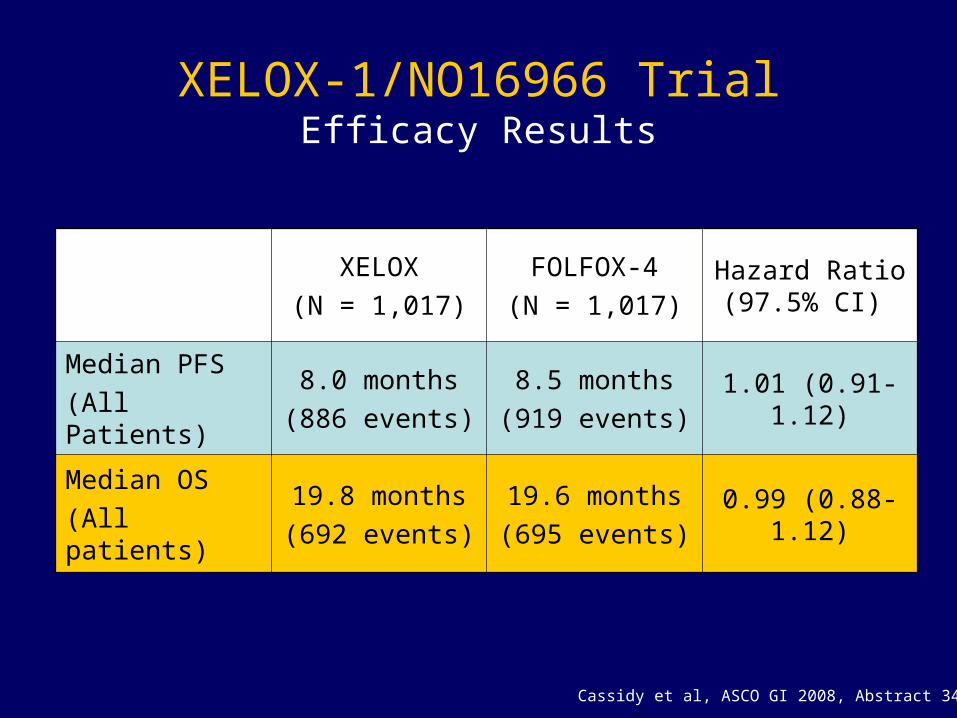
XELOX-1/NO16966 TrialEfficacy Results
XELOX
(N = 1,017)
FOLFOX-4
(N = 1,017)Hazard Ratio (97.5% CI)
Median PFS
(All Patients)
8.0 months
(886 events)
8.5 months
(919 events)1.01 (0.91-1.12)
Median OS
(All patients)
19.8 months
(692 events)
19.6 months
(695 events)0.99 (0.88-1.12)
Cassidy et al, ASCO GI 2008, Abstract 341.

Abstract 340
Cassidy J, Rothenberg M, Saltz L, Twelves C, Van Cutsem E,Hoff P, Kang Y-K, Sirzen F, Gilberg F, Cunningham D
Efficacy of Capecitabine vs. 5-FU in Colorectal and Gastric Cancer:
Meta-analysis of Survival in 6 Clinical Trials
Meta-Analysis: Capecitabine vs 5-FU
• Included individual patient data from 6 phase III trials comparing the efficacy of capecitabine and 5-FU in metastatic colorectal and gastric cancers
• Main endpoint was overall survival
• Assessment completed with unstratified and stratified (by study) data
• Included 6,171 patients (3,074 received 5-FU-based regimens and 3,097 received capecitabine-based regimens)
• Unstratified data found a median OS of 23.1 and 22.4 months for patients who received capecitabine and 5-FU, respectively (HR = 0.96)
Cassidy J et al, ASCO GI 2008, abstract 340.
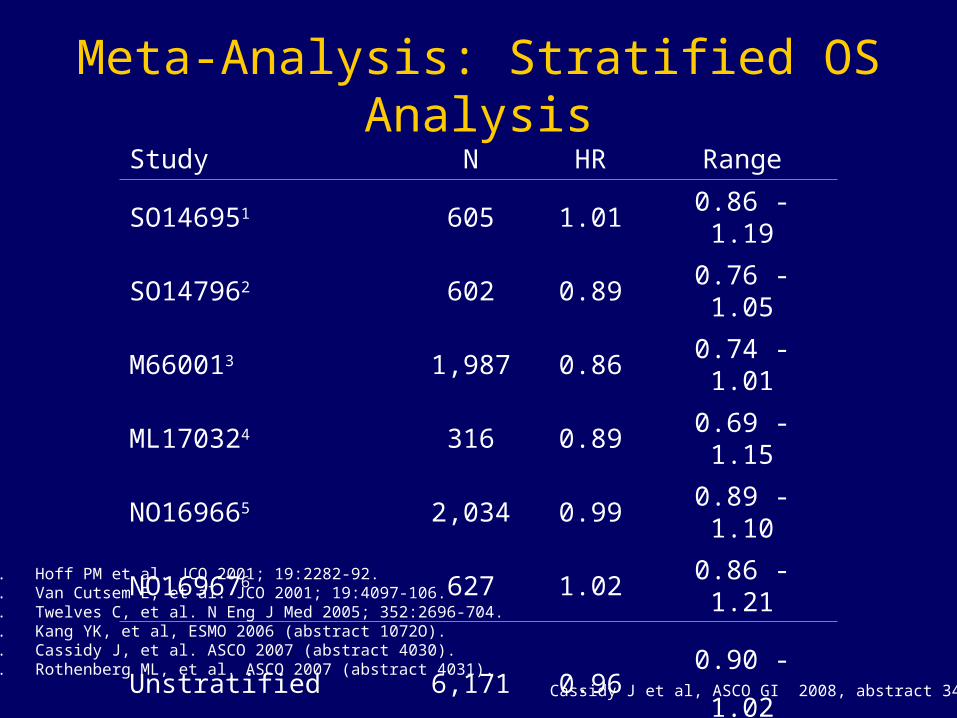
Meta-Analysis: Stratified OS AnalysisStudy N HR Range
SO146951 605 1.01 0.86 - 1.19
SO147962 602 0.89 0.76 - 1.05
M660013 1,987 0.86 0.74 - 1.01
ML170324 316 0.89 0.69 - 1.15
NO169665 2,034 0.99 0.89 - 1.10
NO169676 627 1.02 0.86 - 1.21
Unstratified 6,171 0.96 0.90 - 1.02
1. Hoff PM et al. JCO 2001; 19:2282-92.2. Van Cutsem E, et al. JCO 2001; 19:4097-106.3. Twelves C, et al. N Eng J Med 2005; 352:2696-704.4. Kang YK, et al, ESMO 2006 (abstract 1072O).5. Cassidy J, et al. ASCO 2007 (abstract 4030).6. Rothenberg ML, et al. ASCO 2007 (abstract 4031).
Cassidy J et al, ASCO GI 2008, abstract 340.

