Download - Cardio diseases.ppt
7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 1/17
Diseases
of the CVSystem

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 2/17
CAD
• Refers to the variety of pathologic
conditions that cause narrowing
of the coronary arteries• Atherosclerosis- Deposits of
cholesterol and lipids within the
walls of the artery
• Risk Factors: Family history,
hyperlipidemia, smoking, DM, HPN,
obesity, sedentary/stressful
lifestyle
7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 3/17
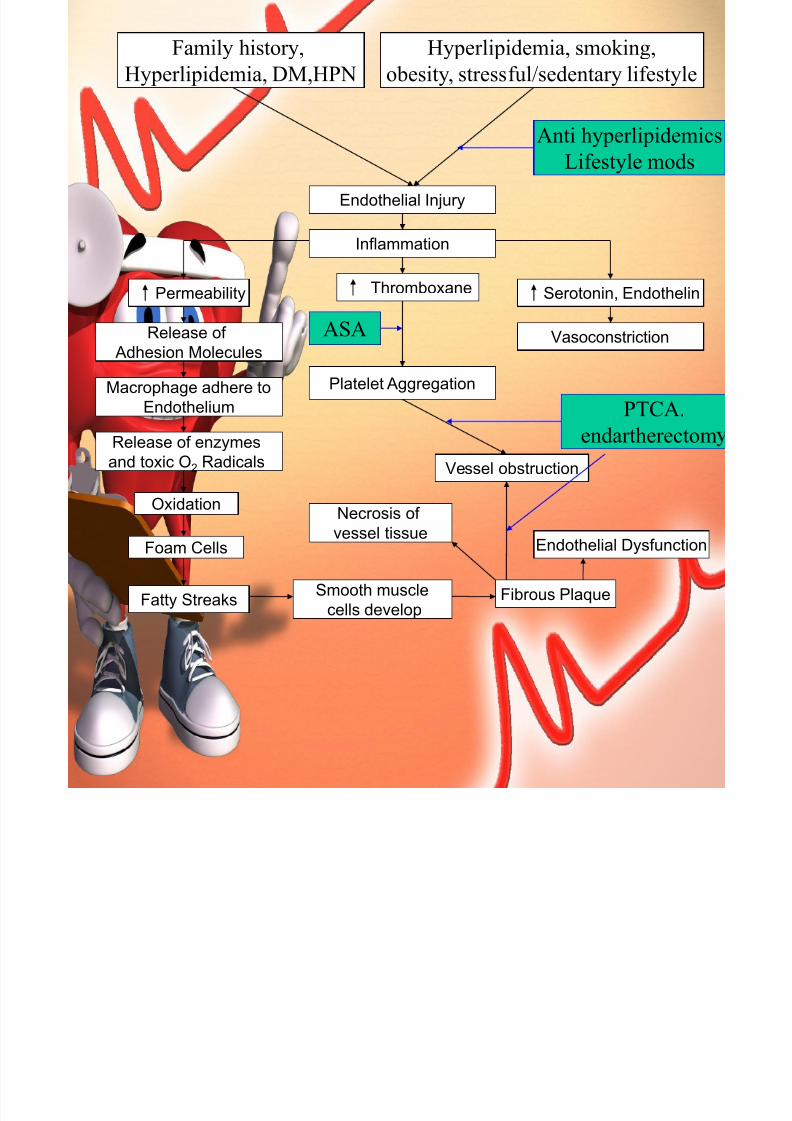
Platelet Aggregation
Release of enzymes
and toxic O2 Radicals
Endothelial Injury
Inflammation
Fatty Streaks
Vasoconstriction
Macrophage adhere to
Endothelium
Release of
Adhesion Molecules
Oxidation
Foam Cells
Thromboxane Serotonin, EndothelinPermeability
Vessel obstruction
Fibrous PlaqueSmooth muscle
cells develop
Necrosis of
vessel tissueEndothelial Dysfunction
Family history,
Hyperlipidemia, DM,HPN
Hyperlipidemia, smoking,
obesity, stressful/sedentary lifestyle
Anti hyperlipidemics
Lifestyle mods
ASA
PTCA.
endartherectom

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 4/17
Metabolism of Fats
Dietary Fats
Micelles absorbed into intestines
Gemfibrozil, niacin
Hmg CoA blockers
Fibrates
Fat emulsification
Liver proceeds fats
Into HDL,LDL
Gall bladder releases bile
Bile acid sequestrants
Enter circulation and
periphery
Bile acids recycled
to liver
Small Intestines
Stomach
Chylomicrons absorbed into
lymphatics
7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 5/17
Myocadial
Infarction
• Death of myocardial cells from
inadequate oxygenation
• Signs and symptoms: Pain, N&V,
dyspnea, cool and clammy skin,
elevated temperature,initial
increase, then drop in
BP,restlessness• Laboratory findings: Elevated WBC,
CPK, AST, LDH
• ECG Changes: pathologicQ wave, ST segment elevation,
inverted T wave

