
ATTENUATION OF THE PRESSOR RESPONSE TO LARYNGOSCOPY
AND ENDOTRACHEAL INTUBATION: A COMPARISON OF
INTRAVENOUS ESMOLOL AND LIDOCAINE.
A DISSERTATION
BY
DR AMENAGHAWON ANDREA EHIOZE-OSIFO
MBBS (LAGOS), DA (BENIN)
SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENT
FOR THE AWARD OF THE FELLOWSHIP OF THE FACULTY OF
ANAESTHESIA, NATIONAL POSTGRADUATE MEDICAL
COLLEGE OF NIGERIA.
NOVEMBER, 2008.
DECLARATION

2
I, AMENAGHAWON ANDREA EHIOZE-OSIFO, here declare that the contents of
this dissertation are the results of work done by me at the Lagos University Teaching
Hospital, Lagos, Nigeria. The work has not been presented for any publication,
examination or fellowship award.
………………………………………………
Dr A.A. Ehioze-Osifo
CERTIFICATION

3
We certify that this work was carried out by Dr Amenaghawon Andrea Ehioze-Osifo
of the Department of Anaesthesia, Lagos University Teaching Hospital, under our
supervision.
Signature/ Date………………………………………………
Dr O.T Kushimo
Associate professor/Consultant Anaesthetist
Department of Anaesthesia
Lagos University Teaching Hospital
Signature/ Date……………………………………………….
Dr J.O Olatosi
Lecturer/Consultant Anaesthetist
Department of Anaesthesia
Lagos University Teaching Hospital
DEDICATION
This work is dedicated to my loving family for their support, understanding and prayers
which saw me through the residency training.

4
AKNOWLEDGEMENTS
I thank the Almighty God for his grace and mercy to start and conclude this work.
I am sincerely grateful to my supervisors Dr O.T Kushimo and Dr J.O. Olatosi for their
unstinted patience, encouragement and intellectual contributions to this book.
I seize this opportunity to express my appreciation to the other consultants in the
Department of Anaesthesia of the Lagos University Teaching Hospital for their
immense contribution to my training.
I also wish to thank the following people for the roles they played during the conduct
of this study. My fellow residents for their support and co-operation in collecting the
data for this study as well as Dr Oridota of the Community Health Department, for his
help with the statistical analysis of this study.
I appreciate the support and encouragement of my parents, brothers and in-laws who
have been very supportive during this period.
To my dear husband, Ehioze and our beloved sons, Obosa and Osasu, I wish to say
thank you for your perseverance, encouragement and support.
TABLE OF CONTENTS

5
1. TITLE i
2. TABLE OF CONTENTS ii
3. DECLARATION iii
4. CERTIFICATION iv
5. DEDICATION v
6. ACKNOWLEDGEMENTS vi
7. LIST OF ABBREVIATIONS vii
8. LIST OF TABLES viii
9. LIST OF FIGURES ix
10. LIST OF APPENDICES x
11. SUMMARY xi
12. INTRODUCTION 1
13. AIM AND OBJECTIVES 4
14. LITERATURE REVIEW 5
15. MATERIALS AND METHODS 20
16. RESULTS 24
17. TABLES 28
18. FIGURES 24
19. DISCUSSION 35
20. CONCLUSION 43
21. RECOMMENDATIONS 45
22. LIMITATIONS 46
23. REFERENCES 47
24. APPENDICES 60
LIST OF ABBREVIATIONS
ANOVA Analysis of Variance
ASA American Society of Anesthesiologists
BP Blood Pressure
CPB Cardiopulmonary bypass

6
DBP Diastolic Blood Pressure
ECG Electrocardiogram
Fig Figure
GA General Anaesthesia
g gram
HR Heart Rate
IV Intravenous
Kg Kilogram
LUTH Lagos University Teaching Hospital
MAP Mean Arterial Pressure
mg milligram
mgkg -1 milligram per kilogram body weight
MI Myocardial Infarction
ml millilitre
min minute
mmHg millimetres of mercury
RPP Rate Pressure Product
SBP Systolic Blood Pressure
SD Standard Deviation
SpO2 Arterial oxygen saturation
µg microgram
LIST OF TABLES
TABLE 1 - Demographic Data and Clinical Characteristics
Of Patients. 24

7
LIST OF FIGURES
FIGURE 1- Distribution of patients according to
Surgical Specialty. 23
FIGURE 2- Mean Heart Rate 25
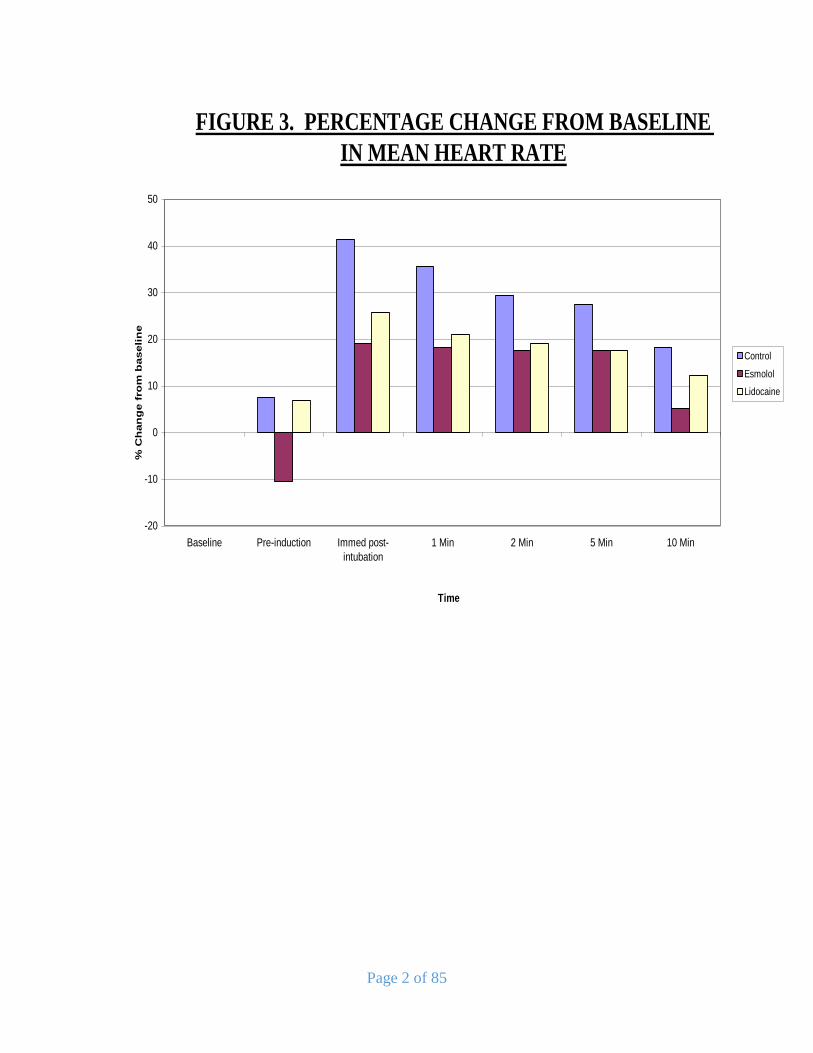
FIGURE 3- Percentage Change From Baseline in Mean Heart Rate. 26
FIGURE 4- Mean Systolic Blood Pressure 27
FIGURE 5- Percentage Change from Baseline in Mean
Systolic Blood Pressure 28
FIGURE 6- Mean Diastolic Blood Pressure 29
FIGURE 7- Percentage Change from Baseline in Mean
Diastolic Pressure. 30
FIGURE 8- Mean Arterial Pressure 31
FIGURE 9- Percentage Change from Baseline in
Mean Arterial Pressure 32
FIGURE 10- Mean Rate Pressure Product 33
FIGURE 11- Percentage Change from Baseline in
Mean Rate Pressure Product 34

8
LIST OF APPENDICES
1. APPENDIX I- Patient Proforma
2. APPENDIX II- Patient Consent Form
3. APPENDIX III- Ethical Committee Approval

9
SUMMARY
Laryngoscopy and tracheal intubation often elicit a haemodynamic response which
could be deleterious in patients with cardiovascular and intracranial pathology.
Lidocaine and esmolol are two of several agents used by anaesthetists to attenuate this
response. Lidocaine is the agent commonly used by anaesthetists practicing in most
developing countries like Nigeria as it is cheap, while esmolol has been used in parts of
North America, Europe and Asia. The effect of esmolol on the pressor response is yet
to be evaluated in an African population. The aim of this study was to evaluate and
compare the effectiveness of these two drugs in attenuating the haemodynamic changes
which accompany laryngoscopy and endotracheal intubation in an adult Nigerian
population at the Lagos University Teaching Hospital (LUTH).
Ninety (90) ASA physical status class 1 and 2 adult patients undergoing elective
surgical procedures under general anaesthesia were included in this randomised, single-
blind, placebo controlled study. The effectiveness of 2mg.kg -1 of esmolol administered
two minutes before laryngoscopy was compared with intravenous lidocaine 1.5mg.kg -
1 given three minutes before laryngoscopy in attenuating the pressor response to
laryngoscopy and endotracheal intubation. The patients were randomly assigned by
blind balloting to one of three groups, Esmolol (E), Lidocaine (L), and Control(C).
Group E patients had 2mg.kg -1 of intravenous esmolol made up to 20mls, given two
minutes before laryngoscopy and intubation. Group L patients had 1.5mg.kg -1 of
lidocaine made up to 20mls, administered intravenously 3 minutes before laryngoscopy
and intubation, while those in the control group were given a placebo of 20mls of 0.9%
saline 3 minutes before laryngoscopy.
Anaesthesia was induced with 4mg.kg -1 of 2.5% thiopentone sodium and tracheal
intubation facilitated with 1.5mgkg-1 suxamethonium chloride in all three groups. Heart

10
rate (HR), systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Mean
Arterial Pressure (MAP) and Rate pressure product(RPP) were recorded as baseline,
immediate post-intubation, 1, 3, 5 and 10minutes after laryngoscopy and intubation.
Readings of HR, SBP, DBP, MAP and RPP were compared with baseline values and
among each group.
All patients showed post-intubation increases in haemodynamic variables but to
varying degrees. The mean heart rate increased by 19.1%, 25.7% and 41.4% in groups
E, L and C respectively. SBP increased by 13.3%, 21.6% and 26.9%, DBP by 16.2%,
34.5% and 46.1%, MAP by 12.2%, 19.1% and 30.2% and RPP by 28.1%, 45.8% and
78.7% in groups E, L and C respectively.
The post-intubation rise in heart rate (HR) was significantly less in both treatment
groups (p<0.05) compared to the control group, but more in the esmolol group. There
was also a significantly lower increase in SBP post-intubation in the esmolol group
(p<0.05), but not in the lidocaine group (p>0.05). The changes in DBP and MAP were
significantly less in both treatment groups compared to the control group. Both
treatment techniques showed significance in attenuating the post-intubation rise in RPP
(P<0.05) but this was more in the esmolol group.
These findings demonstrated that both drugs in the doses used in this study, attenuated
the pressor response to laryngoscopy and intubation to varying degrees. As observed in
similar studies conducted in non-African patients, intravenous esmolol was statistically
superior to intravenous lidocaine for attenuating the haemodynamic response to
laryngoscopy and intubation. There were no complications attributable to the use of
either drug recorded during the course of the study.

