Download - Calculi Formation
CALCULI FORMATION
Bonifacio | Bueno | Burton | Busa | Cariaga
FEU NRMF Medicine 1-C
CALCULI
• An abnormal or pathologic
concretion or mass of
mineral salts that occur in
the body
• Precipitation or
crystallization of minerals
in organs such as the
kidneys or the gall bladder
CALCULI
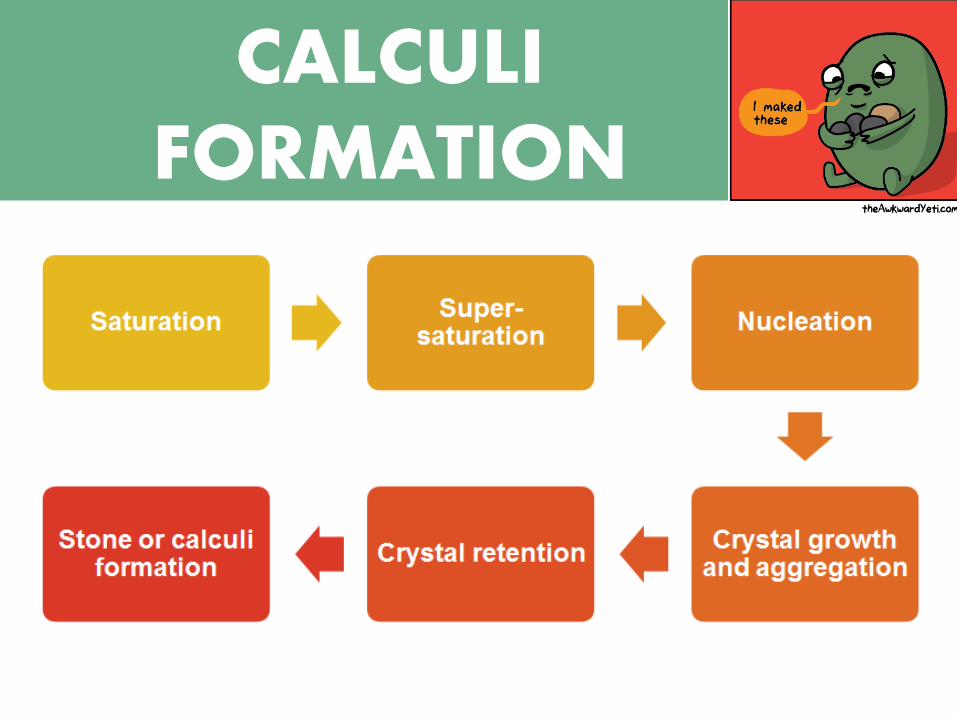
FORMATION CALCULI
FORMATION
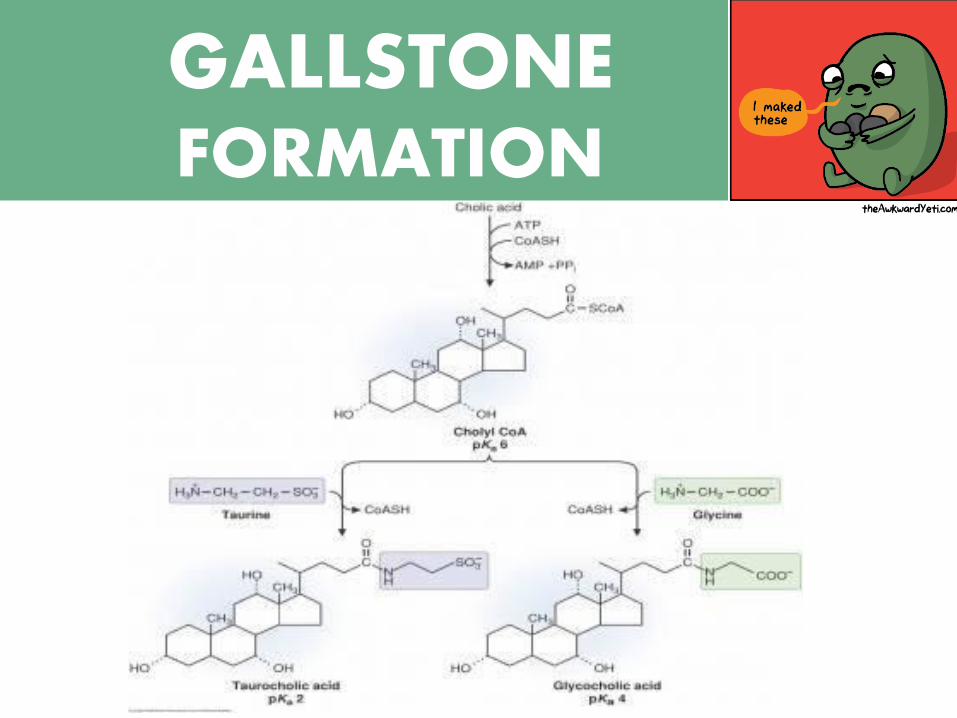
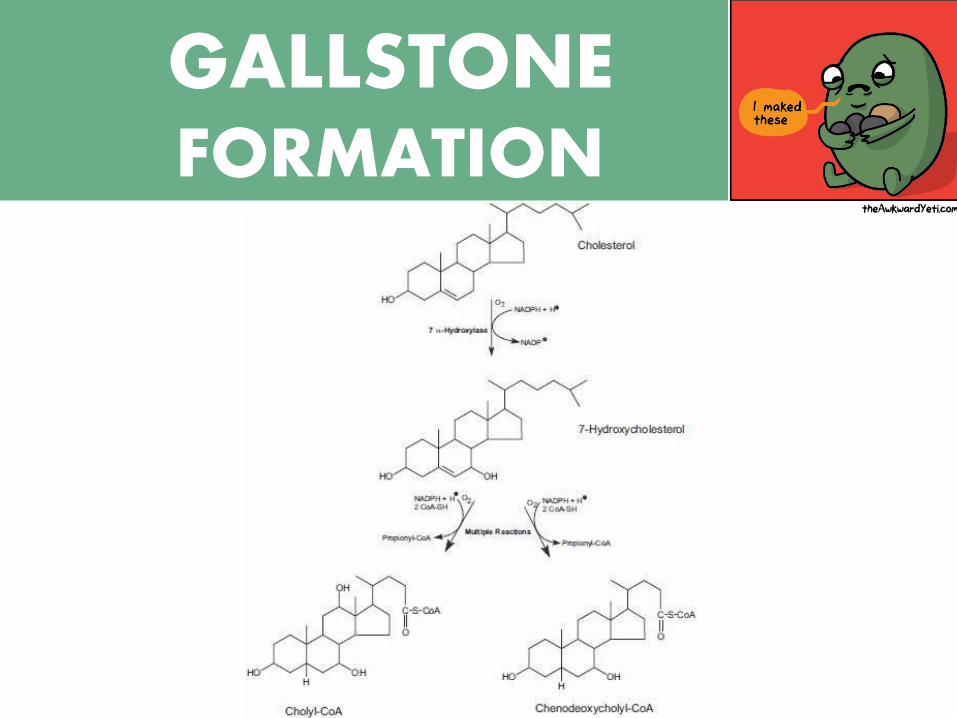
GALLSTONE FORMATION
FORMATION GALLSTONE FORMATION
CALCULI
GALLSTONES
• Cholesterol stones • Most common
• Form when amount of cholesterol exceeds or supersaturates capacity of bile
• Pigment stones
• From crystallization of calcium bilirubinate
• May indicate infection
• Black or brown
TYPES OF CALCULI
CALCULI
RENAL STONES
•Calcium stones
• Most common renal stones
• Contain Ca, PO4, oxalate
• Caused by excessive Ca in the body
• Hyperparathyroidism
TYPES OF CALCULI
CALCULI
•Uric acid
• Formed due to
• Low urine output
• High protein diet
• Increased alcohol
intake
•Struvite
• Affect more women
than men
• May accompany
renal infections
TYPES OF CALCULI