Conclusions
• Findings of meta-analysis suggest:
– Equivalency of capecitabine and 5-FU in the treatment of adjuvant and metastatic colorectal cancer
– Equivalency of capecitabine and 5-FU in the treatment of metastatic gastric cancer
• Equivalency of capecitabine and 5-FU is supported by updated results of the NO16966 trial comparing capecitabine and 5-FU as treatment for metastatic colorectal cancer
Abstract 342
Arkenau H-T, Arnold D, Diaz-Rubio E, Douillard J-Y, Martoni A,Grothey A, Hinke A, Schmiegel W, Schmoll H-J, Porschen R
Capecitabine and Oxaliplatin as First-Line Treatment in Patients with MCRC:A Meta-analysis of Randomized
Phase II-III Trials
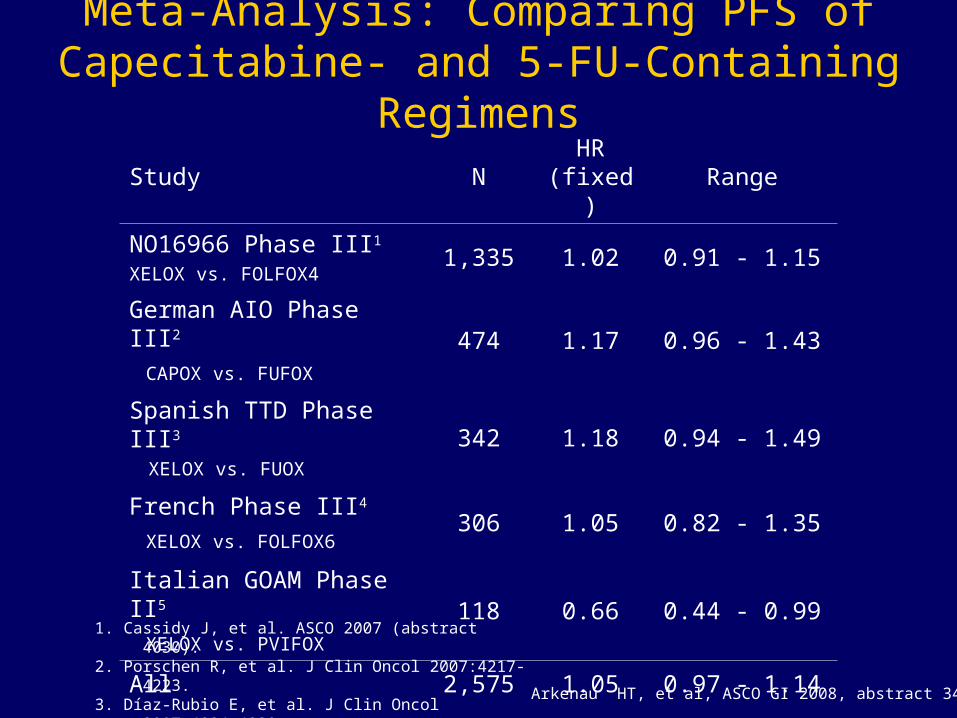
Meta-Analysis: Comparing PFS of Capecitabine- and 5-FU-Containing Regimens
Study NHR
(fixed)Range
NO16966 Phase III1
XELOX vs. FOLFOX41,335 1.02 0.91 - 1.15
German AIO Phase III2
CAPOX vs. FUFOX474 1.17 0.96 - 1.43
Spanish TTD Phase III3
XELOX vs. FUOX342 1.18 0.94 - 1.49
French Phase III4
XELOX vs. FOLFOX6306 1.05 0.82 - 1.35
Italian GOAM Phase II5
XELOX vs. PVIFOX118 0.66 0.44 - 0.99
All 2,575 1.05 0.97 - 1.14
Arkenau HT, et al, ASCO GI 2008, abstract 342.
1. Cassidy J, et al. ASCO 2007 (abstract 4030).2. Porschen R, et al. J Clin Oncol 2007:4217-4223.3. Díaz-Rubio E, et al. J Clin Oncol 2007:4224-4230.4. Ducreux M, et al. ASCO 2007 (abstract 4029).5. Martoni A, et al. Eur J Cancer 2006: 3161-3168.
Conclusions
• Findings of meta-analysis suggest non-inferiority of capecitabine/oxaliplatin compared to 5-FU/oxaliplatin, based on PFS analysis and combination regimens.
Abstract 350
Berry S, Cunningham D, Michael M, Kretzschmar A,Rivera F, DiBartolomeo M, Mazier M, Van Cutsem E,
on behalf of the First BEAT investigators
Preliminary Efficacy of Bevacizumab with First-Line FOLFOX, XELOX, FOLFIRI and Fluoropyrimidines for MCRC: First BEAT
First BEAT: Study Schema
First-line metastatic
CRC (1,965)
Bevacizumab + standard
chemotherapyPD
• Bevacizumab: 5 mg/kg Q2W or 7.5 mg/kg Q3W
• Endpoints: safety and efficacy
• Median follow-up 22.9 months
Berry et al, ASCO GI 2008, abstract 350.
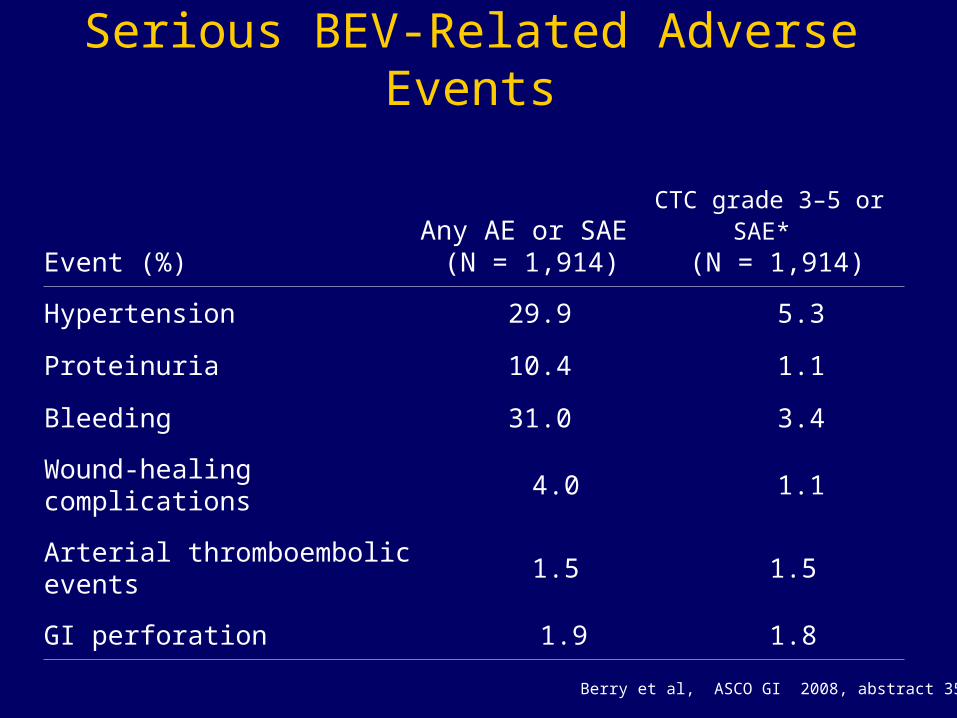
Serious BEV-Related Adverse Events
Event (%)Any AE or SAE
(N = 1,914)CTC grade 3–5 or SAE*
(N = 1,914)
Hypertension 29.9 5.3
Proteinuria 10.4 1.1
Bleeding 31.0 3.4
Wound-healing complications 4.0 1.1
Arterial thromboembolic events 1.5 1.5
GI perforation 1.9 1.8
Berry et al, ASCO GI 2008, abstract 350.