11
INTRODUCTION
Following the first direct vision examination of the human larynx by Albert Kirstein in
18951 and its subsequent modification to involve the insertion of intratracheal tubes by
Chevalier Jackson in 19131,2 laryngoscopy and tracheal intubation became an integral
component of airway management and general anaesthesia.
Physical and direct stimulation of the pharynx and larynx by the laryngoscope blade
and the placement of an endotracheal tube elicit a sympathetic nervous system response

12
with a reflex consisting of a transient increase in blood pressure and heart rate, as well
as the occurrence of cardiac dysrhythmias3. These haemodynamic changes were first
reported by Reid and Brace in 19404. King and colleagues5 described a similar
cardiovascular response to laryngoscopy and intubation in 1951. This reflex has been
termed the “pressor response” and has been attributed to the sudden release of plasma
catecholamines occurring as a consequence of laryngoscopy and endotracheal
intubation6. A 40-50% increase in mean arterial pressure and a 20% increase in heart
rate may occur if the duration of the stimulus is prolonged7. These haemodynamic
changes are greatest one minute after intubation and typically last for about 5-10
minutes before returning to baseline values8. A sudden decrease in blood pressure may
be observed as this response ends due to the rapid metabolism of released plasma
catecholamines6.
A transient haemodynamic change presents a low risk to healthy individuals. In fact,
some researchers have actually questioned the importance attached to the
phenomenon9-11. It is however of major clinical significance in patients with pre-
existing systemic hypertension, hypertensive heart disease, coronary artery disease,
eclampsia, aneurysmal vascular disease and head injury in whom such a change may
culminate in perioperative myocardial ischaemia or infarction, cardiac failure,
dysrhythmias, cerebrovascular accidents or secondary brain injury12.
With advances in medical care and public health, the number of elderly and high risk
patients presenting for elective surgeries has steadily increased. Of particular interest
are patients with hypertension and coronary artery disease (CAD). Anaesthetists often
encounter hypertensive patients scheduled for elective surgical procedures. Some of
these patients are not well controlled or have a background of cardiac, cerebral or renal
complications of hypertension. Perioperative hypertension is an important etiological
1

13
factor for myocardial ischaemia as a sequel to anaesthesia and surgery13. Recently
conducted studies have revealed a high prevalence of essential hypertension amongst
Nigerians and research has shown that optimal control of blood pressure is difficult to
achieve even with proper medication14-16. Despite the fact that diagnosis and treatment
of hypertension are easy, a good number of patients are either not diagnosed or not well
controlled. Hypertensive patients have been shown to exhibit an exaggerated
haemodynamic response to laryngoscopy and intubation, associated with a high
incidence of subendocardial ischaemia.17,18 This has been observed to occur even when
the patients’ blood pressure appears controlled with anti-hypertensive therapy19,20.
Also, under emergency conditions where there is insufficient time for optimisation of
the patients’ intercurrent medical problems, achieving optimal blood pressure control
may be difficult if not impossible.
The prevalence of coronary artery disease is steadily increasing in sub-Saharan Africa
due to trends in urbanisation, changes in life-style and acquisition of technology21
.Ischaemic heart disease previously considered rare now ranks 8th among the leading
causes of death in men and women in the region22,23. In these patients the tachycardia,
hypertension and increase in rate pressure product, concomitant with intubation
represent a serious risk and has been shown to result in perioperative myocardial
ischaemia and infarction22. Since the presence of coronary artery disease may not
always be diagnosed preoperatively, the prevention of these haemodynamic changes
and their adverse sequelae is necessary to reduce perioperative morbidity and mortality.
Several methods of preventing this response have been recommended24-28. These
include the use of alternative guiding devices such as the fibreoptic bronchoscope24,
light wand25 or airway management with the laryngeal mask airway (LMA)26,27.
Recently, the use of the McCoy laryngoscope has been found to reduce the severity of

14
these haemodynamic changes28. Various pharmacological agents have been
administered prior to laryngoscopy in an attempt to attenuate this reflex29-33. Of
particular interest is the use of intravenous lidocaine which is the agent commonly used
by anaesthetists practicing in this environment. The results of studies conducted on its
use in this respect have varied34,35. On the other hand, esmolol, an ultra-short acting
cardioselective beta- adrenergic blocker has been shown to provide more consistent and
reliable protection against the pressor response36. There is however a dearth of research
on its use in an African population.
This prospective study was undertaken to evaluate the effectiveness of these two agents,
namely- esmolol hydrochloride and lidocaine hydrochloride, in attenuating the
haemodynamic response to laryngoscopy and tracheal intubation, and to compare their
relative effectiveness in a Nigerian population.

15
AIM AND OBJECTIVES
AIM
To compare the effectiveness of intravenous lidocaine and esmolol in the prevention of
the haemodynamic response to laryngoscopy and endotracheal intubation in a Nigerian
population at the Lagos University Teaching Hospital.
OBJECTIVES
To evaluate the effect of an intravenous dose of lidocaine on the haemodynamic
response to laryngoscopy and intubation.
To evaluate the effect of an intravenous dose of esmolol on the haemodynamic
response to laryngoscopy and intubation.
To compare the effects of intravenous lidocaine and esmolol on the pressor response
to laryngoscopy and intubation.
To determine the occurrence of complications with the use of either agent.

16
LITERATURE REVIEW
A haemodynamic response of increased heart rate and blood pressure to manipulation
in the area of the larynx, by means of laryngoscopy and intubation was first reported
by Reid and Brace4. Subsequently, Forbes and Dally37 reported an average rise in mean
arterial pressure of 25mmHg following laryngoscopy and insertion of an endotracheal
tube in 22 patients in whom anaesthesia was induced with sodium thiopentone.
These haemodynamic changes have been interpreted as being the result of reflex
sympatho-adrenal stimulation. In a study conducted by Tomori and Widdicombe using
anaesthetised cats, they observed that mechanical stimulation of four areas of the upper
respiratory tract i.e. the nose, epipharynx, laryngopharynx and tracheobronchial tree
induced reflex cardiovascular responses associated with enhanced neuronal activity in
the cervical sympathetic efferent fibres38. These cardiovascular responses, tachycardia
and hypertension, as well as the enhanced neuronal activity were most pronounced
during stimulation of the epipharynx while those arising from the stimulation of the
tracheobronchial tree were least marked38.
Subsequent researchers have confirmed these findings. In a study of 24 patients
undergoing elective surgery under general anaesthesia, Shribman et al reported that
laryngoscopy alone increased blood pressure and that laryngoscopy and intubation
together increased both heart rate and blood pressure39. The study also demonstrated a
significant increase in serum catecholamine levels during laryngoscopy with or without
concomitant intubation. Similarly, Russel and colleagues40 demonstrated a significant
increase in mean arterial pressure and plasma norepinephrine levels following
endotracheal intubation suggesting a predominantly sympathetic response during
intubation. This elevation in blood pressure and heart rate was maximum when the

17
duration of laryngoscopy exceeded 30 seconds .The authors went on to recommend the
need for prophylaxis in high risk patients.
Some authors have questioned the notion that these cardiovascular reflexes are caused
solely by increased sympathetic and sympathoadrenal activity41,42. The efferent
sympathetic outflow to the heart is T1-T4, while that to the adrenal medulla is from T3-
L343,44. Wathill et al45 reported that the cardiovascular response to intubation is
abolished in patients undergoing thoracolumbar epidural anaesthesia. However, Dohi
et al42 observed that acute sympathectomy induced in part by cervical or lumbar
epidural block did not prevent haemodynamic responses to laryngoscopy and
intubation.
Anaesthesia literature contains several studies evaluating various pharmacological
agents used for attenuating these haemodynamic changes in adults. It has been
suggested that the ideal agent for obtunding the pressor response should have a rapid
onset of action, be safe, easily administered and have a relatively short duration of
action10. The following are the various drugs which have been utilised for blunting the
haemodynamic response to laryngoscopy and intubation:
Local anaesthetic agents
The efficacy of intravenous and topical oropharyngeal local anaesthetic agents for
attenuating the pressor response has been extensively studied29,34,46. The postulated
mechanism for inhibiting this sympathetic response is an increased threshold for airway
stimulation and central inhibition of sympathetic stimulation. Derbyshire and
colleagues47 investigated the use of topical anaesthesia of the upper airway using 160mg
of 4% lidocaine in adult patients. They concluded that it was an ineffective means of
ameliorating the pressor and catecholamine response to laryngoscopy and intubation.

18
Several researchers have recommended 1.5mgkg-1 of lidocaine given intravenously 3
minutes before laryngoscopy as optimal for attenuating the response 34,35,48 .
Durrani et al46 found intravenous chloroprocaine an excellent local anaesthetic for
blunting the sympathetic response. A bolus dose of 4.5mgkg-1 given 45 seconds before
laryngoscopy significantly diminished increases in blood pressure as well as plasma
catecholamine concentrations in response to intubation.
Opioids
Narcotics have been used for attenuating the haemodynamic as well as catecholamine
response to endotracheal intubation49,50. The analgesic effects of these agents suppress
the nociceptive stimulation caused by laryngoscopy and intubation. There is also a
centrally mediated decrease in sympathetic tone associated with their use49.
Fentanyl in doses ranging between 2µgkg-1 and 7µgkg-1 given 1 to 2 minutes before
laryngoscopy has been found to be effective in attenuating the increase in heart rate,
blood pressure and rate-pressure product following laryngoscopy and intubation51,52.
Crawford et al53 reported a significant reduction in post-intubation rise in heart rate,
systolic blood pressure and serum epinephrine concentration with the use of 40µgkg-1
of alfentanil. However, the doses of opioids required for attenuation of the pressor
response often result in hypotension, bradycardia, respiratory depression, skeletal
muscle rigidity and delayed recovery51,53.
Remifentanil, which has a rapid onset and short duration of action, has been used for
attenuation of the haemodynamic response. Maguire et al54 found that a bolus
intravenous dose of 0.5µgkg-1 remifentanil followed by a 0.1µgkg-1 min-1 infusion
administered just prior to laryngoscopy, was effective in controlling the response.
Beta adrenergic blockers

19
Selective beta-1 blockade produces a decrease in heart rate and myocardial contractility
whereas antagonism of the beta-2 receptor produces bronchial and vascular smooth
muscle constriction. Achola et al55 studied the use of intravenous practolol 10mg given
just before laryngoscopy for attenuation of the pressor response and concluded that it
lacked efficacy in this respect. The use of 10mg intravenous propranolol by McCamon
and colleagues was associated with excessive myocardial depression (hypotension and
bradycardia) and a duration of action which outlasted the transient haemodynamic
changes induced by laryngoscopy and intubation56. Of the various beta blockers used
for attenuation of the pressor response, esmolol, a beta-1 blocker with an ultra-short
duration of action has yielded the most reliable results.34,57
Vasodilators
Sodium nitroprusside and nitroglycerine have been evaluated for the attenuation of the
pressor response to laryngoscopy and intubation but their use requires continuous intra-
arterial monitoring. Mikawa et al30 reported that intravenous nitroglycerine 2.5µgkg-1
had no effect on the tachycardia but significantly reduced the mean arterial pressure
and rate-pressure product changes associated with tracheal intubation. Similarly,
Stoetling58 reported that rapid intravenous injection of sodium nitroprusside at a dose
of 1-2µgkg attenuated the blood pressure but not the heart rate changes following
laryngoscopy and intubation.
Calcium channel blockers
The commonly evaluated calcium channel blocking agents for attenuating the
haemodynamic response are verapamil, diltiazem and nicardipine59,60. Yaku et al61
found that intravenous verapamil given in a dose of 0.05mgkg-1 attenuated the increase
in mean arterial pressure and rate pressure product after tracheal intubation. Verapamil
failed to prevent the tachycardia despite its negative chronotropic effect. Similarly, both
20
nicardipine and verapamil at intravenous doses of 0.03mgkg-1 and 0.1mgkg-1
respectively failed to control the tachycardia despite being effective in attenuating the
increase in blood pressure associated with laryngoscopy and intubation62.
Volatile anaesthetic agents
Inhalational agents like halothane and enflurane in various concentrations have been
used during induction to increase depth of anaesthesia as well as control the
haemodynamic response63,64. High concentrations may prove detrimental in
cardiovascular compromised patients. Using halothane 2% with nitrous oxide in oxygen
for 2 minutes before laryngoscopy, Kautto et al observed a significant attenuation of
the pressor response63. However, a higher concentration of halothane produced
significant cardiac dysrhythmias. Bedford et al64 found 0.7% enflurane a more suitable
alternative to 2% halothane for attenuation of the pressor response to laryngoscopy and
intubation.
Intravenous induction agents
Agents used to induce anaesthesia have been shown to influence the pressor response
to laryngoscopy and tracheal intubation. Ebegue65 demonstrated that following
induction of anaesthesia with 4mgkg-1of sodium thiopentone, the administration of a
second dose of thiopentone (4mgkg-1) just before laryngoscopy significantly attenuated
the heart rate, systolic blood pressure and rate pressure product changes accompanying
laryngoscopy and intubation. Similarly, Amadasun66 reported that a repeat of an
induction dose of sodium thiopentone given just before laryngoscopy was statistically
superior to intravenous lidocaine for attenuation of the pressor response.
Sood and colleagues67 demonstrated that the administration of a repeat dose (25% of
the induction dose) of intravenous propofol just prior to laryngoscopy limits the