RENAL STONES
CALCULI
RENAL STONES
•Cystine
• Rare
• Typically occur in individuals with family
history of cystinuria
TYPES OF CALCULI
CALCULI
GALLSTONES: Cholesterol
• Supersaturation of bile with cholesterol
• Intestinal hypomotility
• Excess in pro-nucleation factors, deficiency of
anti-nucleation factors
• Hypersecretion of mucus in the gall bladder
PROMOTING FACTORS
CALCULI
GALLSTONES: Pigment
• Elevated levels of unconjugated bilirubin in the blood
• Hemolytic diseases
• Severe ileal dysfunction
• Intestinal hypomotility
• Infection of the biliary tree • Bacteria (E. coli)
• Parasite (Ascaris lumbricoides)
• Fungi (Ophiocordyceps sinensi)
PROMOTING FACTORS
CALCULI
RENAL STONES
•Slow urine flow
•Damaged urinary tract lining
•Absence of inhibitory proteins (nephrocalcin, Tamm-Horsfall protein, uropontin)
• Intake of medication
•Dehydration
PROMOTING FACTORS
CALCULI
RENAL STONES
•Urine pH
• Acidic pH: favour precipitation and formation
of uric acid stones and cystine stones
• Alkaline pH: CaPO4 stones and struvite
stones
PROMOTING FACTORS
CALCULI
RENAL STONES
•Sufficient consumption of water
