Contents lists available at ScienceDirect
Can J Diabetes 39 (2015) 250e252
Canadian Journal of Diabetesjournal homepage:
www.canadianjournalofdiabetes.com
Commentary
Policies, Guidelines and Consensus Statements: PharmacologicManagement of Type 2 Diabetese2015 Interim Update
Canadian Diabetes Association Clinical Practice Guidelines Expert Committee
The initial draft of this commentary was prepared by William Harper MD, FRCPC, Maureen Clement MD,CCFP, Ronald Goldenberg MD, FRCPC, FACE, Amir Hanna MB, BCh, FRCPC, FACP, Andrea Main BScPhm,CDE, Ravi Retnakaran MD, MSc, FRCPC, Diana Sherifali RN, PhD, CDE, Vincent Woo MD, FRCPC,Jean-François Yale MD, CSPQ, FRCPC, and Alice Y.Y. Cheng MD, FRCPC on behalf of the SteeringCommittee for the Canadian Diabetes Association 2013 Clinical Practice Guidelines for the Preventionand Management of Diabetes in Canada
a r t i c l e i n f o
Article history:Received 13 May 2015Accepted 13 May 2015
1499-2671/$ e see front matter � 2015 Canadian Diahttp://dx.doi.org/10.1016/j.jcjd.2015.05.009
The process of the development of the Canadian DiabetesAssociation 2013 Clinical Practice Guidelines for the Prevention andManagement of Diabetes in Canada included provisions to updateindividual chapters prior to the planned published revision in 2018(1). An updated literature search that focused on new evidencepublished since the development of the 2013 guidelines yielded1787 citations. After review of these citations, the chapter authorsadvised the steering and executive committees that there were nosignificant changes in evidence to warrant the formulation ofany new recommendations or the revision of any currentrecommendations. As such, it was recommended that a full updateof the chapter be deferred until the planned revision of the entireClinical Practice Guidelines in 2018.
However, the steering committee decided it was warranted topublish an interim commentary addressing the approval, inCanada, of a new class of antihyperglycemic agentsdsodium-glucose linked transporter 2 (SGLT2) inhibitorsdfor thepharmacologic management of diabetes. Two agents from this classhave received notice of compliance by Health Canada since thepublication of the 2013 guidelines: canagliflozin and dapagliflozin(2). This update was deemed necessary by the steering committeebecause the addition of a new class of pharmacologic therapyrepresents a significant change in the management options fordiabetes, yet the next complete update of the guidelines is still 3years away.
SGLT2 inhibitors block glucose transport in the proximal renaltubule, which results in the urinary excretion of glucose, therebylowering blood glucose and body weight (3,4). Network meta-analyses show that, when added to metformin, SGLT2
