Download - Arriagada, r. breast cancer
Predictive factors of the effect of adjuvant systemic treatments in breast cancer
R. Arriagada 1-3 , S. Michiels 2
1 Karolinska Institutet and University Hospital, Stockholm, Sweden 2 Institut Gustave-Roussy
3 Université de Paris-Sud, France
Predictive factors of the effect of adjuvant systemic treatments
• Why only systemic treatments ?
• Hormonal receptors
• HER2
• Molecular classifications
• Genomics signatures
• Methodological considerations
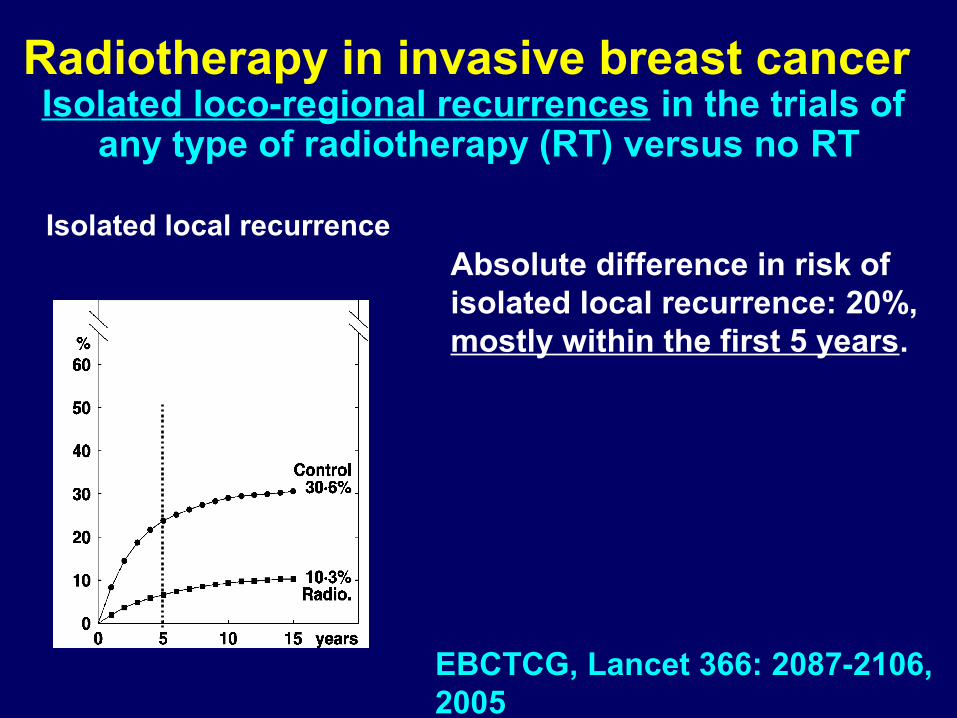
Radiotherapy in invasive breast cancer Isolated loco-regional recurrences in the trials of
any type of radiotherapy (RT) versus no RT
Isolated local recurrenceAbsolute difference in risk of isolated local recurrence: 20%, mostly within the first 5 years.
EBCTCG, Lancet 366: 2087-2106, 2005
Prognostic and predictive factors
• Prognostic factors: those that in multivariate
analysis show an independent effect on the
studied event
• May be studied in large retrospective series
• Predictive factors: those that are shown to be
significantly related to treatment effect
• They should be studied in large randomised
series testing the treatment (subgroup analysis),
or taking tumour response as event (advanced
disease or neo-adjuvant setting)
Hormonal receptors and hormonoresistance
• ER: good predictors but not enough
• Still about 50% of patients with ER+ are non-
responders
• About 10% of patients with ER- are responders
• ER and PR are not enough
• Others markers, pathways and cross-talks
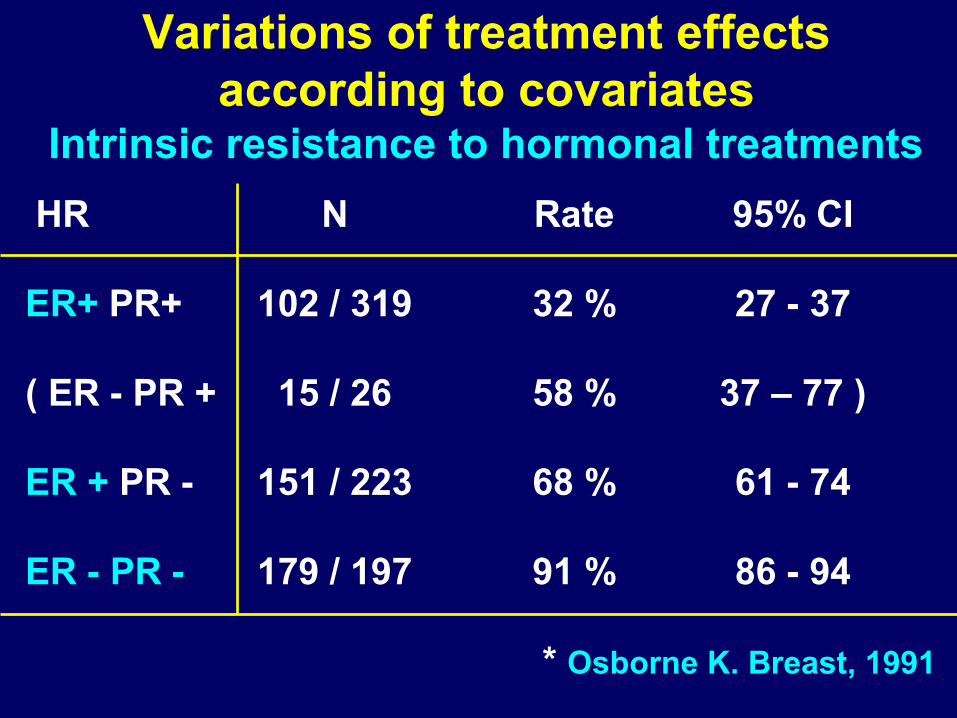
Variations of treatment effects according to covariates
Intrinsic resistance to hormonal treatments
HR N Rate 95% CI
ER+ PR+ 102 / 319 32 % 27 - 37
( ER - PR + 15 / 26 58 % 37 – 77 )
ER + PR - 151 / 223 68 % 61 - 74
ER - PR - 179 / 197 91 % 86 - 94
* Osborne K. Breast, 1991
Hormonoresistance breast cancerRationale
• Two-thirds of tumours have positive ER and/or PR
• ER good predictor of tumour response (50%), but
only a part of the puzzle
- ERα
- ERβ (Gustafsson et al)
- Other factors (EGFR / HER2 receptors)
- Crosstalk ER and GFR pathways
Hormonoresistance breast cancerRationale
• EGFR / HER2 pathway may play a role in
resistance to SERMs (e.g. tamoxifen)
• ER complex with other transcription factors (Fos
and Jun proteins), alter gene transcription (cyclyn
D, ILGF-1,…)
• P53 mutation: poor response to tamoxifen
HormonoresistanceTamoxifen: largely used for 30 years
Hormonoresistance
• Loss of ER expression
• Modification of expression oestrogen-related
genes such as those coding GF or GF receptors
• Altered expression of transcriptional cofactors
associated with ER α• Deterioration of ER α circulation
• Implication of ER β• Alterations of tamoxifen metabolism
• ……
HormonoresistanceTamoxifen: gold standard for 30 years
• Agonistic and antagonistic effects
• Prevents the binding of oestrogen to its receptor
• Intrinsic (50% of ER+) and acquired resistance
• Agonistic effect: increase some side effects
• Adjuvant use for 5 years (however, some patients
could benefit from a longer treatment)
• More accurate and selective predictive factors are
needed.
