Dear New Student Employee,
Concord University
New Hire Process
Concord University's Student Payroll Office would like to welcome you as a new Student Employee of the )
University. Student Payroll will make your hiring process as quick and convenient as possible. Attached are the forms that need to be completed and brought with you to finalize your employee processing. In addition, there are a few things you need to remember to bring with you so we may verify your employment eligibility and authorize you to be placed on payroll. Below are explanations for each form and the associated requirements. Please take a few moments to read through the following steps.
International Employees
International employees will need to bring all of their immigration documents (i.e. passport, visa, 1-94 card, 1-20). Also, they will need to have a social security card or a receipt from the Social Security Administration showing that
they have applied for a social security card.
1-9 Employment Eligibility Verification
The US immigration and Naturalization Service (INS) requires that Student Payroll verify your eligibility for
employment. Form 1-9 is used for this purpose and employment cannot begin until this has been completed along
with the hiring information packet from the hiring department.
Please note that we need to see your Driver's License and Social Security card OR Birth Certificate.
ONLY ORIGINAL UNEXPIRED DOCUMENTS WITH MATCHING NAMES WILL BE ACCEPTED, NO COPIESI
This process must be completed with a member of the Student Payroll Office/Payroll Office.
If you have any questions regarding processing procedures, please call 304.384.5277 for assistance.
Payroll Authorization
IRS requires all earnings be reported for an employee annually. A Social Security Number is needed to fulfill that
requirement. Student Payroll will need to see an "official document" that lists your Social Security Number (SSN). A
document that will satisfy this requirement is: Your Social Security Card.
Personal Information and Emergency Contact
The personal information and emergency contact form addresses two requirements:
1. The personal information allows us to input your information into WV Oasis.
2. The Emergency Contact section is used to indicate your primary contact in the event of an emergency.
IRSFormW-4
The IRS requires that you complete Form W-4 so that the correct federal taxes are withheld from your pay.
A worksheet and instructions prepared by the IRS are included with the form.
State Tax Withholding
If you are a resident of the State of West Virginia or any non-bordering state, you need to complete the West
Virginia Employee's Withholding Exemption Certificate.
Residents of PA, MD, VA, KY and OH may complete tax forms from those states, along with a WV Certificate of
Non-Residence.
Direct Deposit Authorization Form
The State of WV requires direct deposit to a checking or savings account, at a banking institution chosen by the
employee. You need to attach a voided check for funds deposited directly into a checking account, or a deposit slip
for funds deposited into a savings account. The deposit slip is used for saving accounts only. If you do not have any
of the above, a memo from your banking institution on their letterhead providing Concord University with the
routing number, account number and signature of the bank representative completing the memo will suffice.
If you decline the Direct Deposit you must sign up for a WV State Pay Card.
Electronic Notice of Deposit (ENOD)
To enroll in ENOD and receive payroll information on-line and not receive a paper statement, the employee should
log onto the State Auditor's Office website: www.wvsao.gov. Instructions are listed within the Student
Employment Packet.
If you have any questions about this process, please call Student Payroll at 304.384.5277 or email us at [email protected].
Student Payroll welcomes you to Concord University and looks forward to hearing from you.
Erin M Clark
Student Payroll
Admin Building, Room A223
~ • - , ...
