
Cataract in the 21st century
Liana Al-Labadi, O.D.Lecture 9
Thanks To The Ohio State College of Optometry
Presenile cataracts
Presenile Cataract:
Myotonic Dystrophy
Diabetes
Atopic Dermatitis
Blue-Dot Cataract
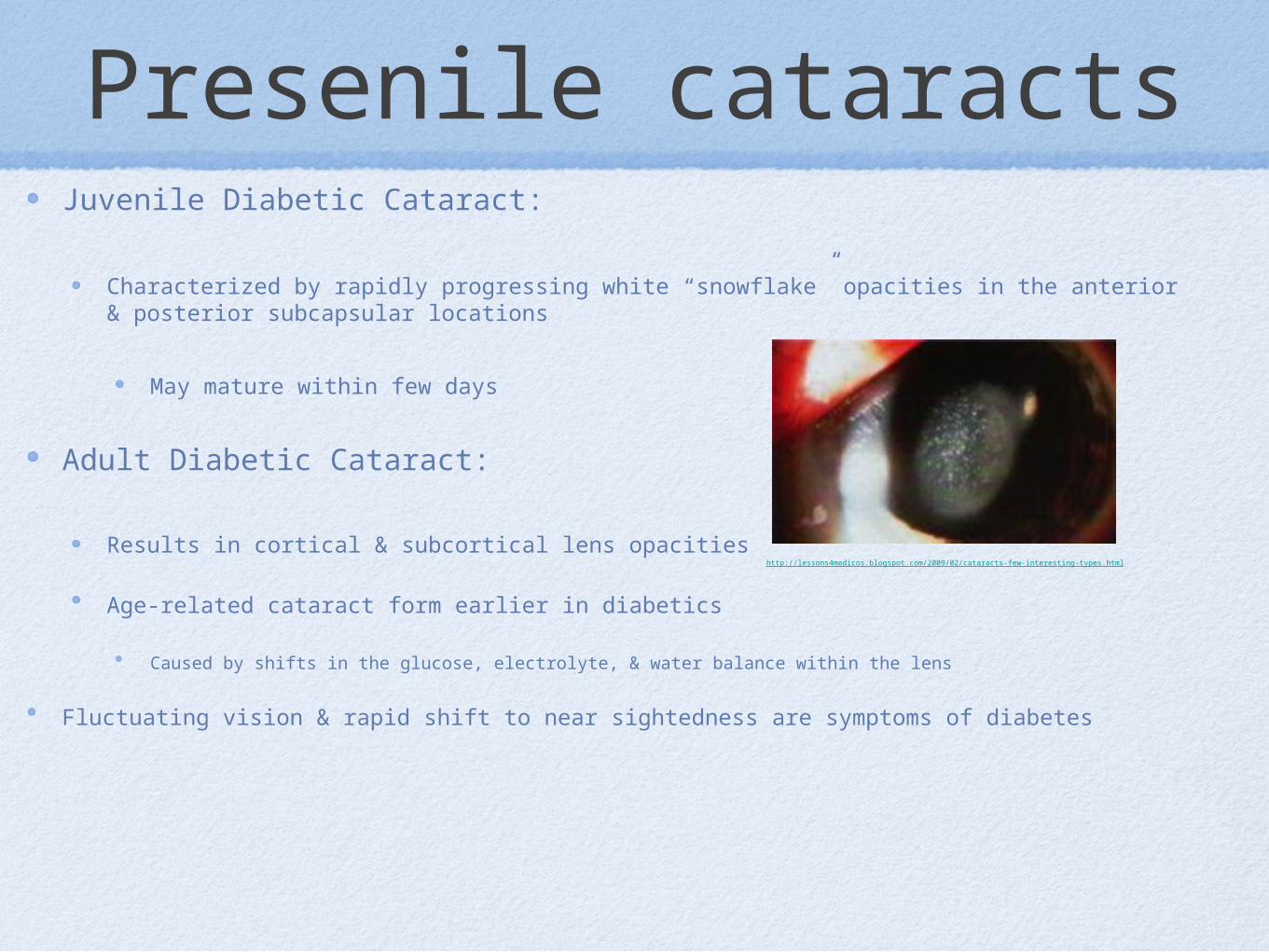
Presenile cataractsJuvenile Diabetic Cataract:
Characterized by rapidly progressing white “snowflake” opacities in the anterior & posterior subcapsular locations
May mature within few days
Adult Diabetic Cataract:
Results in cortical & subcortical lens opacities
Age-related cataract form earlier in diabetics
Caused by shifts in the glucose, electrolyte, & water balance within the lens
Fluctuating vision & rapid shift to near sightedness are symptoms of diabetes