HormonoresistanceAnti-aromatase inhibitors (AIs)
• Exemestane, anastrazole, letrozole
• More effective than TAM in postmenopausal pts
• Optimal treatment and sequencing to be defined
• Adverse effects: joint disorders
• ER+, HER2+ : AIs ?
• ER+, PR+ : sequence of TAM and AIs ?
HormonoresistanceFulvestrant
• Steroidal ER antagonist with no agonist effect
• It binds, blocks and accelerates degradation of
ER protein
• As effective as anastrazole and tamoxifen in
advanced ER+ breast cancer
• Well tolerated
• Lacks cross-resistance with TAM and AIs
• Sequential regimens ?
HormonoresistanceAdditional predictive factors
• ERα + and PR+ only used for practical indications
• Functional genomics: subgroups of gene profile
(e.g. Paik et al)
• Proteomics: study complex protein mixtures with
high resolution, SELDI-TOF-MS and antibody
array (Linderholm et al): 5 new potential
biomarkers
HormonoresistancePractical implications of prediction
• Tumours resistant to TAM could be sensitive to
AIs and viceversa
• The same for the indication of Fulvestrant
• Definition of optimal sequencing (BIG 01-98)
• Knowledge about mechanisms of resistance: new
drugs or treatment of hormonal resistance
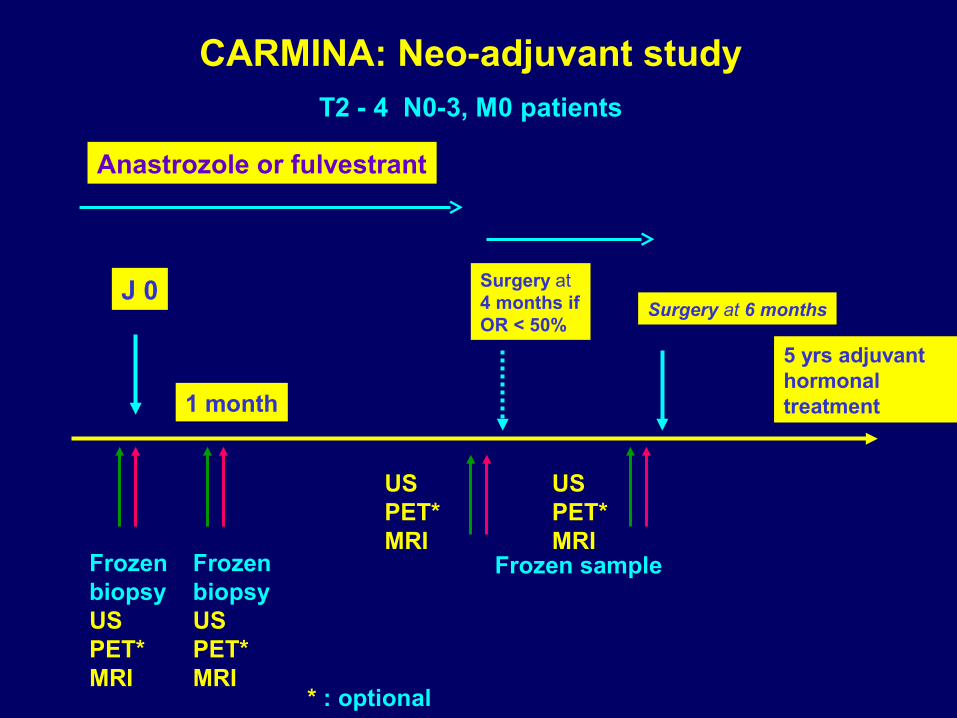
J 0
Frozen biopsyUSPET*MRI
Frozen biopsyUSPET*MRI
1 month
Surgery at 4 months if OR < 50%
Surgery at 6 months
Frozen sample