21
duration of the pressor response to one minute. However, 55.5% of their patients
complained of pain on injection of propofol.
Alpha 2-adrenoceptor antagonists
These agents interact with catecholaminergic neuronal system which modulates tonic
and phasic blood pressure control and reduce the release of norepinephrine from nerve
endings both centrally and peripherally. Ghignone68 showed that cardiovascular
responses following laryngoscopies of less than 30 seconds duration can be attenuated
with 5µg.kg -1oral clonidine given 45 minutes before laryngoscopy. Scheinin et al69
found that intravenous dexmedetomidine at a dose of 0.2-0.7µg.kg -1 attenuates the
stress-induced sympathoadrenal responses to laryngoscopy, intubation and surgery and
provides increased haemodynamic stability.
Miscellaneous
Other drugs that have been used to attenuate the haemodynamic response to
laryngoscopy and intubation are; labetalol, magnesium sulphate, gabapentin, captopril,
prostaglandin E1 and adenosine triphosphate.
Amar et al70 reported that labetalol, a non-selective α and β adrenergic blocker at a
dose of 0.5mgkg-1 significantly attenuated the rise in blood pressure and heart rate, but
did not prevent the rise in plasma catecholamines associated with laryngoscopy and
intubation. The use of larger doses of labetalol was associated with significant
hypotension.
Magnesium sulphate attenuates catecholamine output from adrenal medulla and
adrenergic nerve endings and this reduces the severity of the pressor response. Puri and
colleagues71 found intravenous magnesium sulphate 40mgkg-1 effective for attenuation
of the pressor response to laryngoscopy and intubation as well as producing less ST
segment changes in patients with coronary artery disease undergoing coronary artery

22
bypass grafting. In patients with gestational hypertension, magnesium was found to be
more effective than intravenous lidocaine in attenuating the pressor response72.
Fassoulaki and colleagues73 observed that oral gabapentin at a dose of 800-1600mg
given at 6 hourly intervals before surgery attenuated the pressor response but not the
tachycardia associated with laryngoscopy and endotracheal intubation. Sanir et al74
evaluated the effect of oral captopril on haemodynamic responses and reported that a
dose of 12.5mg administered 45minutes prior to induction of anaesthesia significantly
attenuated the hypertensive, but not the tachycardic response to tracheal intubation. In
a study by Mikawa and colleagues75, prostaglandin E1 given as an infusion at 0.6ugkg-
1 attenuated the hypertension during tracheal intubation but failed to blunt the
tachycardia. It also enhanced the increase in plasma noradrenaline concentration
following intubation. Adenosine, a potent vasodilator has been successfully used at a
dose of 0.05-0.1mgkg-1 to attenuate the haemodynamic response to laryngoscopy and
intubation76. Its onset of action is fast and its duration of action transient. Although it
has a negative chronotropic effect, like other vasodilators it fails to control the
tachycardia associated with the response
INTRAVENOUS LIDOCAINE HYDROCHLORIDE
Lidocaine is an amide –derived local anaesthetic and class IB anti-dysrhythmic agent77.
It has found clinical uses in local and regional anaesthesia, treatment of ventricular
dysrhythmias, and the attenuation of the haemodynamic response to laryngoscopy and
intubation. It acts by stabilising the neuronal membrane by inhibiting the sodium flux
required for the initiation and conduction of impulses78.
Its anti-pressor effect is believed to be via depression of laryngeal reflexes. It also
reduces thiopentone requirements by 13.3%.79,80

23
The use of intravenous lidocaine for the attenuation of the pressor response has been
extensively researched upon with different conclusions.
Abou-Madi et al35 compared 1.5mg.kg -1 of intravenous lidocaine given 3 minutes
before laryngoscopy with placebo in 30 patients; and found that the mean increase in
systolic blood pressure was 10.3% for patients pre-treated with lidocaine and 56% in
patients receiving placebo. The mean increase in heart rate was 16.8% in the lidocaine
group and 38.8% in the placebo group. Using a similar technique, Tam, Chung and
Campbell81 observed complete attenuation of the response when this dose of lidocaine
was administered 3 minutes before laryngoscopy. Splinter and Cevenko82 in a study of
150 geriatric patients, concluded that intravenous lidocaine given 4-4.5minutes before
intubation attenuated the pressor response. They however agreed with Tam et al81 that
in younger adults, the optimal time to administer intravenous lidocaine is 3 minutes
before laryngoscopy.
Lev and Rosen34 conducted a review of twenty-five studies pertaining to the use of
intravenous lidocaine for attenuation of the pressor response. Sixty per cent (60%) of
the studies reviewed demonstrated that lidocaine produced some benefit in attenuating
the cardiovascular response to intubation. A dose of 1.5mg.kg -1 administered
intravenously 3 minutes before intubation was recommended as optimal. None of the
studies documented any harmful effects of prophylactic lidocaine given preintubation.
Amadasun48 investigated the effectiveness of intravenous lidocaine in obtunding the
pressor response in a sample of Nigerian patients. In a randomised, controlled trial, a
total of 80 ASA class 1 and 2 patients were studied in two groups of 40 patients each.
Lidocaine was administered at a dose of 1.5mg.kg -1 three minutes before laryngoscopy
in the study group. He reported that intravenous lidocaine significantly attenuated the

24
post intubation rise in heart rate and rate-pressure products without significant effect on
blood pressure.
Miller and Warren83 in a study of 45 Chinese women could not demonstrate any
significant benefit of 1.5mg of lidocaine given intravenously 1, 2 or 3 minutes before
laryngoscopy. Prior to this, Laurito and colleagues84 administered a combination of
nebulized lidocaine 4mg.kg -1 and an intravenous dose 2mg.kg -1, and reported a lack
of effect on the cardiovascular response to laryngoscopy and intubation compared with
control. However, in their study they intubated their patients one minute after lidocaine
injection. They suggested the abandonment of the use of lidocaine prior to laryngoscopy
for the attenuation of the pressor response.
INTRAVENOUS ESMOLOL HYDROCHLORIDE
The use of beta adrenergic blockers for the attenuation of the pressor response was
pioneered by Prys-Roberts and colleagues in 197985. They studied the haemodynamic
sequelae to laryngoscopy and intubation in hypertensive patients and demonstrated a
significant attenuation of the pressor response in patients pre-treated with intravenous
or oral practolol. Subsequently, various workers have demonstrated the utility of beta
blockade in attenuation of the pressor response56, 86. Beta –adrenoceptor blockade
minimises the increase in heart rate and myocardial contractility (primary determinants
of oxygen consumption) by attenuating the positive chronotropic and inotropic effects
of increased adrenergic activity87. However, the use of beta-blocking agents for the
attenuation is not without risks. Potential negative sequelae related to beta- blockade
for attenuation include: excessive myocardial depression, bronchial constriction, and
the possibility that the duration of action of these agents may outlast the transient
haemodynamic changes induced by laryngoscopy and intubation.88

25
Esmolol, methyl-3-{4-3-[isopropyl amino] propoxy phenyl} propionate is a water
soluble, cardio-selective, ultra-short acting beta-adrenergic antagonist. It has been
shown to be effective in controlling both the heart rate and blood pressure responses to
intubation89.
Esmolol blocks the agonist effect of sympathetic neurotransmitters by competing for
beta 1 receptor sites. At therapeutic doses it lacks intrinsic sympathomimetic or
membrane stabilizing properties. Its anti-arrhythmic activity is due to blockade of
adrenergic stimulation of pacemaker potential. It is a class II antiarrhythmic agent90.
Esmolol undergoes rapid hydrolysis by esterases in red blood cells to a free acid
metabolite and methanol culminating in a short elimination half-life of 9.2 ±
2.0minutes. The short duration of action has led to its use in a number of situations
requiring beta receptor antagonism of limited duration e.g. treatment of
supraventricular dysrhythmias, perioperative hypertension and phaeochromocytoma64.
A total body clearance of 285 ml/min ensures a rapid offset of action and it is eliminated
via the kidneys almost entirely as its metabolite91. It achieves peak effect on heart rate
within one minute and on blood pressure within two minutes of intravenous injection92.
These unique pharmacokinetic and pharmacodynamic properties make esmolol suitable
for administration by either continuous infusion or bolus injection. It has been used in
different doses either as a bolus or in an infusion form to attenuate the haemodynamic
response to laryngoscopy and endotracheal intubation.
The first study conducted on the subject was published by Gold et al93 who found that
peak heart rates and systolic pressures following intubation after ketamine induction
were significantly attenuated by esmolol. Several researchers have established the
effectiveness of esmolol infusions in the prevention of haemodynamic alterations
following tracheal intubation. Ghaus et al94 reported that a bolus infusion of esmolol

26
administered at a dose of 300µg.kg-1.minute-1 for 4 minutes, followed by a maintenance
infusion of 200µg.kg-1.minute-1 for 12 minutes offered significant control of all the
haemodynamic variables. Figueredo and Fuentes95 conducted a meta-analysis of 38
randomised controlled trials on the effect of esmolol on the adrenergic stress response.
Eleven different regimens demonstrated effectiveness in the attenuation of heart rate
and blood pressure after laryngoscopy and intubation, the most effective of which was
a loading dose of 500µg.kg -1.minute-1 over 6 minutes followed by a continuous infusion
of 200-300µg.kg-1.minute-1 for 9 minutes.
Some authors have argued that while infusions are easy to set up, they require
additional equipment and time which may not be readily available96,97. In addition, the
dosing regimen and time required for preparation of an infusion may add a degree of
complexity to the induction process which is often unnecessary. Miller et al97 advocated
that since esmolol has a rapid onset and short duration of action, bolus injection might
be a simple and effective alternative to infusion in situations involving transient
hyperdynamic cardiovascular events such as laryngoscopy and intubation.
The use of bolus dosing of esmolol for the control of the pressor response to
laryngoscopy and intubation has produced different results.97-86 The optimal bolus dose
of esmolol required to attenuate the haemodynamic response to laryngoscopy and
endotracheal intubation has been a subject of debate .Various researchers have
administered esmolol as either fixed doses or on a weight basis. Tariq et al98 used
esmolol at a dose of 1mg/kg 2 minutes before laryngoscopy and concluded that it only
partially attenuated the haemodynamic response but did not abolish it completely.
Miller and Martineau99 demonstrated that bolus doses of esmolol, approximately
1.5mg.kg -1, administered to patients with known or suspected coronary artery diseases
2 minutes before laryngoscopy and intubation, could effectively control post induction

27
increases in heart rate. Hussein and Sultan100 evaluated the efficacy of esmolol at
2mg.kg -1 bolus given 2 minutes before intubation and reported an attenuation of the
increase in heart rate but not arterial pressure. However, following the administration
of an even larger dose of 4mg.kg -1 2 minutes before laryngoscopy in 100 elderly
patients scheduled for cataract surgery, Van den Berg and Honjol reported that esmolol
prevented the rise in heart rate and rate-pressure product only 101. Their findings were
similar to those of Cucchiara et al102 who concluded that although the increase in heart
rate and blood pressure associated with laryngoscopy and endotracheal intubation were
significantly lower when compared with placebo; the incidence of raised blood pressure
was about 60% even with large doses of esmolol.
Oxorn and Knox103 evaluated the effectiveness of esmolol administered in fixed doses
of 100mg and 200mg 90 seconds before laryngoscopy, in 48 patients undergoing
elective hysterectomy. They reported an attenuation of the rise in heart rate for 2.5
minutes following intubation after which it became indistinguishable from placebo. The
rise in blood pressure however, was not mitigated by either dose of esmolol when
compared with placebo. Rathore et al104 went further to compare three bolus doses of
esmolol for attenuation of the pressor response in 100 patients scheduled for elective
surgery under general anaesthesia. The patients were administered 50mg, 100mg or
150mg of esmolol 2 minutes before laryngoscopy and intubation. All the doses were
effective in blunting the pulse rate response but only the 150mg dose proved effective
in blunting the blood pressure response.
However, Bernstein105used similar doses of esmolol in a bolus fashion 2 minutes before
laryngoscopy and intubation, and found that hypertension and tachycardia were both
prevented following rapid sequence induction. He also reported a significantly lower
incidence of post-intubation ventricular tachyarrhythmias in the esmolol group. His

28
findings were attributed to a slightly larger dose of thiopentone (5mg.kg -1 versus
4.6mg.kg -1) given in closer proximity to the time of laryngoscopy and intubation than
was done by Oxorn and colleagues. There were no significant side effects attributable
to the use of esmolol in any of the studies.
ESMOLOL VERSUS LIDOCAINE
Helfman and colleagues106 compared the efficacies of intravenous esmolol and
lidocaine in attenuating the pressor response. In a double-blind, placebo-controlled trial
involving 80 patients undergoing non-cardiac surgery, they compared lidocaine 200mg,
fentanyl 200µg and esmolol 150mg, to determine which best prevented tachycardia and
hypertension due to tracheal intubation. Mean percentage increases in heart rate during
and after intubation were lowest in the esmolol group(12%) compared to the
lidocaine(51%), fentanyl (18%) and placebo(44%) groups; while the mean systolic
blood pressure increases were lowest in the fentanyl group(12%) compared to the
esmolol(19%) and lidocaine (20%) groups. Only esmolol provided consistent and
reliable protection against increases in both heart rate and blood pressure accompanying
laryngoscopy and intubation. Feng et al107 conducted a similar study but the test drugs
were administered on a weight basis as against the fixed doses used by Helfman and
colleagues. The incidence of tachycardia (heart rate more than 100/min) was 15% in
the esmolol group, significantly lower than the lidocaine (75%), fentanyl (55%) and
control (85%) groups. The incidence of hypertension (systolic blood pressure>
180mmHg) was also lower (20%) in the esmolol group compared to the lidocaine
(70%), fentanyl (40%) and control (80%) groups. They concluded that only esmolol
reliably offered protection against increases in both heart rate and systolic blood
pressure.

