
Australian e-Health Research Centre
Anthony Maeder
Professor in Health Informatics
University of Western Sydney
Health Services– a major focus for e-Health research

Australian e-Health Research Centre
Australian Healthcare “Vital Statistics”
• 2003/04 $78.6 billion which is 9.7% GDP • Governments fund 68% of this spend
• Health employs 570,000 people• Chronic workforce shortages
• Health sector growing at 5.5% per year• Hospital admissions up 9% (public), 30% (private) in 5 years• Prescriptions up 41% in 10 years

Australian e-Health Research Centre
Important Drivers in Healthcare
• Rapidly ageing population: over 65s will double 2004-2051• Chronic diseases: cancer and multiple co-morbidities• Diabetes and obesity: dramatic increases population-wide• New technologies increase costs: gene, stem cell, nanotech…
• Maintaining “hope and trust” on which all health care is based• Increased consumer expectations• Deployment of new models of care• Transforming data into knowledge

Australian e-Health Research Centre
Government Information Economy Strategy
A connected and responsive government• Meeting users needs• Establishing connected service delivery• Achieving value for money• Enhancing public sector capability
Issues for health• Privacy and security are paramount• Choice of service delivery models• Interoperability and data utilization• More informed consumers• Innovative technologies• Safety, Quality, Efficiency• Governance and accountability

Australian e-Health Research Centre
COAG Initiatives
National Health & Hospital Reform Commission
1. The Commission will provide advice on the framework for the next Australian Health Care Agreements, including robust performance benchmarks in areas such as elective surgery, aged and transition care and quality of care.
2. The Commission will report on a long-term health reform plan to provide sustainable improvements in the performance of the health system.

Australian e-Health Research Centre
COAG National Health Reform Plan Focus Areas
a. Reduce inefficiencies generated by cost-shifting, blame-shifting and buck passing
b. Better integrate and coordinate care across all aspects of the health sector, particularly between primary care and hospital services around key measurable outputs for health
c. Bring a greater focus on prevention to the health system
d. Better integrate acute services and aged care services and improve the transition between hospital and aged care
e. Improve frontline care to better promote health lifestyles and prevent and intervene early in chronic illness
f. Improve the provision of health services in rural areas
g. Improve Indigenous health outcomes
h. Provide a well qualified and sustainable health workforce into the future

Australian e-Health Research Centre
NeHTA
Over 3 – 5 years will implement:• National patient and provider identifiers• Snomed CT – global terminology for health data• Structured privacy framework• Shared e-health record system
Therefore new services will be needed for hospitals, doctors, state and federal health systems

Australian e-Health Research Centre
What is needed for Quality Healthcare?
Healthcare Quality is defined by several dimensions…• Safety
• Appropriateness
• Access
• Consumer centredness
• Effectiveness
• Efficiency
Health professionals need to have appropriate competencies to support this agenda
How does e-Health support this agenda?

Australian e-Health Research Centre
Health Services Approach
e-Health must help us deliver (as a minimum):• Shared e-health records • Decision support tools• Forecasting of patient flows• Ability to review pathways and compliance with guidelines• Modelling new service delivery processes and structures• Analysis of disease patterns and treatment responses