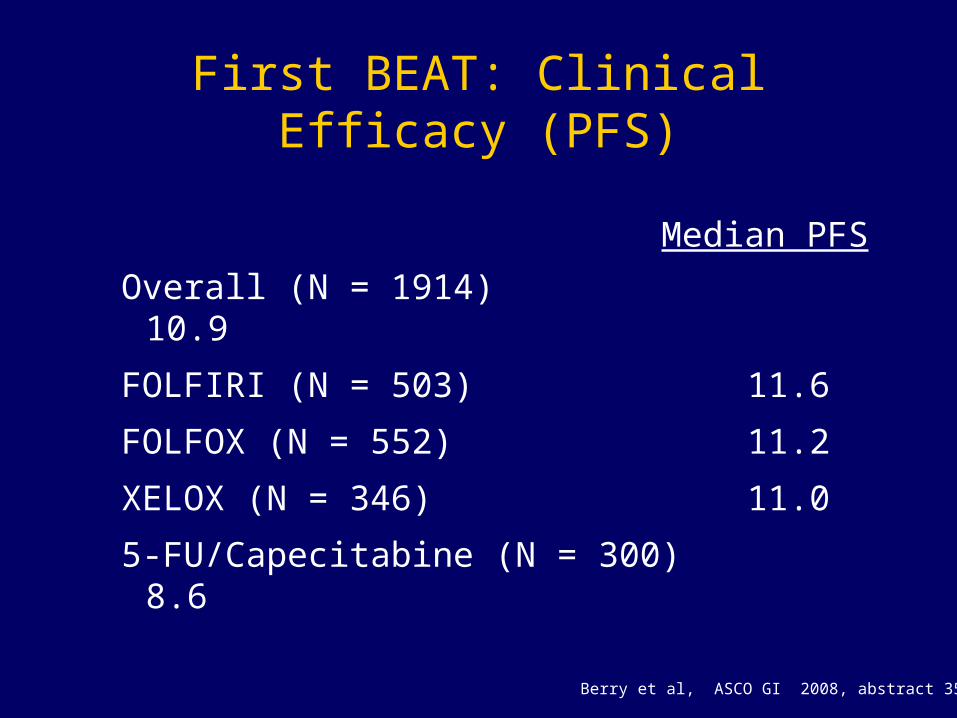
First BEAT: Clinical Efficacy (PFS)
Median PFS
Overall (N = 1914) 10.9
FOLFIRI (N = 503) 11.6
FOLFOX (N = 552) 11.2
XELOX (N = 346) 11.0
5-FU/Capecitabine (N = 300) 8.6
Berry et al, ASCO GI 2008, abstract 350.
Abstract 363
Masi G, Loupakis F, Baldi G, Fornaro L, Di Leo A,Ciarlo A, Amoroso D, Granetto C, Di Donato S, Falcone A
First-line Irinotecan, Oxaliplatin and Infusional 5FU/LV (FOLFOXIRI) in Combination with Bevacizumab (BV) in MCRC Patients (pts):
A Phase II Study by the GONO Group
Study Design
Masi et al, ASCO GI 2008, abstract 363.
• Phase II trial evaluating first-line therapy with FOLFOXIRI plus Bev in patients with initially unresectable mCRC
• Primary endpoint: PFS rate at 10 months
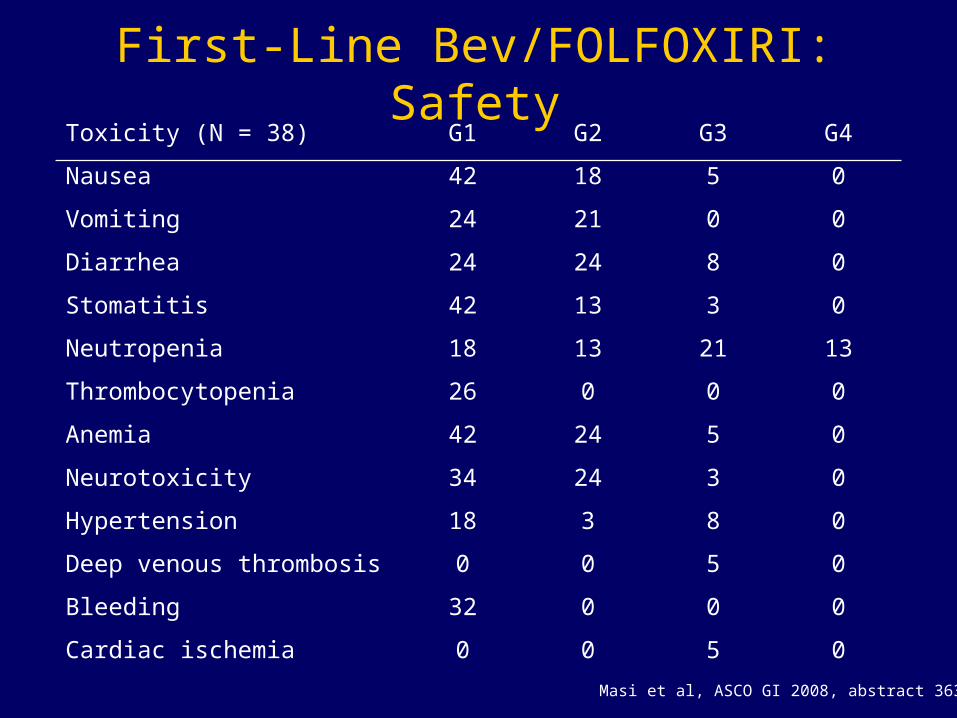
First-Line Bev/FOLFOXIRI: SafetyToxicity (N = 38) G1 G2 G3 G4
Nausea 42 18 5 0
Vomiting 24 21 0 0
Diarrhea 24 24 8 0
Stomatitis 42 13 3 0
Neutropenia 18 13 21 13
Thrombocytopenia 26 0 0 0
Anemia 42 24 5 0
Neurotoxicity 34 24 3 0
Hypertension 18 3 8 0
Deep venous thrombosis 0 0 5 0
Bleeding 32 0 0 0
Cardiac ischemia 0 0 5 0
Masi et al, ASCO GI 2008, abstract 363.
