
1
Understanding and Managing
Reflux/GERD in
Typically Developing Babies
And Older Children with Medical Complexities
A Discussion for Caregivers and
Healthcare Professionals
Developmental and Physiological Considerations,
Therapeutic Approaches, and Recommendations
by Mary B. Pengelley, PT, DPT, ATP
Provider Disclaimer
• Allied Health Education and the presenter of
this webinar do not have any financial or other
associations with the manufacturers of any
products or suppliers of commercial services
that may be discussed or displayed in this
presentation.
• There was no commercial support for this
presentation.
• The views expressed in this presentation are
the views and opinions of the presenter.
• Participants must use discretion when using the
information contained in this presentation.

2
Background and Introductions
Peace Corps Jamaica
Charter School
Pediatric Private Practice
Community Service
Reminders Before We Start
This webinar is aimed at improving understanding, critical thinking and clinical judgment when working with children with reflux
The information presented in this webinar is based on personal and clinical experiences, extensive review of current research, and some ‘gems’ gained from continuing education and graduate school
Please use your own best reasoning and clinical judgment when working with children and making suggestions to families
Refer to appropriate specialists as needed for concerns outside your scope of practice or professional judgment

3
Objectives1. Definitions: What’s the Difference?
a. GER
b. GERD
2. Causes: Getting the Big Picture
a. Typical Infant Anatomy and Physiology
b. Normal Changes to Expect with Development
c. Norms of Various Cultural Practices
d. Perinatal and long term medical complications
3. Consequences: So What?
a. Developmental Delays/Torticollis
b. Sensory Defensiveness/Picky Eaters
c. Poor Weight Gain/Failure to Thrive
4. Treatment Tricks and Techniques: There’s Help! a. Non-pharmaceutical – diet, volume, positioning, strengthening
b. Pharmaceutical
c. Surgical
Definitions: GER1,2 - “Happy Spitters”
Uncomplicated Gastroesophageal Reflux (GER)1
GER: the passage of gastric contents into the esophagus with or without regurgitation and vomiting.
50% of normal full term infants, 0-3 months spit up 1x/day or more
Most common concern at 4-month well-baby check-up
Baby feeds well
Normal weight gain
No unusual irritability

4
Definitions: Gastroesophageal Reflux Disease/GERD1,2
GERD: when GER leads to troublesome symptoms that affect daily functioning and/or results in complications
Refractory GERD: GERD, not responding to optimal treatment after 8 weeks
10% of Full-term Infants
Esophageal – ‘silent reflux’
Extraesophageal
Reflux with Pathological Consequences
Esophagitis/Pain
Nutritional compromise/Poor Weight Gain
Respiratory Complications
Normal vs. Red Flags

