ADRA DRC 1| page
ADRA DRC
Capacity Statement
Adventist Development and Relief Agency in DRC 10102 Route de Matadi, Ngaliema,
Kinshasa, DRC 8802

ADRA DRC 2| page
Summary
The Adventist Development and Relief Agency (ADRA) DR Congo is part of the ADRA Network a
global humanitarian organization with a mission to work with people in poverty and distress to create just
and positive change. ADRA network, comprises of more than 120 supporting and implementing country
offices worldwide. ADRA Network has a regional office in Africa based in Nairobi for technical support.
ADRA is an Agency of the Seventh-day Adventist Church who works in humanitarian development and
relief services. ADRA in DRC shares the same vision with the ADRA global network, while adapting to
the reality and the context in which we operate to better realize sustainable and positive change in our
community programs.
In a welcoming atmosphere marked by the deepest respect for those women and men, girls and boys, we
are committed, in partnership with our donors, to promote a community process, collective and quality
improvement of life. ADRA works in favor of all persons requiring the need for individuals most
vulnerable such as women, children and youth, refugees, IDPs and returnees in order to improve their
wellbeing, regardless of their ethnicity, their political or religious affiliation while preserving the dignity
of all persons.
In DRC, ADRA has five areas of intervention through which the communities are supported: primary
health care ( including nutrition, water, sanitation, prevention of disease, epidemic response, health
education, vaccination, child and mother health, family planning and HIV-AIDS program…), Basic
Education, Economic Development, Food Security and Response to Disasters and Catastrophes. The
HIV-AIDS program is included in all sectors l a crosscutting theme.
ADRA has been working in DRC since 1982 in 11 provinces (Kinshasa, Bas- Congo, Equateur, Kassai-
Occidental, Kassai- Oriental, Katanga, Province-Orientale, Nord-Kivu and Sud-Kivu). With these number
of years, ADRA has built experience with the communities in DRC through several programs
implemented in various sectors. In human resource capacities, ADRA has a big team of more than 279
experienced staff working with the communities in both emergency and development programs. Our
staffs are experimented in the analysis, design, internal control, implementing, monitoring and evaluation
of programs. The administrative and managerial team includes the Country Director, Country Finance
Director, Associate Directors, Program director, program assistants and accountants.
The ADRA program in DRC is based on the enhancing the capacity of communities and improving their
life conditions in order to create a positive change. Our strategic action is summarized in the following
points:
- Actively support communities in need through a variety of development activities planned and
implemented in a spirit of collaboration;
- Provide assistance in the event of disaster or state of chronic need and work with those who are
affected to find long-term solutions and resilience;
- Work through equitable partnerships with those in need to achieve within communities a positive
and lasting change;
- Promote and expand the integration and participation of women and other vulnerable groups in
the development process;
ADRA DRC 3| page
- Supporting and assisting communities to develop their capacity to maintain and manage the
natural resources and environment by integrating responsible governance practices in our
programs.
For the last 5 years to-date, ADRA DRC has worked with WHO, UNICEF, UNDP, Pooled Fund, WFP,
UNHCR, World Bank, USAID, EU, DANIDA, and ADRA international. ADRA share the same vision
for DRC with all donors we have partnered with and the government of DRC through their Ministries.
One of the roles of ADRA in DRC is to support country regarding her National Sanitary Development
Policy which is integrated in all intervention sectors. This policy is also in line with the Sustainable
Development Goals (SDGs).
ADRA also has extensive experience managing large and complex programs in DRC. In projects such as
JENGA II, ADRA’s flagship USAID/FFP project in DRC, ADRA leads a consortium of international
organizations, oversees implementation across the entire project area and ensures technical quality using a
similar coordination and leadership mechanism.
Primary health care
ADRA has set an overall target in accordance with the objective of the Humanitarian Action Plan, and
National Policy, and also the SDG objectives to reduce as far as possible, the morbidity and mortality
associated with various communicable or non-communicable diseases affecting the communities in DRC
and to improve coverage/ access and quality of health services to all people;
ADRA works in partnership with United Nations agencies (WHO, UNICEF, WFP ...) and state
departments of the Ministry of Health of the DRC (Health Zones, and Provincial Health Divisions).
Strategic Approach Our approach to achieving the goals is through the training of medical staff, prevention campaigns,
response to epidemics (measles, cholera), the supply of essential drugs and medical devices in basic
health facilities, supply of inputs and nutritional food in nutritional therapy units (UNS, UNTI, UNTA)
for support, sensitization of communities about nutrition, family planning, prevention of HIV/AIDS.
ADRA builds capacity of health workers in the context of a transfer of responsibility to the community
and promote community ownership as a sustainability strategy.
In this sector, ADRA focuses on a few sub-sectors or specific components. The choice of these sub-
sectors is explained by the context and Country priorities in health care.
Responses to epidemics (cholera, measles ...etc.)
Nutrition support for children with moderate and severe acute malnutrition
Education on health and nutrition
Supports medical expense of vulnerable people.
Access to Water and adequate Sanitation and Hygiene
Mother and child health ( Rehabilitation of maternity and pediatric departments)
Construction of Health Centers
Prevention of HIV-AIDS
Following are some of ADRA DRC’s experience in health projects(Health Sector):
ADRA DRC 4| page
- Emergency response against measles for children and emergency child care measles
immunization in 38 health zones in four provinces (Bandundu, Bas-Congo, North Kivu and
Equateur), more than 915,819 children vaccinated against measles between 2012 and early 2013.
