Download - Bicuspid aortic valve

BICUSPID AORTIC VALVE
By Jyotindra Singh
adult cardiothoracic

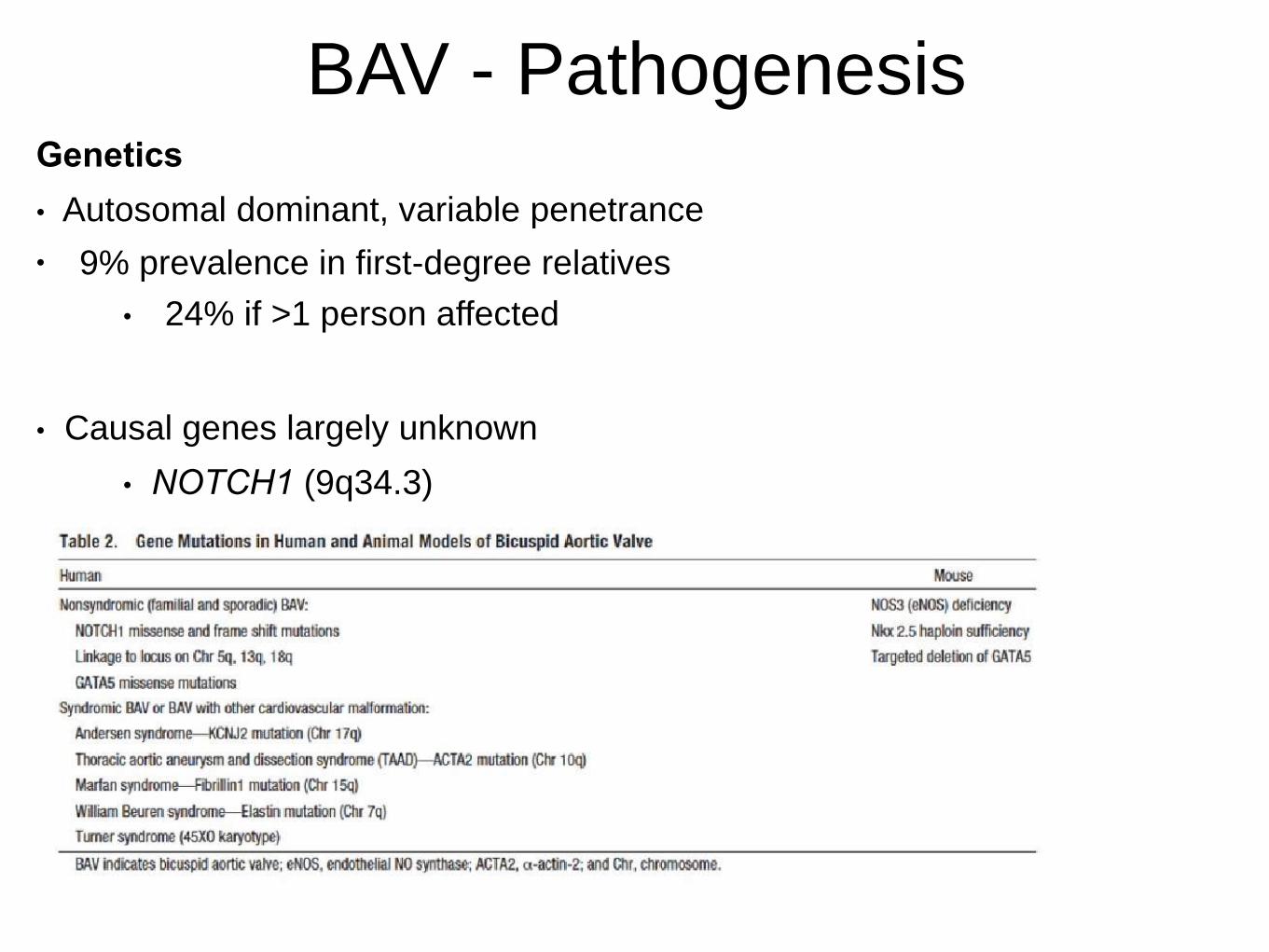
BAV - PathogenesisGenetics
• Autosomal dominant, variable penetrance
• 9% prevalence in first-degree relatives
• 24% if >1 person affected
• Causal genes largely unknown
• NOTCH1 (9q34.3)






BAV - Diagnosis
Transthoracic Echo
• Sensitivity 92%, Specificity 96%
• Accuracy inverse to calcification
• Findings:
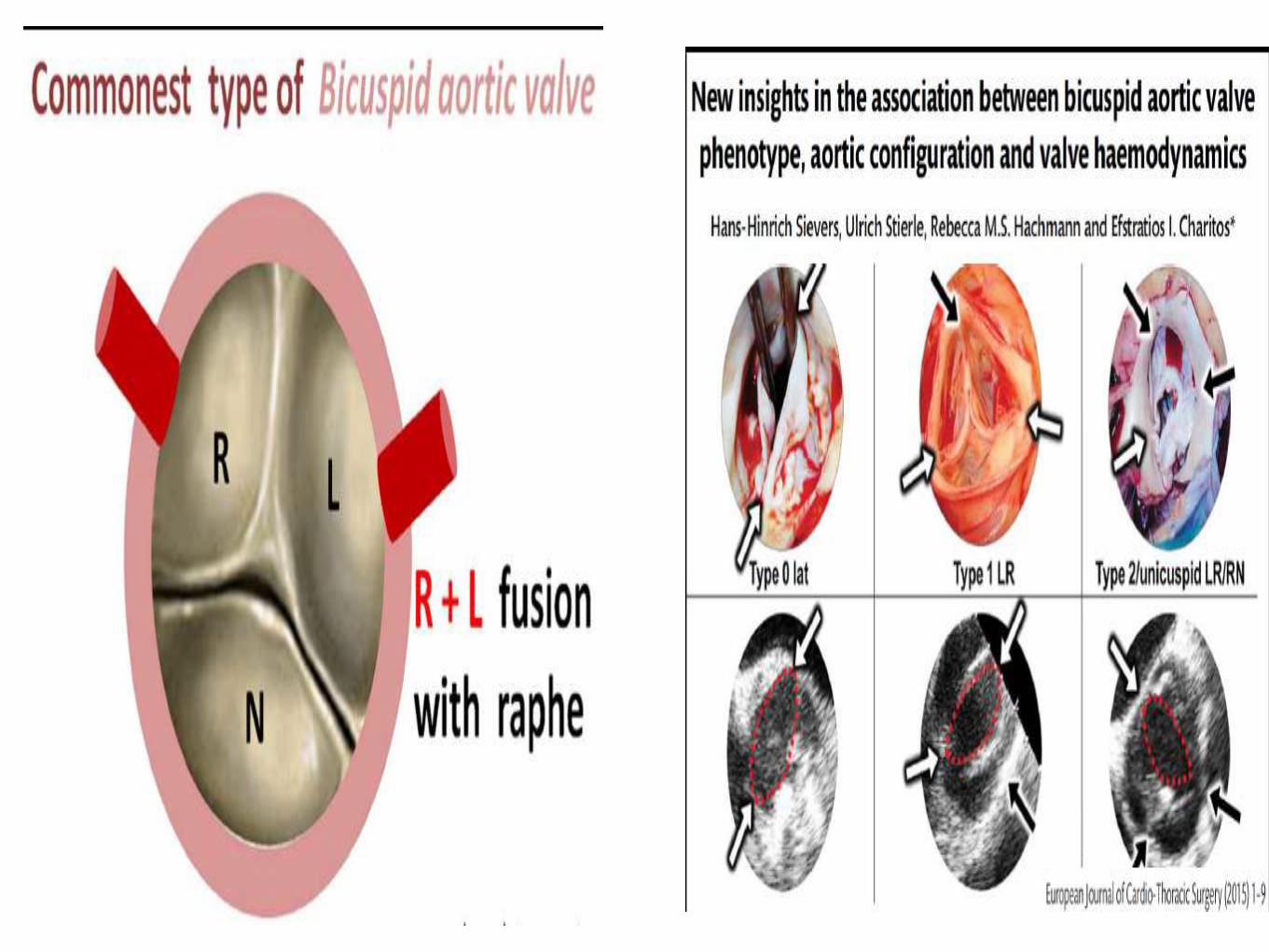
• Raphe
• Systolic doming & eccentric closure line
(LAX)
• Evaluate in systole; raphe may appear
trileaflet
Diastole Systole
Raphe
Doming
BAV - Natural History
• Valvular dysfunction - AS, AR, endocarditis
• Aortopathy
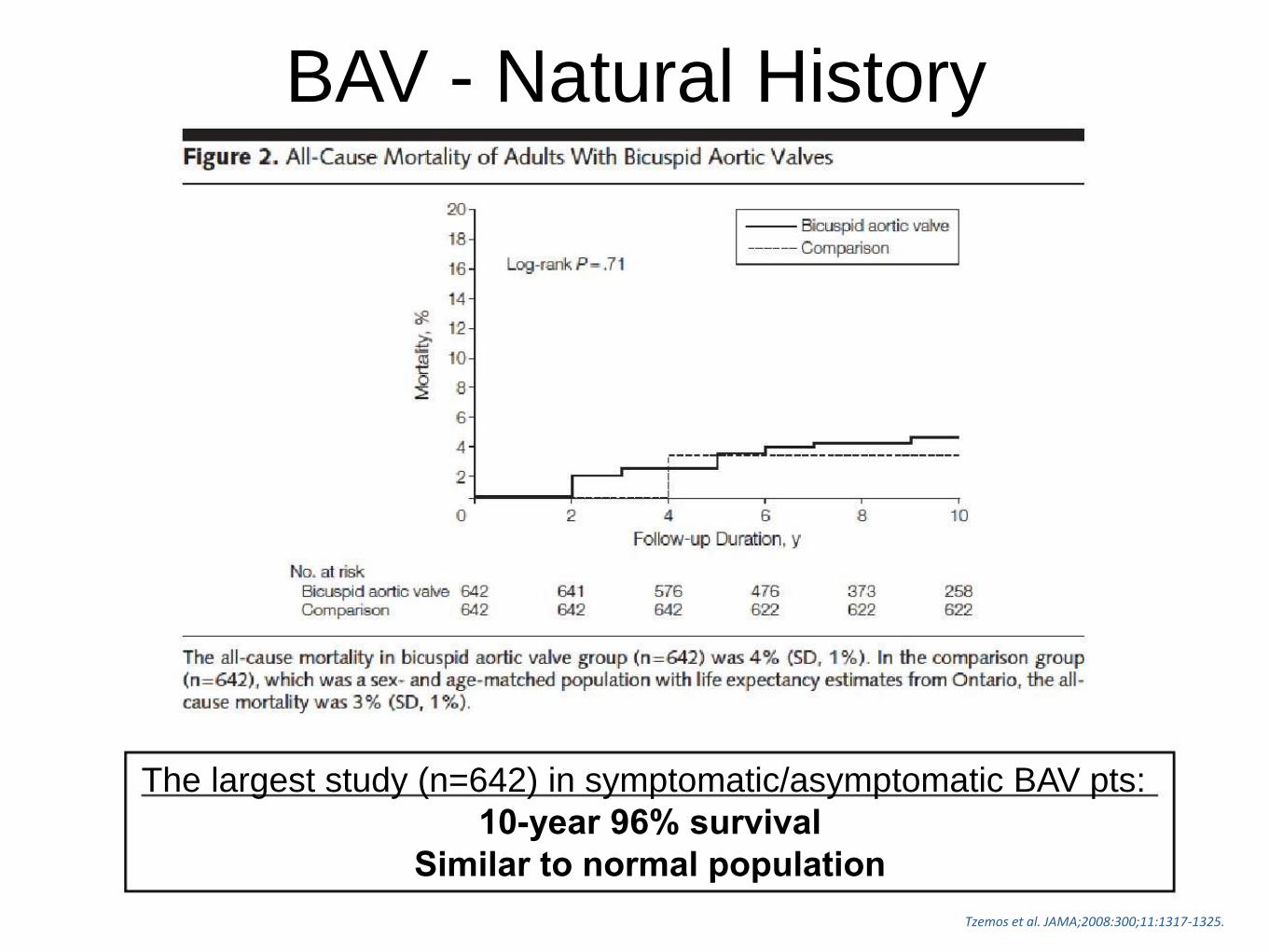
BAV - Natural History
The largest study (n=642) in symptomatic/asymptomatic BAV pts:
10-year 96% survival
Similar to normal population
Tzemos et al. JAMA;2008:300;11:1317-1325.