USPET*MRI
USPET*MRI
* : optional
CARMINA: Neo-adjuvant studyT2 - 4 N0-3, M0 patients
Anastrozole or fulvestrant
5 yrs adjuvant hormonal treatment
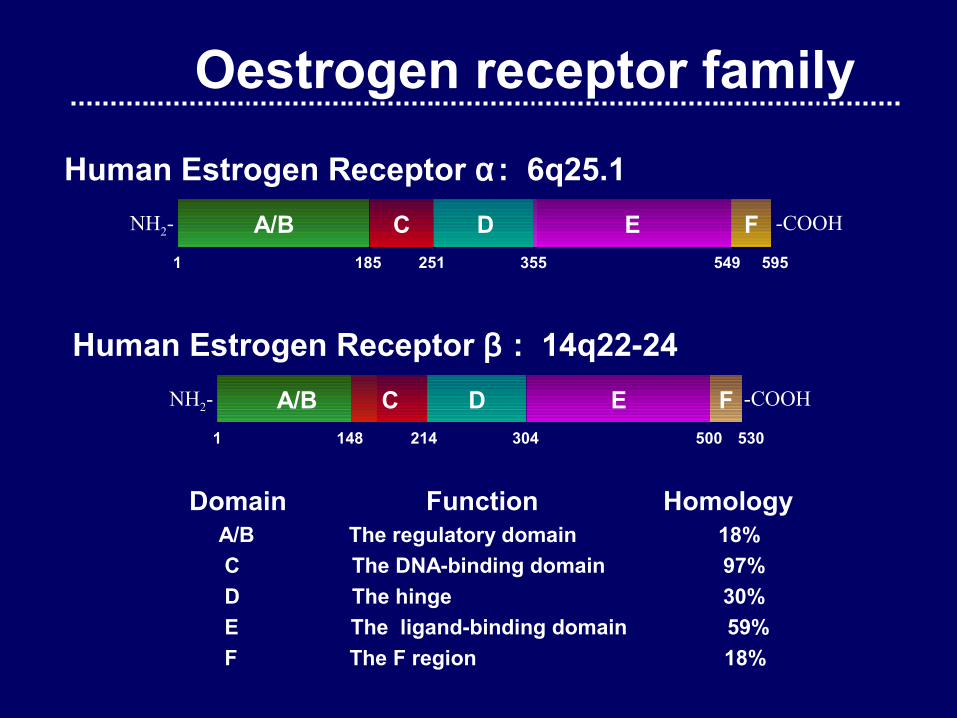
Domain Function Homology A/B The regulatory domain 18%
C The DNA-binding domain 97%
D The hinge 30%
E The ligand-binding domain 59%
F The F region 18%
Oestrogen receptor family
Human Estrogen Receptor α: 6q25.1
Human Estrogen Receptor β : 14q22-24
A/B C D E F -COOHNH2-
1 148 214 304 500 530
NH2- A/B C D E F -COOH
1 185 251 355 549 595
• In ductal cells of the mammary gland, ERα and ERβ oppose each other on proliferation
• The proliferative response to oestrogens is determined by the ratio of ERα / ERβ
• Functions of ERβ in the breast are probably related to both its anti-proliferative and its pro-differentiation functions
• Breast cancer in postmenopausal women: high expression of ERα (cancer cells and normal ducts) indicate a normal elevation of ERα in the absence of its ligand, estradiol
Oestrogen receptor family I
• ERα expression in normal postmenopausal breast is not elevated • ERβ expressed > 60% of breast epithelial cells • In some women, ERβ is not detected but the splice variant ERβ cx may be very abundant • Breast cancer sections showed that ERβ is lost