- Projects of emergency Support to the monitoring and response to the epidemic of Cholera in
health areas of Mbandaka, Wangata, Kitona and Muanda. 130 service providers trained, 176
Community relays formed, 75 communities sensitized, 9 medical kits and pre protection materials
positioned, 7 health zones reinforced their active Community epidemiologic monitoring systems,
8 blocks of latrines, and 1.087.179 people sensitized.
- Support to primary health care emergency in the territory of Kungu Libenge and Bomongo,
Equateur province or 3015 returned were supported.
- Support for the management of severely malnourished children in the areas of health of Bokungu
and Ikela, territory of Bokungu. 476 severely malnourished children are admitted into the
program UNTI / UNTA. (Equateur province 2013).
Support to management of severely malnourished
children in 7 Health zones (Malemba Nkulu, Mulongo,
Lwamba, Kinkondja, Fungurume, Lubudi and Dilala)
supported by Food for Peace/USAID and Ehnacing of
Young and Infant Feeding Promotion in 9 health zones
(Malemba Nkulu, Mulongo, Lwamba, Kinkondja,
Fungurume, Lubudi, Dilala, Manika and Lualaba) in
Katanga province.
Ongoing Project, funded by UNICEF. 6000 severely
malnourished Children will be supported. In this project
we would like to augment the proportion of children, new
born and the family who have access to best quality of
curative, preventive and promotional intervention with
high health impact including the Prevention of mother-to-
child transmission of HIV, nutrition, and water
sanitation.
A similar project was implemented in Pweto and Kilwa in Katanga province in 2015 with support of
WFP ‘’ Support to manage moderately malnourished’’.
- Emergency Support against measles epidemic in the health Zones of Dilala and Lubudi Katanga
province. 185,728 children of 6 months to 15 years vaccinated, 1,226 medical staff trained and
378,962 people sensitized.

ADRA DRC 5| page
Food Support to people living with HIV in the health Zones of Kampemba, Kisanga,
Tshamilemba and Kipushi in Lubumbashi. Project funding by WFP in 2015. 1,821 People
living with HIV assisted with food, 32 medical staff trained and 16 structures supplied
with CSB+ and oil.
- About Water Hygiene and Sanitation: ADRA has implemented several projects in the Water,
Sanitation and Hygiene (WASH) sector through emergency and development projects in order to
supply emergency drinking water in areas affected by epidemics and waterborne diseases; These
projects included drillings of wells, rehabilitation of water sources/points, and building latrines in
the communities and in the schools. Through these projects, several thousands of people had
access to safe drinking water and quality hygienic installations. In these projects, we designed
activities that enhanced community ownership through active community participation in the
project activities and the training of communities in the management of hygiene infrastructures
and promotion of hygiene best
practices.
For example:
- Emergency support Wash with the fight against
the Cholera epidemic in the health zone of
Lilanga Bobangi, province of Ecuador (Project
on-going).
- Water sources constructed at Mbanza Muanda,
construction of a water reservoir for water supply,
6 fountains built and equipped.
- Wash emergency response in favor of Central
African refugees and their host families. Funded
in 2013-2014 by Pooled Fund. 108 people trained
on management of public sewing, 17 pump
remedial technicians trained, 150 community
workers trained, 15 boreholes drilled and installed
with VERGNET pump, 6 water points, 31
latrines, 400 San Plat and 11 incinerators built.
More than 160.000 people have access to water
and sanitation in this area of project.

ADRA DRC 6| page
Basic education
In order to improve access to basic education and the quality of education in the Democratic Republic of
Congo, ADRA has developed partnerships with donors for the construction and rehabilitation of school
quality across the country. These rehabilitation projects and school construction quality enable many child
of school age to access quality education in the best conditions. Our partners and donors in this sector are
in the majority of cases the World Bank through the BCECO the DRC, the SOCIAL FUND, as well as
other donors such as the UNICEF, ADRA International, and also with our own funds.
Strategic Approach Partnerships are to rehabilitate and or build classrooms, latrines, offices and equip these schools in the
ADRA DRC 7| page
standards. To achieve quality results pending the goals, we recommend the following strategies:
The use of local labor is important itself recipient (indirect).
Mobilization of resources available at local level to minimize the cost related to logistics.
Capacity management committee works within communities (community leaders)
Establishment of infrastructure management committees.
Formation of Land Management committees and organization of review meetings.
Since 2008, ADRA has built and rehabilitated more than 20 schools in the 6 provinces of the DRC and
has helped several children of school age to have access to quality education. Currently ADRA is
managing the construction of Kibabi School in Masisi funded by World Bank through Fond Social RDC.
Food security
The Democratic Republic of Congo is full of natural resources with a huge chunk of very fertile soil.
Though with these endowment of natural resources or privileges, the country is plunged into situation of
food insecurity in the rating of the IPC (Integrated food security Phase Classification 2013). The main
reason is probably the climate of insecurity in the country for several consecutive years of armed conflict.