1~1 .~. •• • •• II I~ Ii! ~ -----CONCORD
UNIVERSITY STUDENT PAYROLL OFFICE
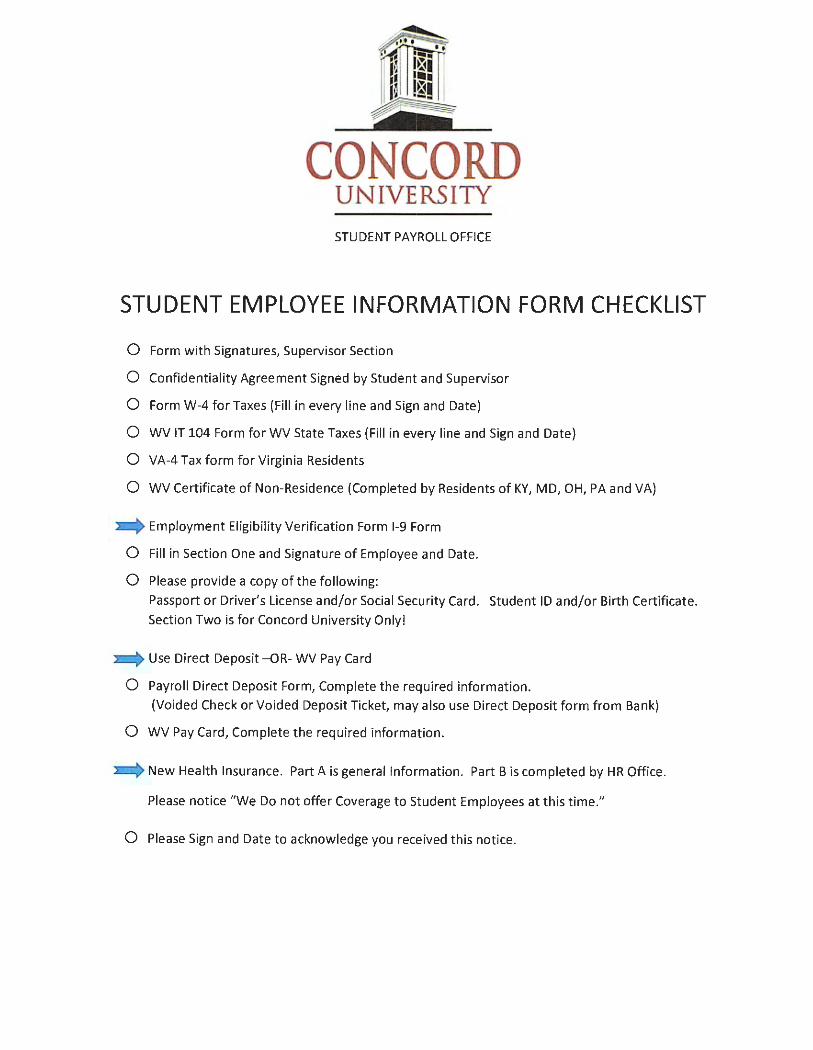
STUDENT EMPLOYEE INFORMATION FORM CHECKLIST
0 Form with Signatures, Supervisor Section
0 Confidentiality Agreement Signed by Student and Supervisor
0 Form W-4 for Taxes (Fill in every line and Sign and Date)
0 WV IT 104 Form for WV State Taxes (Fill in every line and Sign and Date)
0 VA-4 Tax form for Virginia Residents
0 WV Certificate of Non-Residence (Completed by Residents of KY, MD, OH, PA and VA)
- Employment Eligibility Verification Form 1-9 Form
0 Fill in Section One and Signature of Employee and Date.
0 Please provide a copy of the following:
Passport or Driver's License and/or Social Security Card. Student ID and/or Birth Certificate.
Section Two is for Concord University Only!
Use Direct Deposit -OR- WV Pay Card
0 Payroll Direct Deposit Form, Complete the required information.
(Voided Check or Voided Deposit Ticket, may also use Direct Deposit form from Bank)
0 WV Pay Card, Complete the required information.
New Health Insurance. Part A is general Information. Part Bis completed by HR Office.
Please notice "We Do not offer Coverage to Student Employees at this time."
0 Please Sign and Date to acknowledge you received this notice.
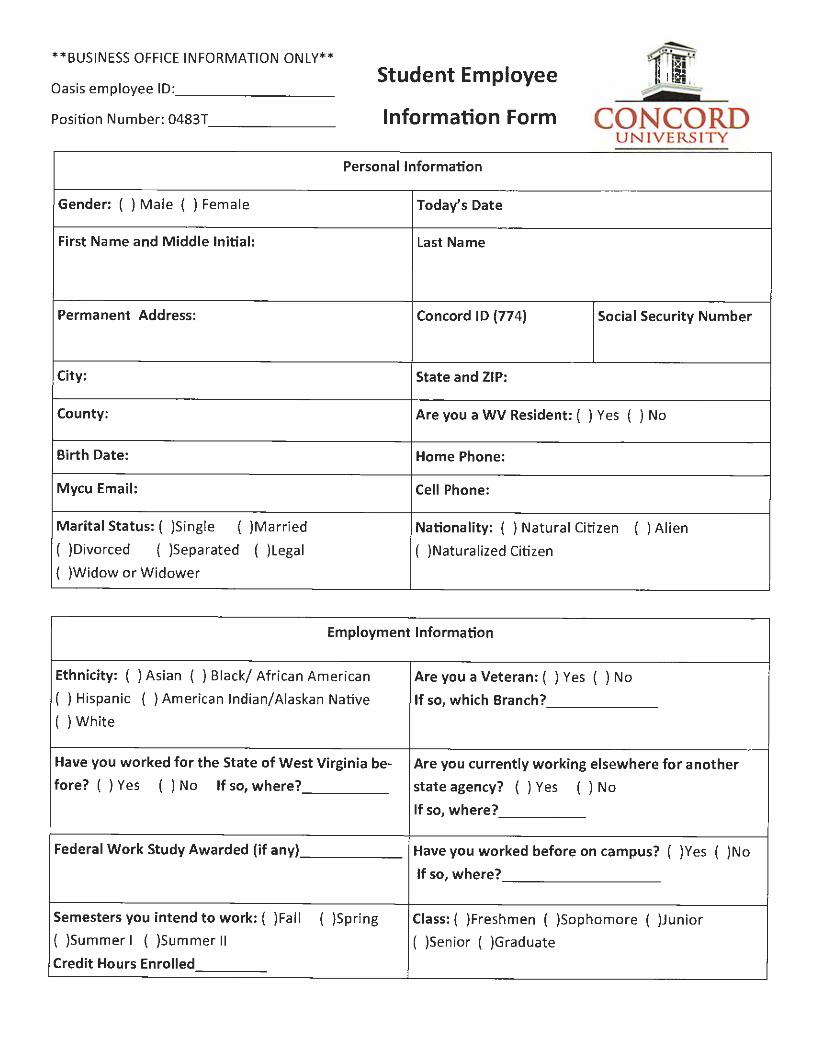
** BUSINESS OFFICE INFORMATION ONLY**
Oasis em ployee ID : ________ _
Position Number: 0483T -------
Student Employee
Information Form CONCORD UNIVERSITY
Personal Information
Gender: ( ) M ale ( ) Female Today's Date
First Name and M iddle Initial : Last Name
Permanent Address: Concord ID (774) Social Security Number
City: State and ZIP:
County: Are you a WV Resident : ( ) Yes ( ) No
Birth Date: Home Phone:
Mycu Email: Cell Phone:
Marital Status: ( )Single ( )Married Nationality: ( ) Natura l Citi zen ( ) Alien
( )Divorced ( )Separated ( )Lega l ( )Nat uralized Citizen
( )Widow or W idower
Employment Information
Et hnicity: ( ) Asian ( ) Black/ Africa n American Are you a Veteran: ( ) Yes ( ) No
( ) Hispanic ( ) American Indian/ Alaskan Native If so, which Branch?