betes Association
inhibitors generally have similar or slightly better efficacy inlowering glycated hemoglobin levels than do other anti-hyperglycemic agents (5,6). The incidence of hypoglycemia withSGLT2 inhibitors is rare unless they are used in combination withinsulin or sulfonylureas (3). Because of the glycosuria resultingfrom the use of these agents, there is an increased risk for urinarytract infections, genital mycotic infections and hypotensioncaused by osmotic diuresis (3). Although SGLT2 inhibitors lowerblood pressure (3) and raise high-density lipoprotein cholesterol,they elevate low-density lipoprotein cholesterol modestly (7,8),and their cardiovascular safety remains unknown and awaitslong-term clinical trials. An imbalance in bladder cancer wasnoted with dapagliflozin in early clinical trials; however, many ofthe subjects with bladder cancer had pre-existing hematuria (9).There have been reported cases of diabetic ketoacidosis, withoutthe usual elevated blood glucose, in patients with type 2 diabetesbeing treated with SGLT2 inhibitors (10e13). These cases are rareand further details await ongoing reviews. Patients on an SGLT2inhibitor with symptoms of breathing difficulty, nausea,vomiting, abdominal pain, confusion or fatigue, even in theabsence of high blood glucose, should be evaluated for ketoaci-dosis. If the ketoacidosis is confirmed, appropriate measuresshould be undertaken to correct the acidosis. The SGLT2inhibitor therapy should be interrupted and its subsequent longterm use should be reassessed (10,13). Use of SGLT2 inhibitorsis not currently approved for type 1 diabetes. Figure 1 sum-marizes the therapeutic considerations for SGLT2 inhibitortherapy in the management of type 2 diabetes mellitus. Theefficacy of SGLT2 inhibitors with respect to glucose lowering is
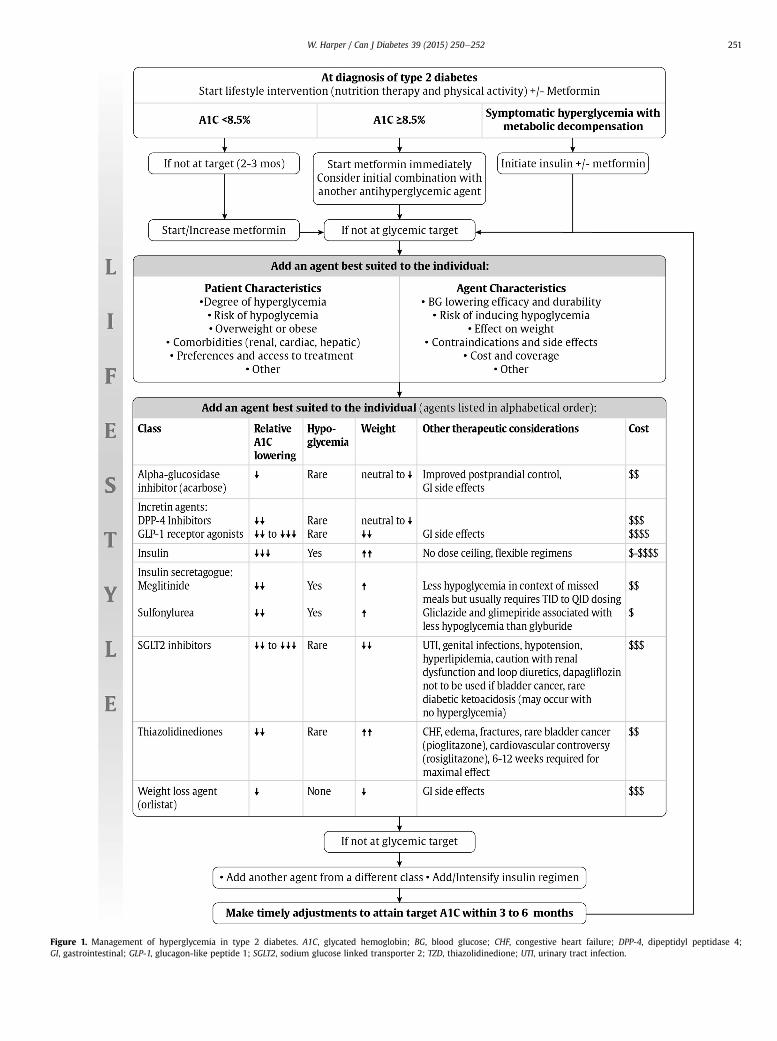
Figure 1. Management of hyperglycemia in type 2 diabetes. A1C, glycated hemoglobin; BG, blood glucose; CHF, congestive heart failure; DPP-4, dipeptidyl peptidase 4;GI, gastrointestinal; GLP-1, glucagon-like peptide 1; SGLT2, sodium glucose linked transporter 2; TZD, thiazolidinedione; UTI, urinary tract infection.
W. Harper / Can J Diabetes 39 (2015) 250e252 251
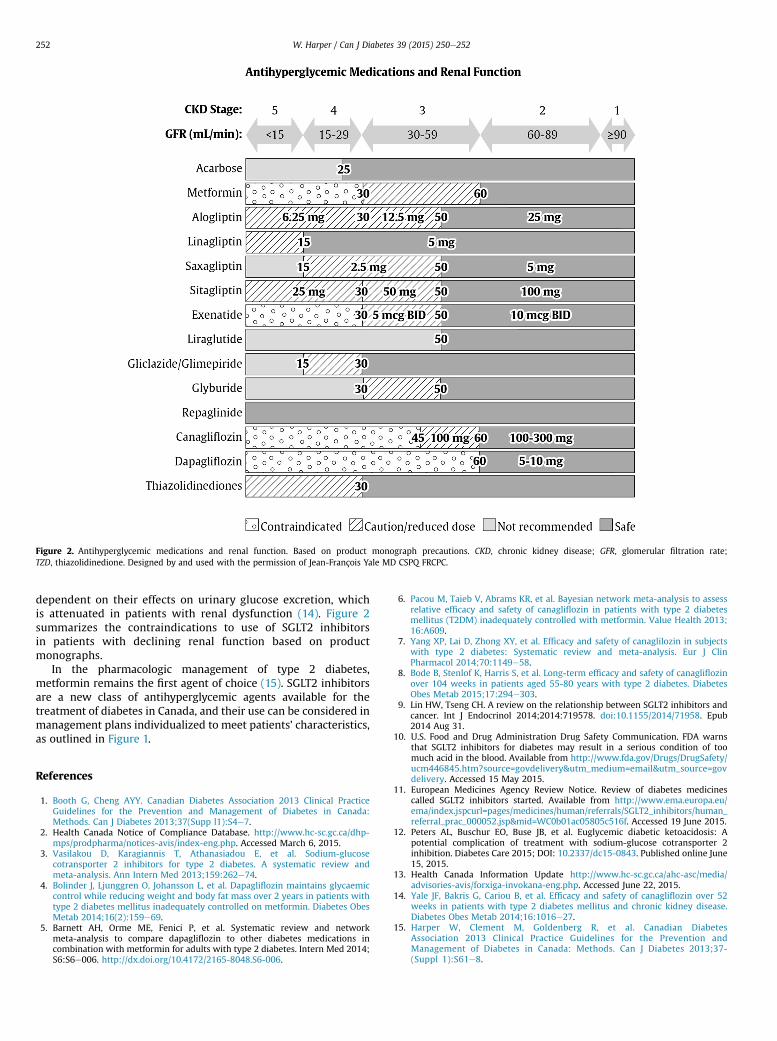
Figure 2. Antihyperglycemic medications and renal function. Based on product monograph precautions. CKD, chronic kidney disease; GFR, glomerular filtration rate;TZD, thiazolidinedione. Designed by and used with the permission of Jean-François Yale MD CSPQ FRCPC.