ADRA work in food security sector in order to provide food and agricultural assistance to households
affected by malnutrition, to restore their livelihood / agricultural production (food market gardening), feed
vulnerable families and all communities. ADRA’s capacity building activities also include helping
smallholder farmers reduce food insecurity, with new techniques readily adopted and a high appreciation
for the new varieties introduced. ADRA DRC integrates agriculture and nutrition programming through
the introduction of new farming technologies and new crops such as soya, as well as, through the
provision of training in food processing, storage and utilization. ADRA has implemented projects in this
sector and helped communities affected by malnutrition, improve their food supply in terms of quantity,
quality and diversity.
Strategic Approach The approach used is that of the communities to prevent malnutrition and not falling into a situation of
food insecurity:
The distribution of agricultural inputs and tools as well as parents cunicoles for small livestock.
Vulnerable people are the target (Household from mining areas during installation and specific
populations in situations of extreme vulnerability (widows headed households, people living with
HIV/ AIDS, VSV, etc.) were also targets.
Organize awareness sessions on nutrition and good food hygiene practices.
Strengthen the capacity of farmers and associations of farmers to improve agricultural techniques
and farms.
Consolidate farmers and breeders association.
Following are some projects implemented and some ongoing:
ADRA DRC 8| page
- In the territory of Dimbelenge specifically in the health Zone and Katende Muetshi in Western
Kasai, communities received agricultural inputs and tools as well as parents cunicoles for small
livestock. Vulnerable people were targeted to reduce the risk of food insecurity in this
community. Households from the mining areas during installation and specific population in
extremely vulnerable position (widows headed households, people living with HIV AIDS, VVS,
etc.) were also targeted. 1,400 households received input kits for food crop and vegetable
gardening (1 kit of 10 kg of the seeds of quality of corn, 10 kgs of quality cowpea seed, 1 hoe
and 1 machete); 1200 ha of land cultivated for food crops; 1400 households were trained in
agricultural techniques and food market gardening. In the field of the livestock breeding,
100 households received cunicoles kits Intrants for the breeding; 100 households received
training on cunicoles breeding. Pooled Fund 2011-2012.
- Support Project for empowering of farmers in the Pangi and Kalima Zone, Maniema
Province. This project involved identification and selection of 2500 vulnerable households
within associations of civil society in 10 localities, training 2500 households on agricultural and
Fishpond technics, distribute 250 agricultural and startup Kits to the associations, position 10
popular saving bank, cultivate 50 hectares for the production of rice and corn, rehabilitation of the
infrastructures, sensitization of household about the activities of this project and other thematic
areas such as HIV-AIDS, Gender, environmental protection… The project is funded by EU
(2014-216). This is an on-going Project.
- JENGA I: The USAID/FFP multi-year program served over 45,000 people in Fizi and Uvira
territories in South Kivu Province, Eastern DRC. The package of program interventions was
implemented in 100 rural communities, benefitting 45,000 people (approximately 7,500
households) with 4,500 households/27,000 individuals from Fizi territory , while 3,000
households/18,000 individuals from Uvira territory. The overall goal of this Multi Year
Assistance Program (MYAP) in DRC was to reduce food insecurity among vulnerable
populations in Fizi and Uvira territories, focusing on female-headed households and returnees.
The three key strategic objectives ADRA achieved were: [1] increased crop production; [2]
increased livelihood options; and [3] improved health and nutrition status among women and
children under 5.
ADRA also incorporated several cross-cutting themes, including women’s empowerment and
gender-sensitive training; capacity building at all levels, including communities, NGOs and
government; and trust-building opportunities for community members. Through the program,
ADRA also promoted transition from relief to development within the target communities,
utilizing participatory methodologies and encouraging appropriate natural resource management
to protect and enhance human capabilities, livelihood capacities and community resiliency, while
creating greater community capacity to influence major factors affecting food security.
- JENGA JAMA II (JENGA II): The five year program began in July 2011 and is being
implemented by ADRA and its partners in Eastern Democratic Republic of the Congo (EDRC).
JENGA II is a follow-on project to JENGA I, which was implemented in 2008-2010. The overall
goal of JENGA II is to sustainably reduce food insecurity among vulnerable households in Fizi,
Uvira, and Kalehe territories of South Kivu Province, in the Democratic Republic of the Congo
(DRC). JENGA II aims to reach over 150,000 individuals during the life of the project.
JENGA II, which utilizes a gender-sensitive programming approach, works to increase incomes
for food insecure farming households; improve health and nutritional status of children under 5;

ADRA DRC 9| page
and increase women’s socio-economic empowerment in food insecure communities; and
strengthen community resilience to food security shocks.
In relation with the approaches for increasing the incomes for food insecure farming
households, JENGA II interventions have allowed farmers to adopt appropriate business
management skills; access joint storage and processing facilities; increase economies of scale and
bargaining power; and improve access to a variety of buyers and input suppliers, resulting in
greater returns for farmers with impacts in food security and nutrition. Experience has shown that
increased production is crucial, but the increase alone is not sufficient in solving poverty and food
insecurity for smallholder farmers. Demand-driven production is mandatory in most cases and
requires a new skill set for many farmers.
JENGA II uses two complementary approaches to commercialize smallholder farmers: the
smallholder extension model, which combines the Farmer Field School (FFS) and Farmer-to-
Farmer (F2F) approaches to reach farmers through training and dissemination of information on
agriculture production, marketing, and natural resources management; and the Farmer Business
Association (FBA), combined with the Agricultural Collecting Center (ACC) approach, which
provides opportunities for smallholder farmers to enhance their market position through larger
economies of scale, improved processing, and product value.