•Decreased protein intake
•Reduced sodium consumption
•Frequent drinking of water
PREVENTIVE FACTORS
CALCULI
RENAL STONES
•Normal concentration of urine elements
•Normal urine parameters (volume, pH,
etc)
•Presence of inhibitory proteins (Tamm-
Horsfall protein, nephrocalcin, uropontin)
•Prevention of urine stasis (timely and
sufficient voiding)
PREVENTIVE FACTORS
CALCULI
GALLSTONES
•Normal composition of gall bladder
contents
•Low-fat, low-cholesterol diet
•High fiber intake
•Decreased sugar consumption
•Physical exertion/exercise
PREVENTIVE FACTORS
CALCULI
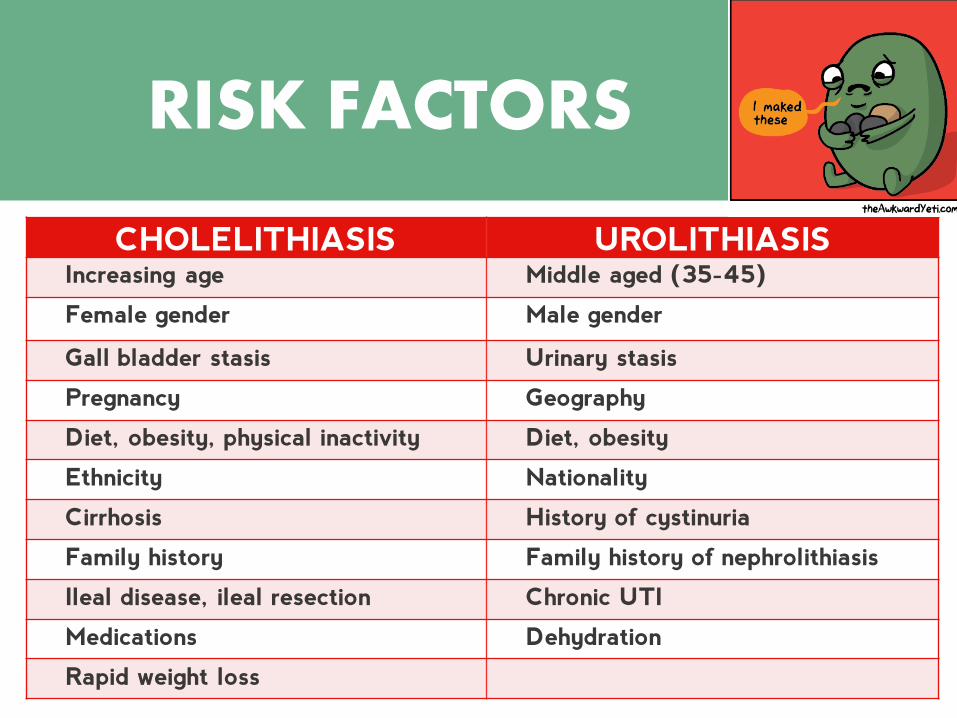
CHOLELITHIASIS UROLITHIASIS Increasing age Middle aged (35-45)
Female gender Male gender
Gall bladder stasis Urinary stasis
Pregnancy Geography
Diet, obesity, physical inactivity Diet, obesity
Ethnicity Nationality
Cirrhosis History of cystinuria
Family history Family history of nephrolithiasis
Ileal disease, ileal resection Chronic UTI
Medications Dehydration
Rapid weight loss
RISK FACTORS
CALCULI
•CLDN-14
•Polymorphisms occuring at:
•Calcium-sensing receptor (CSR)
•Vitamin D receptor (VDR)
•Osteopontin (OPN)