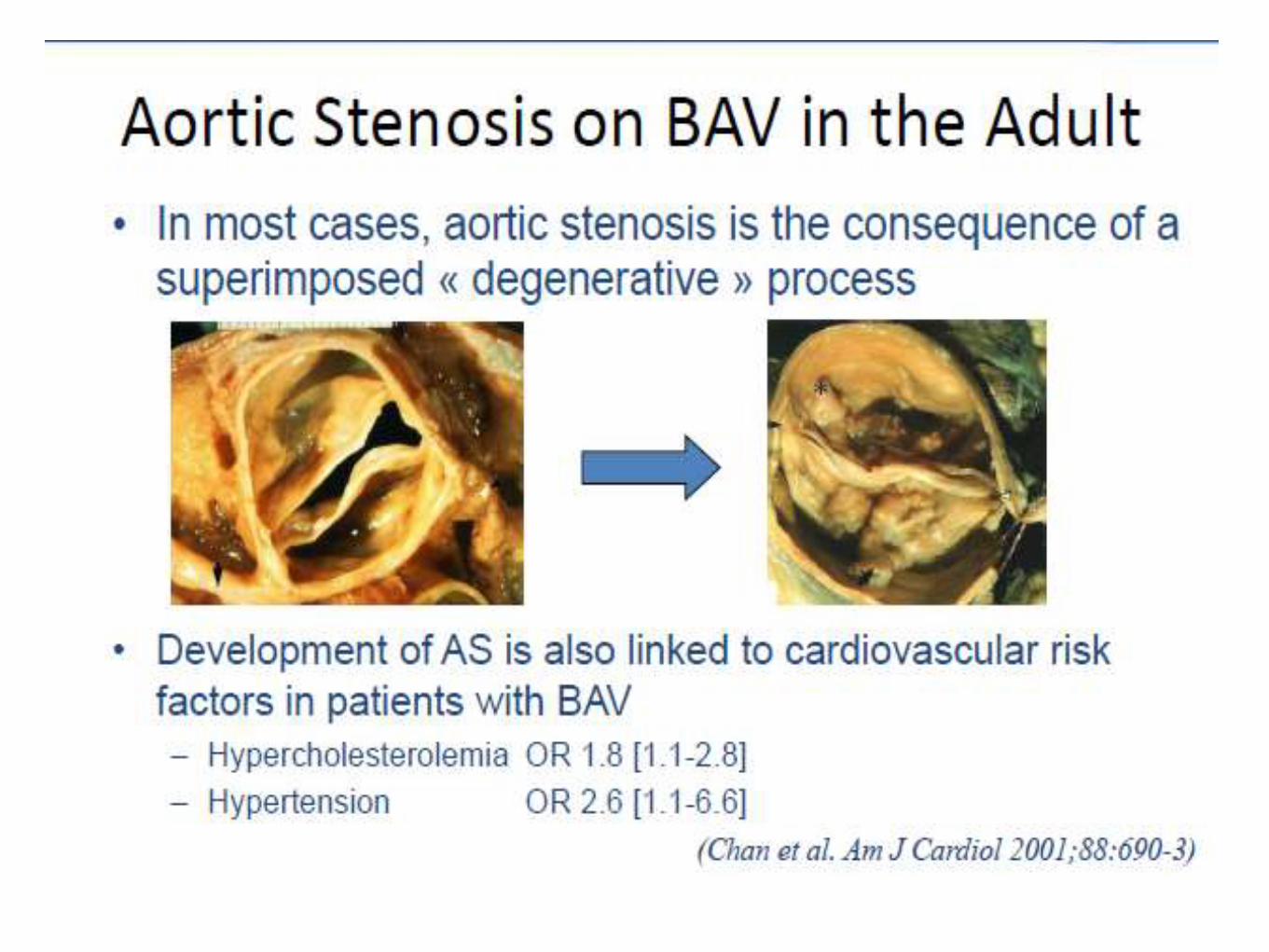
BAV - AS
Surgical series of 932 resected aortic valves for AS:
• 49% had BAV
• Age at intervention
• BAV: 67±11
• Tricuspid: 74±8
Roberts et al. CirculaGon. 2005;111:920-925.

BAV - AS
Disease progression
• Similar degenerative changes as seen in tricuspid
valves
• Exacerbated by BAV folding/creasing/turbulent flow
• Results in accelerated disease progression
• Most common reason for valve replacement
Roberts et al. CirculaGon. 2005;111:920-925.
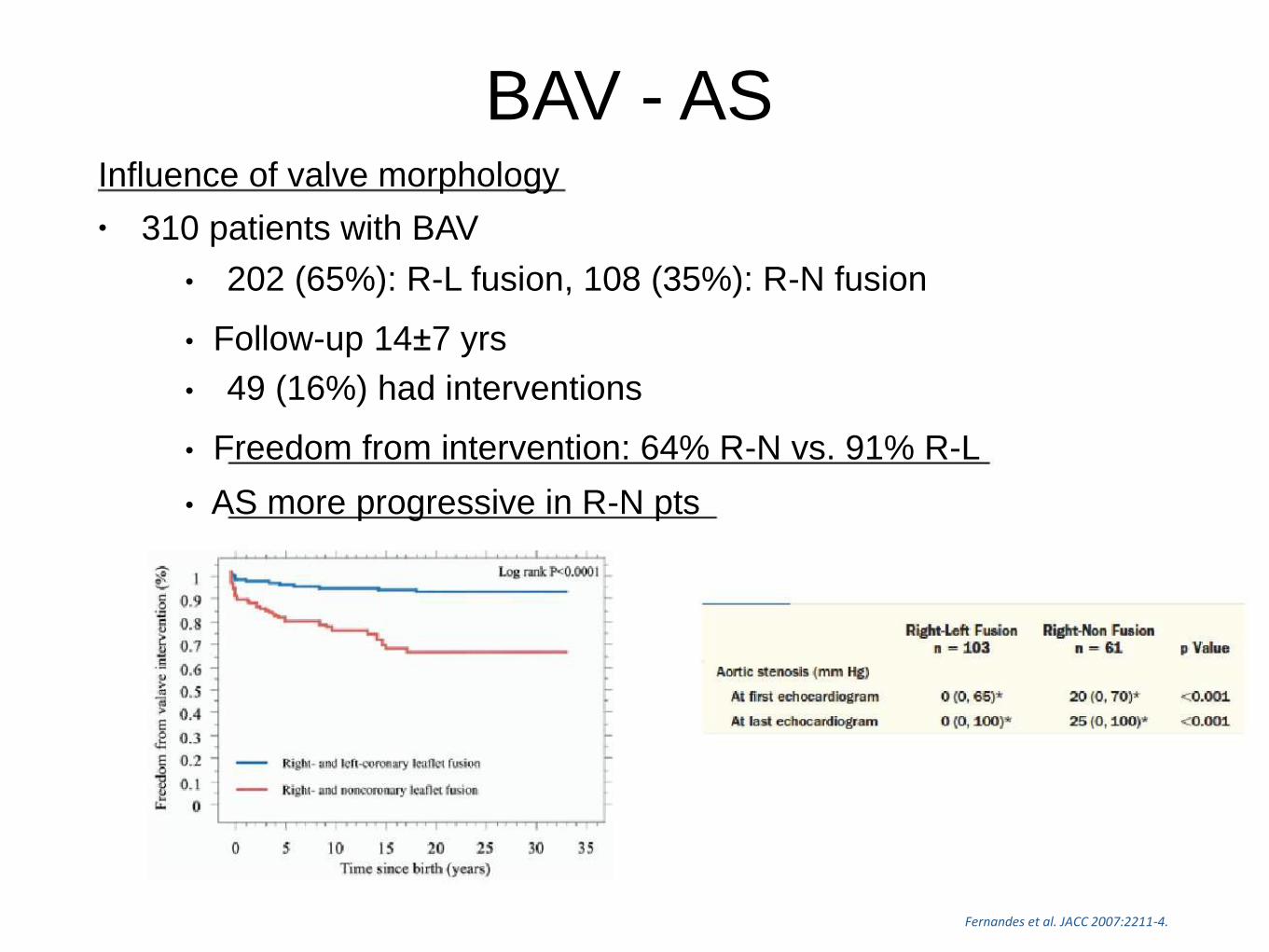
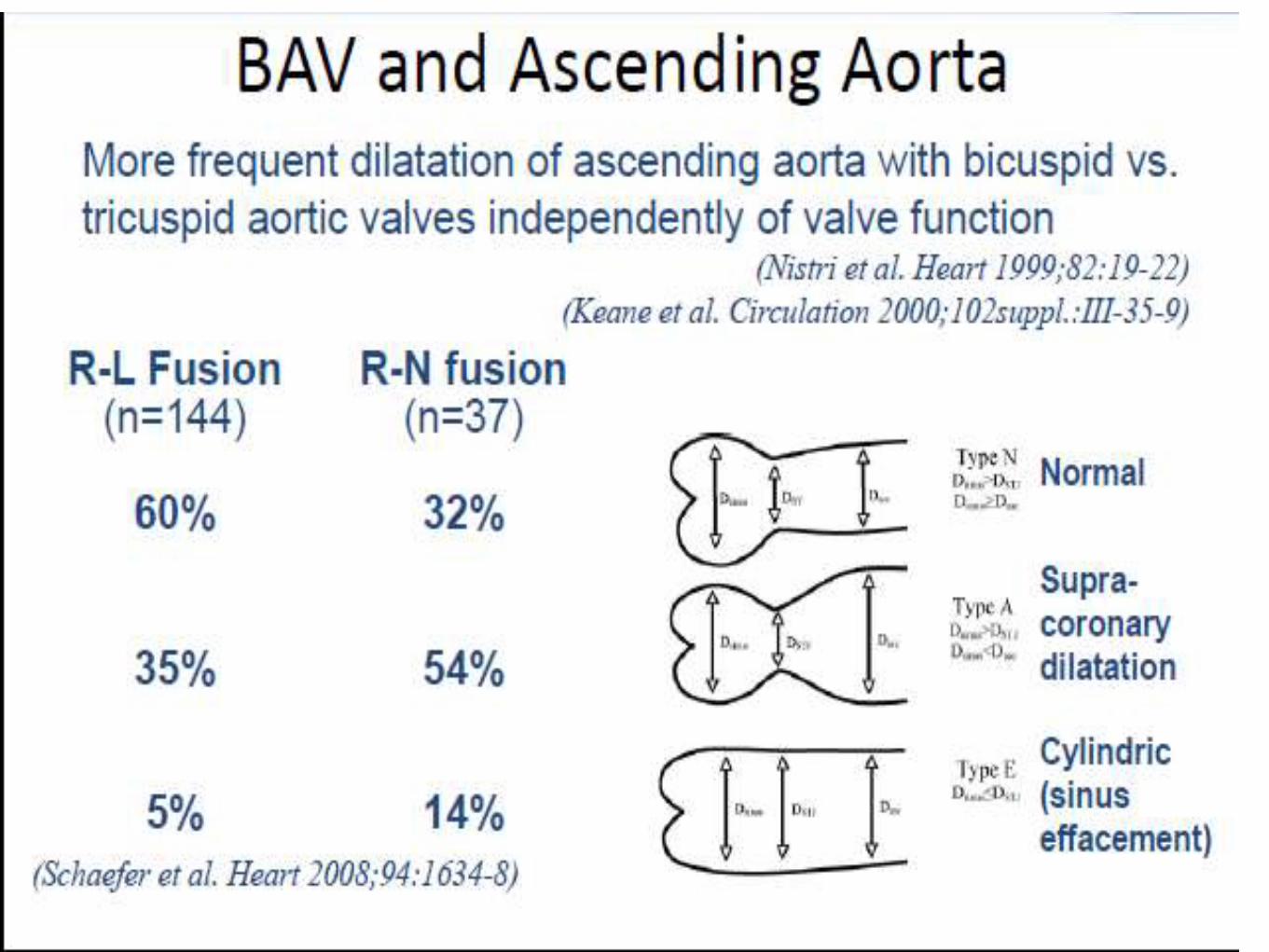
BAV - ASInfluence of valve morphology
• 310 patients with BAV
• 202 (65%): R-L fusion, 108 (35%): R-N fusion
• Follow-up 14±7 yrs
• 49 (16%) had interventions
• Freedom from intervention: 64% R-N vs. 91% R-L
• AS more progressive in R-N pts
Fernandes et al. JACC 2007:2211-4.