ADRA DRC 10| page
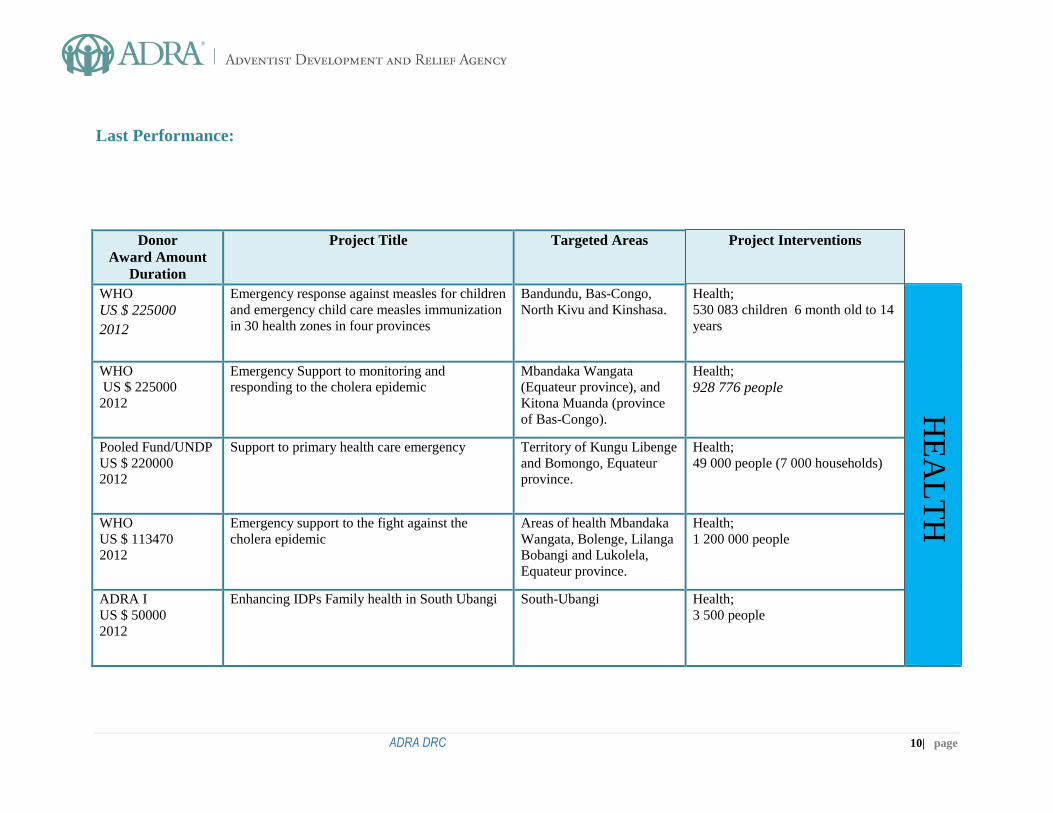
Last Performance:
Donor
Award Amount
Duration
Project Title Targeted Areas Project Interventions
WHO
US $ 225000
2012
Emergency response against measles for children
and emergency child care measles immunization
in 30 health zones in four provinces
Bandundu, Bas-Congo,
North Kivu and Kinshasa. Health;
530 083 children 6 month old to 14
years
HE
AL
TH
WHO
US $ 225000
2012
Emergency Support to monitoring and
responding to the cholera epidemic
Mbandaka Wangata
(Equateur province), and
Kitona Muanda (province
of Bas-Congo).
Health;
928 776 people
Pooled Fund/UNDP
US $ 220000
2012
Support to primary health care emergency Territory of Kungu Libenge
and Bomongo, Equateur
province.
Health;
49 000 people (7 000 households)
WHO
US $ 113470
2012
Emergency support to the fight against the
cholera epidemic
Areas of health Mbandaka
Wangata, Bolenge, Lilanga
Bobangi and Lukolela,
Equateur province.