GENETIC BASIS OF PREDISPOSITION
CALCULI
GALLSTONES
• Pulsating, propagating pain that disappears
shortly after it begins
• Pain in the upper right portion of the abdomen
• Pain immediately below the area of the breast
• Pain in the right shoulder • Referred pain
CLINICAL MANIFESTATIONS
CALCULI
RENAL STONES
• Severe pain in the back and sides of the
abdomen, just below the ribs
• May spread to groin area
• In the case of an infection, symptoms include
nausea or vomiting, fever, and chills
CLINICAL MANIFESTATIONS
CALCULI
RENAL STONES
CLINICAL MANIFESTATIONS
• Painful urination
• Hematuria or pink, red, or
brown urine with a foul
odour
• Changes in the voiding
pattern
• Small amounts of urine
may be voided at a time.
CALCULI
RENAL STONES
• Severe renal obstruction and the possibility of
infection
• Kidney failure
GALLSTONES
• Gall bladder inflammation
• Common bile/pancreatic duct blockage
• Gall bladder cancer
COMPLICATIONS

CALCULI
RENAL STONES
• Urine examination
• Hematuria
• Pyuria
• BUN, creatinine, and electrolytes
• Abdominal ultrasound
• Intravenous pyelogram (IVP)
LAB DIAGNOSIS
CALCULI