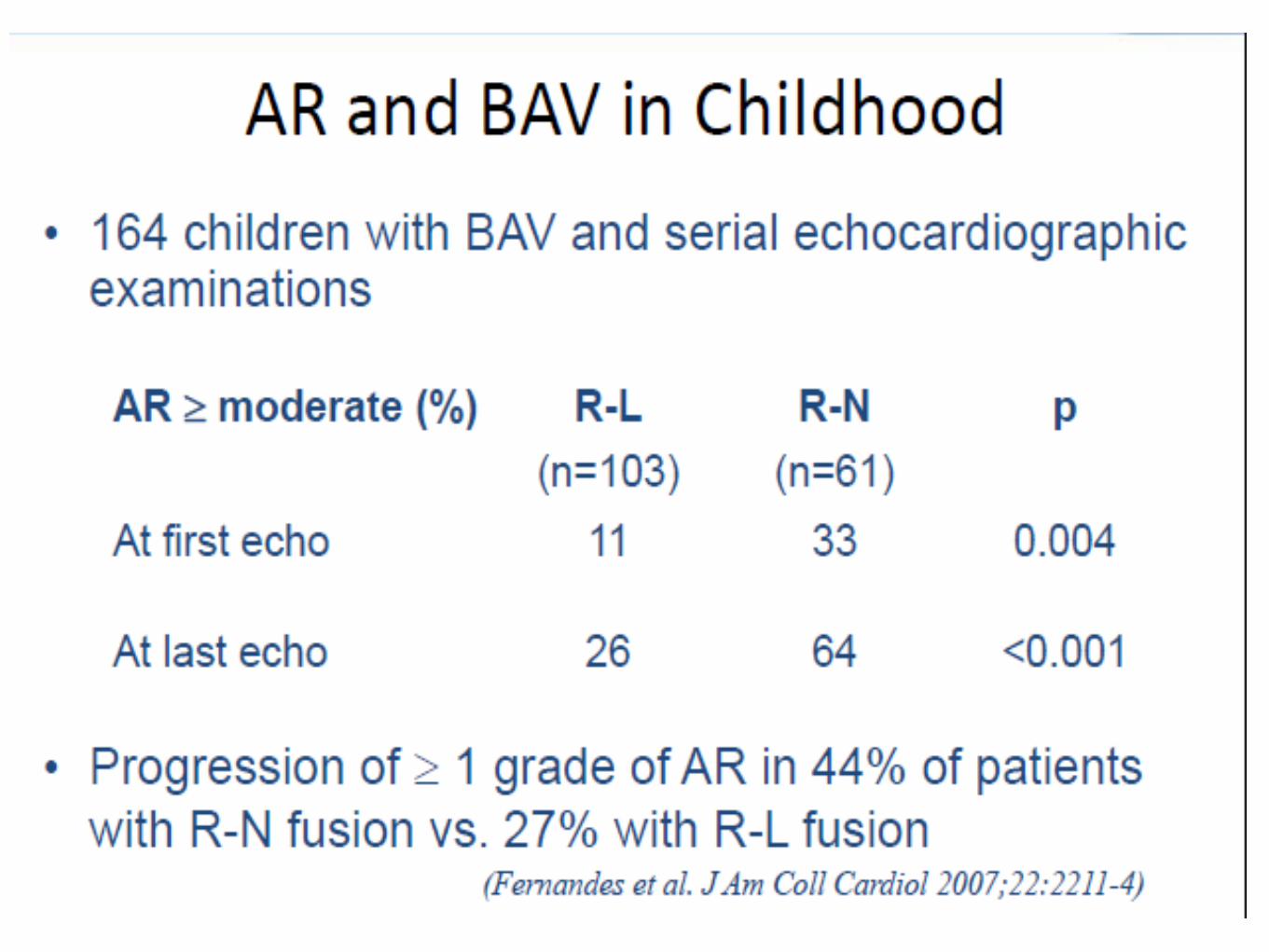
BAV - ARLess frequent occurrence than AS
• Surgical series of 542 pts who underwent AVR (1991-1996):
• 13% (pure AR) vs 75% (pure AS)
• Mean age:
• 46 yrs (AR) vs 65 yrs (AS)
Low intervention rates
• Olmsted county (Michelena): 47% had some degree of AR at baseline; 3% had
intervention for severe AR
• Toronto study (Tzemos): 21% had moderate/severe AR at baseline; 6% had
intervention for symptomatic AR
Mechanisms
• Valve prolapse
• Aortic root/annular dilatation
• Endocarditis
.)

BAV - Endocarditis
Recent studies suggest low incidence:
• Olmsted county:
• 2% per year incidence
• Toronto study:
• 0.3% per year incidence
AHA guidelines no longer suggest bacterial endocarditis
prophylaxis, except if prior history of endocarditis.
Tzemos et al. JAMA;2008:300;11:1317-1325Michelena et al CirculaGon. 2008;117:2776-2784.)

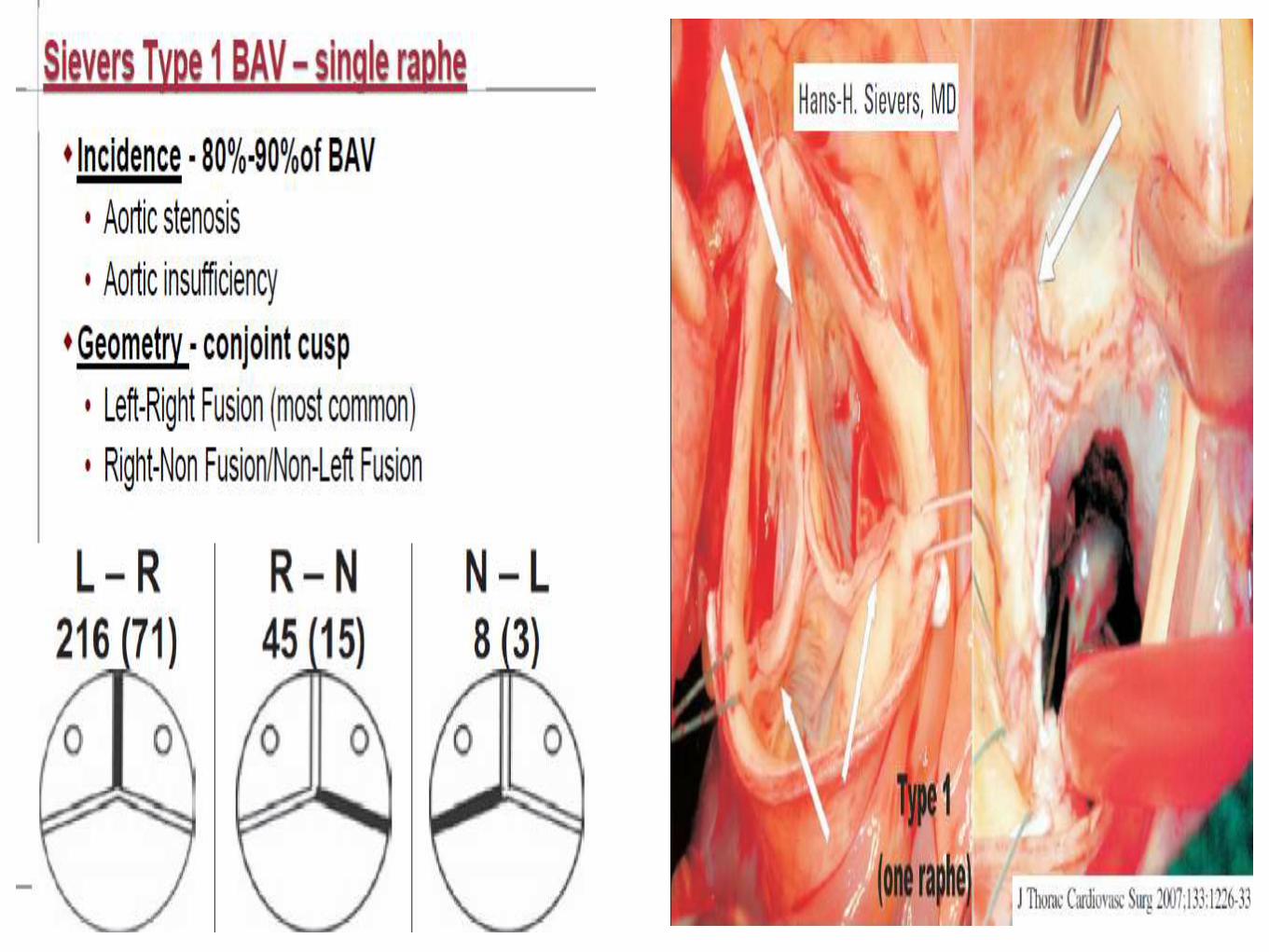
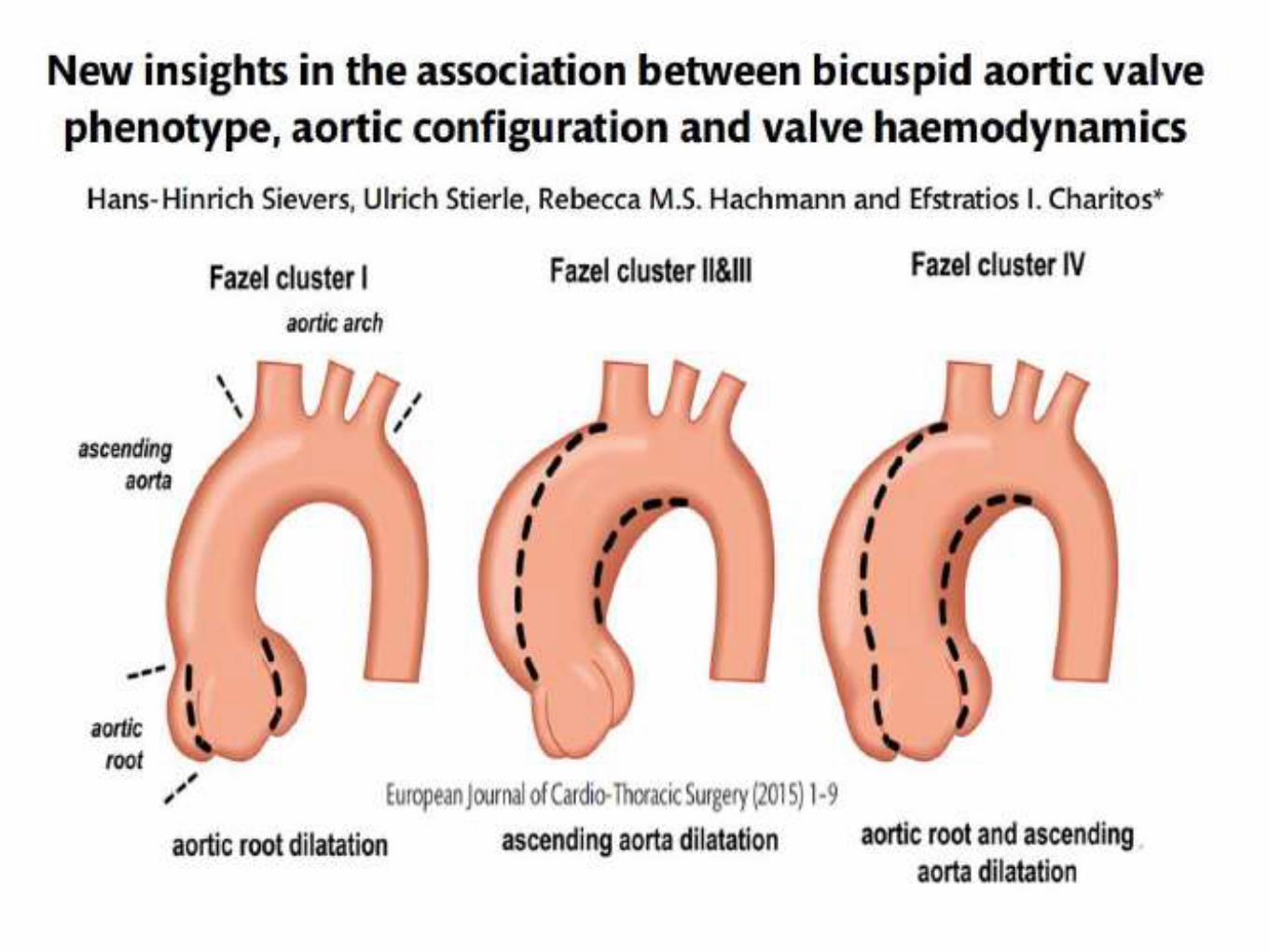
BAV - AortopathyPatterns of Aortic Dilation
Type 1: Dilation of tubular ascending aorta primarily
along convexity with mild-moderate root dilation.
Most common; associated with R-L cusp fusion & AS
Type 2: Isolated tubular ascending aorta dilation,which may extend into the arch, with relative sparing of