Australian e-Health Research Centre
Australian e-Health Research Strategic Areas
• Large scale data integration (e.g. federated databases)• Web services to facilitate data aggregation and analysis• Privacy / security / trusted storage and communications
Australian e-Health Research Centre
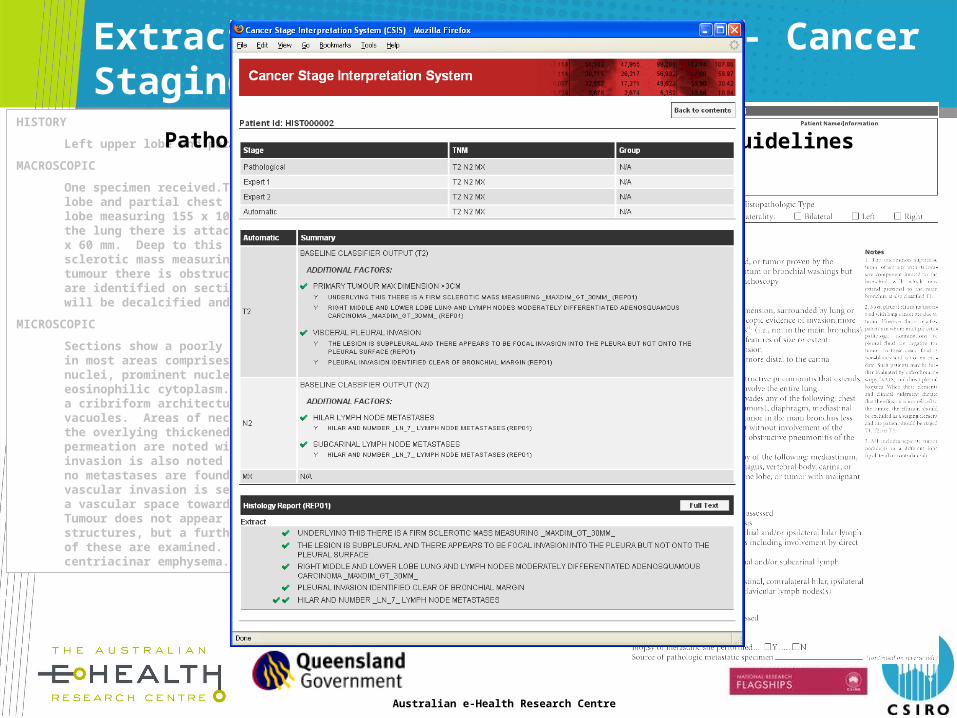
Extracting Meaning from Data - Cancer StagingHISTORY
Left upper lobe and partial chest wall.
MACROSCOPIC
One specimen received.The specimen is labelled "left upper lobe and partial chest wall" and consists of a left upper lobe measuring 155 x 100 x 45 mm. On the lateral aspect of the lung there is attached chest wall and ribs measuring 60 x 60 mm. Deep to this on sectioning, there is a white sclerotic mass measuring 45 x 42 x 40 mm. Surrounding the tumour there is obstructive pneumonitis. No other lesions are identified on sectioning of the lung. The chest wall will be decalcified and a further report will be issued.
MICROSCOPIC
Sections show a poorly differentiated adenocarcinoma which in most areas comprises sheets of large cells with vesicular nuclei, prominent nucleoli and moderate amounts of eosinophilic cytoplasm. Focally within the tumour there is a cribriform architecture and occasional cells contain mucin vacuoles. Areas of necrosis are present. Tumour invades the overlying thickened pleura and foci of lymphatic permeation are noted within this pleural tissue. Lymphatic invasion is also noted within pulmonary parenchyma. However no metastases are found in peribronchial lymph nodes. No vascular invasion is seen, although thrombus is noted within a vascular space towards the inferior aspect of the tumour. Tumour does not appear to extend up to chest wall structures, but a further report will follow when sections of these are examined. Distant lung parenchyma shows mild centriacinar emphysema.
Pathology Report Staging Guidelines