( ) White
Have you worked fo r the State of West Virginia be- Are you currently working elsewhere for another
fore? ( ) Yes ( ) No If so, where? state agency? ( ) Yes ( ) No
If so, where?
~ederal Work Study Awarded (if any) Have you worked before on campus? ( )Yes ( )No
If so, where?
Semesters you intend to work: ( )Fall ( )Spring Class: ( )Freshmen ( )Sophomore ( )Junior
( )Summer I ( )Summer II ( )Senior ( )Graduate
Credit Hours Enrolled
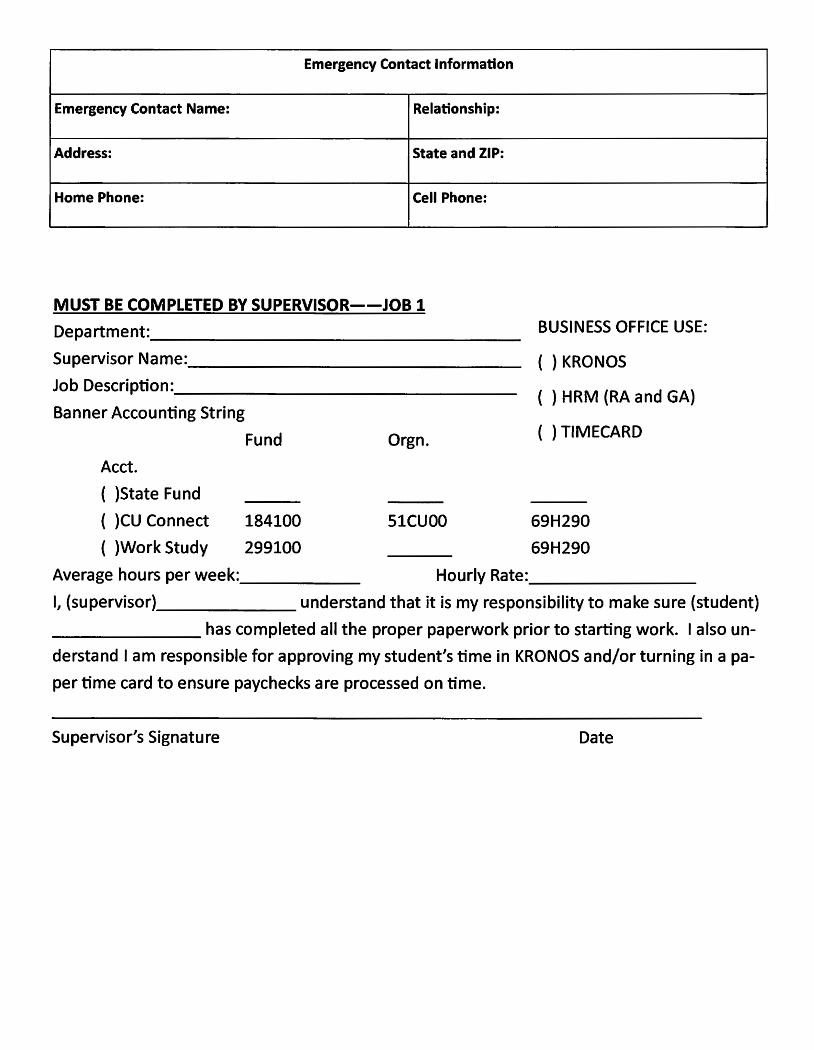
Emergency Contact Information
Emergency Contact Name: Relationship:
Address: State and ZIP:
Home Phone: Cell Phone:
MUST BE COMPLETED BY SUPERVISOR--JOB 1 Department: _________________ _
Supervisor Name: _______________ _
Job Description: _______________ _
Banner Accounting String
Acct.
( )State Fund
( )CU Connect
( )Work Study
Fund
184100
299100
Orgn.
SlCUOO
BUSINESS OFFICE USE:
( ) KRONOS
( ) HRM (RA and GA)
( ) TIMECARD
69H290
69H290
Average hours per week:______ Hourly Rate: _______ _
I, (supervisor) _______ understand that it is my responsibility to make sure (student)
_______ has completed all the proper paperwork prior to starting work. I also un
derstand I am responsible for approving my student's time in KRONOS and/or turning in a pa
per time card to ensure paychecks are processed on time.