Health;
1 200 000 people
ADRA I
US $ 50000
2012
Enhancing IDPs Family health in South Ubangi
South-Ubangi Health;
3 500 people
ADRA DRC 11| page
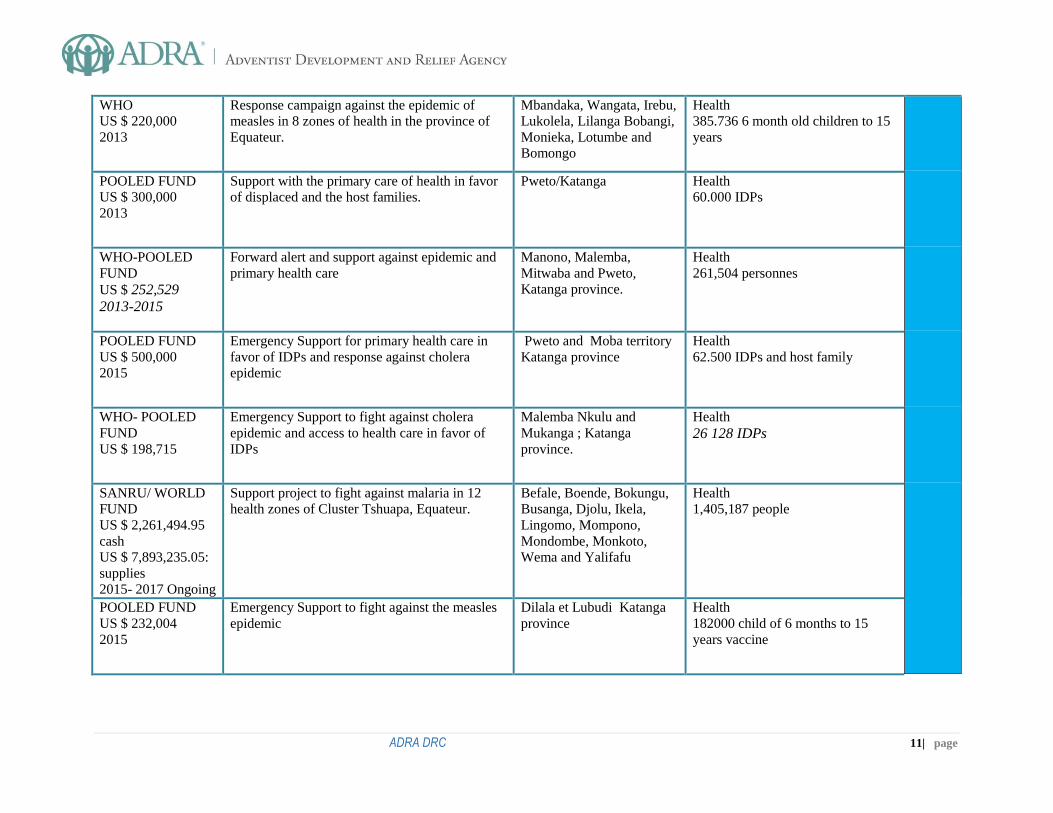
WHO
US $ 220,000
2013
Response campaign against the epidemic of
measles in 8 zones of health in the province of
Equateur.
Mbandaka, Wangata, Irebu,
Lukolela, Lilanga Bobangi,
Monieka, Lotumbe and
Bomongo
Health
385.736 6 month old children to 15
years
POOLED FUND
US $ 300,000
2013
Support with the primary care of health in favor
of displaced and the host families.
Pweto/Katanga Health
60.000 IDPs
WHO-POOLED
FUND
US $ 252,529
2013-2015
Forward alert and support against epidemic and
primary health care
Manono, Malemba,
Mitwaba and Pweto,
Katanga province.
Health
261,504 personnes
POOLED FUND
US $ 500,000
2015
Emergency Support for primary health care in
favor of IDPs and response against cholera
epidemic
Pweto and Moba territory
Katanga province
Health
62.500 IDPs and host family
WHO- POOLED
FUND
US $ 198,715
Emergency Support to fight against cholera
epidemic and access to health care in favor of
IDPs
Malemba Nkulu and
Mukanga ; Katanga
province.
Health
26 128 IDPs
SANRU/ WORLD
FUND
US $ 2,261,494.95
cash
US $ 7,893,235.05:
supplies
2015- 2017 Ongoing
Support project to fight against malaria in 12
health zones of Cluster Tshuapa, Equateur.
Befale, Boende, Bokungu,
Busanga, Djolu, Ikela,
Lingomo, Mompono,
Mondombe, Monkoto,
Wema and Yalifafu
Health
1,405,187 people
POOLED FUND
US $ 232,004
2015
Emergency Support to fight against the measles
epidemic
Dilala et Lubudi Katanga
province
Health
182000 child of 6 months to 15
years vaccine
ADRA DRC 12| page
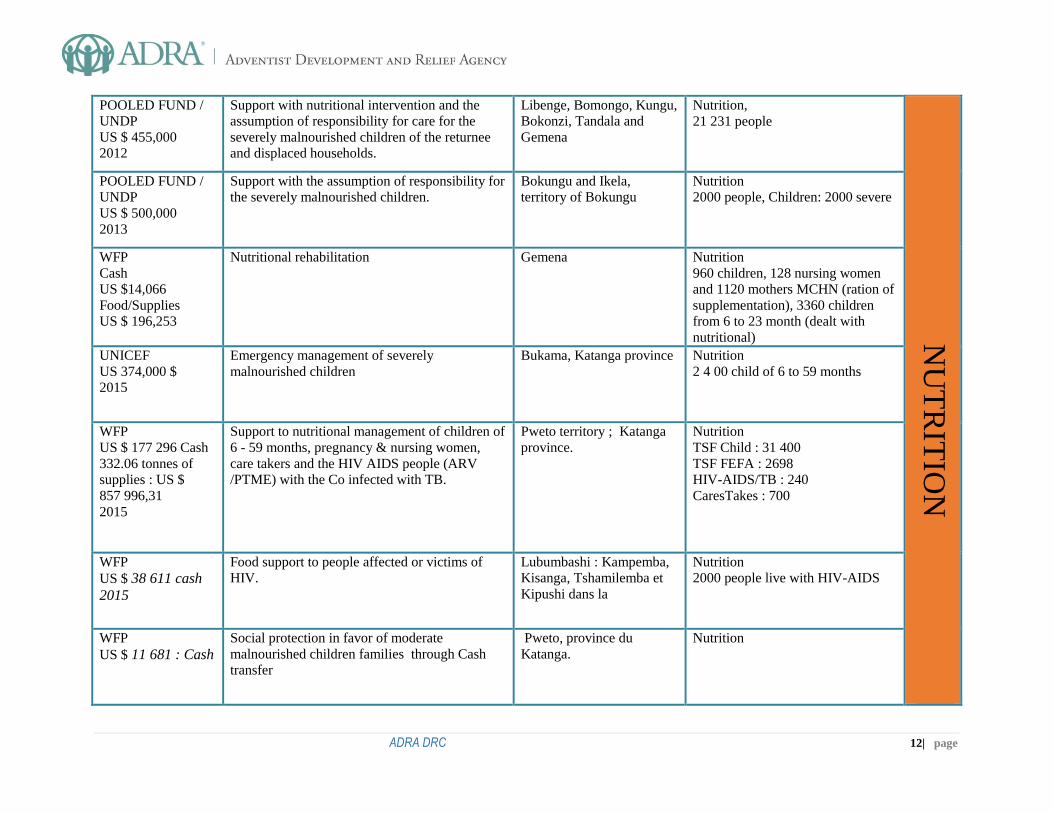
POOLED FUND /
UNDP
US $ 455,000
2012
Support with nutritional intervention and the
assumption of responsibility for care for the
severely malnourished children of the returnee
and displaced households.
