Download - Blood cell counting
BLOOD CELL COUNTRAJESH MOHESS,CLT

BAND (Stab cell)• Band are round or oval in shape and smaller than metamyelocyte. • They can be found in low percentage in the peripheral blood smear 0% -
5%• Bone Marrow: 17% - 33%• Size: 9 to 15 μm • Chromatin: The nucleus has a deeply indented U-shape, C, S, kidney-
bean shape or rod shape of equal thickness• The chromatin is coarse and clumped and is stained dark red or red blue.
No nucleoli• They are often described as ‘stab’ (rod-like) forms.• Cytoplasm: Brown-pink (light acidophilic) and contains secondary
granules characteristic for some species of granulocytes• Differentiating characteristics: No filament
It may resemble a metamyelocyte but indentation is more severe and chromatin is more clumped

BAND (Stab cell)

MATURE NEUTROPHIL (Segmented Neutrophil/PMN)
• Segmented neutrophilic granulocyte is a mature cell, round or oval shape
• Size: 9 to 15 μm • Chromatin: The nucleus is lobulated, with two to five lobes
connected by a thin chromatin thread-like filament • The chromatin stains purple and is coarse and arranged in clumps. • The nucleus of 1-16 % of neutrophils may have a drumstick-
shaped appendage attached to one lobe by a chromatin strand.• Neucleoli are absent • Cytoplasm is pale blue to pink granules• N:C 3:1 in favor of the cytoplasm.• Distinguishing characteristics: if no constriction is observed in
nucleus, then the cell is a band• Bone Marrow: 3% - 11%• Peripheral smear: 50 – 70 % (adults)

NEUTROPHIL
NEUTROPENIANeutropenia - low neutrophil count in the bloodNeutrophils serve as the major defense of the body
against acute bacterialacute bacterial and certain fungal infections. Neutrophils usually constitute about 50 to 70% of all
white blood cells in the bloodstream. When the neutrophil count falls below 1,000 cells per
microliter of blood, the risk of infection increasesWithout the key defense provided by neutrophils,
people have problems controlling infections and are at risk of dying from an infection

CAUSES OF NEUTROPENIANeutropenia significantly increases the risk of life-threatening
infectionNeutropenia is often caused by cancer chemotherapy or radiation
therapyNeutropenia can develop if neutrophils are used up or destroyed in
the bloodstream faster than the bone marrow can make new ones. With some bacterial infections, some allergic disorders, and some
drug treatments, neutrophils are destroyed faster than they are produced.
People with an autoimmune disease can make antibodies that destroy neutrophils and result in neutropenia.
People with an enlarged spleen may have a low neutrophil count because the enlarged spleen traps and destroys neutrophils.
Many drugs, including phenytoin, chloramphenicol, sulfa drugs, and many drugs used in cancer treatment (chemotherapy)

NEUTROPHILIANeutrophilia (Neutrophilic Leukocytosis) is a higher than
normal Neutrophils in the bloodInfections by bacteria, viruses, fungi, and parasites may all
increase the number of neutrophils in the blood. The number may rise in people who have an injury, such as
a hip fracture or burn. Inflammatory disorders, including autoimmune disorders
such as rheumatoid arthritis, can cause an increase in the number and activity of neutrophils.
Some drugs, such as corticosteroids, also lead to an increased number of neutrophils in the blood.
Myelocytic leukemias can lead to an increased number of immature or mature neutrophils in the blood


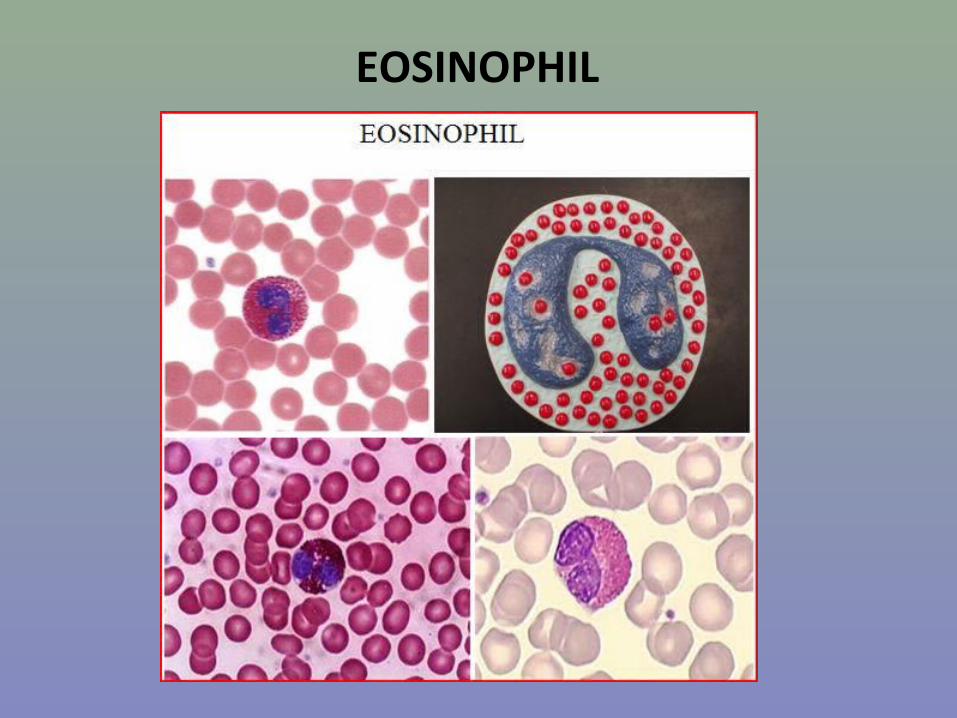
EOSINOPHIL• Eosinophils are round or oval cells that are, on average,
slightly larger than the mature neutrophils.• Size: 10 to 16 μm • N:C: Barely 1:1 • Chromatin: Eccentric nucleus, usually bilobed • Nucleoli is absent• Cytoplasm is large and orange-pink with distinctive red-
orange specific granules which are highly metabolic and contain histamine and other substances
• Distinguishing characteristics: Granules are uniformly round, large, and individualized; if stain is less than adequate, observe granules carefully for their crystalloid nature
• Bone Marrow: 0% - 3%• Peripheral smear: 0% - 4% (adults)
EOSINOPHIL