Supervisor's Signature Date
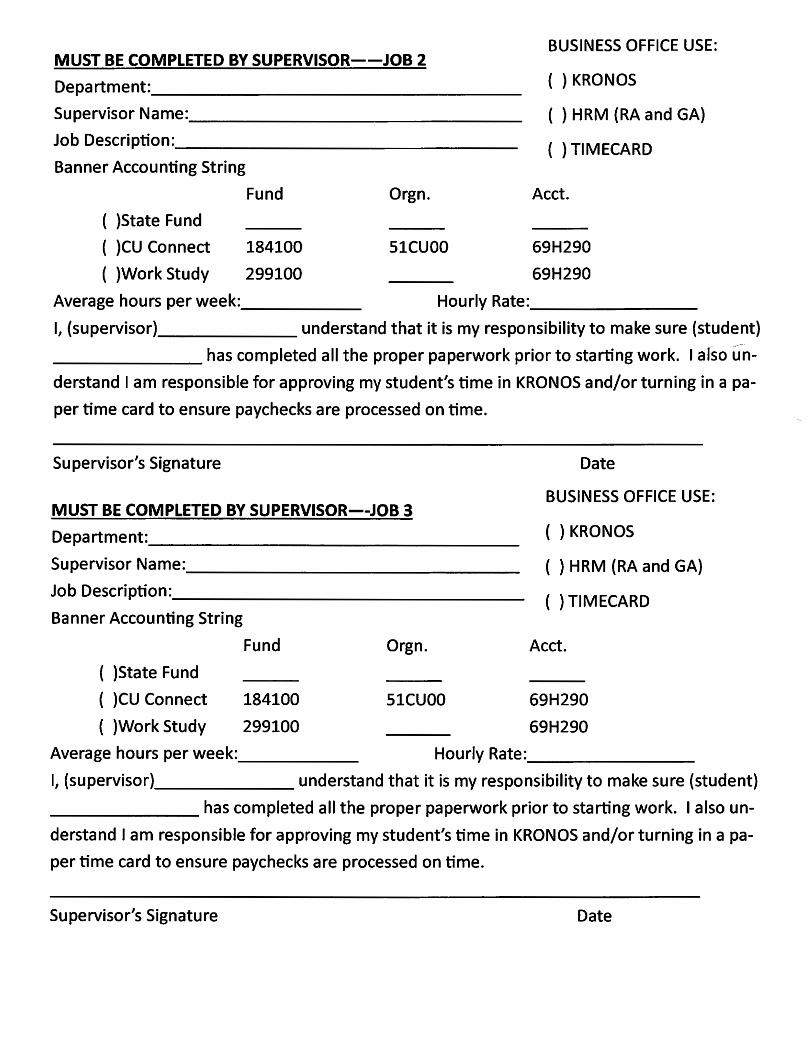
MUST BE COMPLETED BY SUPERVISOR--JOB 2
Department: ________________ _
Supervisor Name: ______________ _
Job Description: _______________ _
Banner Accounting String
( )State Fund
( )CU Connect
( )Work Study
Fund
184100
299100
Orgn.
SlCUOO
BUSINESS OFFICE USE:
( ) KRONOS
( ) HRM (RA and GA)
( ) TIMECARD
Acct.
69H290
69H290
Average hours per week:______ Hourly Rate: _______ _
I, (supervisor) ______ understand that it is my responsibility to make sure (student)
_______ has completed all the proper paperwork prior to starting work. I also un~
derstand I am responsible for approving my student's time in KRONOS and/or turning in a pa
per time card to ensure paychecks are processed on time.
Supervisor's Signature
MUST BE COMPLETED BY SUPERVISOR--JOB 3 Department: ________________ _
Supervisor Name: ______________ _
Job Description: _______________ _
Banner Accounting String
( )State Fund
( )CU Connect
( )Work Study
Fund
184100
299100
Orgn.
SlCUOO
Date
BUSINESS OFFICE USE:
( ) KRONOS
( ) HRM (RA and GA)
( ) TIMECARD
Acct.
69H290
69H290 Average hours per week:______ Hourly Rate: _______ _
I, (supervisor) ______ understand that it is my responsibility to make sure (student)
_______ has completed all the proper paperwork prior to starting work. I also un
derstand I am responsible for approving my student's time in KRONOS and/or turning in a pa
per time card to ensure paychecks are processed on time.
Supervisor's Signature Date
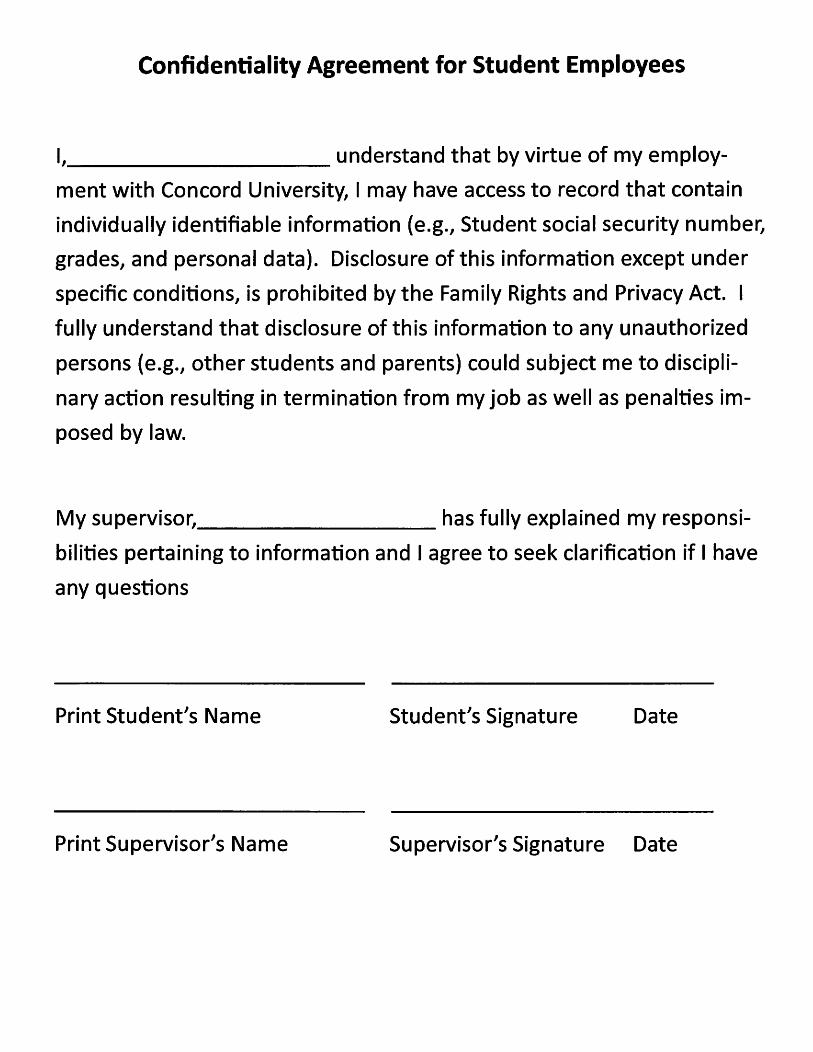
Confidentiality Agreement for Student Employees
I, __________ understand that by virtue of my employ-
ment with Concord University, I may have access to record that contain
individually identifiable information (e.g., Student social security number,
grades, and personal data). Disclosure of this information except under
specific conditions, is prohibited by the Family Rights and Privacy Act. I
fully understand that disclosure of this information to any unauthorized
persons {e.g., other students and parents) could subject me to discipli
nary action resulting in termination from my job as well as penalties im
posed by law.