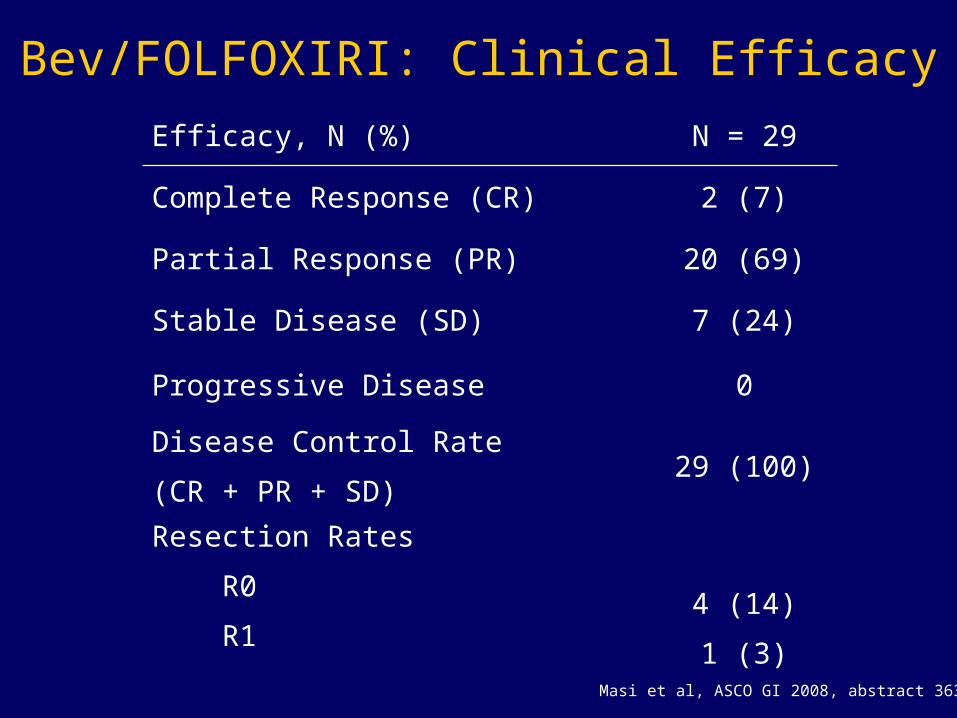
Bev/FOLFOXIRI: Clinical Efficacy
Efficacy, N (%) N = 29
Complete Response (CR) 2 (7)
Partial Response (PR) 20 (69)
Stable Disease (SD) 7 (24)
Progressive Disease 0
Disease Control Rate
(CR + PR + SD)29 (100)
Resection Rates
R0
R1
4 (14)
1 (3)
Masi et al, ASCO GI 2008, abstract 363.

Bev/FOLFOXIRI: Conclusions
• First-line therapy with bevacizumab/FOLFOXIRI associated with high response rates (76%) and 100% tumor control, in patients with MCRC
• High response rates coincided with high R0 resection rate in initially unresectable patients
• Grade 3/4 toxicities included nausea, diarrhea, stomatitis, neutropenia, anemia, neurotoxicity, hypertension, deep vein thrombosis, and cardiac ischemia

Abstract 273
Hecht J. R., Mitchell E, Chidiac T, Scroggin C, Hagenstad C,Spigel D, Marshall J, Cohn A, Shahin S, Griffin T
An Updated Analysis of Safety and Efficacy of Oxaliplatin (Ox)/bevacizumab (bev) +/-
Panitumumab (pmab) for First-line Treatment (tx) of MCRC from a Randomized, Controlled
Trial (PACCE)
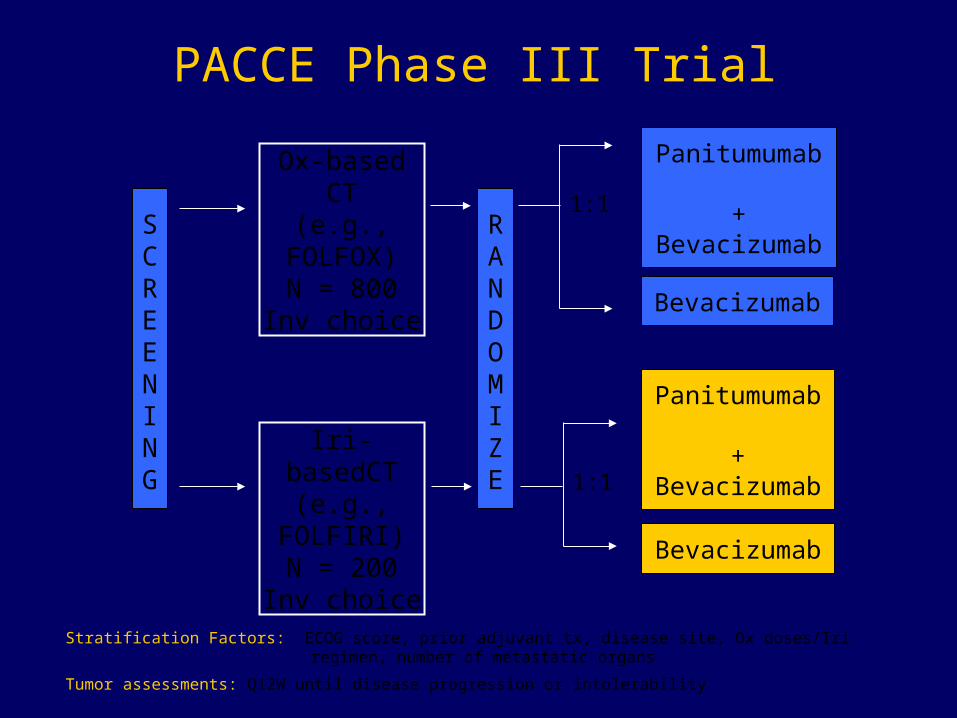
Stratification Factors: ECOG score, prior adjuvant tx, disease site, Ox doses/Iri regimen, number of metastatic organs
Tumor assessments: Q12W until disease progression or intolerability
Panitumumab +
Bevacizumab
Ox-based CT(e.g.,
FOLFOX)N = 800
Inv choice
Iri-basedCT(e.g.,
FOLFIRI)N = 200
Inv choice
Bevacizumab
Panitumumab +
Bevacizumab
Bevacizumab
RANDOMIZE
1:1
1:1
SCREENING