29
Questions have been raised with regards to the methodology deployed by these groups
of researchers which may have inadvertently introduced a bias in favour of esmolol108.
In both studies, laryngoscopy and intubation were performed 2 minutes after induction.
This might be expected to favour the effectiveness of esmolol which has a peak effect
on heart rate and blood pressure at 1 to 2 minutes as against that of lidocaine which is
at 2 to 3 minutes thus explaining why the principal benefits of lidocaine administered
within this time frame were not achieved.
Levitt and Dresden109 compared the effects of esmolol and lidocaine on the pressor
response during intubation of patients with intracranial hypertension following isolated
head trauma. Esmolol 2mg.kg -1 or lidocaine at 2mg.kg -1 was administered
intravenously just prior to intubation. The study did not reveal any significant difference
as neither drug effectively attenuated the haemodynamic response to intubation.
A few researchers have recommended the use of a combination of both drugs for
obtunding the pressor response to laryngoscopy and intubation. In a study conducted
by Kindler et al in 1996 110 , they compared esmolol, lidocaine and a combination of
both drugs administered 2 minutes prior to laryngoscopy. Esmolol 1 to 2 mg.kg -1 was
found to be reliably effective in attenuating the heart rate response to intubation while
the combination of esmolol 2mg.kg-1 and lidocaine 1.5mg.kg -1 attenuated both the heart
rate and blood pressure responses to intubation. Neither esmolol nor lidocaine
administered alone affected the blood pressure response. Bansal and Pawar111compared
the efficacy of two bolus doses of esmolol with or without lidocaine in 80 patients with
pregnancy induced hypertension scheduled to undergo lower segment caesarean
section. The patients were allocated to four groups of 20 patients each and were
administered esmolol 1mg.kg-1 alone, esmolol 2mg.kg-1 alone, esmolol 1mg.kg-1 and
lidocaine 1.5mg.kg-1, or esmolol 2mg.kg-1 and lidocaine 1.5mg.kg-1 2 minutes before

30
laryngoscopy and intubation. The combinations of esmolol and lidocaine were effective
in attenuating the adrenergic responses to laryngoscopy and intubation. There were no
adverse effects in the mothers or their babies.
MATERIALS AND METHODS
This was a prospective study conducted over a period of six months among adult

31
elective surgical patients at the Lagos University Teaching Hospital. The approval of
the Research and Ethics Committee of the hospital (Appendix III) and informed consent
(Appendix II) of each patient were obtained. Ninety (90) patients with the American
Society of Anesthesiologists (ASA) physical status 1 or 2, between the ages of 18 and
60 years were included in the study. There were 50 males and 40 females. Exclusion
criteria included: known allergies to beta-adrenergic antagonists or local anaesthetic
agents; compensatory tachycardia (anaemia, infection, and hypovolaemia); cardiac
diseases (heart block of any degree, myocardial infarction, congestive cardiac failure,
and cardiac dysrhythmias); bronchospastic disease and chronic obstructive airway
disease. Also excluded were those on cardioactive drugs, antihypertensive agents,
theophylline, beta-agonist, and ipatropium bromide or inhaled steroid therapy. All the
patients were seen in the ward at least a day before surgery for pre-operative
assessment. This entailed obtaining a history, conducting physical examination and
requesting relevant investigations. The patients were weighed and their weights were
documented in their case notes. Anaesthetic premedication was prescribed consisting
of 10mg oral diazepam given with a sip of water the night before surgery and one hour
before induction of anaesthesia. Preoperative fasting guidelines of 6 hours to solids and
2 hours to clear fluids were observed.
On arrival at the operating theatre, the patients who required endotracheal intubation
were randomly assigned by blind balloting to one of three groups, L (Lidocaine), E
(Esmolol) and C (Control).The anaesthetic drugs were drawn in appropriate doses and
an equipment check was performed. A multiparameter Siemens™ monitor incorporated
with a blood pressure cuff and pulse oximetry probe was attached to the patients.
Baseline heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP),
mean arterial pressure (MAP) and arterial oxygen saturation (SpO2) were obtained in

32
the supine position and recorded by an anaesthetist registrar (person A). Intravenous
access was established using a size 18G cannula and an infusion commenced with a
0.9% saline solution. Based on the designated study group, the drugs were drawn in
sterile unlabelled 20ml syringes and made up to equal volumes of 20mls with normal
saline by the primary researcher (person B). This was done in the preanaesthetic room
after which the drug was handed over to an anaesthetist registrar for administration to
the patient (person C). All test drugs were colourless.
The patients were pre-oxygenated for five minutes by the primary researcher. During
preoxygenation, the group L patients were given 1.5mg.kg -1 of Lidocaine
hydrochloride while the group E patients received 2mg.kg -1 Esmolol hydrochloride by
slow intravenous injection over 30 seconds. Patients in the control group(C) received
20mls of 0.9% saline solution. Following the administration of the test drugs, the
haemodynamic variables were measured and recorded (pre- induction values) by the
anaesthetist registrar (Person A) who was blinded to the designated agent.
Anaesthesia was then induced in all the groups with 5mg.kg-1 thiopentone sodium by
slow intravenous injection followed with 1.5mg.kg-1 suxamethonium chloride given
intravenously. Prior to and during the induction period, verbal contact was maintained
with the patients to detect any adverse reactions to the test drugs such as tinnitus,
circumoral numbness, pain at the injection site or tightness in the chest.
After adequate muscle relaxation as judged by jaw relaxation or disappearance of
fasciculations, laryngoscopy was undertaken by the primary researcher with a size 4
curved Macintosh blade at 3 minutes in the Lidocaine and Control groups and 2 minutes
in the Esmolol group, and then endotracheal intubation with an appropriate sized
polyvinyl chloride (PVC) tube was done in each case. Following successful passage of
the tracheal tube and immediately after removal of the laryngoscope, HR, SBP, DBP

33
and MAP were recorded from the automatic oscillometer while the Rate Pressure
Product (RPP) was calculated and recorded. Surgical stimulation as well as the
administration of analgesic supplements and muscle relaxants were avoided during the
study period i.e. start of induction to 10 minutes later. Anaesthesia was maintained with
an inspired halothane concentration of 1.5-1.8% in 100 per cent oxygen.
HR, SBP, DBP and MAP readings were obtained at 1, 3, 5 and 10 minutes after tracheal
intubation and at 10 minute intervals thereafter till the end of surgery.
The Rate Pressure Product (RPP) was calculated thus;
Rate Pressure Product = Heart Rate X Systolic Blood Pressure, and recorded.
The duration of laryngoscopy and intubation was determined by stop watch
measurement and recorded. This was taken as the time from oral passage of the
laryngoscope to successful placement of the endotracheal tube. Patients with difficult
and /or repeated laryngoscopy and /or intubation that lasted for over 30 seconds were
excluded from the study. Laryngoscopy was performed by the primary researcher in all
the patients.
The following parameters were defined for the study:1) Hypotension was defined as
SBP< 25% of baseline value or 90 mm Hg; 2) Hypertension was defined as SBP > 25%
of baseline value or 150mm Hg; 3) Tachycardia was defined as HR > 25% of baseline
value; 4) Bradycardia was defined as HR < 60 beats.min-1.
Data collected was entered into a proforma (Appendix I) and analysed with computer
analytical package Epi 6 info, version 6.4.
Data was reported as mean± SD and percentage changes. Repeated measures of
ANOVA were used to compare values for heart rate, systolic blood pressure, diastolic
blood pressure, mean arterial pressure and rate pressure product, to baseline values in
each group. Repeated measures of ANOVA were also used to compare the

34
haemodynamic variables between the three groups. Differences were deemed
significant at a p value<0.05.
Microsoft excel™ software was used for graphical presentation.
RESULTS
Patients were selected from the different surgical specialties. Patients presenting for
general surgical procedures constituted the largest number of 28 (31.1%), while the ear,
nose and throat (ENT) surgery patients were the least (2.2%). Figure 1 shows the
distribution of the sample population according to surgical specialty.
The demographic data was compared among the three groups. There was no significant
difference between the groups with respect to age, gender, weight, ASA score or

35
duration of laryngoscopy (Table 1).
A. HEART RATE
Compared with the baseline readings, the mean heart rate was increased after
laryngoscopy and tracheal intubation in all three groups as depicted in figure 2. This
was highest in the control group where laryngoscopy and intubation caused a rise in the
heart rate from a mean baseline value of 80.6 to 114.0, an increase of 41.4% which was
statistically significant (p=0.000). In the lidocaine group, the heart rate rose from 82.2
to 108.4, an increase of 25.7%. This was significantly less than the rise observed in the
control group (p=0.012). There was an initial decrease in heart rate after the
administration of esmolol which was significant (p=0.04) but this was followed by a
rise following laryngoscopy and intubation. In the esmolol group, mean heart rate
increased from 86.8 to 103.4, an insignificant increase of 19.1%. This differed
significantly from the control group (P=0.001) but not the lidocaine group (p=0.275).
At 1,3 and 5 minutes after laryngoscopy and endotracheal intubation, there was a
decrease in heart rate in all the three groups but the changes were not statistically
significant (P>0.05) and at 10 minutes post-intubation, this parameter closely
approached baseline values in the esmolol and lidocaine groups(figure 3)
B. MEAN SYSTOLIC BLOOD PRESSURE
Compared to the baseline values, the systolic blood pressure (SBP) increased in all three
groups following laryngoscopy and intubation (figure 4). The increase was highest in
the control group where it rose significantly from a mean baseline value of 128.7 to
163.3 (26.9%) post-intubation (p=0.002), and least in the esmolol group, which
increased from 135.1 to 153.1 (13.3%) (p=0.056). There was a significant difference
between the esmolol and control groups (p=0.002). In the lidocaine group there was a

36
significant rise in SBP of 21.6% post laryngoscopy and intubation, but this did not differ
significantly from the esmolol(p=0.066) or control(p=0.055) groups.
Systolic blood pressure gradually declined in all the three groups and decreased below
baseline values after 5 minutes in all the three groups. The decrease was significant in
both treatment groups (p=0.02) but not in the control group (p=0.062). Despite this
drop, systolic blood pressure remained above 110mmHg in all three groups. Figure 5
shows the mean systolic blood pressure changes in all three groups.
C. MEAN DIASTOLIC PRESSURE
The control group (C) and both study groups (L and E) all registered a rise in the mean
diastolic pressure (DBP) immediately after laryngoscopy and intubation. In the esmolol
group there was an initial insignificant fall in diastolic blood pressure following the
administration of the drug (p=0.506). The mean diastolic pressure in the control group
rose from 78.0mmHg to 114.0mmHg (46.1%) at laryngoscopy and intubation, whereas
in the lidocaine and esmolol groups, the values rose from 79.1 and 85.6 mmHg to 106.3
(34.5%) and 99.5mmHg (16.2%) respectively. The difference between both treatment
groups and the control group was significant following intubation but this was more
significant in the esmolol group (p=0.000) compared to the lidocaine group (P=0.001)
(figure 6)
By 5 minutes the mean diastolic blood pressure decreased below baseline values but
remained above 70mmHg in all three groups (figure7).
D. MEAN ARTERIAL PRESSURE
There was an initial decrease in mean arterial pressure (MAP) in the esmolol and
Lidocaine groups following the administration of the study drugs which was not
statistically significant (p=0.06 and p=0.08 respectively). This increased in all groups

37
following laryngoscopy and intubation. In the control group, there was a significant
30.2% increase from mean baseline value of 97.1 to 126.4(p=0.001). In the lidocaine
group, the mean baseline MAP of 109.3 rose to 130.2 post intubation, an increase of
19.1%. The increase was least in the esmolol group where it rose from 103.8 to 116.5
(12.2%). These changes were significantly less in both groups compared to the control
group, but more so in the esmolol group (p=0.000) than the lidocaine group (p=0.02).
(Figure 8). There was no significant difference between both treatment groups (p=0.08).
By 3 minutes post-intubation, there was a progressive decrease in MAP and by 5
minutes the values had dropped to less than the baseline values (figure 9). This drop
was most in the lidocaine group (19.5%) and least in the control group (10% ).
E. THE MEAN RATE PESSURE PRODUCT (RPP)
The mean rate pressure product values in the control group showed a significant
increase at intubation from 10381.3 to 18549.9 (78.7%) p=0.000. The values in the
lidocaine and esmolol groups also showed an increase from 11438.6, 12550.9 to
16681.4 (45.8%) and 16072.7 (28.1%) respectively (figure 10). The difference was
highly statististically significant compared to control group in both lidocaine and
esmolol groups following intubation, p=0.000 and p=0.000 respectively. At 3 minutes
post-intubation, a decrease in the mean rate pressure product below the baseline value
was observed in the esmolol group and was sustained till 10 minutes post intubation
(figure 11).
There were no complications attributable to the use of either study drug recorded during
the course of the study.