Australian e-Health Research Centre
Enhancing Data - SNOMED CT Usage
Australian e-Health Research Centre
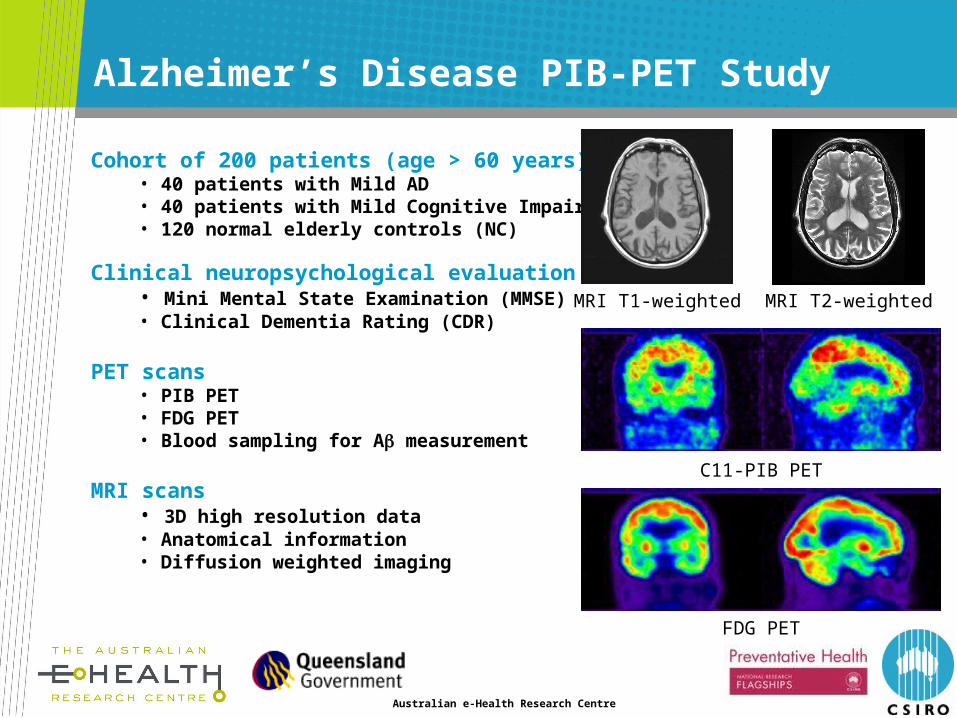
Alzheimer’s Disease PIB-PET Study
Cohort of 200 patients (age > 60 years)• 40 patients with Mild AD• 40 patients with Mild Cognitive Impairment (MCI)• 120 normal elderly controls (NC)
Clinical neuropsychological evaluation• Mini Mental State Examination (MMSE)• Clinical Dementia Rating (CDR)
PET scans• PIB PET• FDG PET• Blood sampling for A measurement
MRI scans• 3D high resolution data• Anatomical information• Diffusion weighted imaging
MRI T1-weighted MRI T2-weighted
C11-PIB PET
FDG PET

Australian e-Health Research Centre
Australian e-Health Research Strategic Areas
• Large scale data integration (e.g. federated databases)• Web services to facilitate data aggregation and analysis• Privacy / security / trusted storage and communications
• Telemedicine tools• Skills training tools• Machine learning tools

Australian e-Health Research Centre
Building Cases from CT images
From 3D CT…. …. to colon model

Australian e-Health Research Centre
Comparison of real and simulated colonoscopy
Real colonoscopy CSIRO simulated colonoscopy

Australian e-Health Research Centre
Integration of Haptic Device into Simulator

Australian e-Health Research Centre
Australian e-Health Research Strategic Areas
• Large scale data integration (e.g. federated databases)• Web services to facilitate data aggregation and analysis• Privacy / security / trusted storage and communications
• Telemedicine tools• Skills training tools• Machine learning tools
• Image analysis • Sensor enabled environments• In depth skills in maths, stats, visual analytics etc. for
Healthcare system modeling and prediction

Australian e-Health Research Centre
Efficient Management of Inpatient Beds
Inpatient beds = elective admissions + acute care episodes
Project premise:
EDs may seem chaotic, but admissions are predictable.

Australian e-Health Research Centre
Analysing ED Presentations 2002-2007
Toowoomba:
(Pop Growth 1.3%)
Gold Coast:
(Pop Growth 3.3%)
Sun Mon Tue Wed Thu Fri Sat80
90
100
110
120
130
140
150
Day of weekT
oow
oom
ba D
aily
Pre
sen
tati
ons
Profile (mean & 95%CI)
10 20 30 40 50 6080
90
100
110
120
130
140
150
Month of Analysis
Too
woo
mba
Da
ily P
rese
nta
tio
ns
Profile (mean & 95%CI)
Sun Mon Tue Wed Thu Fri Sat110
120
130
140
150
160
170
180
190
200
Day of week
Gol
d C
oa
st D
aily
Pre
sen
tati
on
s
Profile (mean & 95%CI)
10 20 30 40 50 60110
120
130
140
150
160
170
180
190
200
Month of Analysis
Gol
d C
oa
st D
aily
Pre
sen
tati
on
s
Profile (mean & 95%CI)

Australian e-Health Research Centre

Australian e-Health Research Centre
Comparison to Existing Prediction Modelling
• Existing Predictions vs New Model
Modelling for Periods % Error with Existing Predictions
%Error with New Model
12/7/06 – 20/5/07 (n=171 days)
20.5% 11.1%
12/7/06 – 9/9/07 (n=261 days)
19.1% 11.1%
12/7/06 – 20/1/08(n=335 days)
30.4%(effect of opening new ED wing)
11.8%