and ERα is gained as we go from normal tissue to cancer• A decreased level of ERβ mRNA may be associated with breast tumourigenesis• DNA methylation: important mechanism for ERβ gene silencing in breast cancer
Oestrogen receptor family II
Pharmacogenetic Tools (TAM)Efficacy
• Polymorphism of TAM metabolising genes : – CYP2D6 : TAM OH-Tam, N-desmethylTam ⇨ ⇨
4 OH-N-desmethylTam (endoxifen) • Antidepressant (selective serotonin re-uptake
inhibitors), currently used for hot flushes linked to TAM, are CYP2D6 inhibitors.
• Plasma concentration of Endoxifen ⇩ if CYP2D6 *4/*4 genotype or paroxetin use.
Goetz et al, 2005,2007; Jin et al, 2005; Borges et al, 2006; Wegman et al, 2007
• AGE• Hormonal receptors• HER2• Others ?
Adjuvant chemotherapy effectPredictive factors
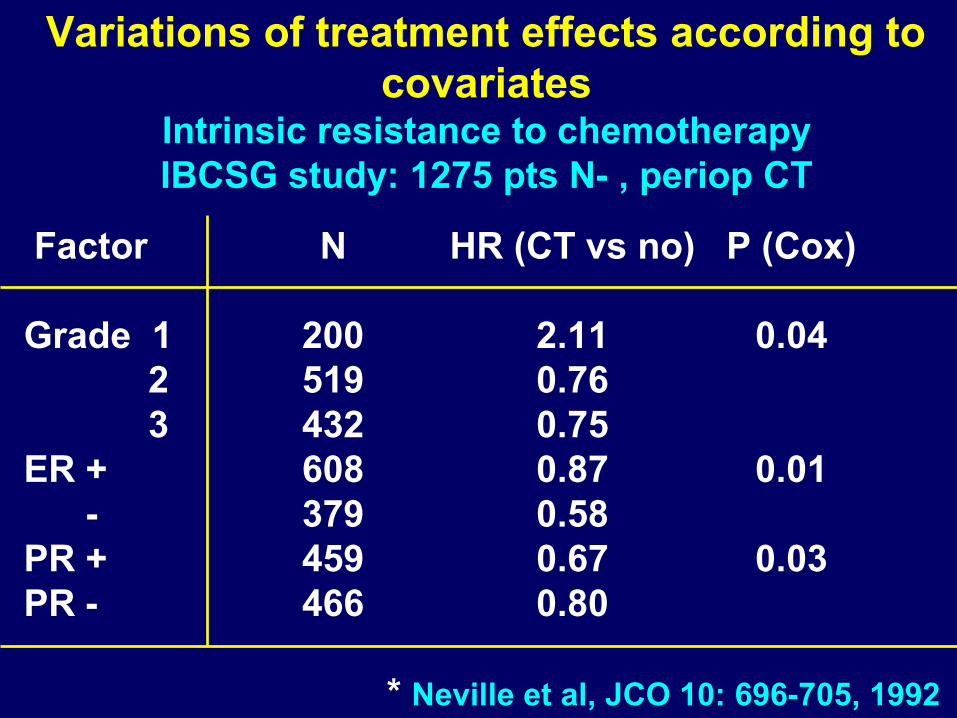
Variations of treatment effects according to covariates
Intrinsic resistance to chemotherapyIBCSG study: 1275 pts N- , periop CT
Factor N HR (CT vs no) P (Cox)
Grade 1 200 2.11 0.04 2 519 0.76 3 432 0.75ER + 608 0.87 0.01 - 379 0.58PR + 459 0.67 0.03PR - 466 0.80
* Neville et al, JCO 10: 696-705, 1992
Variations of treatment effects according to covariates
Adjuvant setting: Hormonal receptors
• In more recent randomised data, HR+ appears as a
marker of intrinsic chemoresistance:
♦ French studies *
♦ IBCSG IX study **
* Arriagada R et al. Ann Oncol, 13: 1378-86, 2002
Arriagada R et al. Acta Oncol, 44: 458-66, 2005