38
31%
29%22%
10%6% 2%
FIGURE 1. THE DISTRIBUTION OF PATIENTS ACCORDING TO SURGICAL SPECIALTY
General Surgery
Gynaecology
Urology
Orthopedics
Burns and Plastics
Ear, nose and throat

39
TABLE 1 DEMOGRAPHIC DATA AND CLINICAL CHARACTERISTICS
OF PATIENT
Control
n=30
Lidocaine
n=30
Esmolol
n=30
P value
Age/years
mean± SD
35.0±13.35 38.8±10.99 36.0±11.72 0.846
Weight/ kg
mean± SD
66.3±8.47 70.5±11.97 60.7±9.79 0.414
Gender ratio
(M:F)
16:14 15:15
18:12 0.302
ASA classification ratio
( I:II)
18:12 16:14 17:13 0.058
Duration of laryngoscopy and
Tracheal intubation/ seconds
(mean ± SD)
20.6±3.90 19.77±3.76 21.3±5.90 0.718

Page 1 of 85
70
75
80
85
90
95
100
105
110
115
120
Ba
se
line
Imm
ed
po
st-
intu
ba
tion
3 M
in
10
Min
Me
an
He
art
Ra
te(b
ea
ts/m
inu
te)
Time
FIGURE 2. MEAN HEART RATE
Control
Esmolol
Lidocaine
Page 2 of 85
FIGURE 3. PERCENTAGE CHANGE FROM BASELINE
IN MEAN HEART RATE
-20
-10
0
10
20
30
40
50
Baseline Pre-induction Immed post-
intubation
1 Min 2 Min 5 Min 10 Min
Time
% C
han
ge f
ro
m b
aseli
ne
Control
Esmolol
Lidocaine

Page 3 of 85
100
110
120
130
140
150
160
170
Baselin
e
Pre-in
ductio
n
Imm
ed p
ost In
tubatio
n
1 M
in
3 M
in
5 M
in
10
Min
Mea
n S
yst
oli
c B
loo
d P
ress
ure
(m
mH
g)
Time
FIGURE 4. MEAN SYSTOLIC BLOOD PRESSURE
Control
Esmolol
Lidocaine

Page 4 of 85
FIGURE 5. PERCENTAGE CHANGE FROM BASELINE IN MEAN SYSTOLIC BLOOD
PRESSURE
-20
-15
-10
-5
0
5
10
15
20
25
30
Baseline Pre-induction Immed post
Intubation
1 Min 3 Min 5 Min 10 Min
Time
% C
han
ge f
rom
baseli
ne
Control
Esmolol
Lidocaine

Page 5 of 85
60
70
80
90
100
110
120
Baselin
e
Pre
-ind
uctio
n
Imm
ed
post
intu
batio
n
1 M
in
3 M
in
5 M
in
10
Min
Mean
Dia
sto
lic B
loo
d p
ressu
re (
mm
Hg
)
Time
FIGURE 6. MEAN DIASTOLIC BLOOD PRESSURE
Control
Esmolol
Lidocain
e

Page 6 of 85
FIGURE 7. PERCENTAGE CHANGE IN MEAN DIASTOLIC
PRESSURE
-20
-10
0
10
20
30
40
50
Baseline Pre-induction Immed post
intubation
1 Min 3 Min 5 Min 10 Min
Time
% c
han
ge i
n D
iasto
lic b
loo
d p
ressu
re
Control
Esmolol
Lidocaine

Page 7 of 85
60
70
80
90
100
110
120
130
140
Ba
se
line
Pre
-ind
uctio
n
Imm
ed
po
st in
tub
atio
n
1 M
in
3 M
in
5 M
in
10
Min
Me
an
Art
eri
al
pre
ss
ure
(m
mH
g)
Time
FIGURE 8. MEAN ARTERIAL PRESSURE
Control
Esmolol
Lidocaine

Page 8 of 85
FIGURE 9. PERCENTAGE CHANGE FROM BASELINE IN MEAN
ARTERIAL PRESSURE
-30
-20
-10
0
10
20
30
40
Baseline Pre-induction Immed post
intubation
1 Min 3 Min 5 Min 10 Min
time
% c
han
ge f
rom
baseli
ne Control
Esmolol
Lidocaine

Page 9 of 85
8000
10000
12000
14000
16000
18000
20000
Base
line
Pre
-ind
uctio
n
Imm
ed p
ost in
tuba
tion
1 M
in
3 M
in
5 M
in
10
Min
Mea
n R
ate
-p
res
su
re P
rod
uct
ch
an
ge
(mm
Hg
bea
ts.m
in-1
)
Time
FIGURE 10. MEAN RATE-PRESSURE PRODUCT
Control
Esmolol
Lidocaine

Page 10 of 85
FIGURE 11. PERCENTAGE CHANGE FROM BASELINE IN MEAN RATE-
PRESSURE PRODUCT
-20
-10
0
10
20
30
40
50
60
70
80
90
Baseline Pre-induction Immed post
intubation
1 Min 3 Min 5 Min 10 Min
Time
% C
han
ge f
rom
baseli
ne
Control
Esmolol
Lidocaine
Page 11 of 85
DISCUSSION
Laryngoscopy and intubation are associated with a cardiovascular response of elevated
blood pressure and pulse rate as well as occasional dysrhythmias. Lidocaine and esmolol
are two drugs which have been used by anaesthetists in an attempt to attenuate this
response.
In this study, treatment with intravenous lidocaine three minutes before laryngoscopy and
intubation significantly attenuated the post-intubation increases in heart rate and rate
pressure product. A dose of 1.5mg.kg -1 was chosen based on work by Tam, Chung and
Campbell who observed complete attenuation of the response when this dose of lidocaine
(1.5mgkg-1) was given three minutes before laryngoscopy and intubation65. Similarly, a
review of 25 studies by Lev and Rosen on the preintubation use of lidocaine revealed that
a dose of 1.5mg.kg -1 given intravenously three minutes before intubation was optimal34.
In the present study, the heart rate increased by 25.7% in patients who received lidocaine
compared to the control value of 33.4%. This shows that lidocaine as used in this study
attenuates but does not abolish the post intubation rise in heart rate. This correlates with

Page 12 of 85
the findings of Wilson et al112 who reported that irrespective of the timing of administration
of intravenous lidocaine, 2, 3 or 4 minutes before tracheal intubation, there was an increase
in heart rate of 21-26 % in all groups studied. In this study, intravenous lidocaine had an
insignificant effect on the systolic blood pressure; 21.6% rise compared to the control value
of 26.9%. The effects of intravenous lidocaine on diastolic blood pressure and mean arterial
pressure were also not significant.

Page 13 of 85
Several authors have emphasized the importance of timing of administration of lidocaine
on its ability to attenuate the pressor response to laryngoscopy and endotracheal intubation.
Tam et al81 showed that when administered intravenously three minutes before intubation,
1.5mg.kg-1 lidocaine significantly attenuated haemodynamic changes secondary to
emergency intubation in patients with raised intracranial pressure following blunt head
injury. Wang et al113 reported that the values of systolic and diastolic pressures one minute
after intubation were significantly less in groups where 1.5mgkg-1 lidocaine was given
either 3 or 5 minutes before intubation.
In Miller and Warren’s study of a group of 45 Chinese women, intravenous lidocaine
1.5mg.kg-1 failed to attenuate the cardiovascular response to laryngoscopy and tracheal
intubation irrespective of the timing of administration i.e. 1, 2 or 3 minutes before
laryngoscopy83. In the same vein, Chraemmer-Jorgensen and colleagues114 reported a total
lack of effect of intravenous lidocaine given 2 minutes prior to laryngoscopy and
intubation, on the haemodynamic responses. Despite pre-treatment of their patients with
intravenous lidocaine, the rate- pressure products were observed to approach levels
considered potentially dangerous to patients with ischaemic heart disease. Differences in
study protocol, patient population, premedication, depth of anaesthesia, duration of
laryngoscopy and interval between lidocaine administration and laryngoscopy may
account for these apparently varied results among the different studies.
The pharmacokinetic properties of intravenous lidocaine may explain its ability to attenuate
the pressor response within a tightly specific time frame. Following intravenous injection,
the onset of action is between 45-90 seconds with a peak effect at 1-3 minutes77. Its
optimum effect on the haemodynamic response to laryngoscopy and intubation is most

Page 14 of 85
likely exerted at about its peak effect. It also obtunds laryngeal reflexes and reduces
thiopentone requirement by 13.3%79,80. Abou-madi et al35 suggested other possible
mechanisms to explain the anti-pressor effects of lidocaine. These include a direct
myocardial depressant effect, a peripheral vasodilating effect and a possible effect on
synaptic transmission.
There were no complications recorded following the administration of intravenous
lidocaine in this study. However, in their study evaluating the haemodynamic response to
laryngoscopy and intubation in geriatric patients, Splinter and Cervenko reported that 34%
of their patients who were given intravenous lidocaine developed tinnitus82.
In this study, the administration of intravenous esmolol resulted in a 19.1% increase in
post-intubation heart rate compared to 41.4% in the control group and 25.7% in the
intravenous lidocaine group. The esmolol group showed a rise in systolic blood pressure
(13.3%) but this was significantly less than those observed in the lidocaine (21.6%) and
control (26.9%) groups. The response to the dose of esmolol used in this study was similar
to that obtained by Helfman et al106 who compared lidocaine and esmolol for attenuation
of the pressor response and reported mean percent increases in heart rate of 44% lidocaine,
51% placebo and 18% in esmolol group. Mean systolic blood pressure percent increases
were 20% in the lidocaine, 36% in the placebo and 19% in the esmolol groups. Only
esmolol provided consistent and reliable protection against increases in both heart rate and
systolic blood pressure accompanying laryngoscopy and intubation.
The rationale for the administration of esmolol as a bolus rather than as an infusion in this
study was twofold; the desire for a rapid onset and short duration of action in order to
promptly treat a transient haemodynamic event as well as the convenience of bolus

Page 15 of 85
administration compared with the preparation and administration of an infusion. A dose of
2mg.kg-1 administered two minutes prior to laryngoscopy and intubation was chosen for
this study based on results of several published trials evaluating the use of esmolol for
attenuation of the pressor response92,99,105. Sintetos et al92 recommended that esmolol be
given 2 minutes before intubation for effective results because its maximum effects on
heart rate and blood pressure occurred in the first and second minutes respectively.
At 5 minutes, both treatment groups showed significant decreases in mean SBP compared
to baseline which persisted even until 10 minutes after intubation. This could be attributed
to the rapid metabolism of released catecholamines, myocardial depressant effect of the
volatile agent (halothane) and the absence of surgical stimulation6,10,63. Although none of
the patients in the study had hypotension, by definition, the 14.5% and 13.8% mean
reduction in SBP observed in the esmolol and lidocaine groups respectively, suggest their
potential for hypotension especially in haemodynamically unstable patients.
The rate-pressure product (RPP) increased post intubation in all the groups. Esmolol
showed significantly greater effects than lidocaine in attenuating the post-intubation rise in
RPP. The rate-pressure product (a product of the systolic blood pressure and heart rate) is
a good index of myocardial oxygen consumption and a threshold of RPP has been
correlated with the onset of angina in patients with known coronary artery diseases or those
who have risk factors for coronary artery disease115. Increased blood pressure and heart
rate lead to elevated myocardial oxygen demand and the haemodynamic changes at
intubation may precipitate myocardial ischaemia and infarction. Tachycardia increases
myocardial oxygen demand, decreases diastolic filling time, and hence coronary blood

Page 16 of 85
flow. A moderate increase in heart rate (15%) has been shown to be accompanied by a 17%
decrease in coronary perfusion pressure116.
Raised blood pressure, on the other hand, increases both oxygen demand and supply and
thus has a less predictable effect on myocardial oxygen balance. Furthermore, the increase
in blood pressure accompanying laryngoscopy and intubation has been attributed to an
increase in cardiac output rather than increased systemic resistance117. Hence, by its
predominant attenuation of increases in heart rate, esmolol is more likely to optimize the
myocardial oxygen supply/demand relationship. Recommendations of maximum permitted
RPP range from 12,000 to 23,000 mmHg beats.minute-1 and values exceeding this are
commonly associated with myocardial ischaemia and angina118. The patient’s preoperative
level should however serve as a guide. Rao et al119 recommended that in the anaesthetic
management of patients with cardiac morbidity presenting for non-cardiac surgery, the
heart rate and systolic blood pressure and thus the RPP should not fluctuate beyond 20%
of the baseline value. Although RPP does not predict regional myocardial supply-demand
relationships, examination of the individual components (heart rate and systolic blood
pressure) is a useful guide in the management of ischaemic heart disease. Of the two
treatment techniques used in this study, esmolol was superior as it significantly attenuated
the heart rate, systolic blood pressure and rate-pressure product changes. However, the
28.06% rise in RPP recorded in the esmolol group still exceeds Rao's 20%
recommendation. This is however significantly superior to the 45.8% of the lidocaine
group and the 78.7% of the control group.
The transient decrease in RPP observed in the esmolol group following the administration
of the drug, correlate with those of Liu and colleagues who using esmolol to control