5
What do RED FLAGS mean?Time to refer out!
General
•Weight Loss•Lethargy•Fever•Excessive Irrritablity/pain
•Dysuria•Onset > 6 months or increasing/persisting > 12-18 months
•May be due to systemic infections, UTI, otitis media, or diagnosis other than GERD
Neurological
•Bulging fonatanels•Rapidly increasing head circumference
•Seizures•Micro or Macro-cephaly
•Subdural hematoma•Intracranial hemorrhage
•May be due to raised intracranial pressure, meningitis, brain tumor or hydrocephalus, shaken baby syndrome
Gastrointestinal
•Persistent Forceful vomiting
•Nocturnal vomiting•Bilious vomiting•Blood in vomit•Rectal bleeding•Chronic diarrhea •Abdominal distension
•Many possible causes: anatomic abnormalities such as pyloric stenosis, intestinal obstruction, GI bleeding, food allergy, gastroenteritis, dysmotility, gastroparesis, appendicitis, pancreatitis
Cardiopulmonary
•Decreased O2 satswhile feeding (cyanosis)
•Poor feeding/sucking•Fatigues quickly while feeding
•Shortness of breath•General lethargy
•May be related to congenital heart disease, cardiac failure, broncopulmonarydysplasia, pneumonia, upper airway infections, restrictive airway disease (asthma)
Metabolic/Toxic
•Normal at birth, develops anorexia within weeks of birth
•Excessive vomiting in newborn
•Convulsions•Jaundice •Hyper or Hypo-ventilation
•Poor thermoregulation
•Galactosemia, hereditary fructose intolerance, metabolic acidosis, urea cycle defects, amino acidemia, congenital adrenal hyperplasia
American Academy
of Pediatrics
Differential
Diagnosis of
GER/GERD 2,3
Recognize Red Flags
Understand complicated GERD
Caregiver Education for Happy Spitters
If not resolved by 18 months consult with GI
6
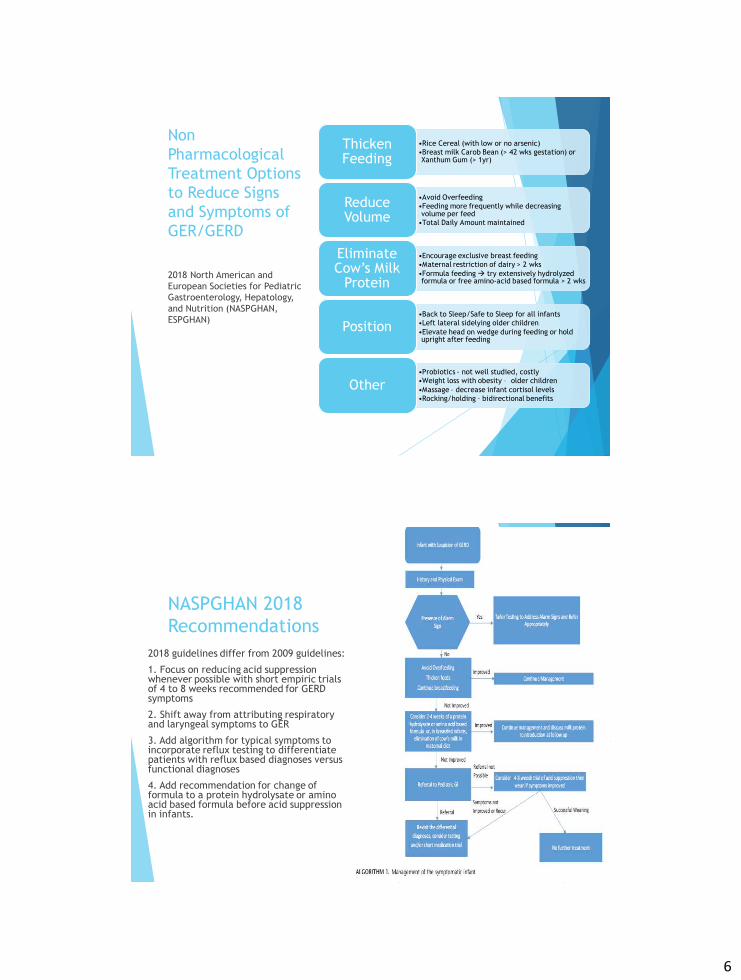
Non Pharmacological Treatment Options to Reduce Signs and Symptoms of GER/GERD
•Rice Cereal (with low or no arsenic)•Breast milk Carob Bean (> 42 wks gestation) or Xanthum Gum (> 1yr)
Thicken Feeding
•Avoid Overfeeding•Feeding more frequently while decreasing volume per feed
•Total Daily Amount maintained
Reduce Volume
•Encourage exclusive breast feeding•Maternal restriction of dairy > 2 wks•Formula feeding try extensively hydrolyzed formula or free amino-acid based formula > 2 wks
Eliminate Cow’s Milk
Protein
•Back to Sleep/Safe to Sleep for all infants•Left lateral sidelying older children•Elevate head on wedge during feeding or hold upright after feeding
Position
•Probiotics - not well studied, costly•Weight loss with obesity – older children•Massage – decrease infant cortisol levels•Rocking/holding – bidirectional benefits
Other
2018 North American and European Societies for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN, ESPGHAN)
NASPGHAN 2018 Recommendations
2018 guidelines differ from 2009 guidelines:
1. Focus on reducing acid suppression whenever possible with short empiric trials of 4 to 8 weeks recommended for GERD symptoms
2. Shift away from attributing respiratory and laryngeal symptoms to GER
3. Add algorithm for typical symptoms to incorporate reflux testing to differentiate patients with reflux based diagnoses versus functional diagnoses
4. Add recommendation for change of formula to a protein hydrolysate or amino acid based formula before acid suppression in infants.

7
Understanding the Big Picture in Typical Development
Review
Infant
A & P
Changes with Development
Impact of Cultural Practices
Normal ‘Spit-up’ or Reflux? When is it a problem?