W. Harper / Can J Diabetes 39 (2015) 250e252252
dependent on their effects on urinary glucose excretion, whichis attenuated in patients with renal dysfunction (14). Figure 2summarizes the contraindications to use of SGLT2 inhibitorsin patients with declining renal function based on productmonographs.
In the pharmacologic management of type 2 diabetes,metformin remains the first agent of choice (15). SGLT2 inhibitorsare a new class of antihyperglycemic agents available for thetreatment of diabetes in Canada, and their use can be considered inmanagement plans individualized to meet patients’ characteristics,as outlined in Figure 1.
References
1. Booth G, Cheng AYY. Canadian Diabetes Association 2013 Clinical PracticeGuidelines for the Prevention and Management of Diabetes in Canada:Methods. Can J Diabetes 2013;37(Supp l1):S4e7.
2. Health Canada Notice of Compliance Database. http://www.hc-sc.gc.ca/dhp-mps/prodpharma/notices-avis/index-eng.php. Accessed March 6, 2015.
3. Vasilakou D, Karagiannis T, Athanasiadou E, et al. Sodium-glucosecotransporter 2 inhibitors for type 2 diabetes. A systematic review andmeta-analysis. Ann Intern Med 2013;159:262e74.
4. Bolinder J, Ljunggren O, Johansson L, et al. Dapagliflozin maintains glycaemiccontrol while reducing weight and body fat mass over 2 years in patients withtype 2 diabetes mellitus inadequately controlled on metformin. Diabetes ObesMetab 2014;16(2):159e69.
5. Barnett AH, Orme ME, Fenici P, et al. Systematic review and networkmeta-analysis to compare dapagliflozin to other diabetes medications incombination with metformin for adults with type 2 diabetes. Intern Med 2014;S6:S6e006. http://dx.doi.org/10.4172/2165-8048.S6-006.
6. Pacou M, Taieb V, Abrams KR, et al. Bayesian network meta-analysis to assessrelative efficacy and safety of canagliflozin in patients with type 2 diabetesmellitus (T2DM) inadequately controlled with metformin. Value Health 2013;16:A609.
7. Yang XP, Lai D, Zhong XY, et al. Efficacy and safety of canaglilozin in subjectswith type 2 diabetes: Systematic review and meta-analysis. Eur J ClinPharmacol 2014;70:1149e58.
8. Bode B, Stenlof K, Harris S, et al. Long-term efficacy and safety of canagliflozinover 104 weeks in patients aged 55-80 years with type 2 diabetes. DiabetesObes Metab 2015;17:294e303.
9. Lin HW, Tseng CH. A review on the relationship between SGLT2 inhibitors andcancer. Int J Endocrinol 2014;2014:719578. doi:10.1155/2014/71958. Epub2014 Aug 31.
10. U.S. Food and Drug Administration Drug Safety Communication. FDA warnsthat SGLT2 inhibitors for diabetes may result in a serious condition of toomuch acid in the blood. Available from http://www.fda.gov/Drugs/DrugSafety/ucm446845.htm?source=govdelivery&utm_medium=email&utm_source=govdelivery. Accessed 15 May 2015.
11. European Medicines Agency Review Notice. Review of diabetes medicinescalled SGLT2 inhibitors started. Available from http://www.ema.europa.eu/ema/index.jspcurl=pages/medicines/human/referrals/SGLT2_inhibitors/human_referral_prac_000052.jsp&mid=WC0b01ac05805c516f. Accessed 19 June 2015.
12. Peters AL, Buschur EO, Buse JB, et al. Euglycemic diabetic ketoacidosis: Apotential complication of treatment with sodium-glucose cotransporter 2inhibition. Diabetes Care 2015; DOI: 10.2337/dc15-0843. Published online June15, 2015.
13. Health Canada Information Update http://www.hc-sc.gc.ca/ahc-asc/media/advisories-avis/forxiga-invokana-eng.php. Accessed June 22, 2015.
14. Yale JF, Bakris G, Cariou B, et al. Efficacy and safety of canagliflozin over 52weeks in patients with type 2 diabetes mellitus and chronic kidney disease.Diabetes Obes Metab 2014;16:1016e27.
15. Harper W, Clement M, Goldenberg R, et al. Canadian DiabetesAssociation 2013 Clinical Practice Guidelines for the Prevention andManagement of Diabetes in Canada: Methods. Can J Diabetes 2013;37-(Suppl 1):S61e8.