Libenge, Bomongo, Kungu,
Bokonzi, Tandala and
Gemena
Nutrition,
21 231 people
NU
TR
ITIO
N
POOLED FUND /
UNDP
US $ 500,000
2013
Support with the assumption of responsibility for
the severely malnourished children.
Bokungu and Ikela,
territory of Bokungu
Nutrition
2000 people, Children: 2000 severe
WFP
Cash
US $14,066
Food/Supplies
US $ 196,253
Nutritional rehabilitation Gemena Nutrition
960 children, 128 nursing women
and 1120 mothers MCHN (ration of
supplementation), 3360 children
from 6 to 23 month (dealt with
nutritional)
UNICEF
US 374,000 $
2015
Emergency management of severely
malnourished children
Bukama, Katanga province Nutrition
2 4 00 child of 6 to 59 months
WFP
US $ 177 296 Cash
332.06 tonnes of
supplies : US $
857 996,31
2015
Support to nutritional management of children of
6 - 59 months, pregnancy & nursing women,
care takers and the HIV AIDS people (ARV
/PTME) with the Co infected with TB.
Pweto territory ; Katanga
province.
Nutrition
TSF Child : 31 400
TSF FEFA : 2698
HIV-AIDS/TB : 240
CaresTakes : 700
WFP
US $ 38 611 cash
2015
Food support to people affected or victims of
HIV.
Lubumbashi : Kampemba,
Kisanga, Tshamilemba et
Kipushi dans la
Nutrition
2000 people live with HIV-AIDS
WFP
US $ 11 681 : Cash
Social protection in favor of moderate
malnourished children families through Cash
transfer
Pweto, province du
Katanga.
Nutrition
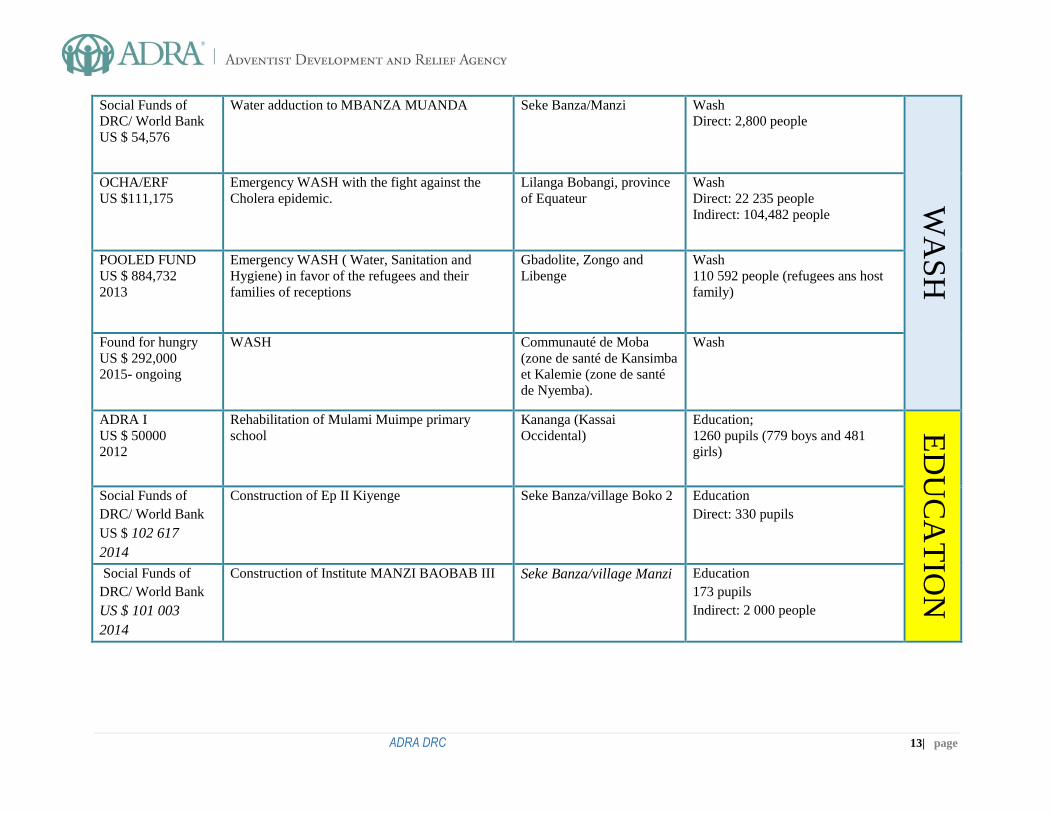
ADRA DRC 13| page
Social Funds of
DRC/ World Bank
US $ 54,576
Water adduction to MBANZA MUANDA Seke Banza/Manzi Wash
Direct: 2,800 people W
AS
H
OCHA/ERF
US $111,175
Emergency WASH with the fight against the
Cholera epidemic.