Page 17 of 85
haemodynamic responses associated with tracheal intubation, reported a decrease in RPP
prior to induction of anaesthesia120. As observed in the present study, Liu et al reported a
post intubation increase in RPP which was 50% less in the esmolol-treated patients
compared to the placebo group. However, Buffington121 was of the opinion that during
anaesthesia, myocardial ischaemia is poorly correlated with RPP. His advocacy of the
Pressure Rate Quotient (PRQ) as a more reliable index of myocardial ischaemia is disputed
by other workers.122
Apart from causing a transient decrease in heart rate and blood pressure following its
administration at induction, there were no adverse effects attributable to the use of esmolol
in this study. Miller et al97 showed that esmolol in doses of 1.5-3.0mg.kg -1 did not alter
stroke volume or depress left ventricular function in patients with preserved cardiac
function.
In this study, the adoption of different time intervals for administration of esmolol and
lidocaine i.e. 2 and 3 minutes respectively, may have introduced a possible source of bias
with respect to blinding. Review of available literature revealed that these doses and time
intervals were safe and produced consistent results with respect to attenuation of the pressor
response34,35,81,92. This bias was reduced by the use of an impartial observer (anaesthetist
registrar) who measured and recorded the haemodynamic data.
Thomson9 and Hung10 have questioned the clinical significance of the haemodynamic
responses associated with laryngoscopy and intubation and argue that the subject does not
deserve the attention it attracts. They are quick to point out that a transient increase in
arterial blood pressure and heart rate occurs in most of our daily activities and may not be
of any clinical importance. Hung10 argued that the interpretation of cardiovascular

Page 18 of 85
responses to anaesthetic drugs is difficult when a noxious intervention such as
laryngoscopic intubation introduces confounding variables such as magnitude and duration
of the noxious intervention as well as variables introduced by various medical conditions
such as cardiovascular diseases and diabetes mellitus. These he postulated, may explain
the inconsistent results reported in previous studies. In his experiment in which 21 healthy
volunteers were subjected to stress tests with continuous haemodynamic monitoring (intra-
arterial blood pressure and heart rate), he was able to demonstrate that haemodynamic
responses occur with normal daily activities and these responses are generally well
tolerated, provided they are short lived .
The clinical significance of the pressor response to laryngoscopy and intubation is most
important in the perioperative management of patients with cardiovascular diseases and
intracranial hypertension. Prys-Roberts et al17 found that hypertensive patients, whether
treated or untreated, are prone to much greater changes in arterial pressure (and thus RPP),
than normotensive patients of the same age group. They found that the excessive swings in
blood pressure observed in their patients, were accompanied by electrocardiograph (ECG)
evidence of myocardial ischaemia. In the hypertensive patient with normal left ventricular
function, the blood pressure falls at induction without a significant fall in heart rate; thus
maintaining left ventricular filling pressure and blood supply. Hence the incidence of
myocardial ischaemic changes in these patients is less than 6%. However, in the patient
with hypertensive heart disease and poor left ventricular function, the heart rate increases
following induction of anaesthesia, with a decrease in filling pressure and left ventricular
blood flow. The risk of ischaemic changes in these patients is almost as high as 33%103.
Urban et alix examined the relationship between several intraoperative haemodynamic

Page 19 of 85
variables, fixed cardiac risk factors, intraoperative myocardial ischaemia and postoperative
myocardial infarction (PMI) in a group of patients undergoing coronary by-pass graft
(CABG) surgery. They found that RPP > 12,000(beats.min-1.mmHg-1) was significantly
associated with pre-cardiopulmonary bypass (pre-CPB) myocardial ischaemia. In addition,
a pre-CPB electrocardiography ischaemia was significantly associated with a postoperative
myocardial infarction.
In an earlier editorial on the subject by Thomson9, several observations were made. He
noted that although researchers documented the haemodynamic changes accompanying
laryngoscopy and intubation, they gave no information on outcome. Thus, the influence of
their interventions on the incidence of perioperative cardiovascular morbidity and mortality
were unknown. Although he admitted that certain subgroups of patients (i.e. those with
symptomatic aortic aneurysm, recent myocardial infarction, cerebral aneurysm or
intracranial hypertension) required careful haemodynamic control during intubation of the
trachea, he noted that such patients were never included in the control group of studies
examining the efficacy of haemodynamic control during laryngoscopy and intubation. He
advocated that since myocardial infarction accompanying perioperative myocardial
ischaemia occurred between the second and fifth postoperative day, greater benefits will
be achieved if haemodynamic control is extended to cover the entire perioperative period,
rather than limited to two minutes following intubation9.
While making pertinent observations, Thompson appears to have ignored the ethical
aspects of such research. Withholding therapy from patients at risk in order to determine
outcome would raise a lot of questions with regards to ethics. Nonetheless, search of the
literature revealed a number of studies performed on patient populations at risk of

Page 20 of 85
developing perioperative complications such as the elderly, those with documented
coronary artery disease, vascular disease, hypertension, diabetes and obesity66,95,97. In these
studies, the duration of laryngoscopy and intubation was limited to 30 seconds to avoid
unduly endangering the patients in the control groups. Although the various researchers
did not advocate the routine use of these agents for all patients undergoing general
anaesthesia, they were recommended as useful adjuncts in patients at risk when it is
imperative to control haemodynamic responses to transient perioperative stimuli.
In this study, the unit costs of esmolol and lidocaine per patient were averagely N1, 700
($14.20) and N200 ($1.70) respectively which makes lidocaine more cost-effective to use
for attenuation of pressor responses to laryngoscopy and endotracheal intubationx. This is
particularly of significance in the face of dwindling health care resources and poor funding.
However, the use of more expensive drugs may be justified in susceptible groups of
patients if it will result in better perioperative management, reduced morbidity or an overall
reduction in length of hospital stay. Although esmolol is currently more expensive than
lidocaine, the observation in the past is that as patent rights expire, regularly used drugs
become cheaper and more readily available for use in Nigeria.
CONCLUSION
This study has confirmed that significant increases in haemodynamic variables accompany
laryngoscopy and endotracheal intubation following the widely utilized technique of
induction of anaesthesia with sodium thiopentone followed by suxamethonium for tracheal
intubation. These changes are maximal immediately after intubation, but return to baseline
values by 5 -10 minutes.
Neither drug deployed in this study completely abolished this response but it was

Page 21 of 85
attenuated to varying degrees. Intravenous lidocaine 1.5mg.kg-1 administered 3 minutes
before laryngoscopy significantly attenuated the heart rate and rate-pressure product
changes following laryngoscopy and intubation. Intravenous esmolol 2mg.kg -1 given 2
minutes prior to laryngoscopy was statistically superior to lidocaine as it significantly
attenuated all the cardiovascular changes. Comparing the results obtained in this study
with those conducted in Europe, North America and Asia in other patient groups,
intravenous esmolol had a significant effect in this African population as it significantly
attenuated every measured haemodynamic variable.
The use of these two agents in the doses deployed in this study was not associated with any
untoward effects.
Page 22 of 85
RECOMMENDATIONS
Based on the findings of this study, it is recommended that;
Greater efforts should be made by hospitals and relevant regulatory agencies to
make esmolol hydrochloride readily and cheaply available to anaesthetists
practicing in Nigeria for the control of periods of intense sympathetic stimulation
such as laryngoscopy and intubation. This would enhance perioperative patient
management and add on to the safety of anaesthetic practice.
Although not recommended for routine administration in all patients, esmolol is a
useful adjunct for use by anaesthetists involved in perioperative management of
patients with identifiable risk factors for coronary artery disease, hypertension or
hypertensive heart disease with preserved cardiac function as these patients are at
high risk for development of myocardial ischaemia and infarction following
laryngoscopy and intubation.
A dose of 2mgkg-1 esmolol administered 2 minutes before laryngoscopy is optimal
for attenuation of the pressor response.
The use of intravenous lidocaine at a dose of 1.5mgkg-1 given 3 minutes before
laryngoscopy should not be abandoned. However it should be reserved for use in
patients in whom beta blockers are contraindicated (reactive airway disease,

Page 23 of 85
diabetes mellitus, heart block, congestive cardiac failure and bradyarrhythmias i.e.
HR<60beats.minute-1) or where more effective agents are unavailable for use.
A combination of lower doses of esmolol and lidocaine may offer better control of
the pressor response in Nigerians and is worth evaluating in the future.
LIMITATIONS
This study had the following limitations.
1. All the patients received the same dose of oral diazepam premedication irrespective
of weight due to the available formulation of diazepam tablets. This may have
modified the observed pressor response as benzodiazepines are known to have a
moderating effect on intraoperative cardiovascular responses103.
2. Cardiac dysrhythmias and myocardial ischaemia are two well documented
consequences of the haemodynamic response to laryngoscopy4. Thus continuous
electrocardiogram (ECG) monitoring of leads II and V5 is highly desirable in a
study like this. The available continuous ECG monitors in this centre were
malfunctional at the time of data collection for this study.
3. Direct intra-arterial measurements which give continuous, beat-to-beat blood pressure
readings would have provided more precise information on the haemodynamic
changes and the effectiveness of the studied drugs in attenuating the pressor
response. Facilities for such monitoring are not available in this centre.
4. Several studies have established that the haemodynamic changes observed during
laryngoscopy and intubation are associated with corresponding increases in serum
adrenaline and noradrenaline levels 6,39,40 It would have been worth determining if

Page 24 of 85
any of the treatment techniques used in this study had an effect on the plasma
catecholamine levels. However, the unavailability of facilities for conducting such
biochemical assays in this centre as well as the cost implications of external analysis
precluded this.
REFERENCES
1 Menges JE, Crown LA. Doctor, which type of blade do you want to use now? A
brief history and review of direct laryngoscopy and laryngoscope blades. Am J Clin
Med 2005; 2(2):15-18.
2. Levitan RM. The “Difficult Airway” and Alternative Airway Devices in the
Emergency Setting. Acad Emerg Med 2001; 8(8):829-832.
3. Ng WA. Pathophysiological effects of tracheal intubation. Difficulties in tracheal
intubation, 1st edition. Bailer Tindall.1985; pp 12-35.
4. Reid LC, Brace DE. Irritation of the respiratory tract and its reflex effect on heart
rate. Surg Gynaecol Obstet 1940; 70:157-162.
5. King BD, Harris IC, Griefensestein EE. Reflex circulatory response ton direct
laryngoscopy and tracheal intubation performed during general anaesthesia.
Anesthesiology 1951; 12:556.
6. Derbyshire DR, Chielewski A, Fell D. Plasma catecholamine response to tracheal
intubation .Br J Anaesth 1983;55:855-858.

Page 25 of 85
7. Stoelting RK. Blood pressure and heart rate changes during direct laryngoscopy
and tracheal intubation; influence of duration of laryngoscopy with or without prior
lidocaine. Anesthesiology 1977; 47:381-384.
8. Bruder N, Ortega D, Granhil C. Consequences and prevention methods of
haemodynamic changes during laryngoscopy and intratracheal intubation. Ann Fr
Anaesth Reanim 1992; 11:57-71.
9. Thomson IR. The haemodynamic response to intubation: a perspective (Editorial).
Can J Anaesth 1989; 36: 367-369.
10. Hung O. Understanding haemodynamic responses to tracheal intubation .Can J
Anaesth 2001; 48:723-726.
11. Bruder N. Haemodynamic changes during laryngoscopy: Does it matter? J Postgrad
Med 2005;51(4):264-265
12. Fox EJ, Sklar GS, Hill CH. Complications related to the pressor response and
endotracheal intubation. Anesthesiology 1977; 47:524-525.
13. Saha U, Jaylalakshmi I. Pressor response and hypertension. Indian J Anaesth 2003;
47(6):443-449.
14. Erhun WO. Olayuwola G, Agbani EO, Omotoso NS. Prevalence of hypertension in
a university community in South West Nigeria. Afr J Biomed Research 2005;
8(1):15-19.
15. Osotimehin B, Rotimi C, Ataman S, McGee D, Cooper R. The prevalence of
hypertension in seven populations of West African origin. Am J Pub Health 1997;
87:155-156.

