Download - Card &, Health Care - University of Tasmania
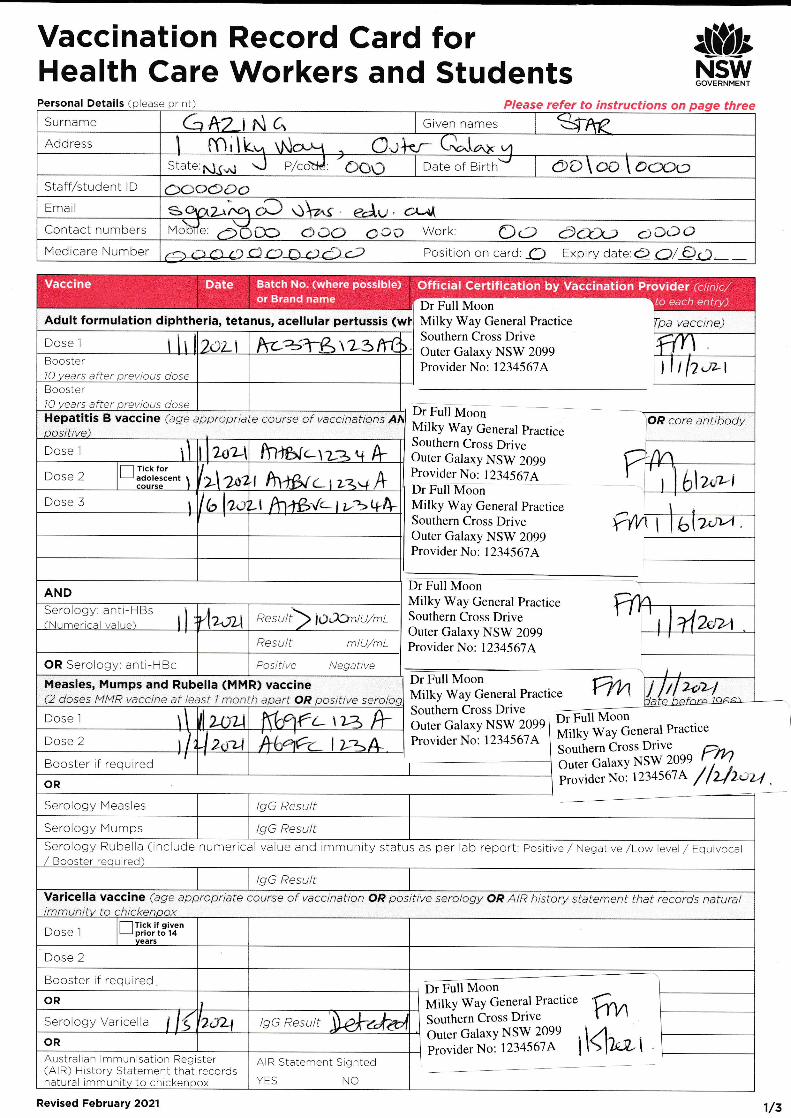
Vaccination Record Card forHealth Care Workers and Students
&,NSWGOVERNMENT
Personal Details ( ease Please refer to instructions on three
Dr Full MoonMilky Way General PracticeSouthern Cross DriveOuter Galaxy NSW 2099Provider No: 1234567A
Tpa vacclne)
m4
JLI
r2rn
I
Dr Full MoonMilky Way General pracriceSouthern Cross DriveOuter Galaxy NSW 2099Provider No: 12345674Dr Full MoonMilky Wa1 Ceneral PracticeSouthern Cross DriveOuter Galaxy NSW 2099Provider No: 1234567.4
OR core antibody
Dr Full MoonMilky Way General PracticcSouthern Cross DriveOuter Galaxy NSW 2099Provider No: 1234567,4
Dr Full MoonMilky Way General Practice
Southern Cross DriveDr Full Moon
Outer Galaxy NSW 2099
Provider No: 1234-567,4 Milky Way General Practice
Southern Cross Drive
Outer Gal axy NSW 2099
ProviderNo: I234567A 7f z/t-r,/
Surname G Azr N c., Given names
Address C-lSiate:gg.; J p/cottJ: 'CCIO Date of BirthJ e)D\co \ o(^)c)
Staff/student lD
Email qA/r^q c;".-: gt .a e.Av. dr-r{Contact numbers Mo co aco iO Work i) d*)') doooMedicare Number € >1r1X) aOLpA{) Position on card: Cl Expiry date:q1 O/€!) - _
Adult formulation diphtheria, tetanus, acellular pertussis (wI
Dose l rlrl )iLl kc=;l-&'tL3lYt ) nY\Booster1O years after previous dose
Hepatitis B vaccine (age appropriate course of
C-\Dose I
Boosterdoseafterto
Dose 2\
Tick foradolescent ltr\a, I h+f>r c t ,=,u h I blz--i
Dose 3 t 2o. '-l hllfr,/-lt-r*N\
AND
2a4Resu/t mlU/mL
OR Sero ogy ant -HBc Positive Negative
2-e,2-/Measles, Mumps and Rubella (MMR) vaccine(2 doses [4MR vacctne at ieasf 1 month apart OR pasttive seroloa
Dose l \ I ll zou Ktgt(. \)z /+k(,"1?c- I tz/\Dose 2
Booster if required
OR
Serology Meas es lgG Result
Serology Mumps lgG ResultSerology Rubella (include numerical value and immunity status as per lab report: Positive,/ Negative /Low level / Equivocal/ Booster required)
lgG ResultVaricella vaccine (agetmmunitv to chtckenpox
approprlate course of vacclnatlon OP posrtlve serology OR AIR history statement that records natural
Dose Iif given
prior to l4vears
Dose 2
Booster if required
ORI