PACCE Phase III Trial
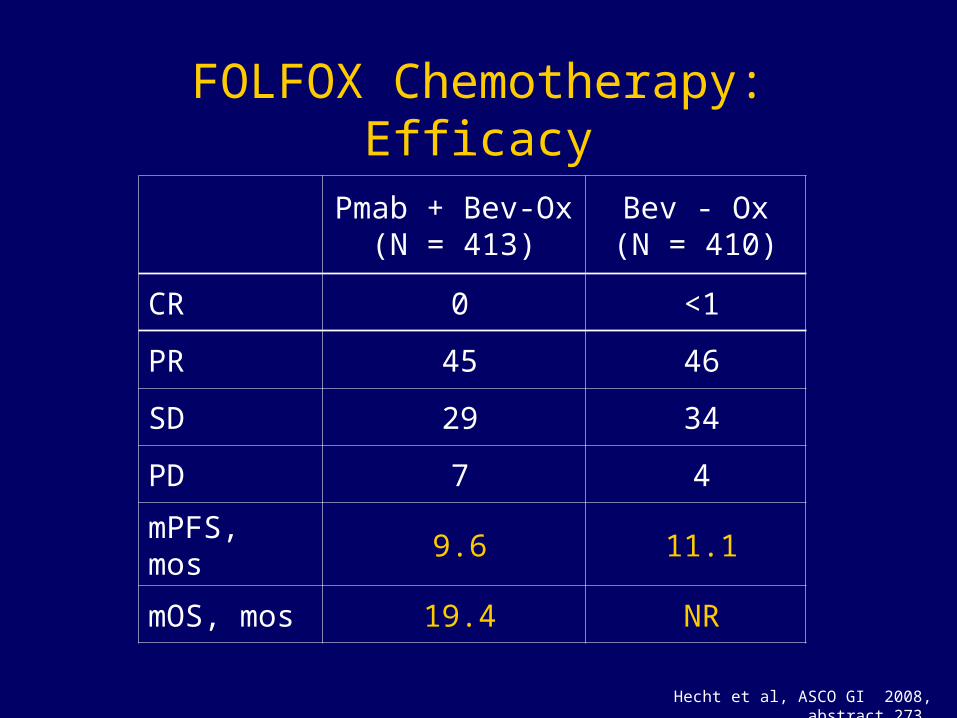
FOLFOX Chemotherapy: Efficacy
Pmab + Bev-Ox(N = 413)
Bev - Ox(N = 410)
CR 0 <1
PR 45 46
SD 29 34
PD 7 4
mPFS, mos 9.6 11.1
mOS, mos 19.4 NR
Hecht et al, ASCO GI 2008, abstract 273.
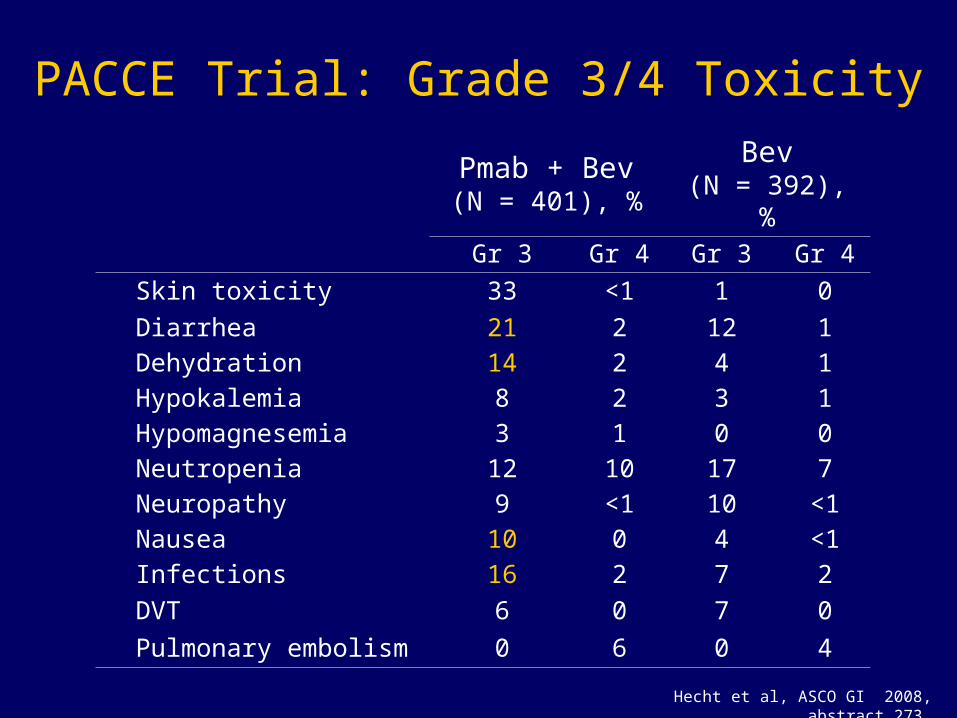
Pmab + Bev(N = 401), %
Bev(N = 392), %
Gr 3 Gr 4 Gr 3 Gr 4
Skin toxicity 33 <1 1 0
Diarrhea 21 2 12 1
Dehydration 14 2 4 1
Hypokalemia 8 2 3 1
Hypomagnesemia 3 1 0 0
Neutropenia 12 10 17 7
Neuropathy 9 <1 10 <1
Nausea 10 0 4 <1
Infections 16 2 7 2
DVT 6 0 7 0
Pulmonary embolism 0 6 0 4
PACCE Trial: Grade 3/4 Toxicity
Hecht et al, ASCO GI 2008, abstract 273.
Abstract 279
Hecht J. R., Mitchell E, Chidiac T, Scroggin C, Hagenstad C,
Spigel D, Marshall J, Cohn A, Suzuki S, Griffin T
Interim Results from PACCE: Irinotecan (Iri)/bevacizumab (bev) + Panitumumab (pmab)
as First-line Treatment (tx) for MCRC

FOLFIRI Chemotherapy: Efficacy
Hecht et al, ASCO GI 2008, abstract 279.
Pmab+ Bev-Iri(N = 115)
Bev-Iri(N = 115)
CR 0 0
PR 43 39
mut KRAS (N = 46)
30 38
WT KRAS (N = 57)
54 47
SD 27 38
PD 13 3
mPFS, mos 10.1 11.7
mOS, mos 20.7 20.5

PACCE FOLFIRI Chemotherapy: Discontinuation of Treatment
Reason for Discontinuation, N(%)
Pmab+ Bev-Iri(N = 115)
Bev-Iri(N = 115)
Discontinued First-line 102 (89) 99 (86)
Disease Progression 36 (35) 27 (27)
Death 6 (6) 2 (2)
Adverse Events 17 (17) 6 (6)
Protocol Violation 3 (3) 5 (5)
Consent Withdrawn 15 (15) 33 (33)
Hecht et al, ASCO GI 2008, abstract 279.