http://lessons4medicos.blogspot.com/2009/02/cataracts-few-interesting-types.html
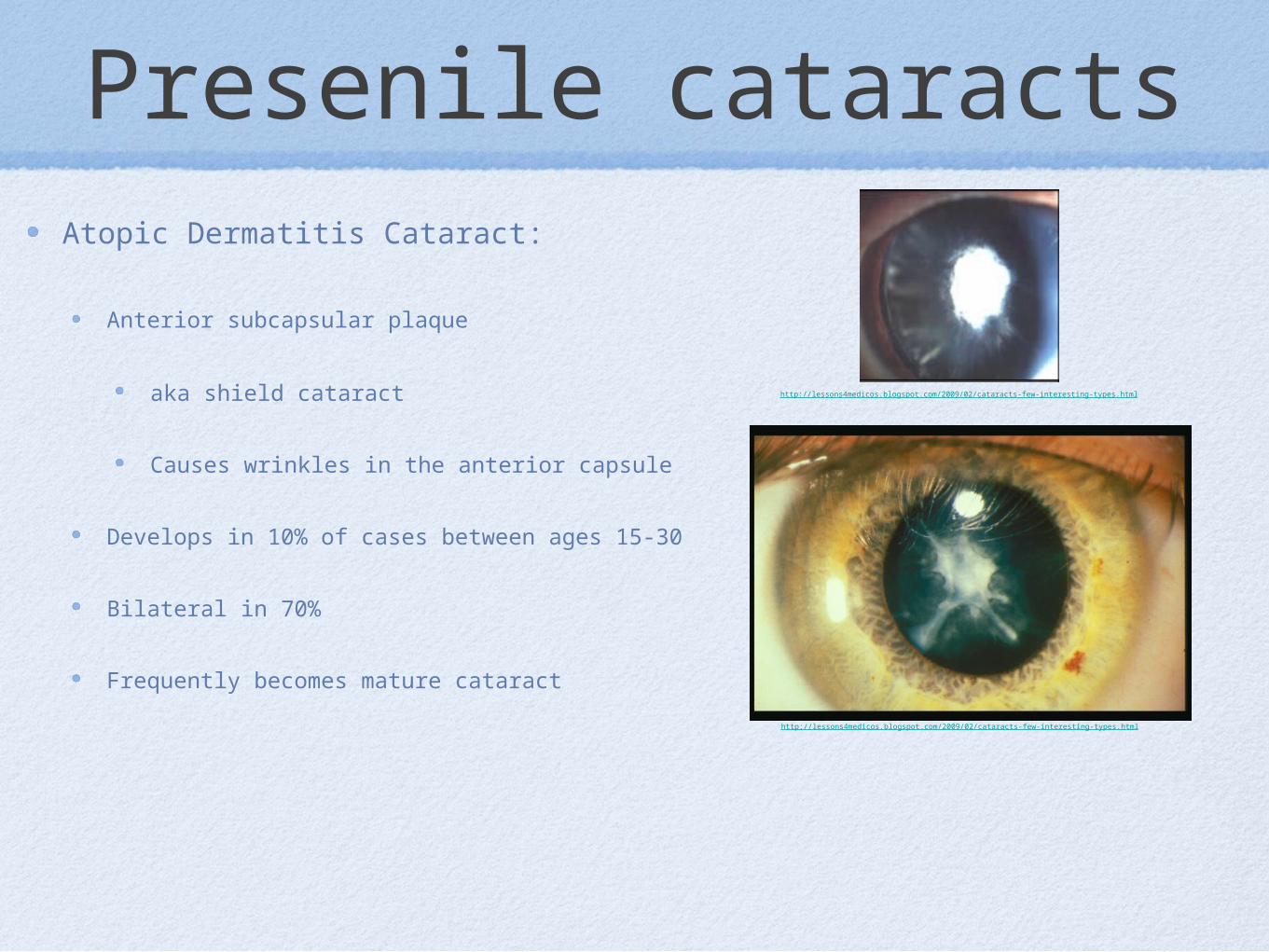
Presenile cataractsAtopic Dermatitis Cataract:
Anterior subcapsular plaque
aka shield cataract
Causes wrinkles in the anterior capsule
Develops in 10% of cases between ages 15-30
Bilateral in 70%
Frequently becomes mature cataract
http://lessons4medicos.blogspot.com/2009/02/cataracts-few-interesting-types.html
http://lessons4medicos.blogspot.com/2009/02/cataracts-few-interesting-types.html
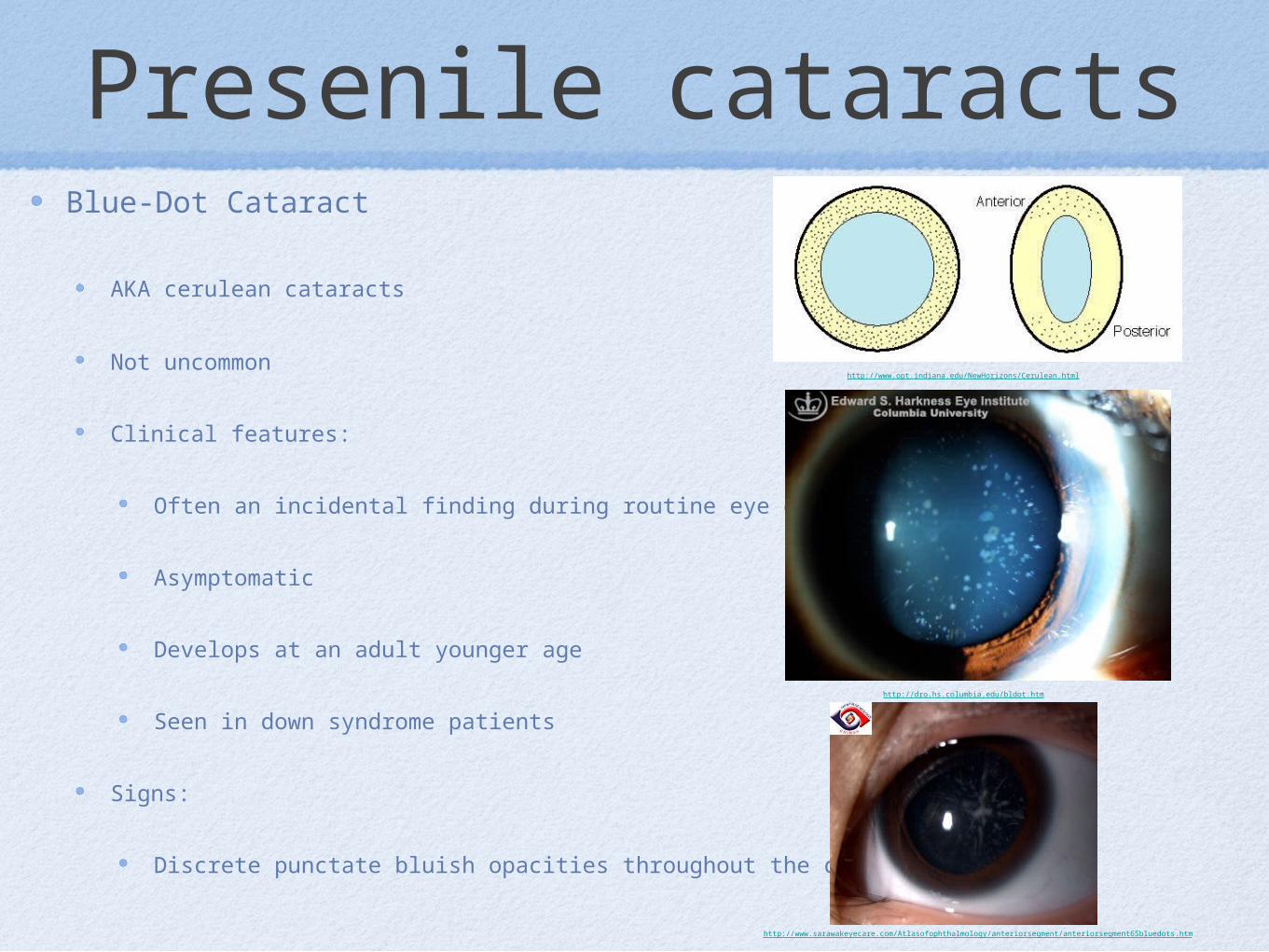
Presenile cataractsBlue-Dot Cataract
AKA cerulean cataracts
Not uncommon
Clinical features:
Often an incidental finding during routine eye exam
Asymptomatic
Develops at an adult younger age