My supervisor, has fully explained my responsi-
bilities pertaining to information and I agree to seek clarification if I have
any questions
Print Student's Name Student's Signature Date
Print Supervisor's Name Supervisor's Signature Date
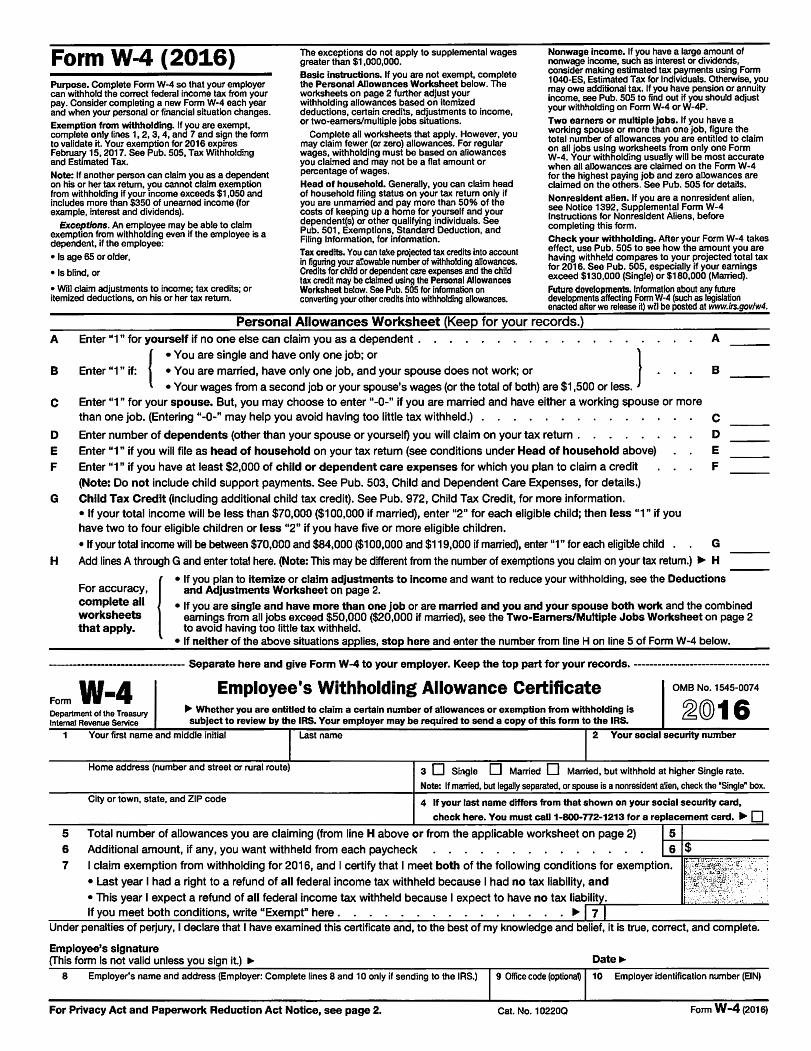
Form W-4 (2016) The exceptions do not apply to supplemental wages greater than $1,000,000.
Nonwage income. If you have a large amount of nonwage income, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you may owe additional tax. If you have pension or annuity income, see Pub. 505 to find out if you should adjust your withholding on Form W-4 or W-4P.
Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes.
Basic instructions. If you are not exempt, complete the Personal Allowances Worksheet below. The worksheets on page 2 further adjust your withholding allowances based on itemized deductions, certain credits, adjustments to income, or two-earners/multiple jobs situations. Two earners or multiple jobs. If you have a
working spouse or more than one job, figure the total number of allowances you are entitled to claim on all jobs using worksheets from only one Form W-4. Your withholding usually will be most accurate when all allowances are claimed on the Form W-4 for the highest paying job and zero allowances are claimed on the others. See Pub. 505 for details.