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 6/17
Types of MITYPE Location of
ST/Q wave
changes
Artery
Occluded
Anterior V 1-V 4 LADA
Inferior II, III, Avf RCA
Lateral I, Avl, V5-V6 LCX
Posterior V 1-V 2 RCA

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 7/17
Types of MITYPE Layer affected
Subendocardial Inner layer
Subepicardial Inner and middle
layer
Transmural All layers
d

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 8/17
ASHD,CAD, DM, age, gender, HPN,
Stress, thrombosis/embolism
Myocardial Ischemia
Anaerobic Metabolism
Cellular Hypoxia
O2 Supply ≠ O2 Demand
H Ions Lactic Acid
Chest Pain
LDH Flipping
Cell membrane permeability
Sympathetic ResponseK,Ca,Mg
Glucose,
Fatty Acids BP
After Load
N & V
Cool,
Clammy Skin
Diaphoresis HR
Disatolic Filling
CO
Leukocytosis,ESR
Cellular Necrosis
CKMB, TROP I, T
Contractility
O2, CBR,
Laxatives,
NTG,
LifestyleMod
PTCA,CABG,ASA Thrombolytocs
MorphineAntiarrythmics
Cardiotonics

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 9/17
Rheumatic Heart
Disease
• Inflammatory disorder that involves
the heart, joints, muscle and CNS
• Assessment findings• Major (Jone’s Criteria)
• Carditis
• Aschoff nodules,
• valvular insuffucienscy
• Cardiomegaly
• SOB, hepatomegaly, edema
• Polyarthritis
• Sunbcutaneus nodules• Chorea/ Sydenham’s chorea/St.
Vitus’ dance
• Erythema marginatum

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 10/17
• Minor
• History of GAS infection
• Fever
• Elevated ESR, WBC, ASO titer

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 11/17
GAS infection
(Beta hemolytic Streptococcus)
Binds to receptors
within….
Activation of T cells by streptococcal antigens
Inflammatory
responseFever, elevated
WBC,ESR
Heart JointsCNS
Polyarthritis
Swelling, heat, pain
arthralgiaSubcutaneus nodules
Decrease stimulation
Safety precautions
Chorea
Anti-inflammatory
ents ( steroids,NSAIDS)
Penicillin/
Erythromycin
Positioning
ASA

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 12/17
Heart
Pericarditis
Clumping of vegetation
With platelets & fibrin
Erosion of leaflet
contact
Inflammation of
valve leaflets
EndocardialInflammation
Scarring/shortening
Chest pain
Decreased elasticity
Friction rub
Aschoff nodules
Fibrin depositsDevelop with area o
necrosis
Penetrates
myocardium
Mitral/ Tricuspid
regurgitation
CHF
Murmur
Valve replacement,
thrombolytics
Bed rest
7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 13/17
Arrythmias
• Disruption in the normal events of
cardiac cycle which may/ may notlead to decreased c rdi c output
(to which the manifestations are
attributed).
7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 14/17
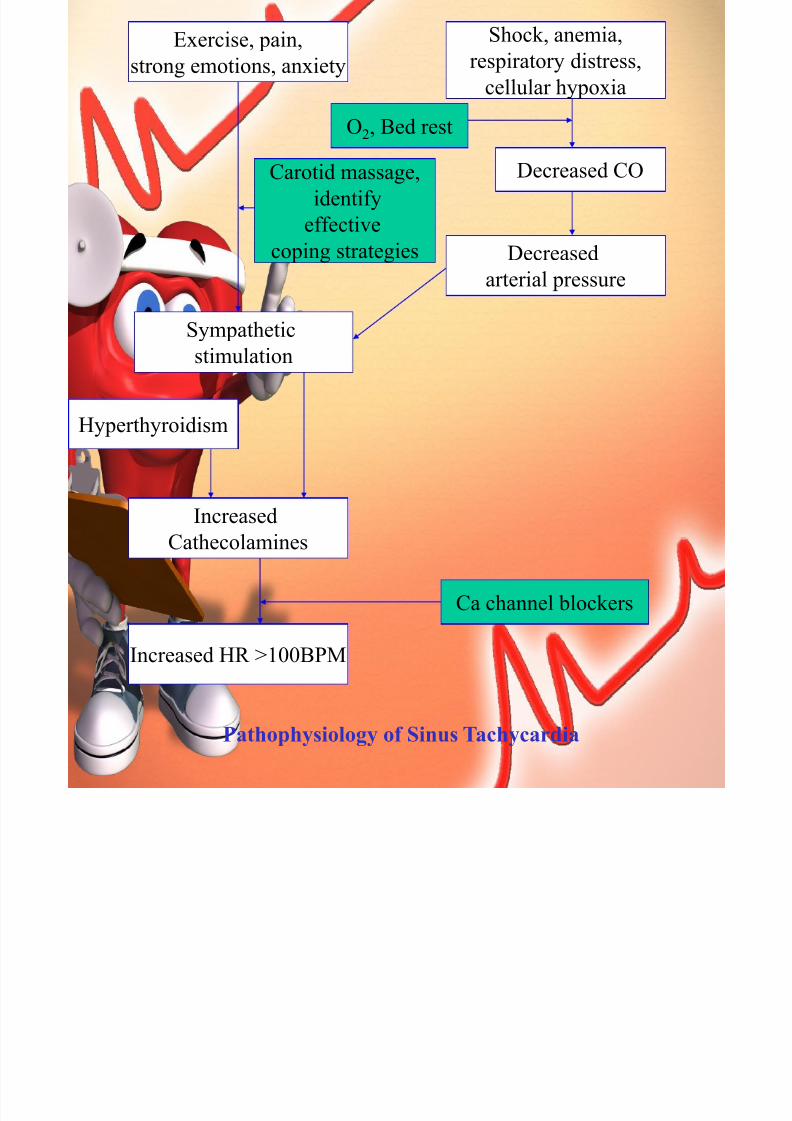
Shock, anemia,
respiratory distress,
cellular hypoxia
Exercise, pain,
strong emotions, anxiety
Carotid massage,
identify
effectivecoping strategies
O2, Bed rest
Ca channel blockers
Increased HR >100BPM
Hyperthyroidism
Increased
Cathecolamines
Sympathetic
stimulation
Decreased
arterial pressure
Decreased CO
Pathophysiology of Sinus Tachycardia