8
Typical Infant Anatomy and Physiology
Understanding Development of the Infant Respiratory and GI Systems

9
Musculo-Skeletal
Newborn Anatomy
and Physiology:
1.Triangular shaped chest
Ribs horizontal &
cartilaginous
1.Diaphragmatic nose
breather &
pulmonary reserve
Thin intercostal
spacing & sternal
stability
1.Demands paradoxical breathing
1.Soft trachea, high Respiratory Rate, low Tidal
Volume

10
• Visible sternal retraction due to soft cartilaginous ribs and sternum
• Strong abdominal contractions
• Crying helps develop abdominal strength and stretch out the intercostals for deeper breathing
3-6 Months What Happens in Normal Development
Baby begins reaching with UE’s against gravity
Trunk extensor control develops if baby is given adequate tummy time
Anterior chest wall opens up and becomes more rectangular
Ribs remain fairly horizontal precluding development of intercostal muscles
Increased tidal volume and decreased respiratory rate
Baby remains primarily diaphragmatic breather

11
3-6 Months • Chest cavity is
more rectangular shaped
• Ribs remain fairly horizontal until baby begins sitting independently.
6-12 Months What Happens in Normal Development
Baby begins sitting. Antigravity control means strength in all muscles of trunk are above a fair grade (3/5)
Ventilation no longer impacted by contact with supporting surface in prone
Gravity and developing trunk muscles pull and rotate the ribs down, thereby elongating chest wall, especially lower ribs
Downward rotation of ribs improves overall efficiency and strength of diaphragm, abdominals, and intercostal muscles (think: length-tension curve)

12
6-12 Months• Ribs begin to rotate downward
and intercostal spaces are wider.
• This allows for deeper, more efficient breathing patterns
• Rib position also helps the diaphragm to assume a more dome-shape at rest.
Let’s Take a Closer Look at the Diaphragm, Intercostals and Abdominals
Lateral, anterior and posterior fibers of diaphragm attach to the lower borders of the ribs 8, 9, and 10 in a ring
As ribs rotate downward the diaphragm becomes domed shaped, allowing for greater excursion with contraction -> stronger diaphragmatic contractions
Abdominal viscera supported by strong abdominal muscles provide intra-abdominal pressure up on the diaphragm for more effective diaphragmatic breathing and for coughing, by helping diaphragm to relax in a domed position.
Intercostal spacing increases with downward rotation of ribs, allowing them to stabilize chest wall and expand laterally and anteriorly during inhalation
Intercostal muscles also help compress chest wall during coughing

13
Diaphragm attaches to the ribs in a complete ring
What’s so important about the Diaphragm? • Note the position of the
esophagus passing through the diaphragm.
• This is also the exact point of the Gastro-Esophageal Sphincter.
• A dome-shaped diaphragm, when it contracts, helps to close off the GE sphincter, thereby decreasing reflux.
• A more horizontally (flat) shaped diaphragm does not contract strongly enough to assist with closure of the sphincter.
• This results in greater chance of GE reflux, especially with supine lying and trunk flexion.
View from below.

14
Action of the Diaphragmhttps://www.youtube.com/watch?v=Fn3W1xJ8ERo
Diaphragm is relaxed on exhalation and rises up into dome shape. GE sphincter is more relaxed with exhalation.
Diaphragm is contracting on inhalation and flattens out, this closes off the GE sphincter with every breath if there is excursion of the muscle
GE sphincter
The Bottom Line with Typical Infant Development and Reflux
All infants will experience reflux due to anatomical alignment of ribs, decreased diaphragmatic excursion and strength, short esophagus during first 6 months of life
Attainment of independent sitting balance often results in significant reduction of reflux in infants

15
Impact of Cultural Practices on Infant Reflux4,5
“Breast is Best” promoted in developing countries –often changes in US with WIC programs providing formula, concerns with weight gain
Exclusive breast feeding often becomes mixed feeding by 2 months of age
Working mothers versus stay at home mothers – responsiveness to babies needs/schedules for sleep and feeding
Feeding Practices Sleep Management
Sensory Nourishment On Demand vs. Schedule
Infant Reflux Excessive Crying5
Baby holding vs. Baby Seat
Breast feeding on Demand
Co-Sleeping
Formula scheduled feeding
16
Understanding Reflux in Children with Medical Complexities
G-tube
Down Syndrome
Cerebral Palsy
Reflux in Babies with Down Syndrome6
Trisomy 21 77% of all neonates with DS have
GI concerns
19% require hospitalizations related to GI issues
Most common issue is GERD
Related to delayed motility, hypotonia, strictures in GI system
Often under or mis-diagnosed
Results in growth retardation, respiratory complications
17
Reflux in Children with Neurological Impairments7
Cerebral Palsy Unique Challenges
38-57% prevalence in first year of life
Poor postural control of head and trunk, positioning
Decreased oral motor control
Increased or decreased muscle tone
Reflexive movements of head, jaw, tongue
Medications, arousal state, GMFCS Levels
Reflux after Naso-Gastric Tubes
NG tube especially if greater than 4 weeks
• Prevalence of GERD in premature infants with NG tube placement in stomach increased 50%
• Mechanical reason:
• GE sphincter matures around the NG tube when it contracts
• When tube removed GE sphincter contracts the same as when tube was in place –muscle training
• Results in a “hole” in the sphincter from position of NG tube