Page 26 of 85
16. Russel B, Anderton JL, Cormack JJC et al. Management of hypertension- a study
of hospital out patient practice. J R Coll Gen Pract 1990;33:221-227
17. Pry-Roberts C, Greene LT, Meloche R, Foex P. Studies of anaesthesia in relation
to hypertension. Haemodynamic consequence of induction and endotracheal
intubation. Br J Anaesth 1971; 43:531-536.
18. Goldman L, Caldera DL: Risks of general anaesthesia and elective operation in the
hypertensive patient. Anesthesiology 1979; 50:29-31.
19. Sear JW, Jewkes C, Foex P. Does the choice of antihypertensive therapy influence
haemodynamic responses to induction to induction, laryngoscopy and intubation.
Br J Anaesth 1994; 73(3):303-308.
20. Foex P, Sear J. The surgical hypertensive patient .Continuing Education in
Anaesthesia, Critical care and Pain 2004; 4(5):139-143.
21. Akinboboye O, Idris O, Akinkugbe O. Trends in coronary artery disease and
associated risk factors in sub-Saharan Africans. J Human Hypertens
2003;17(6):381-387.
22. Mensah GA. Ischaemic heart disease in Africa. Heart 2008; 94:836-843.
23. Kadiri S. Tackling cardiovascular disease in Africa. Br med J 2005;31:711-712
24. Finfer SR. Cadiovascular responses to tracheal intubation; a comparison of direct
laryngoscopy and fibreoptic intubation. Anaesth Intensive Care 1989; 17:44-48
25. Freidman PG, Rosenberg HK, Lebenard HM. A comparison of light wand and
suspension laryngoscopic intubation techniques in out-patients. Anesth Analg
1997; 85:578-582.

Page 27 of 85
26. Ojo OO. Cardiovascular response to laryngeal mask airway insertion or tracheal
intubation: normotensive versus hypertensive patients in Lagos University
Teaching Hospital. Dissertation submitted to the West African College of Surgeons
in part fulfilment of the requirement for the ward of the fellowship in Anaesthesia,
2002.
27. Kaul TK, Valech V, Kathuria S. Catecholamine responses to endotracheal
intubation and laryngeal mask airway insertion. Indian J Anaesth 1999; 43:30-35.
28. Tewari P, Gupta D, Kumar A. Opioid sparing during endotracheal intubation using
the McCoy laryngoscope in neurosurgical patients: the comparison of
haemodynamic changes with Macintosh blade in a randomised trial.
Anesthesiology 2005; 51(4):260-264.
29. Hamil JF, Bedford RF, Weaver DC, Colohan AR. Lidocaine before endotracheal
intubation: intravenous or laryngotracheal. Anesthesiology 1981; 55:578-581.
30. Mikawa K, Hasegawa M, Suzuki T. Attenuation of the hypertensive response to
tracheal intubation with nitroglycerine. J Clin Anaesth 1994; 4:367-371.
31. James MF, Esser ID. Intravenous magnesium sulphate inhibits catecholamine
release associated with tracheal intubation. Anesth Analg 1989; 68:772-776.
32. Koichi T, Yuji M, Osamu K. Tracheal lidocaine attenuates the cardiovascular
response to endotracheal intubation. Can J Anaesth 2001; 48:732-736.
33. Fassoulati A, Melemeni A, Petropoulos G. Gabapentin attenuates the pressor
response to direct laryngoscopy and tracheal intubation. Br J Anaesth 2006; 24:56-
58.

Page 28 of 85
34. Lev R, Rosen P. Prophylactic lidocaine use preintubation: a review. J Emerg Med
1994; 12:499-506.
35. Abou-madi MN, Kiezler H, Yacoub JM. Cardiovascular reactions to laryngoscopy
and intubation following small and large intravenous doses of lidocaine. Can J Anaesth
1977; 24:12-19.
36. Miller DR, Martineau RJ. Bolus administration of esmolol in controlling the
haemodynamic response to tracheal intubation. The Canadian Multicenter Trial. Can J
Anaesth 1999:8:133-135.
37. Forbes AM, Dally FG. Acute hypertension during induction of Anaesthesia and
endotracheal intubation in normotensive man. Br J Anaesth 1970; 42: 618.
38. Tomori Z, Widdecombe JG. Muscular, bronchomotor, and cardiovascular reflexes
elicited by mechanical stimulation of the respiratory tract. J Physiol 1969; 25: 200.
39. Shribman AJ, Smith G, Achola KJ. Cardiovascular and catecholamine responses to
laryngoscopy with and without tracheal intubation. Br J Anaesth 1989; 59:295-299.
40. Russel WJ, Morris RG, Frewi DB, Drew SE. Changes in plasma catecholamine
concentrations during endotracheal intubation. Br J Anaesth 1988; 53:837-839.
41. Yoo KY, Lee J, Kim HS, Im WM. Haemodynamic and catecholamine responses to
laryngoscopy and intubation in patients with complete spinal cord injuries.
Anesthesiology 2001; 95:647-651.
42. Dohi S, Nishikawa T, Ujike Y, Mayumi T. Circulatory response to airway
stimulation and cervical epidural blockade. Anesthesiology 1982; 57:359-363
43. Bonica JJ. Autonomic innervation o the viscera in relation to nerve block.
Anesthesiology 1968; 29:793-813.

Page 29 of 85
44. Landsberg L, Young JB. Cathecolamines and the adrenal medulla. In: Williams
Textbook of Endocrinology. Wilson JD(Ed). Philadelphia, Saunders; 1996, pp 621-
705.
45. Wathil M, Sundberg A, Olsson J, Nordstrom S. Thoracolumbar epidural
anaesthesia blocks the circulatory response to laryngoscopy and intubation. Acta
Anaesthesiol Scand 1987; 31:529-531
46. Durrani BM, Barwise JA, Johnson RF, Kambam JR. Intravenous chloroprocaine
attenuates haemodynamic changes associated with direct laryngoscopy and
tracheal intubation. Anesth Analg 2000; 90:1208-1212.
47. Derbyshire DR, Smith G, Achola KJ. Effect of topical lignocaine on the
sympathoadrenal responses to tracheal intubation. Br J Anaesth 1987; 59(3):300-
304
48 Amadasun FE. Study of the effectiveness of intravenous lidocaine in obtunding the
circulatory response to intubation. Nigerian Journal of Clinical Practices .Volume
3, No. 1, June 2000.
49. Thompson JP, Hall AP, Russel J. Effect of remifentanil on the haemodynamic
response to intubation. Br J Anaesth 1998; 80:467-469.
50. Albertini A, Casati A, Den F. Clinical comparison of either small doses of fentanyl
or remifentanil for blunting of cardiovascular changes induced by tracheal
intubation. Minerva Anestesiol 2000; 66:691-696.

Page 30 of 85
51. Dahlgren N, Messeter K. Treatment of stress response to laryngoscopy and
intubation with fentanyl. Anaesthesia 1987; 36:1022-1026.
52. Martin DE, Rosenberg H, Aukburg SJ et al. Low-dose fentanyl blunts circulatory
responses to tracheal intubation. Anesth Analg 1982; 61:680-684
53. Crawford DC, Fell D, Achoa KJ, Smith G. Effects of alfentanil on the pressor and
catecholamine responses to tracheal intubation. Br J Anaesth 1987; 59:707-712
54. Maguire AM, Kumar N, Parke JL et al. Comparison of effects of Remifentanil and
alfentanil on cardiovascular response to tracheal intubation in hypertensive
patients. Br J Anaesth 2001; 86:90-93
55. Achola KJ, Jones MJ, Mitchell RW, Smith G. Effects of beta-adrenoceptor
antagonism on the cardiovascular and catecholamine responses to tracheal
intubation. Anaesthesia 1988; 43(6):433-436.
56. McCamon RL, Hilgenberg JC, Stoetling RK. Effect of propranolol on circulatory
responses to induction of diazepam-nitrous oxide anaesthesia and to endotracheal
intubation. Anesth Analg 1981; 60:579-583.
57. Muhammad F, Butt HA, Abdul C. Management of cardiovascular stress responses
to laryngoscopy and tracheal intubation using esmolol hydrochloride. Ann King
Edward Med Coll 1999; 5:128-130.
58. Stoetling RK. Attenuation of the blood pressure response to laryngoscopy and
tracheal intubation with sodium nitroprusside. Anesth Analg 1879; 58:116-119.
59. Mikawa K, Obara H, Kusunoki M. Effect of nicardipine on the cardiovascular
response to tracheal intubation. Br J Anaesth 1990; 64:240-242.

Page 31 of 85
60. Yaku H, Mikawa K, Maekewa N. Effect of verapamil on the cardiovascular
responses to tracheal intubation. Br J Anaesth 1991; 68:85-89.
61. Yaku H, Mikawa K, Makawa N. Effect of verapamil on the cardiovascular
responses to tracheal intubation Br J Anaesth 1992;68:85-89
62. Wig J, Sharma M, Bauchoo N. Nicardipine and verapamil attenuate the pressor
response to laryngoscopy and intubation. Can J Anaesth 1994; 41:1185-1188
63. Kautto UM, Saarnivaara L. Attenuation of the cardiovascular intubation response
with nitrous oxide, halothane or enflurane. Acta Anaesthesiol Scand 1983; 27:289-
293.
64. Bedford RE, Marshall WK. Cardiovascular response to endotracheal intubation
during four anaesthetic techniques. Acta Anaesthesiol Scand 1984; 28:563
65. Ebegue AF. Second dose thiopentone attenuates the haemodynamic response to
laryngoscopy and intubation. Middle East J Anesthesiol 2001; 16(1):81-90
66. Amadasun FE. Comparison of the effectiveness of second dose thiopentone and
intravenous lignocaine for attenuating the pressure response to laryngoscopy and
intubation. The Niger Postgrad Med J 1999; 6(4):175-178.
67. Sood D, Nurula N, Katyal S, Saini S. Repeat dose of propofol; a prophylaxis against
the pressor response to laryngoscopy and tracheal intubation .J Anesthesiol Clin
Pharmacol 2002;18:304-308.
68. Ghignone M. Effects of clonidine on narcotic requirements and haemodynamic
response during induction of fentanyl anaesthesia and endotracheal intubation.
Anesthesiology 1986; 62:42-46.

Page 32 of 85
69. Scheinin B, Lindgren L, Randell T. Dexmetomidine attenuates sympathoadrenal
responses to tracheal intubation and reduces the need for thiopentone and
preoperative fentanyl. Br J Anaesth 1991; 68:126-131.
70. Amar D, Sharmoon H, Frishman WH et al. Effect of labetalol on perioperative
stress markers and isoflurane requirements. Br J Anaesth 1991; 67:296-301.
71. Puri GD, Maradachalam KS, Chari P. The effect of magnesium sulphate on
haemodynamics and its efficacy in attenuation the response to endotracheal
intubation in patients with coronary artery disease. Anesth Analg 1998; 87:808-
811.
72. Allen RW, James MFM, Uys PC. Attenuation of the pressor response to tracheal
intubation in hypertensive proteinuric pregnant patients by lidocaine, alfentanil and
magnesium sulphate. Br J Anaesth 1991; 66:216-223.
73. Fassoulaki A, Melemeni A, Paraskena A, Petropoulous G. Gabapentin attenuates
the pressor response to direct laryngoscopy and tracheal intubation. Br J Anaesth
2006; 96:769-773
74. Sanir S, Kumar D, Chabra B, Deepak K. Effect of oral captopril on the
haemodynamic responses to laryngoscopy and tracheal intubation. J Anaesthesiol
Clin Pharmacol 1996; 12(2):133-137.
75. Mikawa K, Maekawa N, Goto. Prostaglandin E1 and tracheal intubation:
relationship between the cardiovascular responses and plasma catecholamine
concentrations. J Intern Med Research 1991; 19:457-464.
76. Mikawa K, Maekawa N, Kaetsu H. Effects of Adenosine Triphosphate on the
cardiovascular response to tracheal intubation. Br J Anaesth 1991; 67:410-415.