7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 15/17
Hyperkalemia, digoxin,
MI, hypothermia
Symphatomimetics
pacers
Late hypoxia
HR <60BPM
Decreased
automaticity
Increased vagal
stimulation
Decreased
ATP
Sleep, valsalva maneuver
vomiting
O2, Bed rest
Pathophysiology of Sinus Bradycardia
7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 16/17
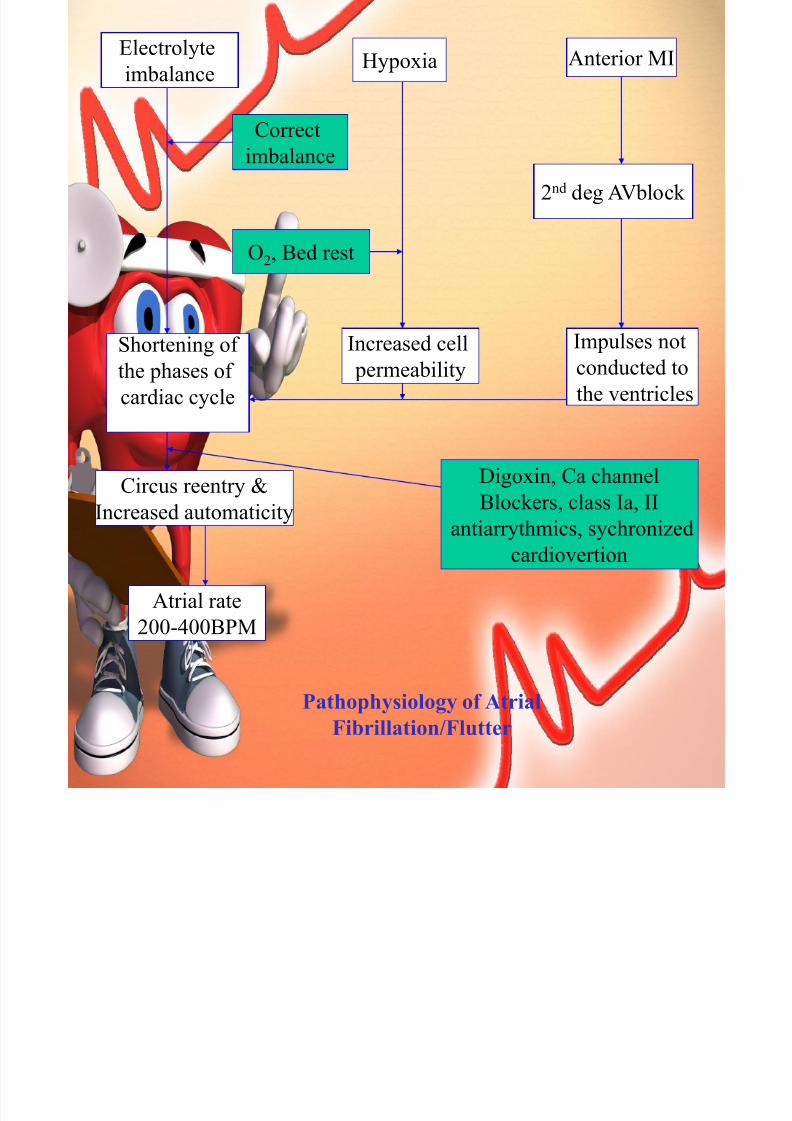
Pathophysiology of AtrialFibrillation/Flutter
Electrolyte
imbalance
Circus reentry &
Increased automaticity
Digoxin, Ca channel
Blockers, class Ia, II
antiarrythmics, sychronized
cardiovertion
Correct
imbalance
Atrial rate
200-400BPM
Impulses notconducted to