Seen in down syndrome patients
Signs:
Discrete punctate bluish opacities throughout the cortex
http://dro.hs.columbia.edu/bldot.htm
http://www.sarawakeyecare.com/Atlasofophthalmology/anteriorsegment/anteriorsegment65bluedots.htm
http://www.opt.indiana.edu/NewHorizons/Cerulean.html
Traumatic cataract
Traumatic cataract causes:
Penetrating injuries
Concussion injuries
Electric shock
Radiation
Traumatic cataractTraumatic cataract:
Most common complication of non-perforating & perforating injuries to the globe
Intraocular trauma by surgical instruments, lodged FB or intraocular filtration tube are possible causes
Clinical Features:
Cataract formation after non-penetrating injury (contusion or concussion) may occur without any damage to lens capsule
Cataract formation may be slowly progressive or mature suddenly
No always easy to observe initial changes of the lens
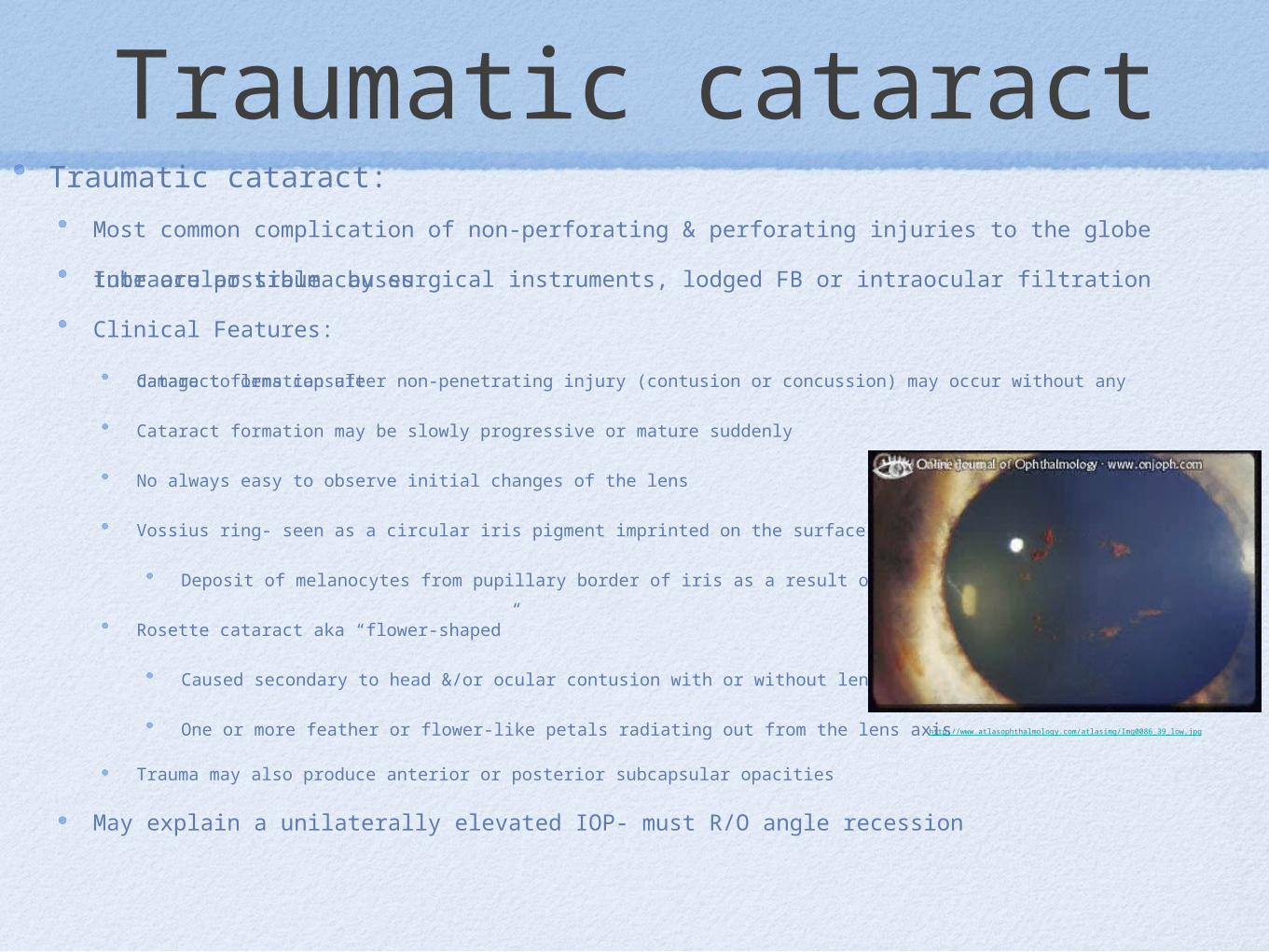
Vossius ring- seen as a circular iris pigment imprinted on the surface of the lens anterior capsule
Deposit of melanocytes from pupillary border of iris as a result of a concussion
Rosette cataract aka “flower-shaped”
Caused secondary to head &/or ocular contusion with or without lens rupture
One or more feather or flower-like petals radiating out from the lens axis
Trauma may also produce anterior or posterior subcapsular opacities
May explain a unilaterally elevated IOP- must R/O angle recession