PACCE: Safety Analysis of FOLFIRI Arms Pmab+ Bev/Iri (N = 111) Bev/Iri (N = 113)
Adverse Event, % Grade 3 Grade 4 Grade 3 Grade 4
Skin Toxicity 37 0 0 0
Diarrhea 27 1 9 0
Neutropenia 14 3 17 4
Dehydration 14 0 6 0
Infections 12 2 9 0
Nausea 10 2 6 0
Hypokalemia 9 2 4 0
Vomiting 8 2 7 0
Paronychia 4 0 0 0
Hypomagnesemia 3 2 0 1
Hypertension 2 0 3 0
Deep Vein Thrombosis 13 0 6 0
Pulmonary Embolism 0 11 0 5
Hecht et al, ASCO GI 2008, abstract 279.

PACCE Trial: Conclusions• Addition of panitumumab to oxaliplatin-containing
chemotherapy+bevacizumab worsened PFS and increased toxicity
• Panitumumab added to irinotecan modestly increased response, although PFS and OS were similar for both treatment arms
• Toxicity of panitumumab/bev-iri was considerable, additionally causing 2% grade 5 infections and gastrointestinal perforation, and 1% grade 5 pulmonary embolism
• Most patients discontinued treatment for non-progressive events
• Panitumumab/bev-iri improved response rates (54% vs. 47%) in patients with wild type KRAS tumor status
• Evaluation of toxicity is ongoing
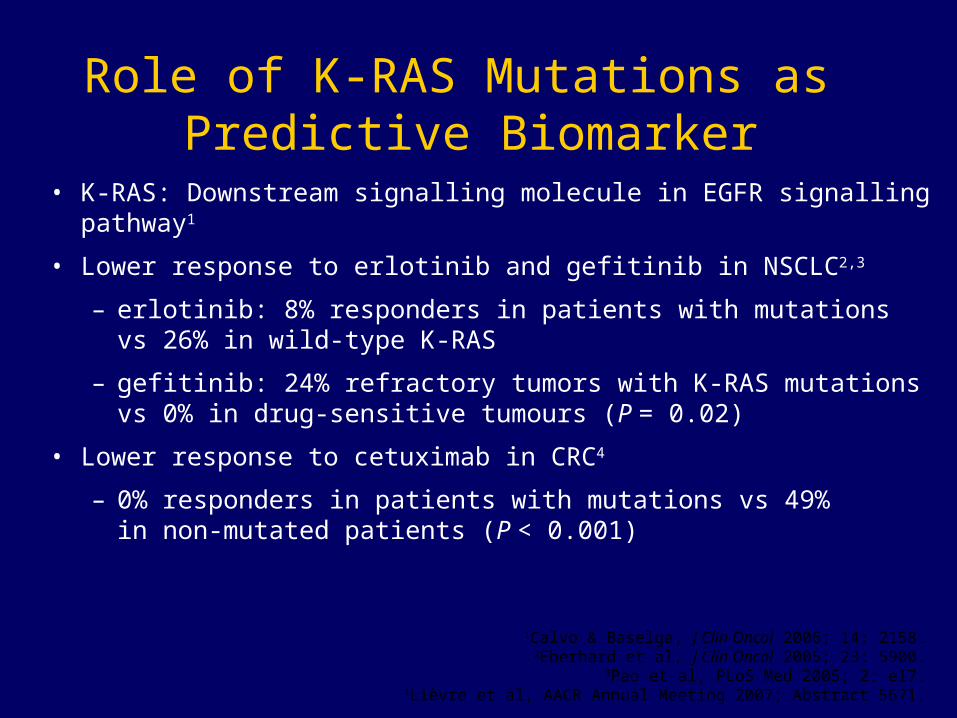
Role of K-RAS Mutations as Predictive Biomarker
• K-RAS: Downstream signalling molecule in EGFR signalling pathway1
• Lower response to erlotinib and gefitinib in NSCLC2,3
– erlotinib: 8% responders in patients with mutations vs 26% in wild-type K-RAS
– gefitinib: 24% refractory tumors with K-RAS mutationsvs 0% in drug-sensitive tumours (P = 0.02)
• Lower response to cetuximab in CRC4
– 0% responders in patients with mutations vs 49% in non-mutated patients (P < 0.001)
1Calvo & Baselga, J Clin Oncol 2006; 14: 2158.2Eberhard et al, J Clin Oncol 2005; 23: 5900.
3Pao et al, PLoS Med 2005; 2: e17.4Lièvre et al, AACR Annual Meeting 2007; Abstract 5671.
Abstract 278
Amado R, Wolf M, Freeman D, Peeters M, Van Cutsem E,Siena S, Suggs S, Devercelli G, Woolley M, and Chang D
Panitumumab Efficacy and Patient-Reported Outcomes in MCRC Patients withWild-Type KRAS Tumor Status
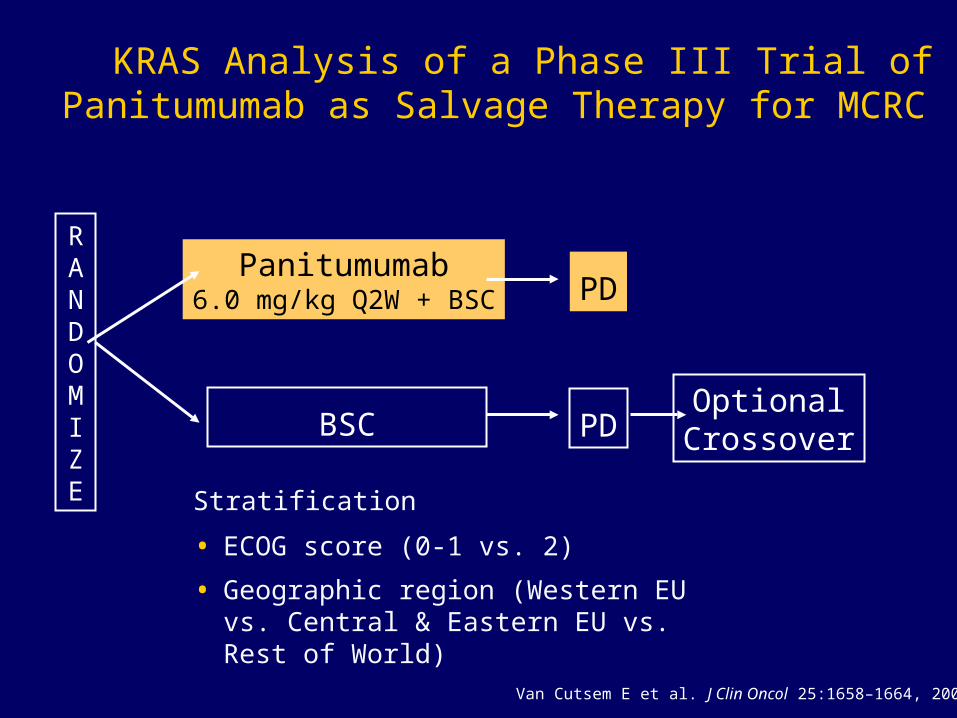
Stratification
• ECOG score (0-1 vs. 2)
• Geographic region (Western EU vs. Central & Eastern EU vs. Rest of World)
KRAS Analysis of a Phase III Trial of Panitumumab as Salvage Therapy for MCRC
Van Cutsem E et al. J Clin Oncol 25:1658–1664, 2007.