18
Reflux after NICU
Sensory/motor reasons
• Premature or Immature GI and Respiratory systems
• Neurological concerns
• Surgical, medical interventions (intubation, medications)
• Sensory Overload
Reflux in Infants with Tracheostomy7,8,9
50% Infant cardiac patients have reflux
Premies = 50% of all infant trachs are in premies
• Dysphagia in 80% of Infant/Toddlers with tracheostomies • 75% of all Infants with trachs require nutritional support, via Naso-gastric
or Gastrostomy-tube

19
Reflux in Older Children with Tracheostomy7,8,9
• 20-50% of Infants with Craniofacial anomalies require tracheostomies• Open tracheostomy poor postural control• Use of one way Passy Muir Valve allows ability to close airway to
create internal pressures• Mary Massery relates to the Soda Can• Closed system is strong and can’t be crushed• Open system and it can be crushed with very little force
A Word about Passy Muir Valves – They Are Not Just for Talking!
• Use of Passy Muir Valve improves diaphragmatic control for pressure management and postural control in upright
• Introduce Passy Muir Valve while monitoring O2 and Resp Rate short periods
• Assess behavior – quiet alert vs distressed
• Assess reflux – less frequent, may be generated with more force in cough
• Assess postural control with and without PMV
• Increase ability to reach up with arms above shoulder level
• More consistent sitting balance, more willing to stand up, less anxiety

20
Consequences of Reflux
Feeding refusals, sour breath, infant distress
Inconsistent sitting balance when reflux is active – abdominals ‘shut-off’
Reflux esophagitis, dysphagia, apneic episodes
Recurrent respiratory complications, ‘asthma’, ear infections
Consequences of Reflux
Sensory Defensiveness, Picky Eaters
• Reflux discomfort quickly becomes associated with foods
• Colicky babies, difficult to sooth
• Parental frustration, need for support and advice

21
Sandifer’s Syndrome• Paroxysmal Dystonic Movement
Disorder
• Occurs in association with GER
• Characterized by abnormal posturing of the head and neck (torticollis) and severe arching of the spine
• Episodes can last 1-3 minutes, occur up to 10 times per day
• Usually associated with ingestion of food
• Vomiting, anemia, epigastric discomfort, abnormal eye movements and reflux esophagitis may be present
• Posturing may be attempt to relieve gastric pain
• Often misdiagnosed as seizure activity or paroxysmal dystonia
• Elimination of GER resolves abnormal posturing
Consequences of Reflux
• Avoidance of trunk flexion or reaching against gravity continued abdominal weakness
• Posturing in extension and right cervical rotation to relieve intra-abdominal pressure

22
Reflux and G-tubes with or without Fundoplication
• Placement of gastrostomy feeding tube is required with severe GERD and failure to thrive
• Fundoplication is often done if risk of aspiration• Fundus of the stomach is wrapped around the lower
sphincter of the esophagus to help close
A Word About G-tubes and Reflux Formulas are prescribed based on
calories and nutritional needs
Organic and non-dairy formulas are now available by prescription
Families may make their own g-tube feeding with support of GI and nutritionist
Reflux may continue after G-tube placement
If reflux persists, try giving bolus of water equal to feeding 30 minutes prior to g-tube feeding
Expands stomach
Water is absorbed quickly
Excessive stomach acid reduced by water

23
Tricks and Techniques for the Typical Baby with Reflux10,11
Elimination of Cow’s Milk Protein
Maternal/Infant
Frequent burps
Smaller more frequent feedings
Thickened feeding
No water or thin liquids after
thickened feeds
Give equal amount of water as feeding 30 minutes prior to g-tube or bottle feeds
Positioning:Upright during/after feeding
Prone or left side positioning with supervision after feeding
(caregiver’s lap)
Parental Reassurance and Support
Refer to Pediatrician/GI
If no improvement
Therapy treatment suggestions
Strengthen abdominal muscles on an empty stomach - teach family!
Slow reverse pull to sit with every diaper change but before feedings for consistency and frequency – progress to regular pull to sit
Active reaching, hands to midline, hands to feet play, lifting feet from surface
Straddle sit on parent lap or holding baby with legs around waist, reaching to both sides

24
Therapy treatment suggestions
If baby doesn’t want to activate abdominals, try placing baby on incline at first, then progress lower to more horizontal positions
Look at those Abs!
Don’t do this on a
full tummy!
Work-outs before Feeding!