http://www.atlasophthalmology.com/atlasimg/Img0086_39_low.jpg
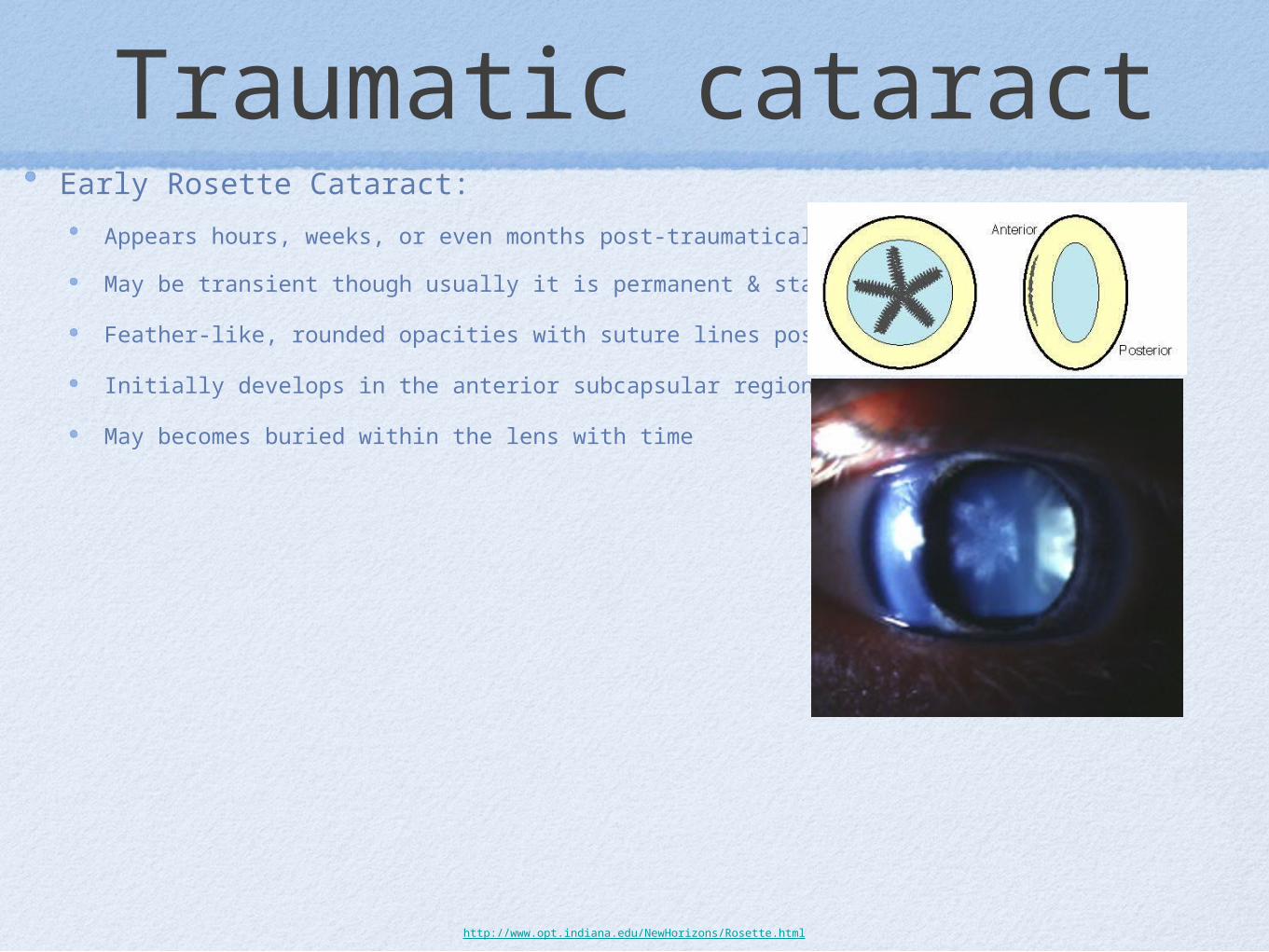
Traumatic cataractEarly Rosette Cataract:
Appears hours, weeks, or even months post-traumatically
May be transient though usually it is permanent & stationary
Feather-like, rounded opacities with suture lines positioned centrally
Initially develops in the anterior subcapsular region
May becomes buried within the lens with time
http://www.opt.indiana.edu/NewHorizons/Rosette.html
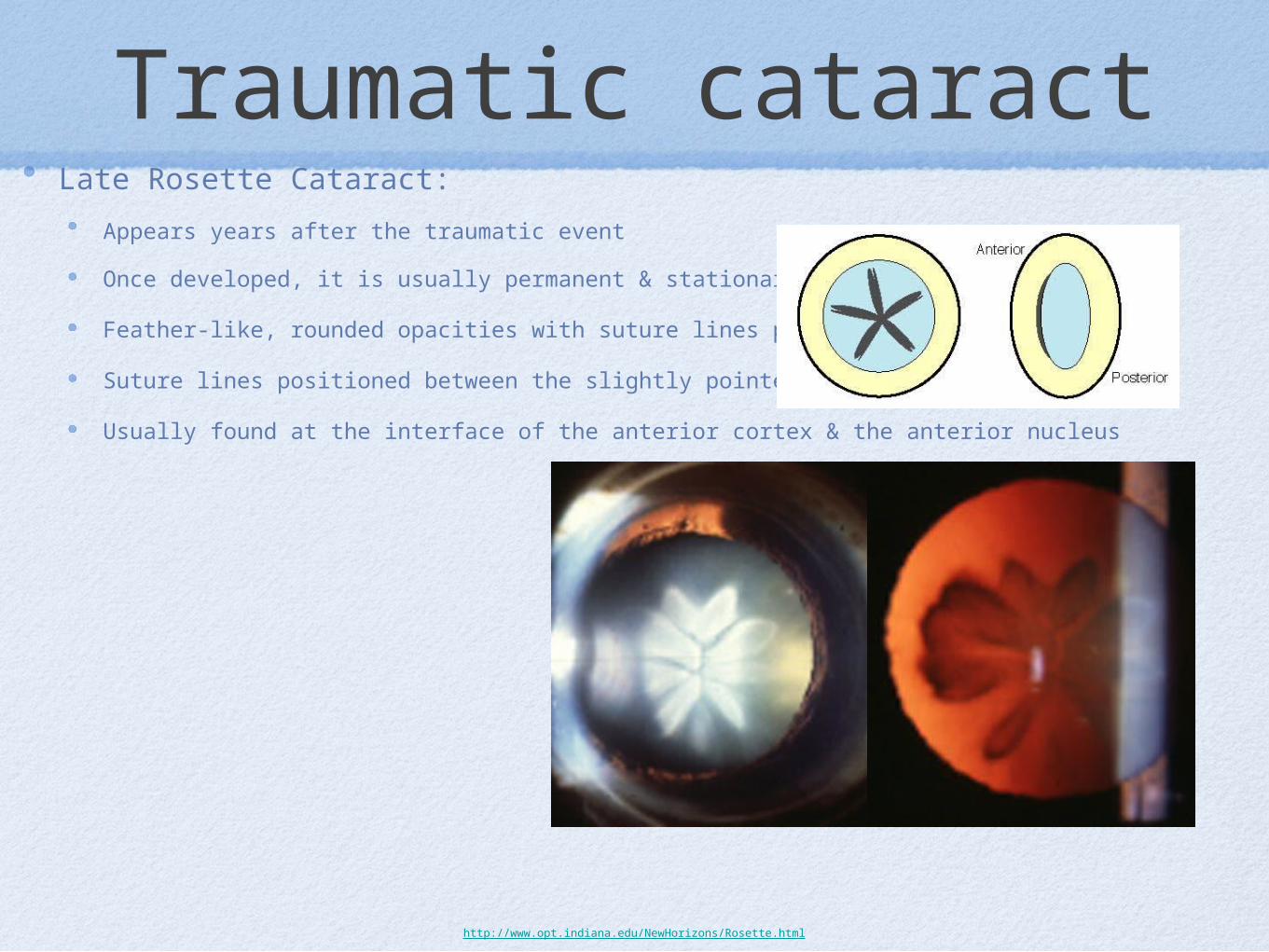
Traumatic cataractLate Rosette Cataract:
Appears years after the traumatic event
Once developed, it is usually permanent & stationary
Feather-like, rounded opacities with suture lines positioned centrally