Exemption from withholding. If you are exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2016 expires February 15, 2017. See Pub. 505, Tax Withholding and Estimated Tax.
Complete all worksheets that apply. However, you may claim fewer (or zero) allowances. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages. Note: If another person can claim you as a dependent
on his or her tax return, you cannot claim exemption from withholding if your income exceeds $1,050 and includes more than $350 of unearned income (for example, interest and dividends).
Head of household. Generally, you can claim head of household filing status on your tax return only if you are unmarried and pay more than 50% of the costs of keeping up a home for yourself and your dependent(s) or other qualifying individuals. See Pub. 501, Exemptions, Standard Deduction, and Filing Information, for information.
Nonresident alien. If you are a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form. Exceptions. An employee may be able to claim
exemption from withholding even if the employee is a dependent, if the employee:
Tax credits. You can take projected tax credits into account in figuring your allowable number of withholding allowances. Credits for child or dependent care expenses and the child tax credit may be claimed using the Personal Allowances Worksheet below. See Pub. 505 for information on converting your other credits into withholding allowances.
Check your withholding. After your Form W-4 takes effect, use Pub. 505 to see how the amount you are having withheld compares to your projected total tax for 2016. See Pub. 505, especially if your earnings exceed $130,000 (Single) or $180,000 (Married).
• Is age 65 or older,
• Is blind, or
• Will claim adjustments to income; tax credits; or itemized deductions, on his or her tax return.
Future developments. Information about any future developments affecting Fonn W-4 (such as legislation enacted after we release it) will be posted at www.irs.gov/w4.
A
B
C
D E F
G
Personal Allowances Worksheet {Keep for your records.) Enter "1" for yourself if no one else can claim you as a dependent .
{
• You are single and have only one job; or } Enter "1" if: • You are married, have only one job, and your spouse does not work; or
• Your wages from a second job or your spouse's wages (or the total of both} are $1,500 or less. Enter 111" for your spouse. But, you may choose to enter 11-0-" if you are married and have either a working spouse or more than one job. (Entering 11-0-11 may help you avoid having too little tax withheld.} .
Enter number of dependents (other than your spouse or yourself} you will claim on your tax return .
Enter "1" if you will file as head of household on your tax return (see conditions under Head of household above}
Enter "1" if you have at least $2,000 of child or dependent care expenses for which you plan to claim a credit
(Note: Do not include child support payments. See Pub. 503, Child and Dependent Care Expenses, for details.}
Child Tax Credit (including additional child tax credit}. See Pub. 972, Child Tax Credit, for more information. • If your total income will be less than $70,000 ($100,000 if married}, enter "2" for each eligible child; then less "1" if you have two to four eligible children or less 11211 if you have five or more eligible children.
• If your total income will be between $70,000 and $84,000 ($100,000 and $119,000 if married}, enter "1" for each eligible child .
A
B
C D E F
G
H Add lines A through G and enter total here. (Note: This may be different from the number of exemptions you claim on your tax return.) ... H
! • If you plan to itemize or claim adjustments to Income and want to reduce your withholding, see the Deductions
For accuracy, and Adjustments Worksheet on page 2.
complete all • If you are single and have more than one job or are married and you and your spouse both work and the combined worksheets earnings from all jobs exceed $50,000 ($20,000 if married), see the Two-Earners/Multiple Jobs Worksheet on page 2 that apply. to avoid having too little tax withheld.
• If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 below.
---------------------------------- Separate here and give Form W-4 to your employer. Keep the top part for your records. ---------------------------------
Form W•4 Employee's Withholding Allowance Certificate
~@16 0MB No. 1545-0074
Department of the Treasury IJI,, Whether you are entitled to claim a certain number of allowances or exemption from withholding is Internal Revenue Service subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
1 Your first name and middle initial Last name 2 Your social security number
Home address (number and street or rural route) 3 D Single D Married D Married, but withhold at higher Single rate.
Note: If married, but legally separated, or spouse is a nonresident alien, check the "Single" box.
City or town, state, and ZIP code 4 If your last name differs from that shown on your social security card,
check here. You must call 1-800-772-1213 for a replacement card . ... D 5 Total number of allowances you are claiming (from line H above or from the applicable worksheet on page 2)
6 Additional amount, if any, you want withheld from each paycheck
7 I claim exemption from withholding for 2016, and I certify that I meet both of the following conditions for exemption.
• Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and
• This year I expect a refund of all federal income tax withheld because I expect to have no tax liab-;..:.:il:.:.:.ity~.:..._ ____ .11;:.;.;.~~..:.:.:.;;;;.!.;.;._~
If you meet both conditions, write "Exempt" here . • ..,. 7 Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete.
Employee's signature (This form is not valid unless you sign it.) ..,. Date..,.