EOSINOPHIL DISORDERS
• Eosinophilic granulocytes are mostly located in tissues, and not in the peripheral blood.
• Before moving to tissues they remain in the peripheral blood for about 10 hours.
• Eosinophilia accompanies immune, allergic reactions and parasitic reactions.
• Eosinophilic granulocytes have antihistaminic function – preventing edema and smooth muscles spasm.
• They have power of phagocytosis, but not as great as the neutrophils
• Eosinopenia can occur with Cushing's syndrome, stress reactions, and treatment with corticosteroids


BASOPHIL• The mature basophilic is a round or oval cell. • Size: 10 to 14 μm • N:C: Difficult to determine • Nucleus is round, kidney-shaped or uneven, with a larger number of
notches, and occupies the major part of the cell. • The nucleus is segmented into different lobes connected by chromatin
filaments• Chromatin: Coarse, clumped bilobed• Nucleoli are absent • Cytoplasm: Rose- or lavender-colored or sometimes does not stain. • Has large, round, deeply stained blue to black unevenly distributed
granules that may overlap and obscure the nucleus. • Distinguishing characteristics: Size and color of granules will obscure the
nucleus• Bone Marrow: <1% • Peripheral smear: 0% - 2% (adults)

BASOPHIL

BASOPHILS DISORDERS• Basophilic granulocytes take part in the reactions of having the role of
degrading lipids. • Basophilic granules contain histamine and heparin. • Under the influence of histamine release factors, basophilic granulocytes
release histamine responsible for numerous allergic reactions. • Basophilic granulocytes release all stored heparin during hyperlipemia
after food intake, which enables the degradation of triglycerides into fatty acids and glycerol (heparin activates lipoproteinic lipase)
• Basopenia can occur as a response to thyrotoxicosis, acute hypersensitivity reactions, and infections
• Basophilia can occur in people with hypothyroidism• In the myeloproliferative disorders (e.g., polycythemia vera and
myelofibrosis), a marked increase in the number of basophils can occur


Monocyte• Monocyte is round or oval shape• Due to ameboid movements on the edge of the cell, 1, 2 or
more pseudopods can be seen• The size is 12-20 µm• N:C 2:1 – 1:1• The cytoplasm is relatively abundant dull grey-blue
It may have a ground-glass appearance with a number of evenly distributed fine azurophilic granules. Vacuoles common
• The nucleus is usually round or kidney-shaped or horse-shoe shaped but may be markedly indented or even lobulated, with two or more lobes
• Nucleoli are not usually visible• Bone Marrow: 2% • Peripheral Smear: 2% - 9% (adults)

Monocyte

MONOCYTE DISORDERS Monocytes help other white blood cells remove
dead or damaged tissues, destroy cancer cells, and regulate immunity against foreign substances.
After a few hours in the bloodstream, they migrate to tissues (such as spleen, liver, lung, and bone marrow tissue), where they mature into macrophages as the main scavenger cells of the immune system

MONOCYTE DISORDERS • Monocytosis occurs in response to chronic
infections, in autoimmune disorders, in blood disorders, cancers and in sarcoidosis (an infection of the lung)
• Monocytopenia can occur in response to the release of toxins into the blood by certain types of bacteria as, well as in people receiving chemotherapy or corticosteroids


LYMPHOCYTE
• Two types of lymphocytes can be distinguished:
- Small lymphocyte
- Large lymphocyte

SMALL LYMPHOCYTE
• Small lymphocytes are the major part of lymphocytes in the blood. • The cell has a large roundish and regular nucleus.• Size: about 9 - 12 μm • N:C: 4:1 • Chromatin: Nucleus is eccentrically located, round or oval, often with
an indentation in one place; chromatin is heavily clumped, forming compact lumpy accumulations without sharp demarcations
• Nucleoli not present• Cytoplasm: Scanty cytoplasm is often barely visible and quite often
seen only at the nuclear peripheryNo granules. Distinctly basophilic
• Bone Marrow: 5% - 15%• Peripheral smear: 20% - 44% (adults)