GALLSTONES • Elevated serum aminotransferase, alkaline phosphatase, bilirubin and amylase
• Blood test: look for signs of infection, obstruction, pancreatitis, or jaundice.
• Oral cholecystogram
• Bile microscopy
• Cholescintigraphy
• Physical examination (Murphy’s technique)
• MRI, CT scan, ultrasound
LAB DIAGNOSIS
CALCULI
GALLSTONES
DIAGNOSIS
CALCULI
GALLSTONES
•Administration of Ursodiol
•Contact distribution therapy
•Use organic solvent methyl tert-butyl
ether (MTBE)
•Surgical removal
TREATMENT
CALCULI
RENAL STONES
•Extracorporal shockwave lithotripsy
(ESWL)
•Percutaneous nephrolithotomy
•Ureteroscopy
•Open surgery
•Medication
TREATMENT
CALCULI
RENAL STONES
TREATMENT
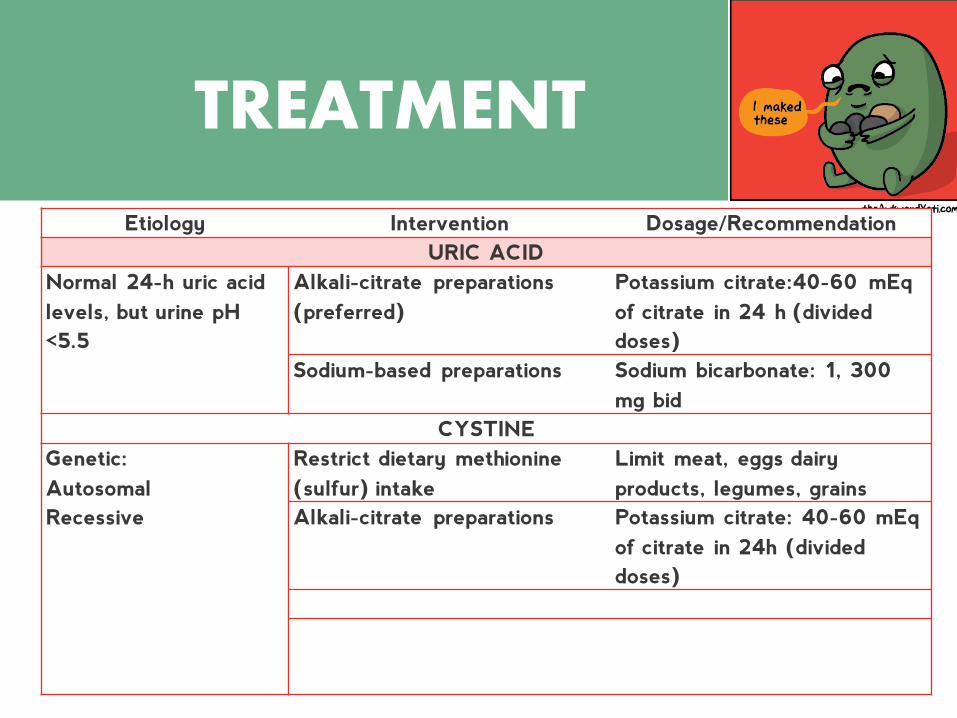
Etiology Intervention Dosage/Recommendation
URIC ACID
Normal 24-h uric acid
levels, but urine pH
<5.5
Alkali-citrate preparations
(preferred)
Potassium citrate:40-60 mEq
of citrate in 24 h (divided
doses)
Sodium-based preparations Sodium bicarbonate: 1, 300
mg bid
CYSTINE
Genetic:
Autosomal
Recessive
Restrict dietary methionine
(sulfur) intake
Limit meat, eggs dairy
products, legumes, grains
Alkali-citrate preparations Potassium citrate: 40-60 mEq