8 Employer's name and address (Employer: Complete lines 8 and 10 only if sending to the IRS.) 9 Office code (optional) 10 Employer identification number (EIN)
For Privacy Act and Paperwork Reduction Act Notice, see page 2. Cat. No. 102200 Form W-4 (2016)
Form W-4 (2016)
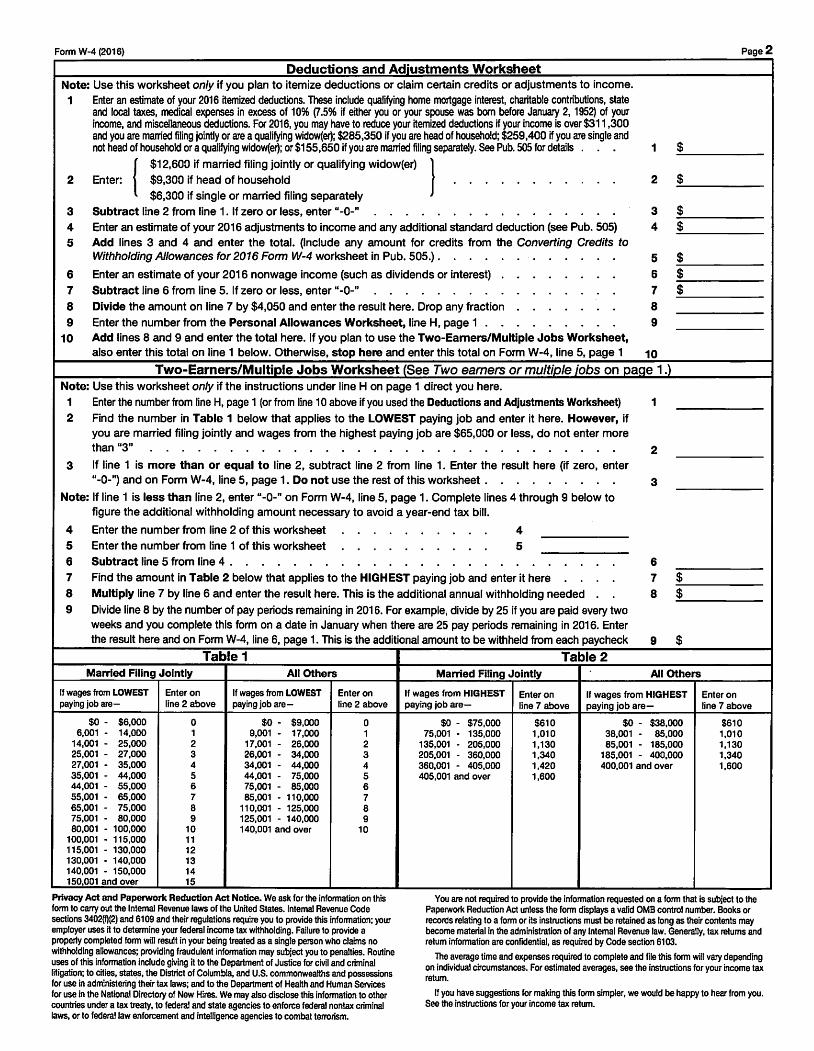
Deductions and Adjustments Worksheet Note: Use this worksheet only if you plan to itemize deductions or claim certain credits or adjustments to income.
1 Enter an estimate of your 2016 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes, medical expenses in excess of 10% (7 .5% if either you or your spouse was born before January 2, 1952) of your income, and miscellaneous deductions. For 2016, you may have to reduce your itemized deductions if your income is over $311,300 and you are married filing jointly or are a qualifying widow(er); $285,350 if you are head of household; $259,400 if you are single and not head of household or a qualifying widow(er}; or $155,650 if you are married filing separately. See Pub. 505 for details
{
$12,600 if married filing jointly or qualifying widow(er) } 2 Enter: $9,300 if head of household
$6,300 if single or married filing separately
Page2
1 $
2 $
3 Subtract line 2 from line 1. If zero or less, enter "-0-" 3 _;._$ ___ _
4 $ 4 Enter an estimate of your 2016 adjustments to income and any additional standard deduction (see Pub. 505) ------5 Add lines 3 and 4 and enter the total. (Include any amount for credits from the Converting Credits to
Withholding Allowances for 2016 Form W-4 worksheet in Pub. 505.) . 5 ....:....$ ___ _
6 Enter an estimate of your 2016 nonwage income (such as dividends or interest) 6 $ ..;..... ____ _ 7 Subtract line 6 from line 5. If zero or less, enter "-0-" 7 _;._$ ___ _
8 Divide the amount on line 7 by $4,050 and enter the result here. Drop any fraction 8 9 Enter the number from the Personal Allowances Worksheet, line H, page 1 . 9
1 O Add lines 8 and 9 and enter the total here. If you plan to use the Two-Earners/Multiple Jobs Worksheet, also enter this total on line 1 below. Otherwise, stop here and enter this total on Form W-4, line 5, page 1 10
Two-Earners/Multiole Jobs Worksheet (See Two earners or multiole iobs on oaae 1 .) Note: Use this worksheet only if the instructions under line H on page 1 direct you here.
1 Enter the number from line H, page 1 (or from line 10 above if you used the Deductions and Adjustments Worksheet) 1
2 Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you are married filing jointly and wages from the highest paying job are $65,000 or less, do not enter more than "3" 2
3 If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter "-0-"} and on Form W-4, line 5, page 1. Do not use the rest of this worksheet .
Note: If line 1 is less than line 2, enter "-0-" on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill.