** IBCSG JNCI 94: 1054-1065, 2002
Variations of treatment effects according to covariates
Chemotherapy
• Drug type: anthracycline vs CMF-like
regimens (EBCTCG)
• Anthracycline dose: Belgian and French trials*
• Hormonal receptors: French study**
• Age (EBCTCG)
* Piccart M et al, JCO 19: 3103-10, 2001; Bonneterre J et al,
JCO 19: 602-11, 2001
** Arriagada R et al. Acta Oncol 44: 458-66, 2005
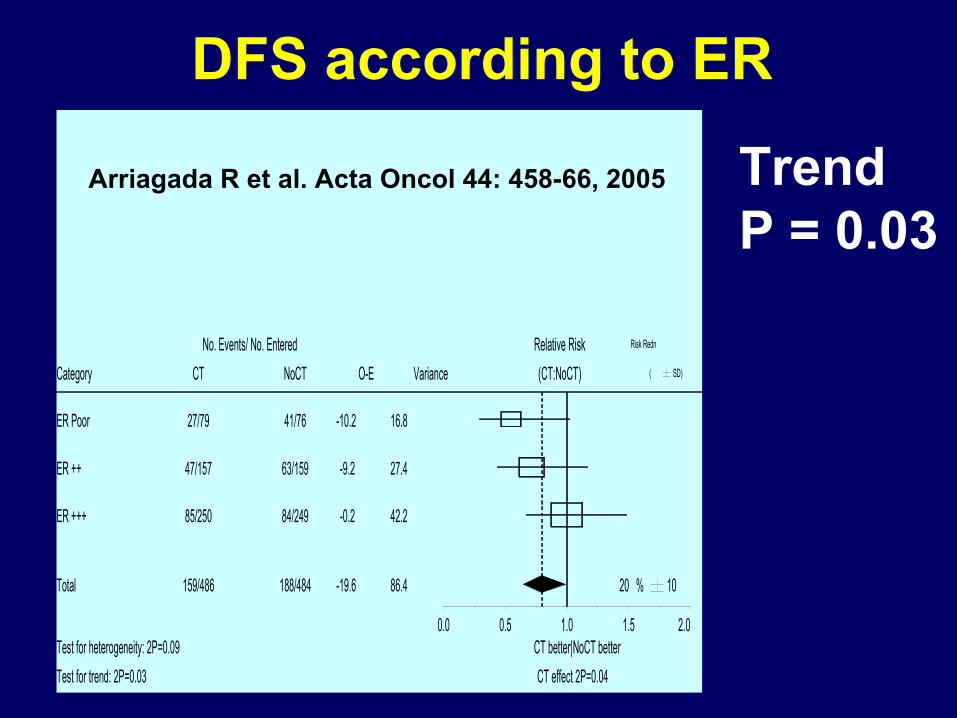
DFS according to ER
ER Poor 27/79 41/76 -10.2 16.8
ER ++ 47/157 63/159 -9.2 27.4
ER +++ 85/250 84/249 -0.2 42.2
Total 159/486 188/484 -19.6 86.4
Category CT NoCT O-E Variance (CT:NoCT) ( SD)
No. Events/ No. Entered Relative Risk Risk Redn
CT effect 2P=0.04
CT better|NoCT betterTest for heterogeneity: 2P=0.09
Test for trend: 2P=0.03
20 % 10
0.0 0.5 1.0 1.5 2.0
TrendP = 0.03
Arriagada R et al. Acta Oncol 44: 458-66, 2005
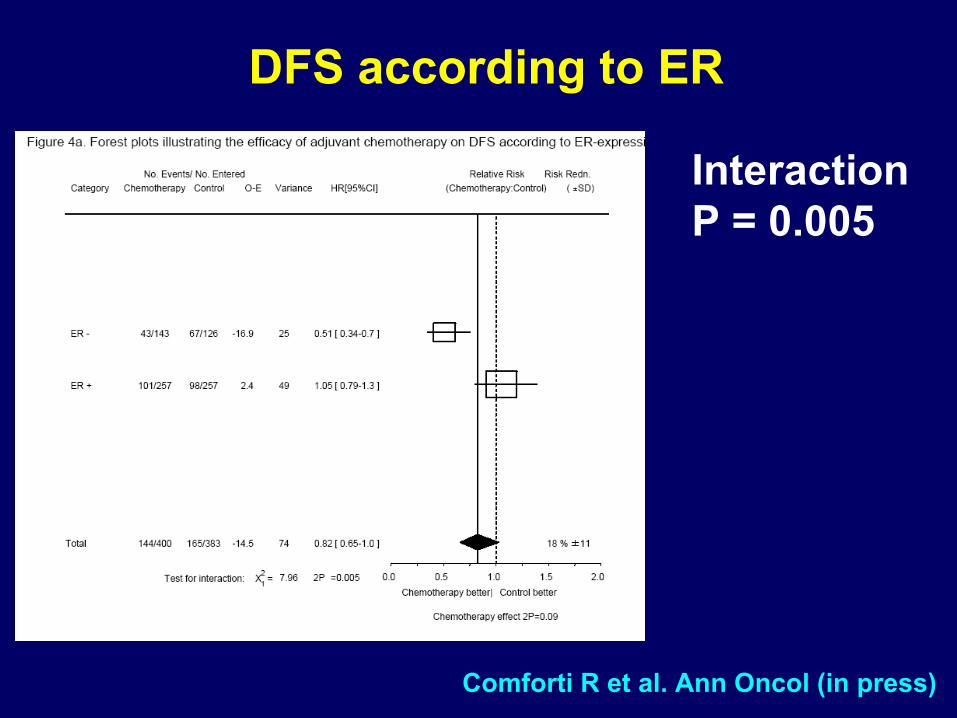
DFS according to ER
InteractionP = 0.005
Comforti R et al. Ann Oncol (in press)
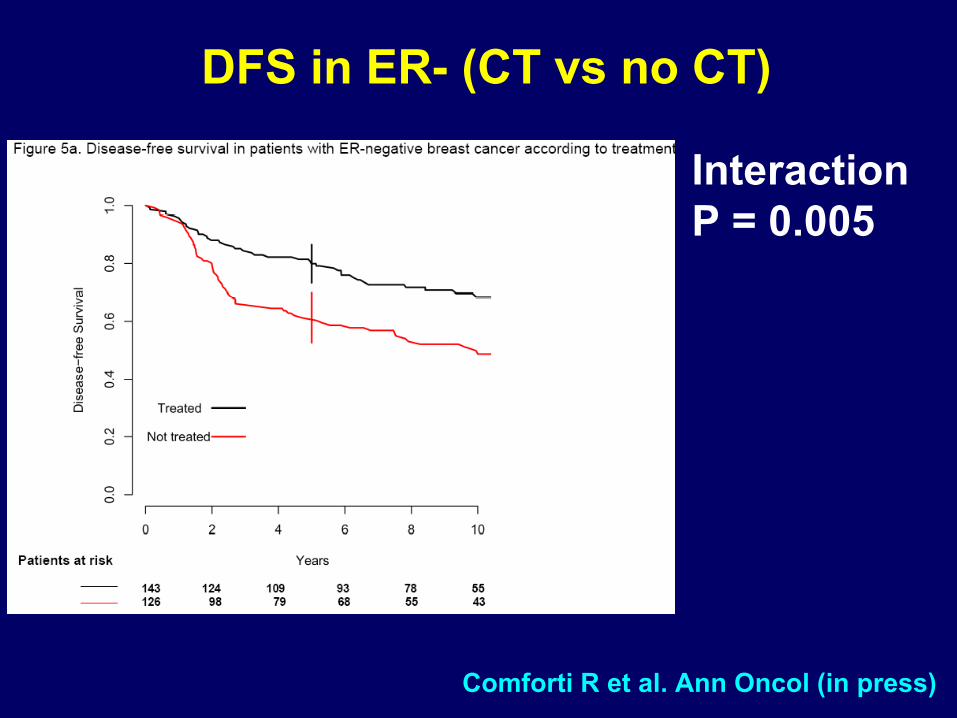
DFS in ER- (CT vs no CT)
InteractionP = 0.005
Comforti R et al. Ann Oncol (in press)
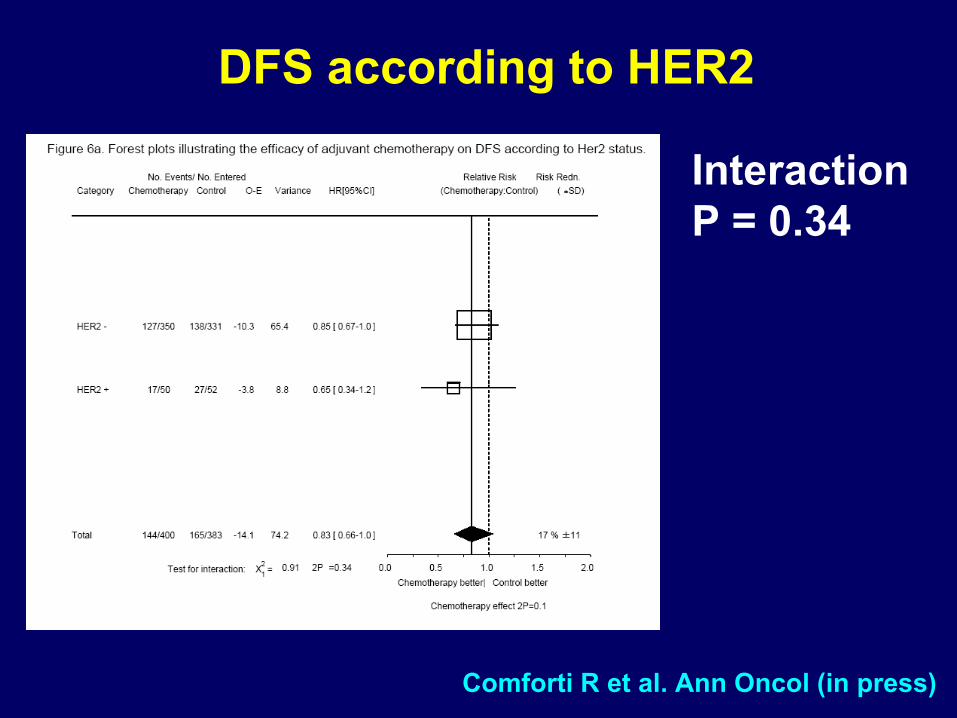
DFS according to HER2
InteractionP = 0.34
Comforti R et al. Ann Oncol (in press)
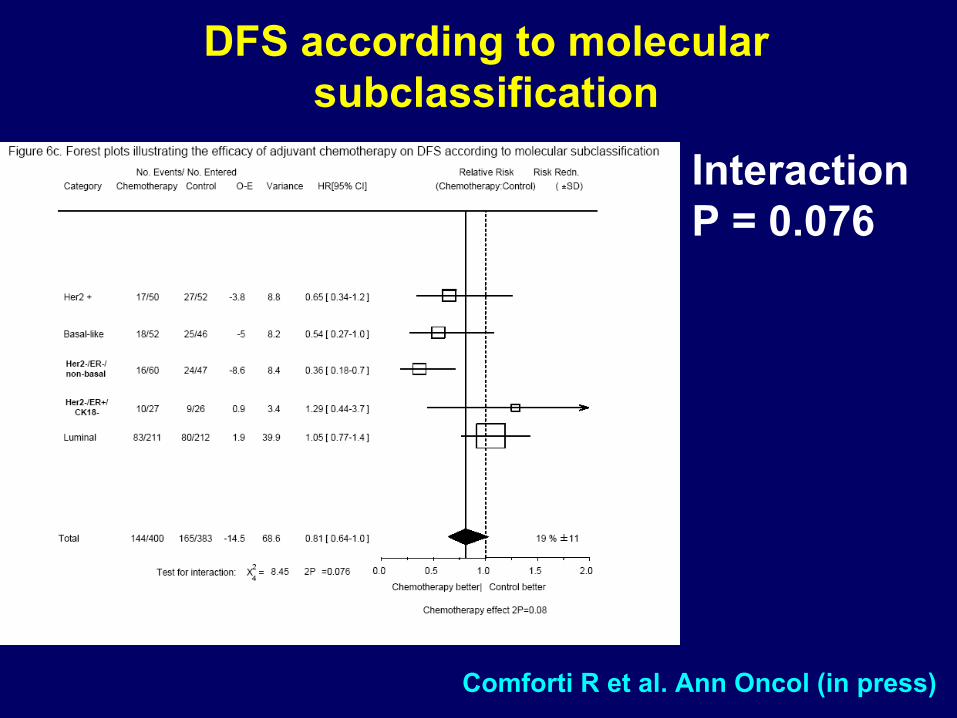
DFS according to molecular subclassification
InteractionP = 0.076
Comforti R et al. Ann Oncol (in press)