RANDOMIZE
Panitumumab6.0 mg/kg Q2W + BSC PD
OptionalCrossoverBSC PD
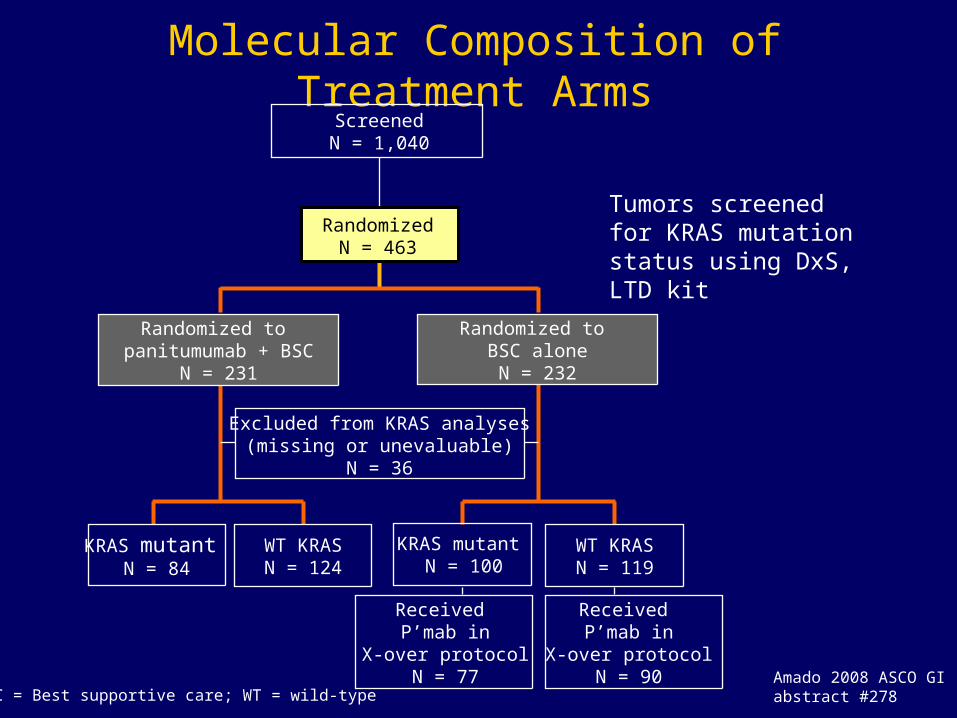
Molecular Composition of Treatment ArmsScreenedN = 1,040
RandomizedN = 463
Randomized to panitumumab + BSC
N = 231
Randomized to BSC alone
N = 232
Excluded from KRAS analyses(missing or unevaluable)
N = 36
KRAS mutant N = 84
WT KRASN = 124
KRAS mutant N = 100
WT KRASN = 119
Received P’mab in
X-over protocolN = 77
Received P’mab in
X-over protocolN = 90
BSC = Best supportive care; WT = wild-type
Tumors screened for KRAS mutation status using DxS, LTD kit
Amado 2008 ASCO GIabstract #278

Percent Decrease of Target Lesions in KRAS Evaluable Patients
16014012010080604020%
Cha
nge
-20-40-60-80
0
PR (0%) SD (12%) PD (70%)
Mutant
Patient
Pmab+ BSC
16014012010080604020%
Cha
nge
-20-40-60-80
0
PR (17%) SD (34%) PD (36%)
Wild-Type
Patient16014012010080604020
% C
hang
e
-20-40-60-80
0
PR (0%) SD (8%) PD (60%)
Patient
BSCAlone
16014012010080604020%
Cha
nge
-20-40-60-80
0
PR (0%) SD (12%) PD (75%)
Patient
BSC = Best supportive care; Pmab = panitumumab Amado et al, ASCO GI 2008, abstract 278.
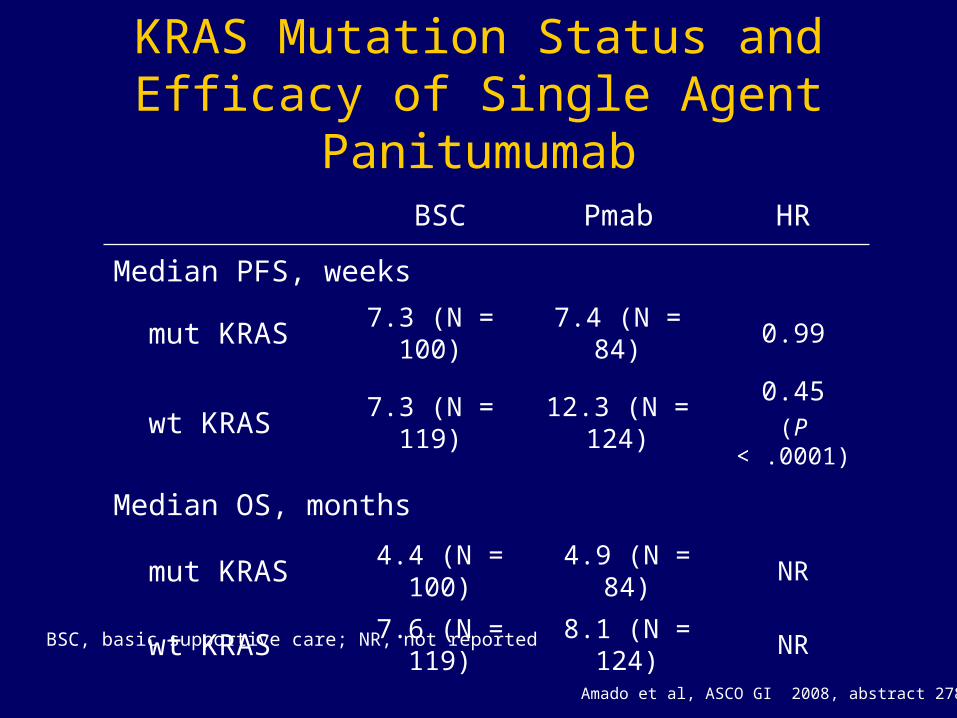
KRAS Mutation Status and Efficacy of Single Agent Panitumumab
BSC Pmab HR
Median PFS, weeks
mut KRAS 7.3 (N = 100) 7.4 (N = 84) 0.99
wt KRAS 7.3 (N = 119) 12.3 (N = 124)0.45
(P < .0001)
Median OS, months
mut KRAS 4.4 (N = 100) 4.9 (N = 84) NR
wt KRAS 7.6 (N = 119) 8.1 (N = 124) NR
BSC, basic supportive care; NR, not reported
Amado et al, ASCO GI 2008, abstract 278.