Lilanga Bobangi, province
of Equateur
Wash
Direct: 22 235 people
Indirect: 104,482 people
POOLED FUND
US $ 884,732
2013
Emergency WASH ( Water, Sanitation and
Hygiene) in favor of the refugees and their
families of receptions
Gbadolite, Zongo and
Libenge
Wash
110 592 people (refugees ans host
family)
Found for hungry
US $ 292,000
2015- ongoing
WASH Communauté de Moba
(zone de santé de Kansimba
et Kalemie (zone de santé
de Nyemba).
Wash
ADRA I
US $ 50000
2012
Rehabilitation of Mulami Muimpe primary
school
Kananga (Kassai
Occidental)
Education;
1260 pupils (779 boys and 481
girls)
ED
UC
AT
ION
Social Funds of
DRC/ World Bank
US $ 102 617
2014
Construction of Ep II Kiyenge Seke Banza/village Boko 2 Education
Direct: 330 pupils
Social Funds of
DRC/ World Bank
US $ 101 003
2014
Construction of Institute MANZI BAOBAB III Seke Banza/village Manzi Education
173 pupils
Indirect: 2 000 people
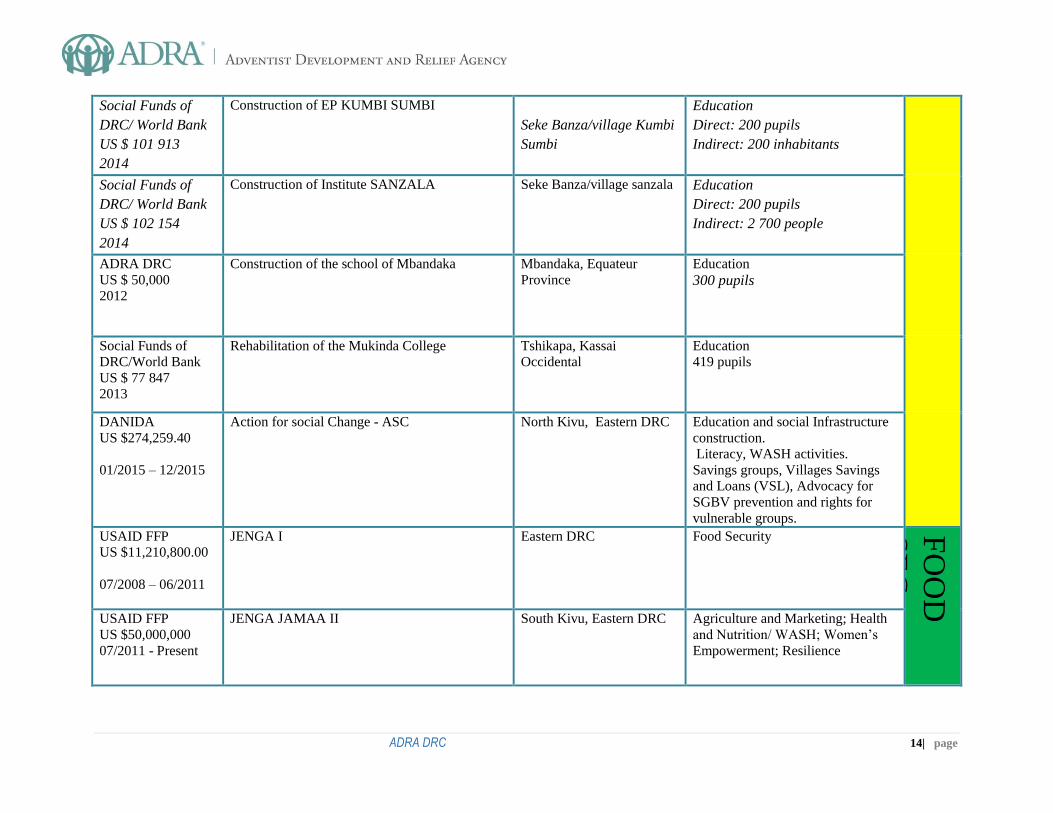
ADRA DRC 14| page
Social Funds of
DRC/ World Bank
US $ 101 913
2014
Construction of EP KUMBI SUMBI
Seke Banza/village Kumbi
Sumbi
Education
Direct: 200 pupils
Indirect: 200 inhabitants
Social Funds of
DRC/ World Bank
US $ 102 154
2014
Construction of Institute SANZALA
Seke Banza/village sanzala
Education
Direct: 200 pupils
Indirect: 2 700 people
ADRA DRC
US $ 50,000
2012
Construction of the school of Mbandaka Mbandaka, Equateur
Province
Education
300 pupils
Social Funds of
DRC/World Bank
US $ 77 847
2013
Rehabilitation of the Mukinda College Tshikapa, Kassai
Occidental
Education
419 pupils
DANIDA
US $274,259.40
01/2015 – 12/2015
Action for social Change - ASC North Kivu, Eastern DRC Education and social Infrastructure
construction.