Overcoming drug resistanceDrug Doses
Lower doses of anthracyclines have a lower effect
than higher doses
1. CALGB *
2. Belgian trial **
3. French trial ***
4. Counterpart: AML ?
* Budman et al. JNCI 90: 1205-11, 1998** Piccart et al. JCO 19: 3103-10, 2001*** Bonneterre et al. JCO 19: 602-11, 2001**** Ann Oncol 14: 663-5, 2003
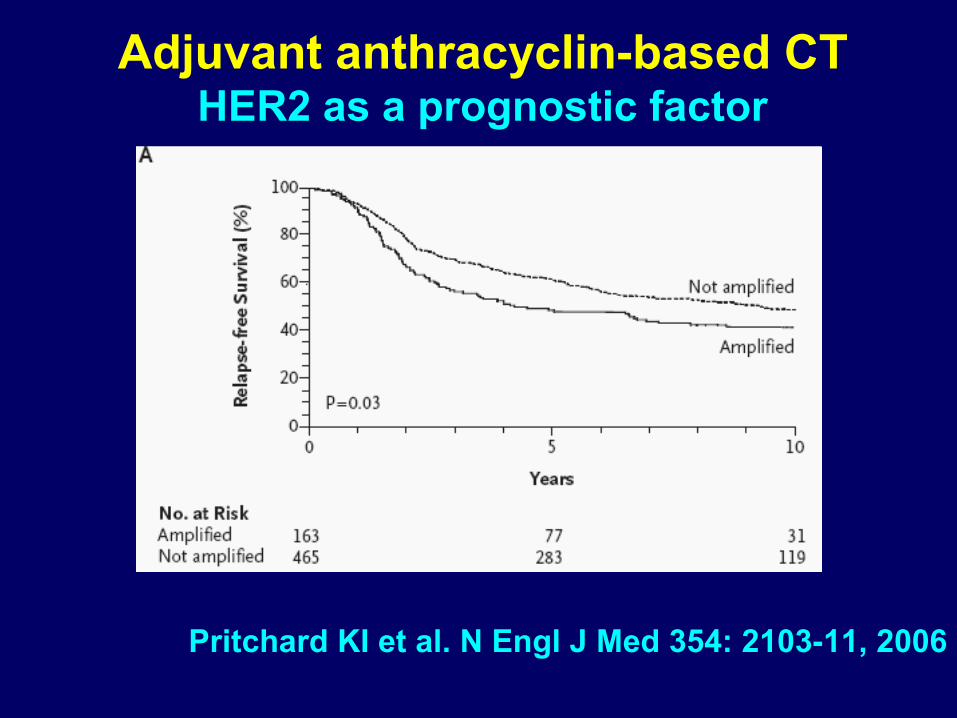
Adjuvant anthracyclin-based CTHER2 as a prognostic factor
Pritchard KI et al. N Engl J Med 354: 2103-11, 2006
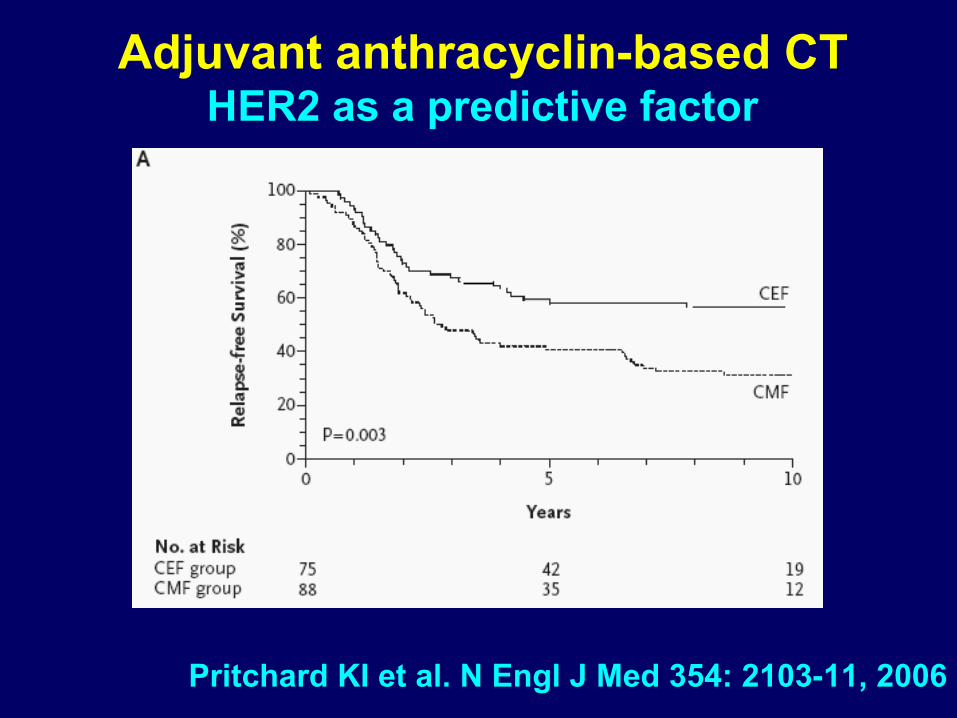
Adjuvant anthracyclin-based CTHER2 as a predictive factor
Pritchard KI et al. N Engl J Med 354: 2103-11, 2006
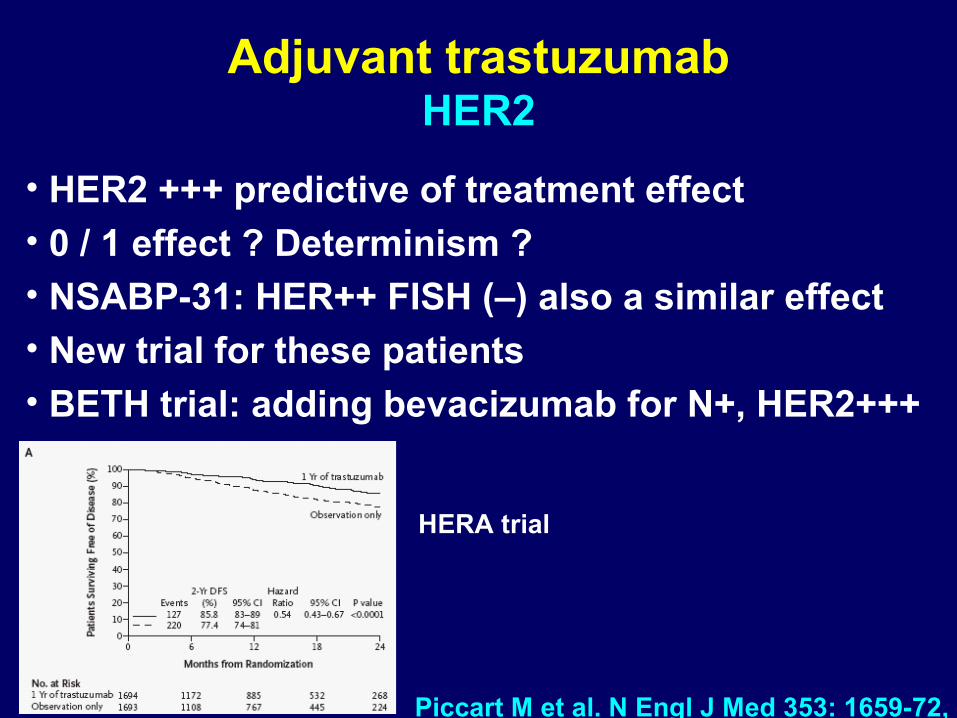
Adjuvant trastuzumabHER2
• HER2 +++ predictive of treatment effect• 0 / 1 effect ? Determinism ?• NSABP-31: HER++ FISH (–) also a similar effect• New trial for these patients• BETH trial: adding bevacizumab for N+, HER2+++
Piccart M et al. N Engl J Med 353: 1659-72, 2005
HERA trial
Definition of new predictive factors Genomics / Proteomics
1. Knowledge about the human genoma