Suture lines positioned between the slightly pointed lobes
Usually found at the interface of the anterior cortex & the anterior nucleus
http://www.opt.indiana.edu/NewHorizons/Rosette.html

Toxic Cataract
Chloropromazine Cataract:
Used in the treatment of psychotic disorders & hyperexcitability
Cataract begins as fine particulate deposits in the anterior subcapsular area which progresses to a star-shaped opacity
Usually develops after treatment for at least 2 years with more than 300mg/day
http://www.opt.indiana.edu/NewHorizons/Chlorpromazine.html
Toxic CataractToxic Cataract:
Steroids
Long-acting miotics
Amiodarone
Busulfan- cancer drug
Secondary cataract
Secondary PSC can develop with:
Chronic anterior uveitis
Ciliary body tumor
Ionizing Radiation
MRI causes NS, CC, ASC
High myopia
Hereditary fundus dystrophies
RP
Leber congenital Amaurosis
Gyrate Atrophy
Wagner & Stickler Syndrome
Angle closure glaucoma
Glaucomflecken
Secondary cataract
Glaukomflecken
Focal cortical opacities resulting from:
Acute closure glaucoma
Sudden IOP spike
Results in central, anterior subcapsular opacities
Subepithelial lens opacification
Due to lens epithelial cells ischemia & necrosis caused by elevated IOP

Glaukomflecken
Metabolic Cataract
Wilson Disease- Metabolic AR disease
Multi-system disorder due to impaired hepatic excretion of copper
Results in low serum ceruloplasmin level & subsequent elevated serum & urine copper levels