aortic root.
Associated with R-N cusp fusion.
Type 3: Root phenotype - isolated root dilation, normal
tubular/arch dimensions.
Rarer; associated with younger age at diagnosis;
genetic.

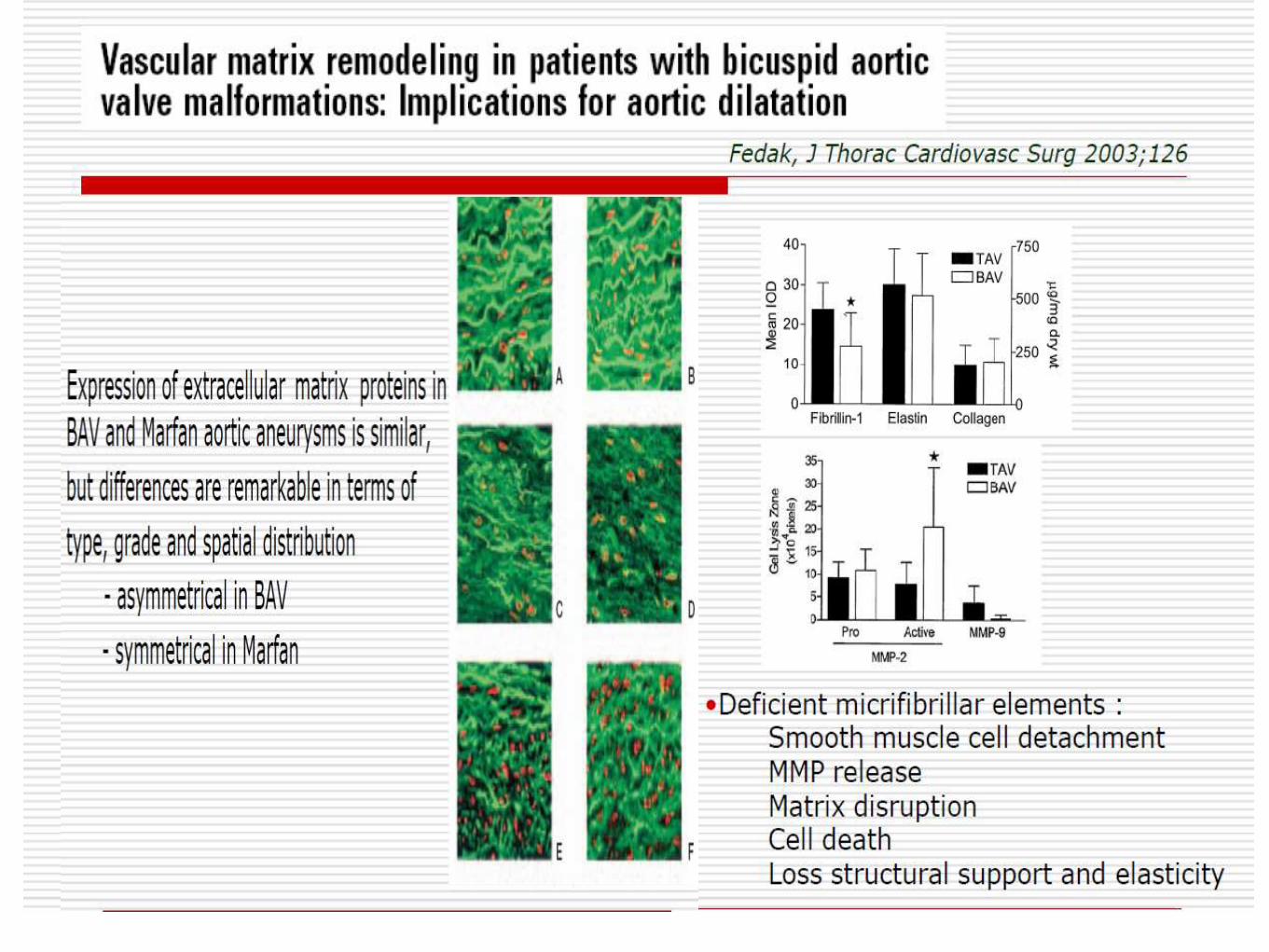
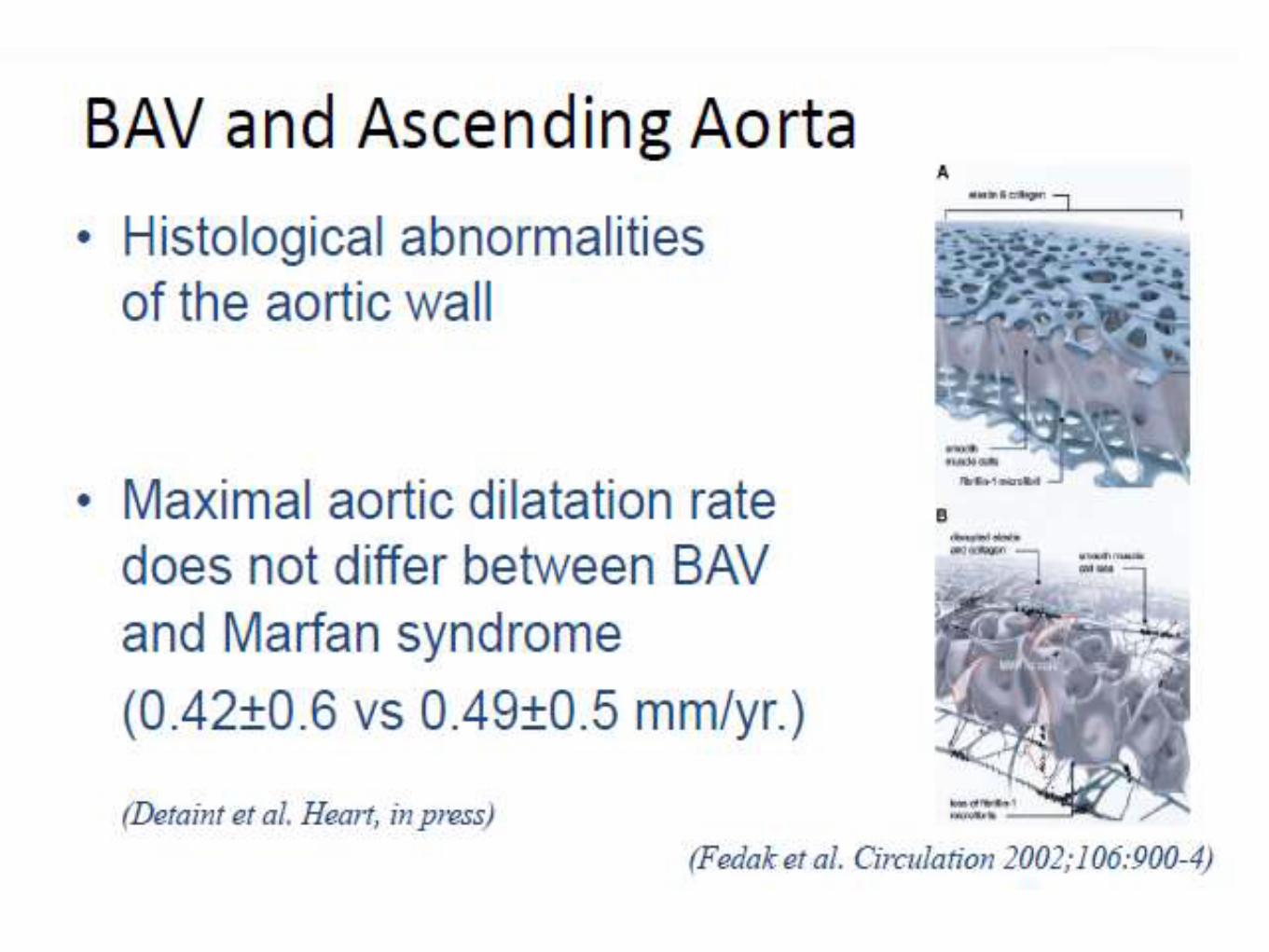
BAV - AortopathyPathophysiology
Haemodynamic evidence
Recent MRI studies -
• Abnormal transvalvular-flow patterns despite apparent normally
functioning BAVs
• Regional increases in wall-shear stress
However, valve morphology did not predict events in population studies
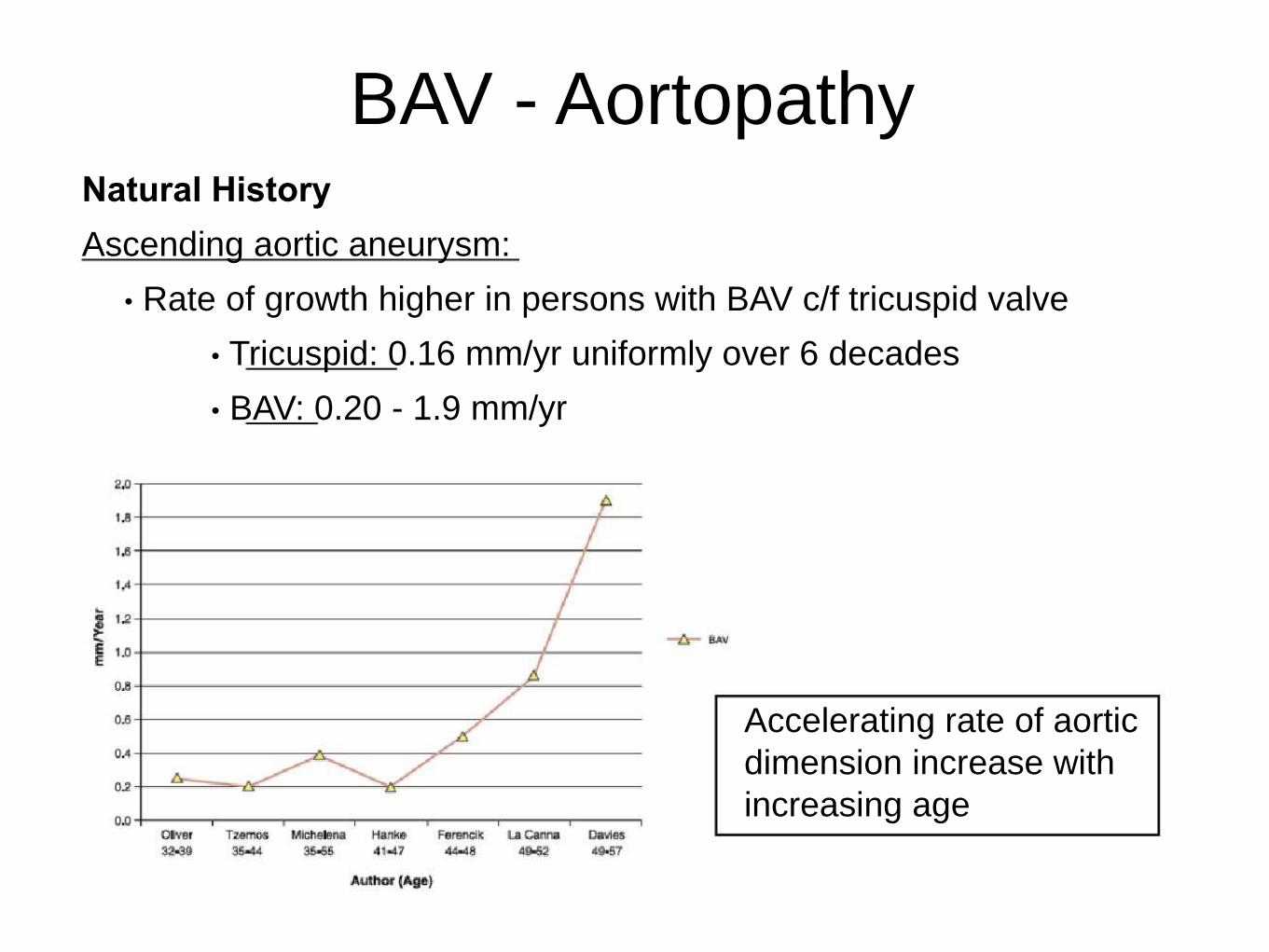
BAV - AortopathyNatural History
Ascending aortic aneurysm:
• Rate of growth higher in persons with BAV c/f tricuspid valve
• Tricuspid: 0.16 mm/yr uniformly over 6 decades
• BAV: 0.20 - 1.9 mm/yr
Accelerating rate of aortic
dimension increase with
increasing age
BAV - ManagementAHA 2014: Surgical Intervention
Class 1
Diameter of the aortic sinuses or ascending aorta is greater than 5.5 cm [B]
Class 2a
Diameter of the aortic sinuses or ascending aorta is greater than 5.0 cm and a
risk factor for dissection is present (family history of aortic dissection or if the