Serology Varicella 2ctL1 lgG Result
OR
Australian lmmunisation Register(AlR) History Statement that recordsnatural immunity to chickenpox
AIR Statement Slghted
YES NO
Dr Full MoonMilky WaY General Practice
Soulhern Crclss Drivc
Outer GalaxY NSW 2099
Provider No: 1234567A
frv\41u1I
Batch No. (where possible)or Brand name
Off icia I Certif ication by Vacci nation Provid er (c I i n i c,/Vaccine Dateto each entry)
Revised February 2O21 1/z
er^A€
aOOOOc)
i 2$L\ z lVtr
Serology: anti-HBs(NLrmerical rralr rc) I rlz-ozt Resu/) iO,Ajntu/mt
I
I
2ifZ)I
Surname Caku rt)r,r Given
=r7\€Date of Birth frT: oclc&D StaffAtudent 1D
Contact Mobiie: O AO clJ3 Work: OC oOQ) C{x-D
I
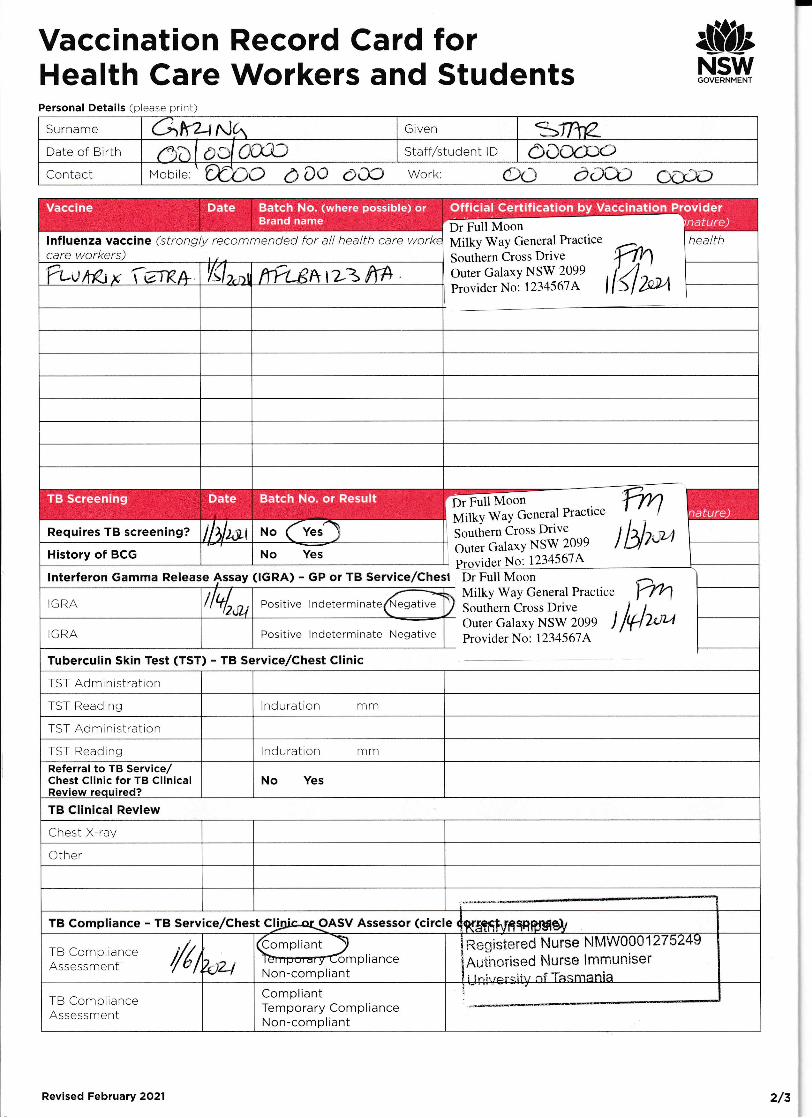
Vaccination Record Card forHealth Care Workers and Students
&;NSv[f
Personal Details (please print)
lnfluenza vaccine (strongly recommended for all health care workecare workers)
health
y'ua&, r,; {etB-+ [{lt,",t ftrts*tzz ff#
Dr Full MoonMilky WaY General Practice
Southern Cross DriveOuter GalaxY NSW 2099
Provider No: 1234567A bt4
Requires TB screening? iltlzor r.ro (veslHistory of BCG No Yes
IGRA il4,*, oositive lndetermrrateKIilI\
TST Administration
]GRA Positive lndeterminate Negative
lnterferon Gamma Release
Tuberculin Skin Test (TST) - TB Service/Chest CIinic
fullrl,*
tbfp,Dr Full Moon
PractrceGeneralwayMilkYveDtiCrosSouthern
2099NSWGal axyOuterA6'l51 234N
(IGRA) - GP or TB Service/Chesl Dr Full MoonMilky Way General PracticeSouthern Cross DriveOuter Calaxy NSW 2099 JProvider No: 123.1567A
TST Reading nduration mm
TST Administration
TST Reading I nd u ratio n mmReferral to TB Service/Chest Clinic for TB ClinicalReview reouired?
No Yes
TB Clinical Review
Chest X-ray
Other
TB Compliance - TB Service/Chest CjjAic-oqQASV Assessor (circle ( KStfiT.IfiqqRIHB}
ltrTB ComplranceAssessment 7,J2-l Non-compliant
mplianceRsrtistered Nurse t{MW000 1 27 5249
Auii-roi"ised ir!u rse i mmuniseri lr.i, rar:i'ir,, ri -[h.r,fifenia
TB ComplianceAssessment
CompliantTemporary ComplianceNon-compliant
TB Screening Date Batch No. or Result
Vaccine Date Official Certification by Vaccination ProviderBatch No. (where possible) orBrand name
Revised February 2O2l 2/z
CCccPo