Conclusions
• Salvage single agent panitumumab significantly (P < .0001) improved PFS in patients with KRAS wild type tumors with no benefit in those having mutant KRAS tumors
• Only patients with wild type KRAS benefited from single agent panitumumab in the salvage setting
• Long-term outcome of patients was primarily dictated by KRAS mutation status
• Future studies will focus on prospective analysis of the efficacy of panitumumab-containing combination therapy in patients with wild type and mutant KRAS tumors
Abstract 343
Hecht JR, Mitchell EP, Baranda J, Richards D, Reiner M, Stout S, Amado RG
Panitumumab Efficacy in Patients with MCRC with Low or Undetectable Levels of Epidermal Growth Factor Receptor: Final Efficacy and KRAS Analysis

Trial Design
Hecht et al, ASCO GI 2008, abstract 343.
• Phase II single-arm, open-label study
• Patients received panitumumab 6 mg/kg (Q2W) until disease progression or unacceptable toxicity
• Previous analyses indicated that panitumumab efficacy is independent of tumor EGFR expression levels (Mitchell, ASCO 2007 abstract 4082, Hecht, ASCO GI 2007 abstract 350)
• Exploratory analysis of KRAS mutation status
– Total of 203 pts enrolled
– EGFR expression levels available for 195 pts
– KRAS mutation status available for 171 pts (55% wild type, 45% mutant)
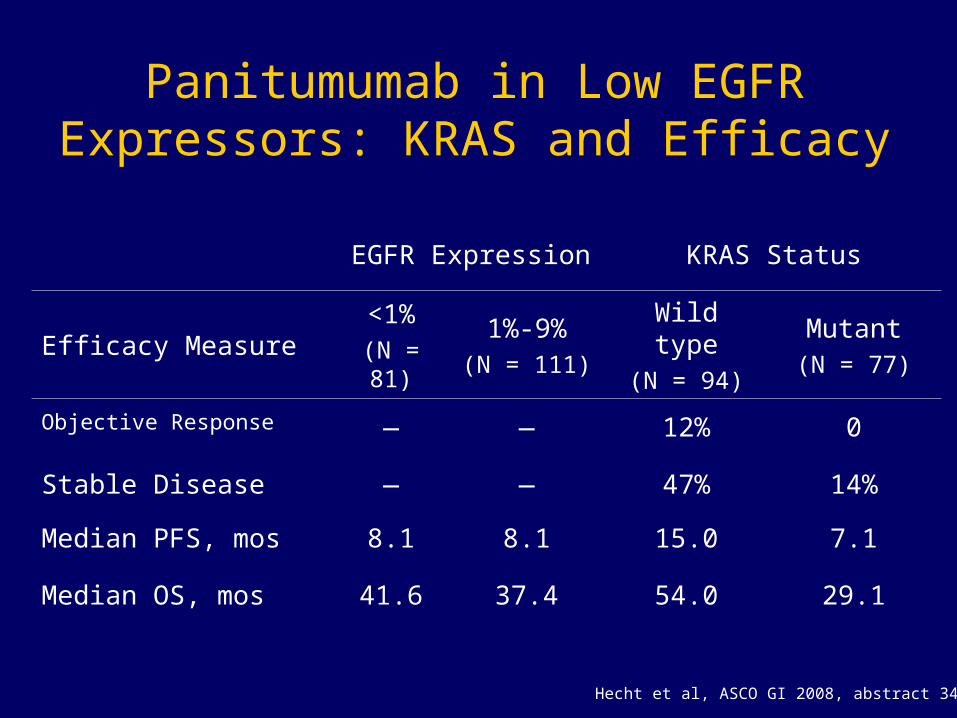
EGFR Expression KRAS Status
Efficacy Measure<1%
(N = 81)
1%-9%(N = 111)
Wild type(N = 94)
Mutant(N = 77)
Objective Response — — 12% 0
Stable Disease — — 47% 14%
Median PFS, mos 8.1 8.1 15.0 7.1
Median OS, mos 41.6 37.4 54.0 29.1
Panitumumab in Low EGFR Expressors: KRAS and Efficacy
Hecht et al, ASCO GI 2008, abstract 343.
Conclusions
• Patients received panitumumab 6 mg/kg (Q2W) until disease progression or unacceptable toxicity
• EGFR expression levels, by immunohistochemistry, do not correlate with clinical benefit in treated patients
• Response to panitumumab in treated patients correlates with wild-type KRAS status
• Progression-free survival is doubled, and overall survival nearly doubled, when comparing clinical benefit in patients with wild type and mutant KRAS
Hecht et al, ASCO GI 2008, abstract 343.
Abstract 411
Tejpar S, De Roock W, Biesmans B, De Schutter J, Piessevaux H,Humblet Y, Peeters M, Celik I, Van Cutsem E
High Amphiregulin and Epiregulin Expression in KRAS Wild Type Colorectal Primaries Predicts
Response and Survival Benefit After Treatment with Cetuximab and Irinotecan for Metastatic Disease
Study Design
• Primary tumor specimens from patients treated on clinical trials with cetuximab and irinotecan for metastatic colorectal carcinoma
• 152 patients with irinotecan-refractory disease were identified who had been treated with cetuximab
• Tumors were analyzed for KRAS mutation status and amphiregulin and epiregulin mRNA levels
Tejpar et al, ASCO GI 2008, abstract 411.
Findings
• mRNA levels of epiregulin and amphiregulin were significantly correlated (P < .0001)
• KRAS was mutated in 43% (64/149) patients
• Wild type KRAS and high EGFR ligand levels significantly correlated (P = .03 for amphiregulin and P = .02 for epiregulin) with each other
• Response correlated with mutation status: ORR was 39.7% for patients with wild type KRAS and < 1% for those with mutant KRAS
• Patients who achieved objective response were approximately 4 times more likely to have tumors with high (above median) levels of amphiregulin and epiregulin
Tejpar et al, ASCO GI 2008, abstract 411.

Findings
KRAS Status Epiregulin Exp.Median PFS
mos
Median OS
mos
All < 0.5233 12 26
> 0.5233 30 45.86
Overall 18 36
Wild-type < 0.5233 12 31.57
> 0.5233 36 65.4
Overall 24.14 44.29
Mutant < 0.5233 12 22.86
> 0.5233 12 29.14
Overall 12 24.3
P < .001
P < .001
Tejpar et al, ASCO GI 2008, abstract 411.

Conclusions
• Patients with irinotecan-refractory disease who have mutant KRAS status received no benefit from cetuximab treatment in terms of response
• Patients with tumors expressing above-median levels of epiregulin and amphiregulin, excluding those with mutant KRAS, have significantly longer progression-free and overall survival than those with below-median levels
• This study supports the notion that response to cetuximab therapy depends upon KRAS status, and further suggests that patients with high expression of epiregulin and amphiregulin benefit the most from cetuximab therapy
Tejpar et al, ASCO GI 2008, abstract 411.

A Report from ASCO GI 2008
Up-to-Date Review of the Treatment of Metastatic Colorectal Cancer
Thank You!