rate of increase in diameter is 0.5 cm per year) [C]
Replacement of the ascending aorta is reasonable in patients with a bicuspid
aortic valve who are undergoing aortic valve surgery because of severe AS or
AR if the diameter of the ascending aorta is greater than 4.5 cm. [C]
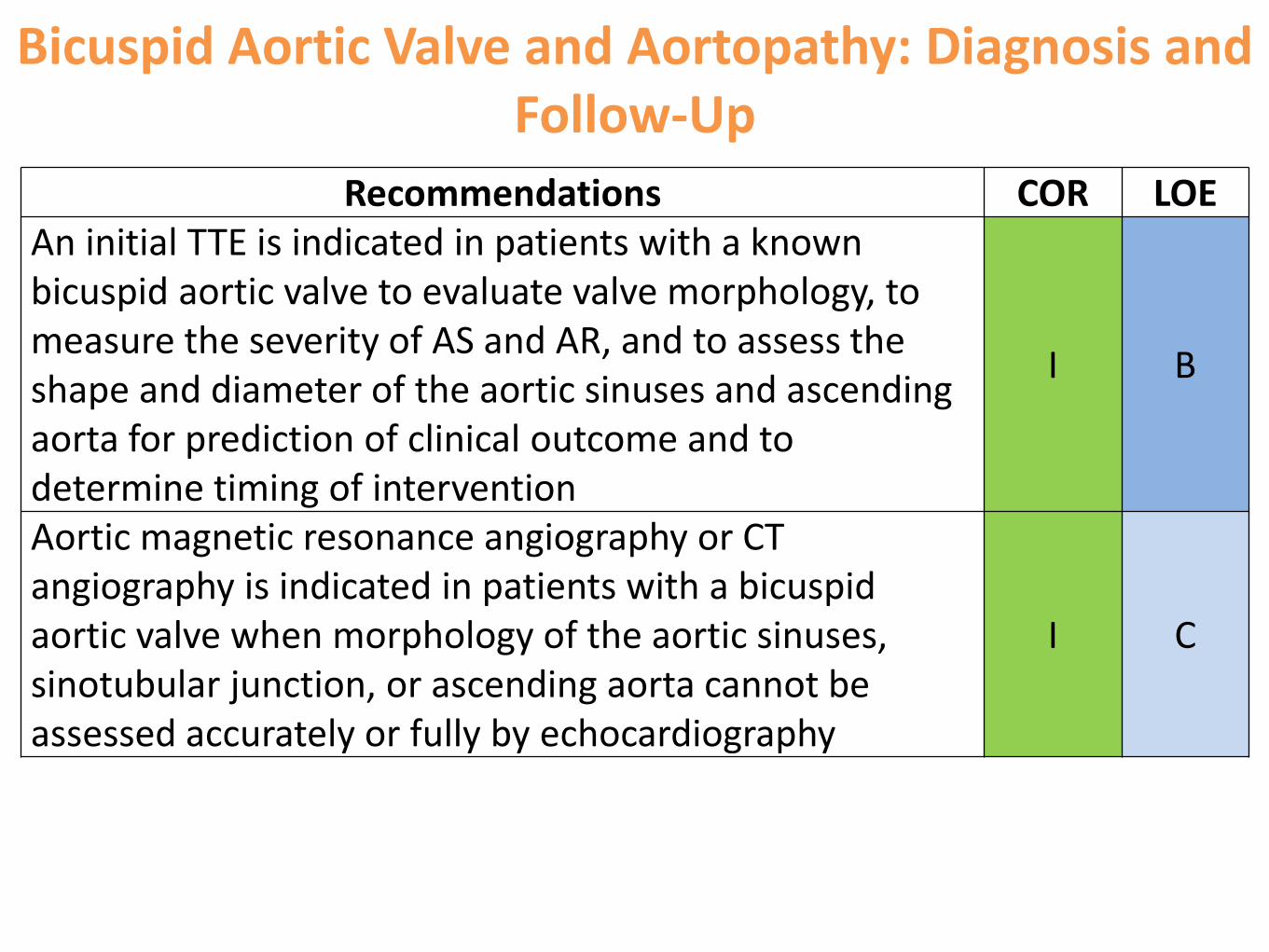
Bicuspid Aortic Valve and Aortopathy: Diagnosis and Follow-Up
Recommendations COR LOEAn initial TTE is indicated in patients with a known bicuspid aortic valve to evaluate valve morphology, to measure the severity of AS and AR, and to assess the shape and diameter of the aortic sinuses and ascending aorta for prediction of clinical outcome and to determine timing of intervention
I B
Aortic magnetic resonance angiography or CT angiography is indicated in patients with a bicuspid aortic valve when morphology of the aortic sinuses, sinotubular junction, or ascending aorta cannot be assessed accurately or fully by echocardiography
I C
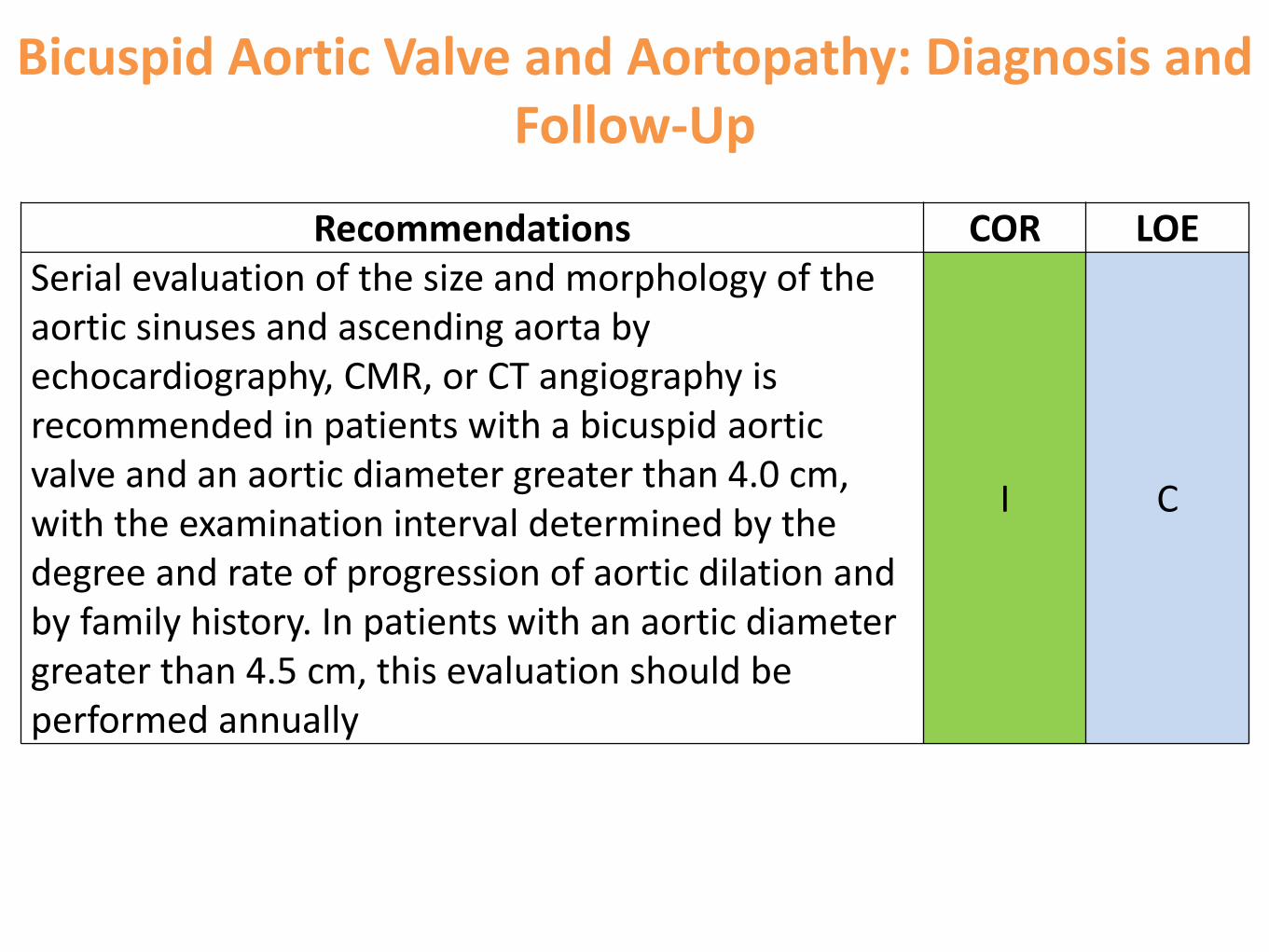
Bicuspid Aortic Valve and Aortopathy: Diagnosis and Follow-Up