Excess copper in CNS, liver, kidney, cornea & other organs
This copper deposition leads to liver & brain damage

Metabolic Cataract
Wilson Disease- Metabolic AR disease
Symptoms:
Ocular complaints are rare
May experience sx of cirrhosis, neurological disorders, psychiatric problems, or renal disease
Begins typically between 5 to 40 years of age
Signs
Kayser-Fleisher ring
A 1-3mm brown, green, or red band that represents copper deposition in the peripheral descemet membrane
Present in 50-60% of patients with isolated hepatic involvement
Present in more than 90% of patients with neurological manifestation
“Sunflower” cataract- due to anterior & posterior subcapsular copper deposition
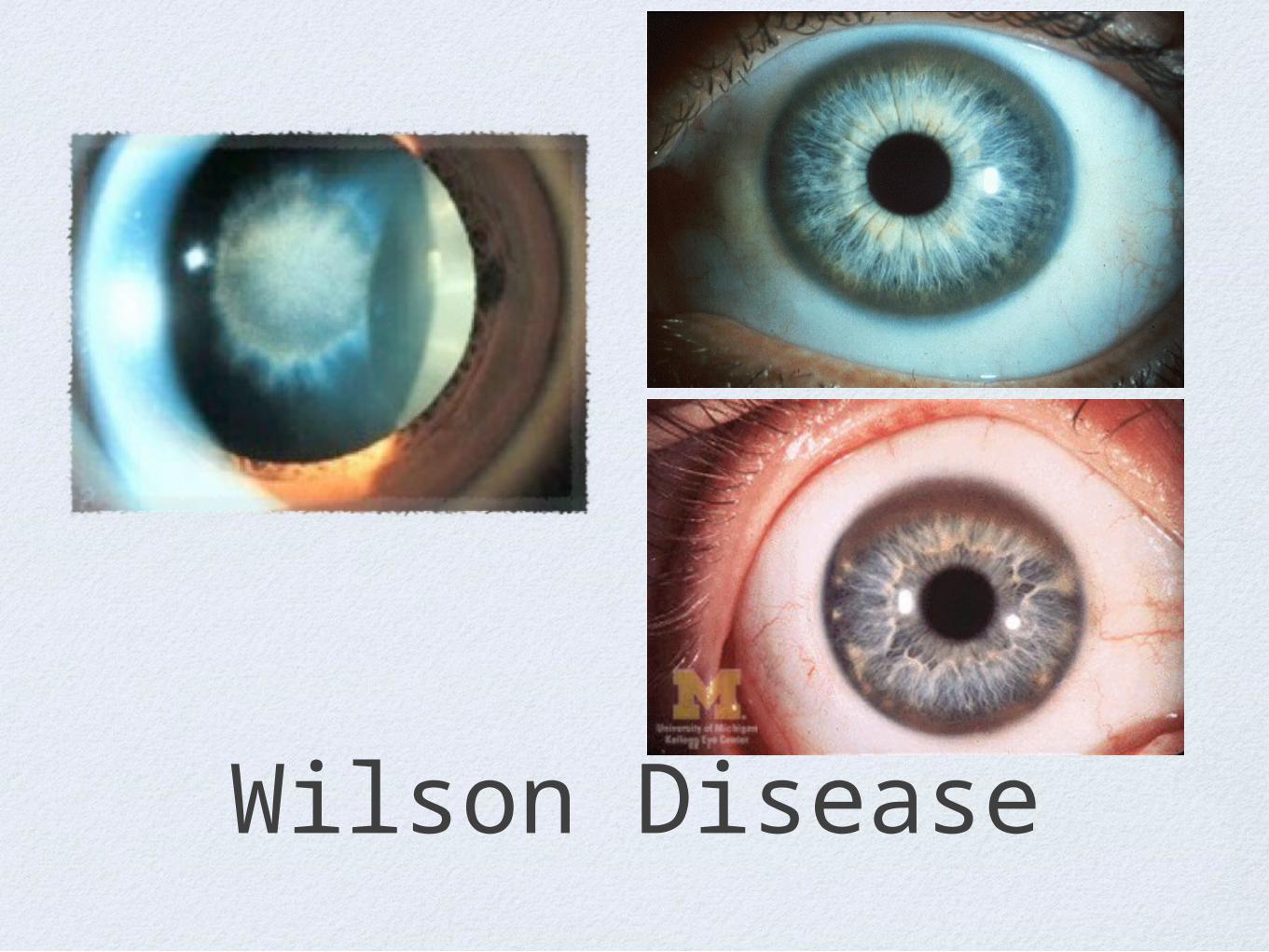
Wilson Disease