25
Tummy Time – Start Early, Do Often!
• Activate trunk extensors while lower costal borders are resting on surface • Elongates ribcage, intercostal spacing• Supports diaphragm externally• Prone positioning reduces reflux in infants – note NICU positioning
Tricks to Keep Tummy Time Fun Reduce use of “containers”
(baby seats) - leave the car seat in the car!
Starting at birth, during every diaper change, place baby on tummy for a few minutes
Hold baby prone across your lap, while you watch TV, sit in church, wait in the doctor’s office
Hold baby on your shoulder often and alternate shoulders
Use the football hold
Prop up over the arm of the sofa or stuffed easy chair
Tummy time whenever awake

26
External support to promote abdominals and diaphragm
• Try taping to support obliques and bring lower costal borders down
• Simple elastic abdominal binders extending from lower costal borders to pelvis
• Neoprene vests to provide stronger support and allow cocontraction of core muscles
A Word About Thoraco-Lumbar-Sacral Orthoses
• TLSOs all need abdominal relief to allow normal excursion of diaphragm
• Cutouts should be expanded and/or customized to follow the lower costal borders
• Cutouts need an elastic gusset to provide external support to viscera

27
Ribcage stretching to increase diaphragmatic control
• Place hands gently but firmly around lower costal borders• Direction of stretch is towards pelvis, not squeezing• Allow traction to gently follow breathing• Continue for several minutes if possible• Easy to teach caregivers• Infants and toddlers are often ‘squirmy’ until you start then become
very calm and attentive
Infant with Tracheostomy Ribcage Stretching
Normal breathing
Facilitated diaphragmatic breathing
• Introduce Passy Muir Valve• Monitor O2 and Resp Rate• Assess behavior – quiet alert vs
distressed• Assess postural control with and
without PMV

28
Mary Pengelley, PT, DPT, [email protected]
Q&A
References1. Rosen R, Vandenplas Y, Singendonk M, Cabana M, Di Lorenzo C, Gottrand F, et al. Pediatric Gastroesophageal Reflux Clinical Practice
Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr 2018; 66: 516–54
2. Rybak A, Pesce M, Thapar N, Borrelli O. Gastro-Esophageal Reflux in Children. Int J Mol Sci. 2017;18(8):1671. Published 2017 Aug 1. doi:10.3390/ijms18081671
3. Jenifer R. Lightdale, David A. Gremse. Gastroesophageal Reflux: Management Guidance for the Pediatrician, Pediatrics May 2013, 131 (5) e1684-e1695; DOI: 10.1542/peds.2013-0421
4. Suzinne Pak-Gorstein, Aliya Haq, Elinor A. Graham. Cultural Influences on Infant Feeding Practices. Pediatrics in Review Mar 2009, 30 (3) e11-e21; DOI: 10.1542/pir.30-3-e11
5. Pamela S. Douglas. Excessive crying and gastro-oesophageal reflux disease in infants: misalignment of biology and culture. Medical Hypotheses, Volume 64, Issue 5, 2005, Pages 887-898.
6. Macchini F, Leva E, Torricelli M, Valadè A. Treating acid reflux disease in patients with Down syndrome: pharmacological and physiological approaches. Clin Exp Gastroenterol. 2011;4:19-22.
7. Sullivan PB, Lambert B, Rose M, Ford‐Adams M, Johnson A, Griffiths P. Prevalence and severity of feeding and nutritional problems in children with neurological impairment: Oxford Feeding Study. Dev Med Child Neurol 2000; 42: 674–80.
8. Ibrahim J. et al. Outcome of tracheostomy after pediatric cardiac surgery. Journal of the Saudi Heart Association, Volume 24, Issue 3, 2012, Pages 163-168.
9. Vivienne Norman, Brenda Louw, Alta Kritzinger. Incidence and description of dysphagia in infants and toddlers with tracheostomies: A retrospective review, International Journal of Pediatric Otorhinolaryngology, Volume 71, Issue 7, 2007, Pages 1087-1092.
10. Mahida JB, Asti L, Boss EF, et al. Tracheostomy Placement in Children Younger Than 2 Years: 30-Day Outcomes Using the National Surgical Quality Improvement Program Pediatric. JAMA Otolaryngol Head Neck Surg. 2016;142(3):241–246. doi:10.1001/jamaoto.2015.3302
11. Salvatore S, Abkari A, Cai W, et al. Review shows that parental reassurance and nutritional advice help to optimise the management of functional gastrointestinal disorders in infants[published online ahead of print, 2018 May 25]. Acta Paediatr. 2018;107(9):1512–1520. doi:10.1111/apa.14378