Recommendations COR LOESerial evaluation of the size and morphology of the aortic sinuses and ascending aorta by echocardiography, CMR, or CT angiography is recommended in patients with a bicuspid aortic valve and an aortic diameter greater than 4.0 cm, with the examination interval determined by the degree and rate of progression of aortic dilation and by family history. In patients with an aortic diameter greater than 4.5 cm, this evaluation should be performed annually
I C
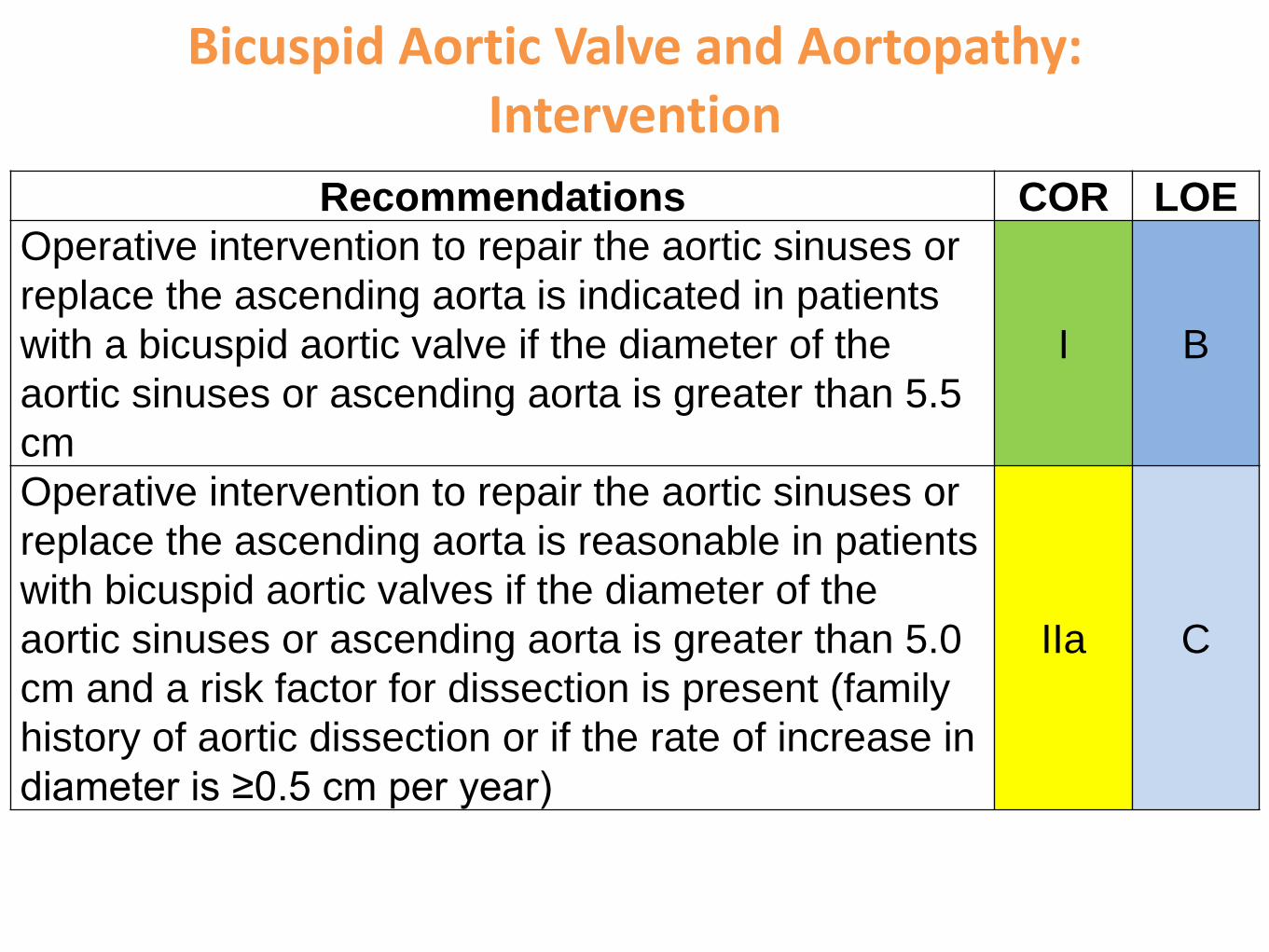
Bicuspid Aortic Valve and Aortopathy: Intervention
Recommendations COR LOE
Operative intervention to repair the aortic sinuses or
replace the ascending aorta is indicated in patients
with a bicuspid aortic valve if the diameter of the
aortic sinuses or ascending aorta is greater than 5.5
cm
I B
Operative intervention to repair the aortic sinuses or
replace the ascending aorta is reasonable in patients
with bicuspid aortic valves if the diameter of the
aortic sinuses or ascending aorta is greater than 5.0
cm and a risk factor for dissection is present (family
history of aortic dissection or if the rate of increase in
diameter is ≥0.5 cm per year)
IIa C
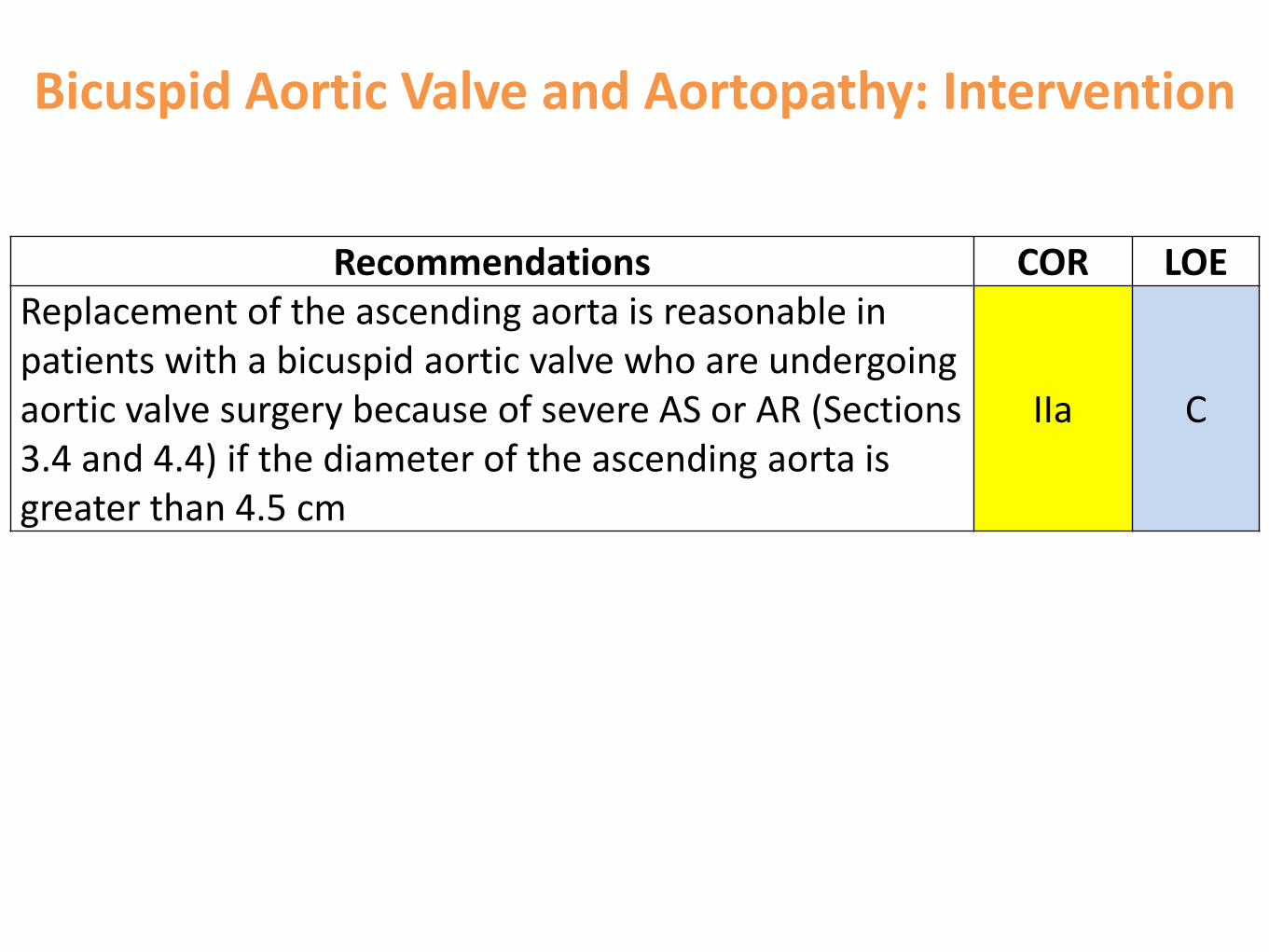
Bicuspid Aortic Valve and Aortopathy: Intervention