Literacy, WASH activities.
Savings groups, Villages Savings
and Loans (VSL), Advocacy for
SGBV prevention and rights for
vulnerable groups.
USAID FFP
US $11,210,800.00
07/2008 – 06/2011
JENGA I Eastern DRC Food Security
FO
OD
SE
C
USAID FFP
US $50,000,000
07/2011 - Present
JENGA JAMAA II South Kivu, Eastern DRC Agriculture and Marketing; Health
and Nutrition/ WASH; Women’s
Empowerment; Resilience
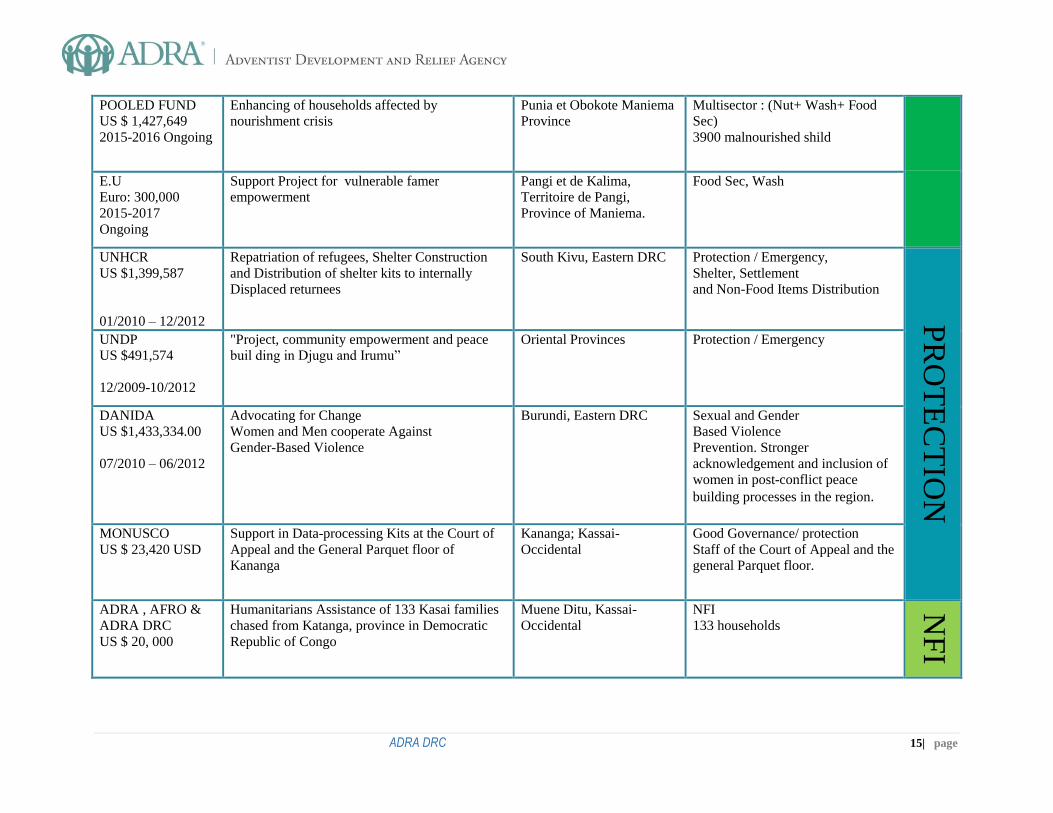
ADRA DRC 15| page
POOLED FUND
US $ 1,427,649
2015-2016 Ongoing
Enhancing of households affected by
nourishment crisis
Punia et Obokote Maniema
Province
Multisector : (Nut+ Wash+ Food
Sec)
3900 malnourished shild
E.U
Euro: 300,000
2015-2017
Ongoing
Support Project for vulnerable famer
empowerment
Pangi et de Kalima,
Territoire de Pangi,
Province of Maniema.
Food Sec, Wash
UNHCR
US $1,399,587
01/2010 – 12/2012
Repatriation of refugees, Shelter Construction
and Distribution of shelter kits to internally
Displaced returnees
South Kivu, Eastern DRC Protection / Emergency,
Shelter, Settlement
and Non-Food Items Distribution
PR
OT
EC
TIO
N
UNDP
US $491,574
12/2009-10/2012
"Project, community empowerment and peace
buil ding in Djugu and Irumu”
Oriental Provinces Protection / Emergency
DANIDA
US $1,433,334.00
07/2010 – 06/2012
Advocating for Change
Women and Men cooperate Against
Gender-Based Violence
Burundi, Eastern DRC Sexual and Gender
Based Violence
Prevention. Stronger
acknowledgement and inclusion of
women in post-conflict peace
building processes in the region.
MONUSCO
US $ 23,420 USD
Support in Data-processing Kits at the Court of
Appeal and the General Parquet floor of
Kananga
Kananga; Kassai-
Occidental
Good Governance/ protection
Staff of the Court of Appeal and the
general Parquet floor.
ADRA , AFRO &
ADRA DRC
US $ 20, 000
Humanitarians Assistance of 133 Kasai families
chased from Katanga, province in Democratic
Republic of Congo
Muene Ditu, Kassai-
Occidental
NFI
133 households
NF
I
ADRA DRC 16| page