SMALL LYMPHOCYTE

LARGE LYMPHOCYTE
• Large lymphocytes are the minor part of lymphocytes in the bloodstream.
• The cell has a large roundish and regular nucleus• Size: 9 to 18 μm • N:C: 3:1• Chromatin: Nucleus is slightly eccentric located, round or
oval, sometimes slightly indented• Chromatin has a looser pattern and more transparent. • Nucleoli is not present• Cytoplasm: Larger amount of cytoplasm, sky-blue color• There may be up to 10 azurophilic granules• Distinguishing characteristic: Cytoplasm is more abundant
with tendency for azurophilic granules

LARGE LYMPHOCYTE

LYMPHOCYTES DISORDERS
• T- and B-lymphocytes have different roles in generating acquired immunity:
- T-lymphocytes in cellular - B-lymphocytes in humoral immunity
• Both types produce antibodies• Together with natural killer-cells (NK-cells) and the
complement system they compose a powerful defensive system in the organism
• Lymphocytopenia is an abnormally low lymphocyte count in the body
• A reduction in the number of lymphocytes may not cause a significant decrease in the total number of white blood cells

LYMPHOCYTOPENIA • Viral infections – including HIV infection• Lymphocytes can decrease briefly during
starvation, times of severe stress, and during use of corticosteroids, chemotherapy for cancer, and radiation therapy
• Cancer – leukemias, lymphomas• Rheumatoid Arthritis• Systemic Lupus Erthematosus (SLE)

LYMPHOCYTOSISLymphocytosis is an abnormally high lymphocyte count in
the bloodThe number of lymphocytes can increase in response to
infections, especially by virusesSome bacterial infections, such as tuberculosis, may also
increase the number. Certain types of cancer, such as lymphomas and acute or
chronic lymphocytic leukemia, may produce an increase in the number of lymphocytes, in part by releasing immature lymphocytes (lymphoblasts) or the lymphoma cells into the bloodstream.
Graves' disease and Crohn's disease may also result in an increase in the number of lymphocytes in the bloodstream


PLASMA CELL• Size: 8 to 20 μm • N:C: 2-1:1• Nucleoli: None• Nucleus: Round or oval, eccentric• Chromatin: coarse• Cytoplasm: Deeply basophilic, often with perinuclear zone (hof)• Vacuoles: None to several• Bone Marrow: 0% - 1%• Peripheral blood: 0%• Function of plasma cells is the synthesis and excretion of
immunoglobulins (antibodies) • Plasma cells may be found in peripheral blood of patients with
measles, chickenpox, scarlet fever, multiple myeloma and plasmacytic leukemia

PLASMA CELL

PLASMA CELL

REFERENCE RANGE
Cell 0- 4 years (%) Adult (%)
• NeutrophilsNeutrophils 20-4420-44 50-7050-70• BandsBands 0-50-5 2-62-6• LymphocytesLymphocytes 48-7848-78 20-4420-44• MonocytesMonocytes 2-112-11 2-92-9• EosinophilsEosinophils 1-41-4 0-40-4• BasophilsBasophils 0-20-2 0-20-2

WHITE BLOOD CELLS

RELATIVE VS ABSOLUTE COUNT• Relative and absolute Relative and absolute counts are terms referring to the white cell
differential. • The relative count refers to the percentage of a particular cell
counted from the 100 WBC differential • The absolute count refers to the count derived from the total
white count multiplied by the percentage of any particular white cell.
• The absolute count is clinically significant in many disease states providing important information to the clinician.
• It provides a more accurate measure of the actual numbers of cells present in the peripheral blood
• For example, Neutropenia in a patient, will place the patient at a higher risk for infections. Patients undergoing chemotherapy will need to get an absolute neutrophil count to monitor their immune status

RELATIVE VS ABSOLUTE COUNT
Example: • If the WBC is 5.0 x 103/µL• And the differential reads:
- Segmented neutrophils: 40% (Range: 50% to 70%)- Bands: 3% (Range: 2% to 6%)- Lymphocytes: 55% (Range: 20% to 44%)- Monocytes: 2% (Range: 2% to 9%)
• Then the absolute count of lymphocytes would be :5000 X 0.55 = 2750OR: (5 x 55) X 10 = 2750 OR: (5000 x 55) / 100 = 2750
• Absolute Neutrophil count = (% of Neutrophils + Bands) X total WBC

RELATIVE VS ABSOLUTE COUNT
Normal values• Neutrophils: 1800 – 6800 /µL• Band Neutrophils: 0 – 700 /µL• Lymphocytes: 1000 – 3400 /µL• Monocytes: 200 – 800 /µL• Eosionphils: 0 – 400 /µL• Basophils: 0 – 100 /µL

BLOOD CELL COUNTING
THE END