Recommendations COR LOEReplacement of the ascending aorta is reasonable in patients with a bicuspid aortic valve who are undergoing aortic valve surgery because of severe AS or AR (Sections 3.4 and 4.4) if the diameter of the ascending aorta is greater than 4.5 cm
IIa C
BAV - Management
Medical
• Scarce evidence of efficacy
• No evidence for altering natural history in BAV
• AHA recommendation
• Dilated aortic root/ascending aorta:
• ACEI/ARB & BB to reduce SBP to the lowest tolerated
levels
• AS/AR:
• Treatment of systemic hypertension
Current trial:
Atenolol and Telmisartan in BAV aortopathy - RCT
BAV - Management
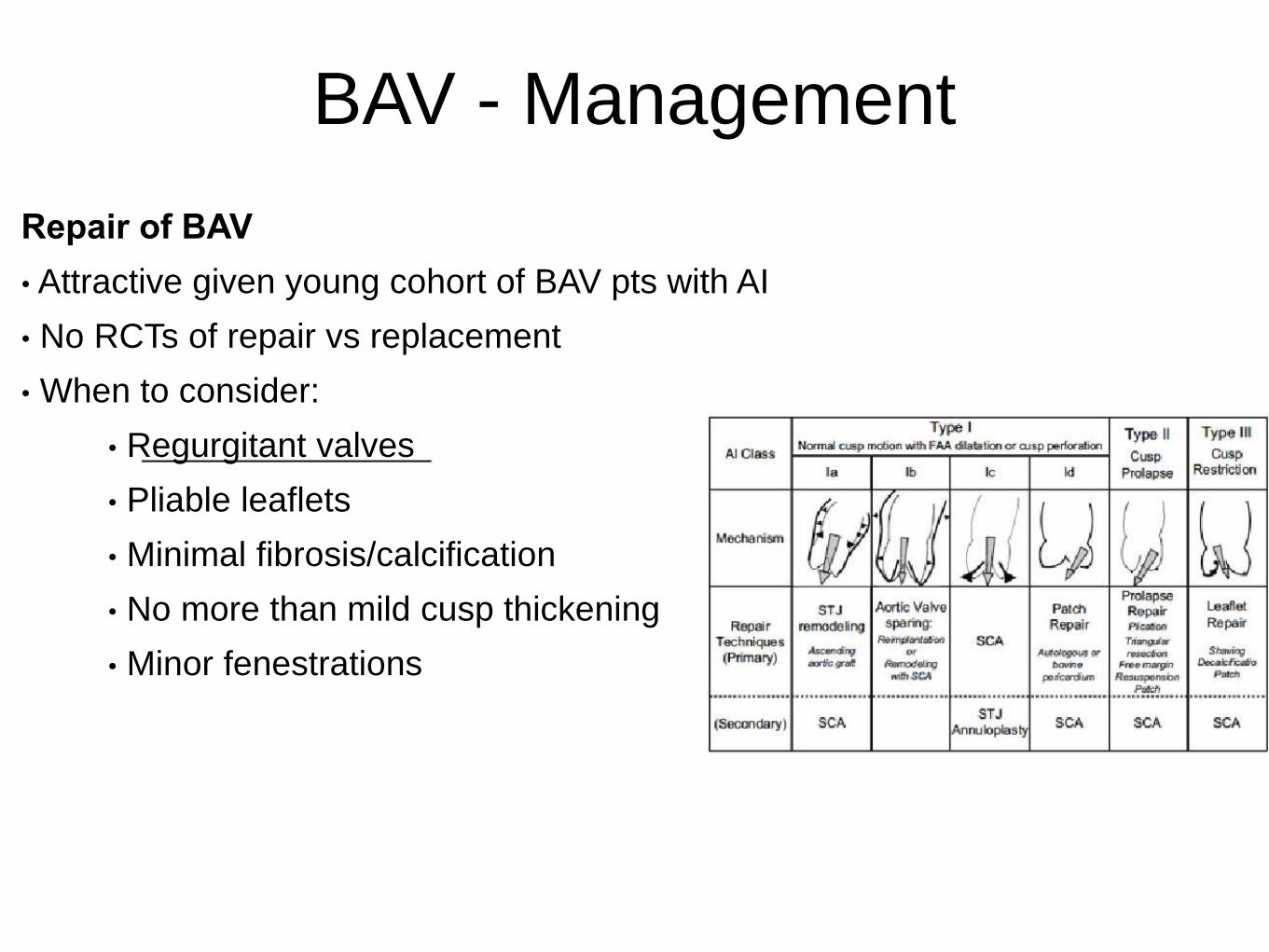
Repair of BAV
• Attractive given young cohort of BAV pts with AI
• No RCTs of repair vs replacement
• When to consider:
• Regurgitant valves
• Pliable leaflets
• Minimal fibrosis/calcification
• No more than mild cusp thickening
• Minor fenestrations

BAV - ManagementRepair of BAV - Techniques
Restore cusp integrity
• Closing tears/perforations by direct suture or autologous
pericardial patching
Line-up discloses presence of tissue redundancy
Sufficient tissue; closure of cleft
Excess tissue; triangular resection, plication

BAV - ManagementRepair of BAV - Techniques
Deficient tissue
• Overcorrecting free margin of the conjoint cusp to a length