of citrate in 24h (divided
doses)
CALCULI
RENAL STONES
TREATMENT
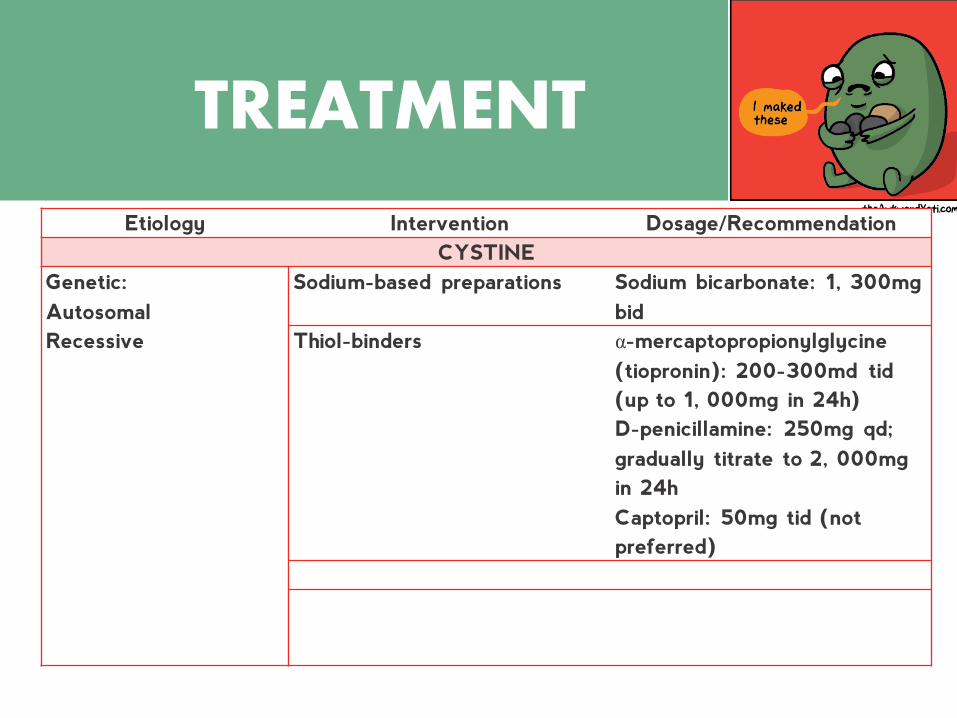
Etiology Intervention Dosage/Recommendation
CYSTINE
Genetic:
Autosomal
Recessive
Sodium-based preparations Sodium bicarbonate: 1, 300mg
bid
Thiol-binders α-mercaptopropionylglycine
(tiopronin): 200-300md tid
(up to 1, 000mg in 24h)
D-penicillamine: 250mg qd;
gradually titrate to 2, 000mg
in 24h
Captopril: 50mg tid (not
preferred)
CALCULI
RENAL STONES
TREATMENT
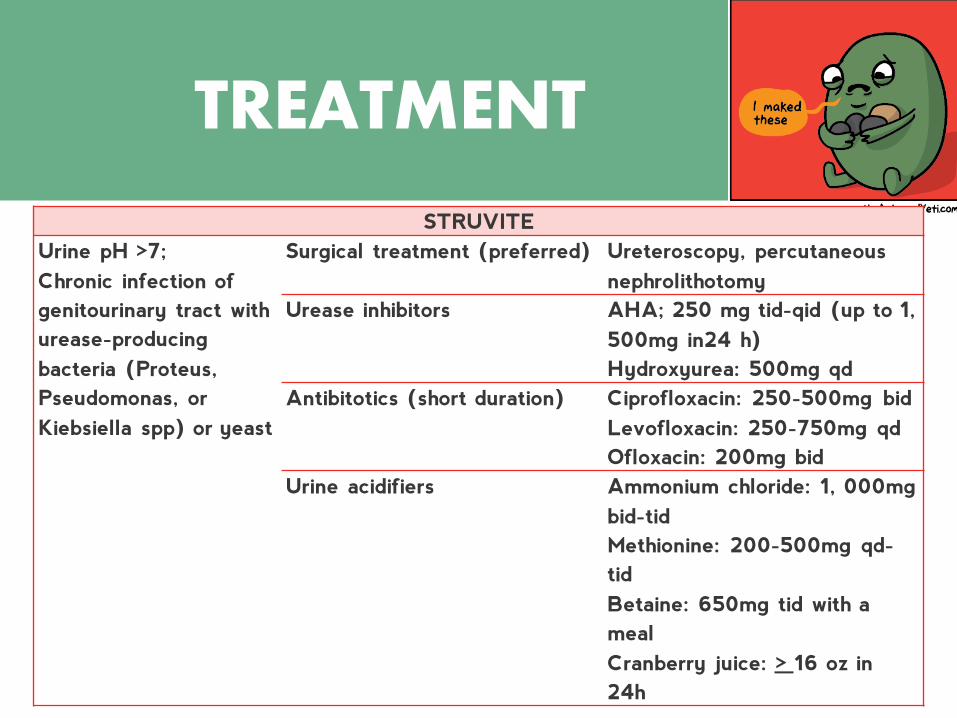
STRUVITE
Urine pH >7;
Chronic infection of
genitourinary tract with
urease-producing
bacteria (Proteus,
Pseudomonas, or
Kiebsiella spp) or yeast
Surgical treatment (preferred) Ureteroscopy, percutaneous
nephrolithotomy
Urease inhibitors AHA; 250 mg tid-qid (up to 1,
500mg in24 h)
Hydroxyurea: 500mg qd
Antibitotics (short duration)
Ciprofloxacin: 250-500mg bid
Levofloxacin: 250-750mg qd
Ofloxacin: 200mg bid
Urine acidifiers Ammonium chloride: 1, 000mg
bid-tid
Methionine: 200-500mg qd-
tid
Betaine: 650mg tid with a
meal
Cranberry juice: > 16 oz in
24h
CALCULI FORMATION
THANK YOU!