Page 33 of 85
77. Yentis SM, Hirsch NP, Smith GB .Lidocaine Hydrochloride. Anaesthesia and
Intensive care A-Z: an encyclopaedia of principles and practice.3rd edition
.Butterworth and Heinemann 2004; 333.
78. Omoigui S. The anaesthesia drug handbook. 11th Edition. Mosby Year Book 1992;
pp 102-105.
79. Hines RS, Difazi O. Effect of lidocaine on the anaesthetic requirements for nitrous
oxide and halothane. Anesthesiology 1977; 47:437-440.
80. Phillips OC, Lyons WB, Harris LC. Intravenous lidocaine as an adjunct to general
anaesthesia: A clinical evaluation. Anesth Analg 1960; 39:317-322.
81. Tam S, Chung F, Campbell JM. Attenuation of circulatory responses to
endotracheal intubation using intravenous lidocaine: a determination of the optimal
time of injection. Can J Anaesth 1985; 32:565-569.
82. Splinter WM, Cervenko F. Haemodynamic responses to laryngoscopy and tracheal
intubation in geriatric patients: effects of fentanyl, lidocaine and thiopentone. Can
J Anaesth 1989; 36:370-376.
83. Miller CD, Warren SJ. Intravenous lidocaine fails to attenuate the cardiovascular
response to laryngoscopy and tracheal intubation. Br J Anaesth 1990; 65:216-219.
84. Laurito CE, Baughman VL, Polek VU. Aerosolised and intravenous lidocaine is no
more effective than placebo for the control of haemodynamic responses to
intubation. Anesthesiology 1987; 67:429.
85. Prys-Roberts, Foex P, Biro G: Studies of anaesthesia in relation to hypertension
versus adrenergic beta blockade. Br J Anaesth 1979; 45:671.

Page 34 of 85
86. Maharaj RJ, Thompson M, Williamson R. Treatment of hypertension following
endotracheal intubation: a study comparing the efficacy of labetalol, practolol and
placebo. S Afr Med J 1983, 63:691-694.
87. Menkhaus PG, Reeves JG, Kissin I et al. Cardiovascular effects of esmolol in
anaesthetised humans. Anesth Analg 1985; 64:327-334.
88. Devereaux PJ, Beattie WS, Choi PT, Badner NH. How strong is the evidence for
the use of perioperative beta blockers in non cardiac surgery? A systemic review
and meta-analysis of randomised controlled trials. Br Med J 2005; 331:313-321.
89. Angaran DM, Shultz NJ, Tschida VH. Esmolol Hydrochloride: an ultra short
acting, beta adrenergic blocking agent. Clin Pharmacol 1986; 5:288-303.
90. Gorczynski RJ. Basic Pharmacology of Esmolol. Am J Cardiol 1985; 56:3F-13F.
91. Yacoub A, Kartzinel R, Lai CM .Esmolol: a pharmacokinetic profile of a new
cardio selective beta –blocking agent. J Pharmacol Ther 1983; 73:710-711.
92. Sintetos AL, Hulse J, Pritchett EL. Pharmacokinetics pharmacodynamics of
esmolol administered as an intravenous bolus. Clin pharmacol Ther 1987; 41:112-
117.
93. Gold MI, Brown M, Coverman S, Herrington C. Heart rate and blood pressure
effects of esmolol after ketamine induction and intubation. Anesthesiology 1986;
64:718-723.
94. Ghaus MS, Singh V, Kumar A, Wahal R et al. A study of cardiovascular responses
during laryngoscopy and intubation and their attenuation by ultra short acting beta
blocker esmolol. Indian J Anaesth 2002; 46:104-106.

Page 35 of 85
95. Figueredo E, Garcia-Fuentes EM. Assessment of the efficacy of esmolol on the
haemodynamic changes induced by laryngoscopy and tracheal intubation: A meta-
analysis. Acta Anaesthesiol Scand 2001; 4:1011
96. Sheppard S, Eagle C, Strunin L. A bolus dose of esmolol attenuates tachycardia
and hypertension after tracheal intubation. Can J Anaesth 1990; 37(2):202-205.
97. Miller DR, Martineau RJ, Hull KA, Hill J. Bolus administration of esmolol for
controlling the haemodynamic response to laryngoscopy and intubation: efficacy
and effects on myocardial performance. J Cardiothorac Anaesth 1990; 4:31-36.
98. Tariq S, Aziz A, Waheed A. Attenuation of haemodynamic response to intubation
with esmolol. Presentation at the 3rd Saca Congress 1997.
99. Miller DR, Martineau RJ. Esmolol for control of haemodynamic responses during
anaesthetic induction. Can J Anaesth 1989; 36:164-165
100. Hussain AM, Sultan ST. Efficacy of fentanyl and esmolol in the prevention of
haemodynamic response to laryngoscopy and endotracheal intubation .J Clin
Anaesth 2005; 15(8):454-457.
101. Van den Berg AA, Honjol DN. Attenuation of the haemodynamic responses to
noxious stimuli in patients undergoing cataract surgery. A comparison of
magnesium sulphate, esmolol, lidocaine, nitroglycerine and placebo given with
induction of anaesthesia. Eur J Anaesthesiol 1997; 14(2)134-147.
102. Cucchiara RF, Benefiel DJ, Matteo RS, Dewood M. Evaluation of esmolol in
controlling increases in heart rate and blood pressure during endotracheal
intubation in persons undergoing carotid endarterectomy. Anesthesiology 1986;
65; 528-531.

Page 36 of 85
103. Oxorn D, Knox JD. Bolus doses of esmolol for the prevention of perioperative
hypertension and tachycardia. Can J Anaesth 1990; 37:206-209.
104. Rathore A, Gupta HK, Tanwar GL, Rehman A. Attenuation of the pressor response
to laryngoscopy and endotracheal intubation with different doses of esmolol. Indian
J Anaesth 2002; 40(6):449-452.
105. Bernstein JS. Single intravenous bolus esmolol prior to rapid sequence induction
effectively blunts the intubation response. Anesth Analg 1989; 68:24.
106. Helfman SM, Gold MI, DeLisser EA, Herrington CA. Which drug prevents
tachycardia and hypertension associated with tracheal intubation: lidocaine,
fentanyl or esmolol? Anesth Analg 1991; 72:482-6.
107. Feng CK, Chan KH, Liu KN, Or CH. A Comparison of lidocaine, fentanyl and
esmolol for attenuation of cardiovascular response to laryngoscopy and tracheal
intubation. Acta Anaesthesiol Sin 1996; 34:61-67.
108. Atkins RF. Prevention of tachycardia and hypertension associated with tracheal
intubation. Anesth Analg 1991,73:502-504
109. Levitt MA, Graham M. The efficacy of esmolol versus lidocaine to attenuate the
haemodynamic response to intubation in isolated head trauma patients. Acad
Emerg Med 2001; 1:19-24.
110. Kindler CH, Schumacher PG, Schneider MC. Effects of intravenous lidocaine
and/or esmolol on haemodynamic responses to laryngoscopy and intubation: A
double-blind, controlled clinical trial. J Clin Anaesth 1996; 8:491-496.

Page 37 of 85
111. Bansal S, Pawar M. Haemodynamic responses to laryngoscopy and intubation in
patients with pregnancy-induced hypertension: effect of intravenous esmolol with
or without lidocaine. Int J Obstet Anaesth 2002; 11(1):4-8.
112. Wilson IG, Meiklejohn BH, Smith G. Intravenous lignocaine and
sympathoadrenal responses to laryngoscopy and intubation. The effect of varying
time of injection. Anaesthesia 1991; 46:177-180.
113. Wang YM, Chung KC, Lu HF, Huang YM, Lin KC, Yang LC. Lidocaine: the
optimal timing of intravenous administration in attenuation of increase of
intraocular pressure during tracheal intubation. Acta Anaesthesiol Sin 2003;
41:71-75
114. Chraemmer-Jorgensen B, Hoilund-Carlsen PF, Marving J, Christen V. Lack of
effect of intravenous lidocaine on haemodynamic responses to rapid sequence
induction of general anaesthesia. Anesth Analg 1986; 65:1037-1041
115. White B. Heart rate and rate-pressure product as determinants of cardiovascular
risk in patients with hypertension. Am J Hypertens 1999; 12(2):508-518
116. Reiz S. Myocardial ischaemia associated with general anaesthesia: a review of
clinical studies. Br J Anaesth 1988; 6:68-84.
117. Corbett JL, Kerr JH, Prys-Roberts C. Cardiovascular responses to aspiration of
secretions from the respiratory tract in man. J Physiol (Lond) 1969:201:51
118. Amadasun FE. The relationship of age and the rate-pressure product (RPP)
response to endotracheal intubation. Afr J Anaesth and Intensive Care 2005; 6 (1):
12-15.

Page 38 of 85
119. Rao TLK, Jacobs KH. Reinfarction following anaesthesia in patients with
myocardial infarction. Anesthesiology 1983; 59:499-504.
120. Liu P, Gatt S, Gugino LD, Mallampati SR, Covino BG. Esmolol for control of
increases in heart rate and blood pressure during tracheal intubation after
thiopentone and succinylcholine .Can Anaesth Soc J 1986; 33:556-562
121. Buffington CW. Haemodynamic determinants of ischaemic myocardial
dysfunction in the presence of coronary stenosis in dogs. Anesthesiology 1985;
63:651-662.
122. Harris SN, Gordon MA, Urban MK et al. The pressure rate quotient is not an
indicator of myocardial ischaemia in humans. An echocardiographic evaluation.
Anesthesiology 1993; 78:242-250
123. Urban MK, Gordon MA, Harris SN. Intraoperative haemodynamic changes are not
good indicators of myocardial ischaemia. Anesth Analg 1993; 76:942-949
124. British National Formulary 47, 2006.

Page 39 of 85

Page 40 of 85
APPENDIX I
PROFORMA
ATTENUATION OF THE PRESSOR RESPONSE TO
LARYNGOSCOPY AND ENDOTRACHEAL INTUBATION: A
COMPARISION OF ESMOLOL AND LIDOCAINE
Name: Hospital No: Date:
Age: Sex: Weight:

Page 41 of 85
Height: Drug history: Diagnosis: Surgical
procedure: ASA score: Premedication:
Study Group : Group L ( )
Group E ( )
Group C ( )
Duration of laryngoscopy and intubation:
Parameters Baseline Pre-
Induction
Immediate
Post intubation Post Intubation
1 min 3mins 5mins 10mins
HR
SBP
DBP
MAP
RPP
HR = Heart rate, SBP = Systolic Blood Pressure, DBP = Diastolic Blood Pressure, MAP =
Mean Arterial Pressure, RPP = Rate Pressure Product.
Complications
Bradycardia
Bronchospasm
Hypotension
Tinnitus
Circumoral numbness
Pain on injection
Others (specify)

Page 42 of 85
APPENDIX II
PATIENT INFORMED CONSENT
TITLE OF THE STUDY: Attenuation of the pressor response to laryngoscopy and
endotracheal intubation: A Comparison of intravenous esmolol and lidocaine.
Page 43 of 85
INTRODUCTION
You are being approached because you are going to have elective surgery under general
anaesthesia. Laryngoscopy and endotracheal intubation are an integral component of
airway management during general anaesthesia. They have been shown to result in a rise
in heart rate, blood pressure and the occurrence of arrhythmias. This may have detrimental
effects in susceptible patients e.g. patients with ischaemic heart diseases, hypertension and
head injuries. Various drugs have been suggested to prevent these haemodynamic changes.
Esmolol and Lidocaine are two of such drugs.
PURPOSE AND DESCRIPTION OF STUDY
The aim of this study is to evaluate the effects of each drug and compare their effects in
preventing these haemodynamic changes. During the preoperative anaesthetic visit on the
ward, an anaesthetist will explain the study protocol, answer any questions you may have
and ask for a written informed consent.
In the operating theatre, according to our routine management, an intravenous infusion will
be set up in order to give you appropriate anaesthetic drugs. We will monitor your blood
pressure, heart rate and oxygen level as part of standard practice.
You will be assigned to one of three groups by balloting. The groups would be named
according to the study drug that will be used. The same drugs will be given to every patient
for induction of anaesthesia and maintenance of anaesthesia will be standard for every
patient.
POTENTIAL RISKS
Since the study drugs will be administered on a weight basis, with adequate consideration
given to maximum safe doses and contraindications to their use, the risk s involved in
participating in this study are minimal.
CONFIDENTIALITY
All information obtained during the study will be held in strict confidence

Page 44 of 85
CONSENT FORM
Signing this consent form does not wave your legal rights nor does it relieve the
investigators or this institution from legal and professional responsibilities.
CONSENT
I have had an opportunity to ask all necessary questions regarding the information of my
participation in this study and have received satisfactory answers. I understand that my
participation in this study is entirely voluntary. I, the undersigned, accept to participate
freely in this research project.
----------------------------------------------- ------------------------------
Patient’s name signature and date
----------------------------------------------- ------------------------------
Witness name signature and date

Page 45 of 85
ATTENUATION OF THE PRESSOR RESPONSE
TO LARYNGOSCOPY AND ENDOTRACHEAL INTUBATION: A
COMPARISON OF INTRAVENOUS ESMOLOL AND LIDOCAINE
Page 46 of 85
DR. A. A. EHIOZE-OSIFO
MBBS (Lagos) 1996, PGDA (Benin) 2001
DEPARTMENT OF ANAESTHESIA
LAGOS UNIVERSITY TEACHING HOSPITAL
IDI-ARABA, LAGOS.
1.