shorter than free margin of reference cusp
• Increases systolic doming

BAV - ManagementRepair of BAV - Techniques
Commissural repair
Resuspension of detached commissure Misalignment & splaying
-pledgeted sutures & plication -pledgeted oblique Cabrol-like stitch

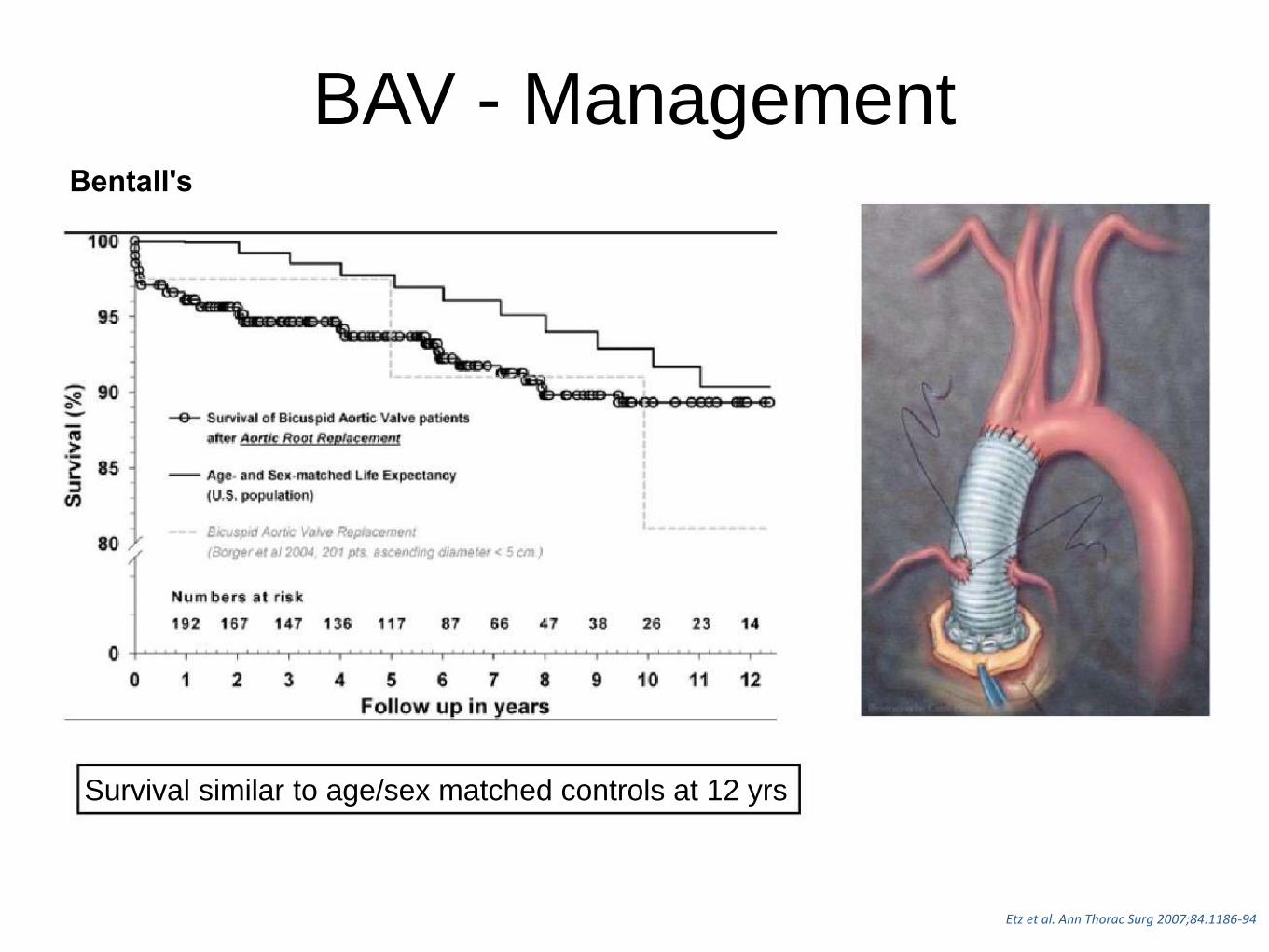
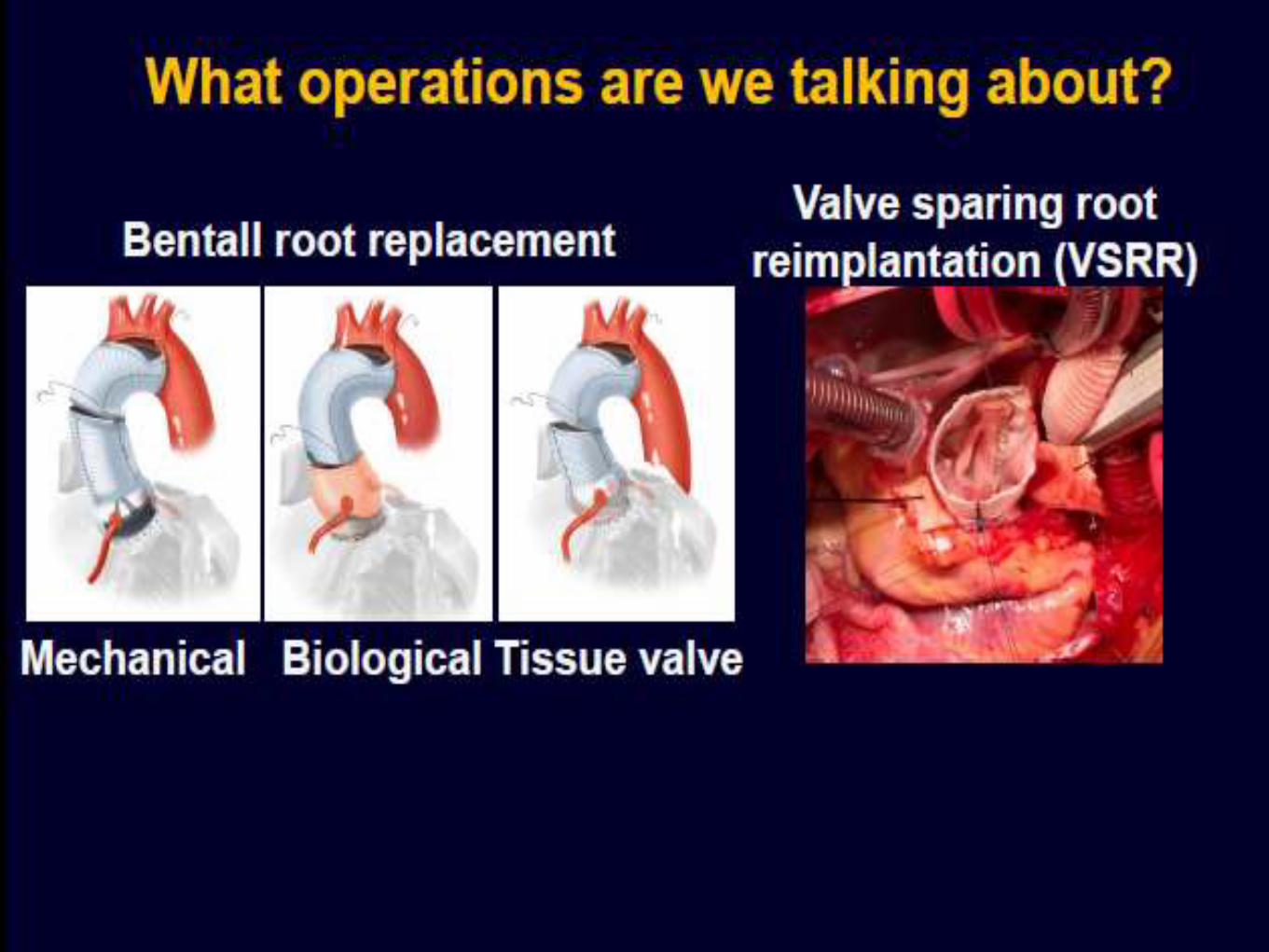
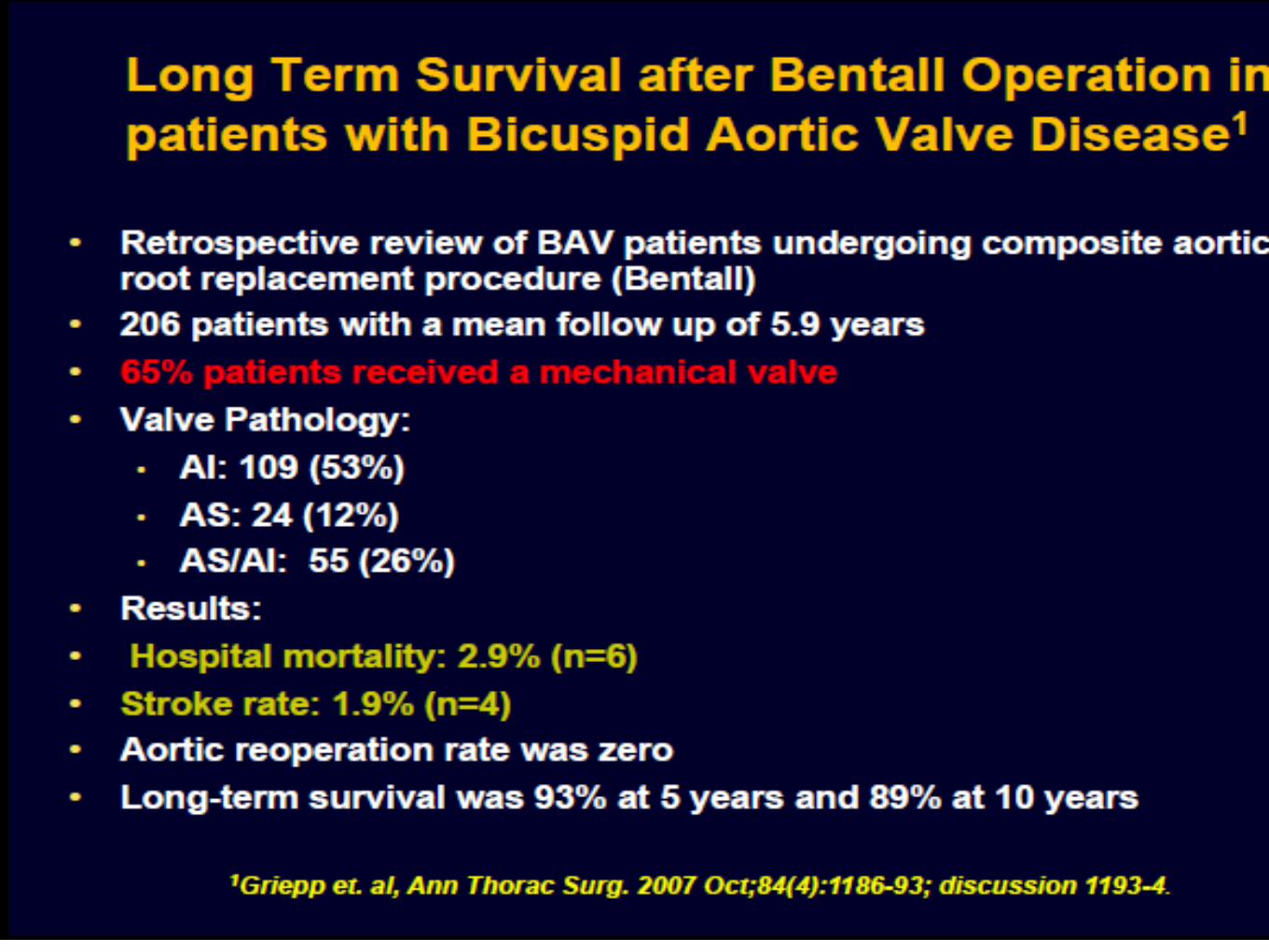
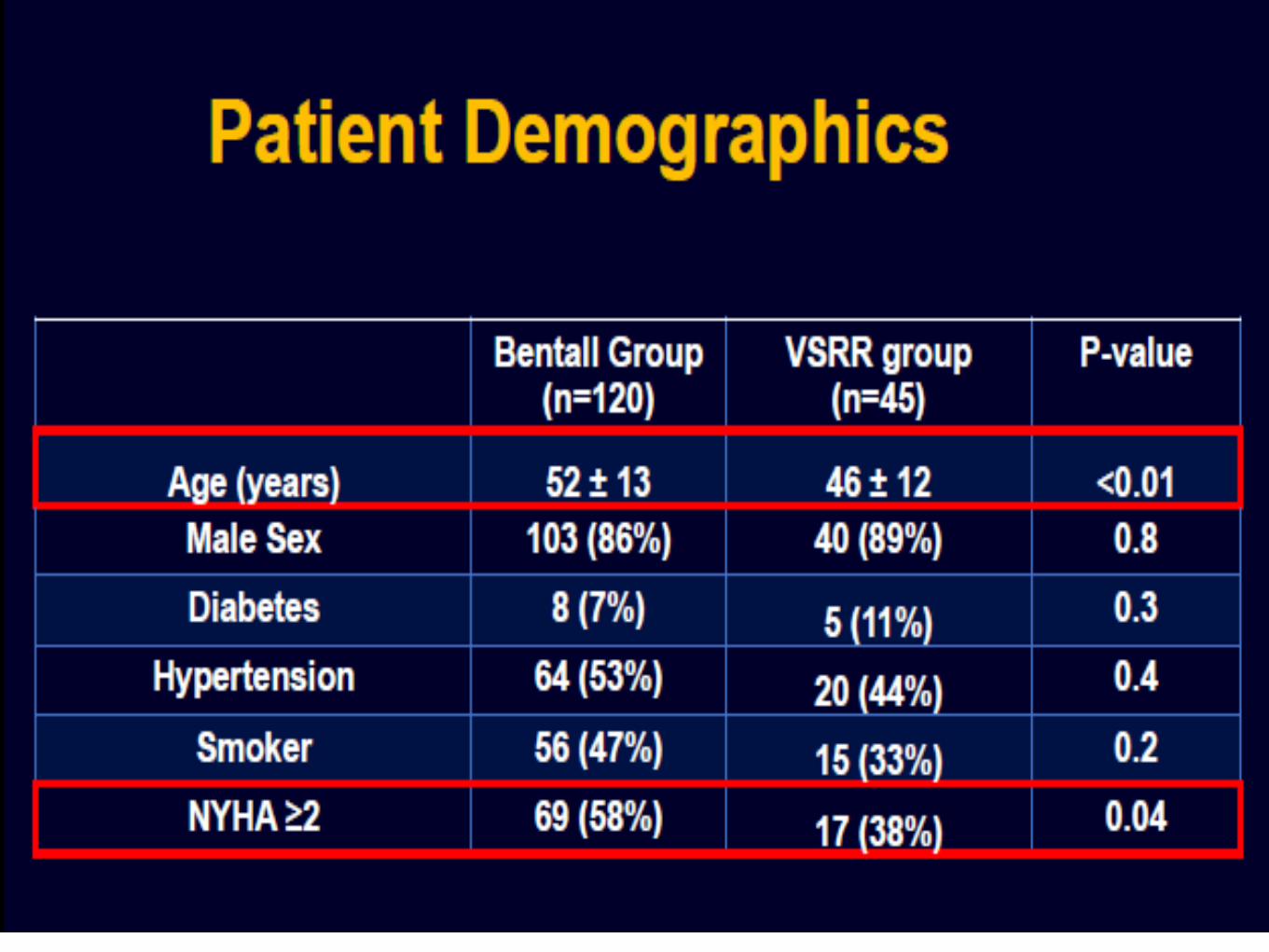
BAV - ManagementBentall's
Survival similar to age/sex matched controls at 12 yrs
Etz et al. Ann Thorac Surg 2007;84:1186-94














Much more to come
Are we all still awake?
"The key overall conceptual question in
front of the cardioaorticsurgical community is: Can
we repair virtually every pure BAV AI presentation
as we presently perform in the mitral valve repair
arena?
Factors – Poor repair Outcomes
• excessive calcification of the leaflets, including the commissures or raphe;
• severely enlarged annular diameters without robust subannularstabilization;
• leaflet surface areas that are not adequate to provide excellent cusp coaptation (and therefore would require leaflet augmentation);
• and reimplantation with very extensive cusp repair.