2. Knowledge about functional genes
3. Investigation of gene expression: proteins
4. Technical facilities: Micro-arrays
1. Frozen tissues
2. Fresh tissues
These investigations will be introduced in
prospective randomised trials (e.g. MINDACT)
Definition of new predictive factors Genomics / Micro-arrays
1. Determination of 25,000 genes
2. Selection of a genetic profile (or signature)
based on 70 genes
3. Used in limited database and evaluated as a
prognostic factor *
4. The introduction in randomised trials will allow
to evaluate their predictive value
* van’t der Veer L et al. Nature, 2002
Van der Vijver M et al. NEJM, 2003
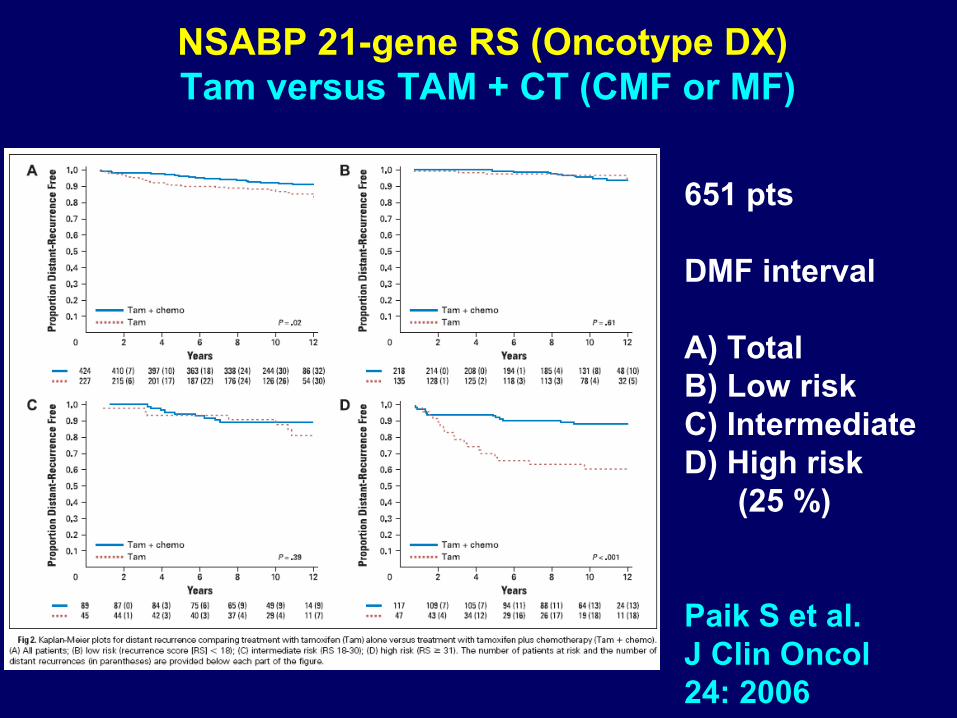
NSABP 21-gene RS (Oncotype DX) Tam versus TAM + CT (CMF or MF)
651 pts
DMF interval
A) TotalB) Low riskC) IntermediateD) High risk (25 %)
Paik S et al.J Clin Oncol24: 2006
Definition of new predictive factors BIG/TRANSBIG: Mindact
US Intergroup TAILORx trial
• Thousands of N- patients to be included
• Europe: Amsterdam signature
• US: Oncotype
• Randomising adjuvant CT and HT
• Expensive +++
• Feasibility ?