the ventricles
2nd deg AVblock
Increased cell permeability
Shortening ofthe phases of
cardiac cycle
Anterior MIHypoxia
O2, Bed rest
7/27/2019 Cardio diseases.ppt
http://slidepdf.com/reader/full/cardio-diseasesppt 17/17
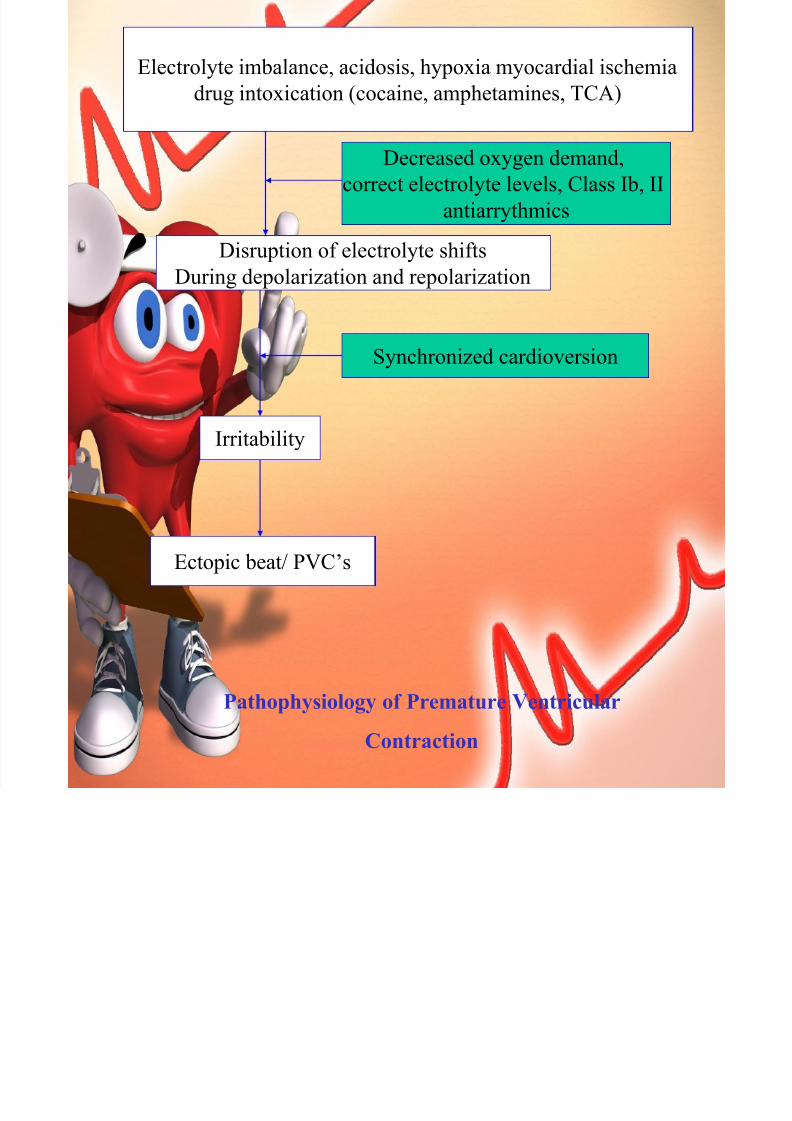
Pathophysiology of Premature Ventricular
Contraction
Electrolyte imbalance, acidosis, hypoxia myocardial ischemia
drug intoxication (cocaine, amphetamines, TCA)
Disruption of electrolyte shifts
During depolarization and repolarization
Decreased oxygen demand,
correct electrolyte levels, Class Ib, II
antiarrythmics
Synchronized cardioversion
Irritability
Ectopic beat/ PVC’s