Prognostic signature challengesC. Sotiriou (Brussels)
• 10 – 20% discordance between labs• Molecular classification: suboptimal
reproducibility• Fine-tuning needed• Very small gene overlap• Some validations
• Most prognostic genes are markers of proliferation
Statistical challenges related to micro-chips
Hopes and false positive results
S. Michiels, S. Koscielny, T. Boulet, C. Hill
Biostatistics and Epidemiology Department
16 April 2007
Some issues
Molecular signature
• Limited number of genes defining patient groups• Predictive signature for a defined metastatic risk
assumes the existence of an unique genetic combination for this risk
The old story of numbers
• Analysed series with a small number of patients and thousands of covariates
• Statistical power issues, interpretation and results validation
Taille de l'échantillon d'apprentissage
Tau
x d
e m
auva
ises
cla
ssifi
catio
ns
20 40 60 80 100
0.2
0.3
0.4
0.5
0.6
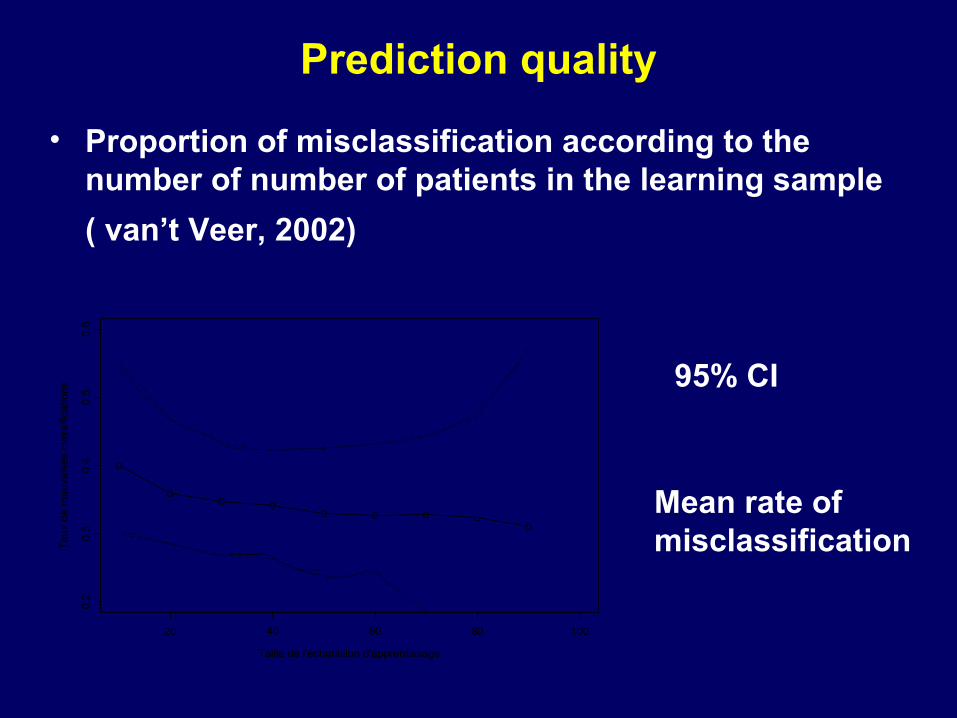
Prediction quality
95% CI
Mean rate of misclassification
• Proportion of misclassification according to the number of number of patients in the learning sample
( van’t Veer, 2002)
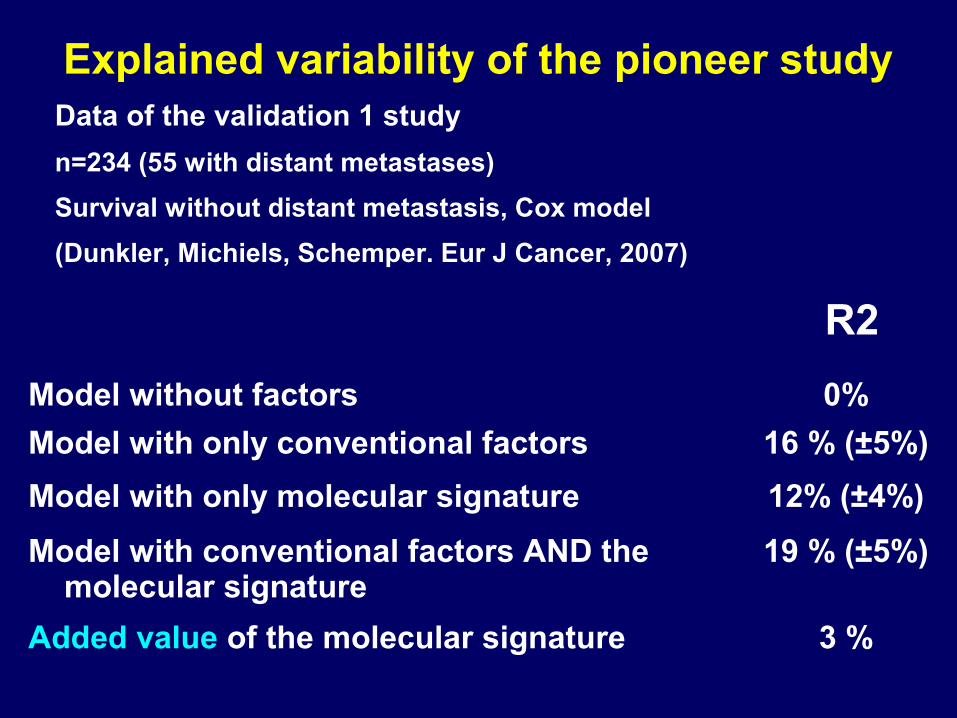
Data of the validation 1 study
n=234 (55 with distant metastases)
Survival without distant metastasis, Cox model
(Dunkler, Michiels, Schemper. Eur J Cancer, 2007)
Explained variability of the pioneer study
R2
Model without factors 0%
Model with only conventional factors 16 % (±5%)
Model with only molecular signature 12% (±4%)
Model with conventional factors AND the molecular signature
19 % (±5%)
Added value of the molecular signature 3 %
Predictive factors of the effect of systemic treatments Conclusions
• Useful predictive factors: HR, HER2• However, they explain only a part of the
variability• They give probabilities and are not
deterministic• Biomics signatures: Hopes and a large field of
research• Clinical application: only robust results