4 Enter the number from line 2 of this worksheet 4 5 Enter the number from line 1 of this worksheet 5
6 Subtract line 5 from line 4 .
7 Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here
3
6 7 $ ------
8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed 8 _;._$ ___ _
9 Divide line 8 by the number of pay periods remaining in 2016. For example, divide by 25 if you are paid every two weeks and you complete this form on a date in January when there are 25 pay periods remaining in 2016. Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck 9 $
Table 1 Table 2 Married Filing Jointly
If wages from LOWEST paying job are-
$0 - $6,000 6,001 - 14,000
14,001 - 25,000 25,001 - 27,000 27,001 - 35,000 35,001 - 44,000 44,001 - 55,000 55,001 - 65,000 65,001 - 75,000 75,001 - 80,000 80,001 - 100,000
100,001 - 115,000 115.001 - 130,000 130,001 - 140,000 140,001 - 150,000 150,001 and over
Enter on line2 above
0 1 2 3 4 5 6 7 8 9
10 11 12 13 14 15
All Others
If wages from LOWEST paying job are-
$0 - $9,000 9,001 - 17,000
17,001 - 26,000 26,001 - 34,000 34,001 - 44,000 44,001 - 75,000 75,001 - 85,000 85,001 - 110,000
110.001 - 125,000 125,001 - 140,000 140,001 and over
Enter on line2 above
0 1 2 3 4 5 6 7 8 9
10
Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(ij(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism.
Married Filing Jointly
If wages from HIGHEST paying job are-
$0 - $75,000 75,001 - 135,000
135,001 - 205,000 205,001 - 360,000 360,001 - 405,000 405,001 and over
Enter on line 7 above
$610 1,010 1,130 1,340 1.420 1,600
All Others
If wages from HIGHEST paying job are-
$0 - $38,000 38,001 - 85,000 85,001 - 185,000
185,001 - 400,000 400,001 and over
Enter on line 7 above
$610 1,010 1,130 1,340 1,600
You are not required to provide the information requested on a form that is subject to the Paperwork Reduction Act unless the form displays a valid 0MB control number. Books or records relating to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential. as required by Code section 6103.
The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return.
If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.
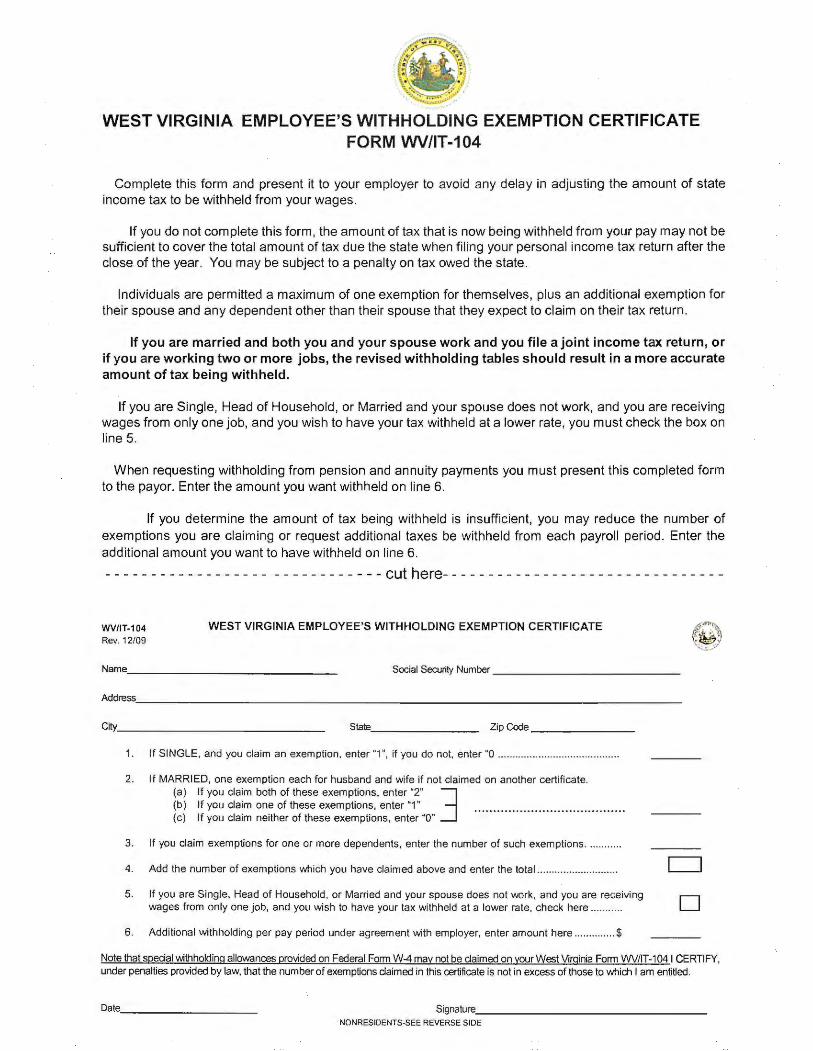
WEST VIRGINIA EMPLOYEE'S WITHHOLDING EXEMPTION CERTIFICATE FORM WV/IT-104
Complete this form and present it to your employer to avoid any delay in adjusting the amount of state income tax to be withheld from your wages.
If you do not complete this form, the amount of tax that is now being withheld from your pay may not be sufficient to cover the total amount of tax due the state when filing your personal income tax return after the close of the year. You may be subject to a penalty on tax owed the state.
Individuals are permitted a maximum of one exemption for themselves, plus an additional exemption for their spouse and any dependent other than their spouse that they expect to claim on their tax return.
If you are married and both you and your spouse work and you file a joint income tax return, or if you are working two or more jobs, the revised withholding tables should result in a more accurate amount of tax being withheld .
If you are Single, Head of Household, or Married and your spouse does not work, and you are receiving wages from only one job, and you wish to have your tax withheld at a lower rate, you must check the box on line 5.
When requesting withholding from pension and annuity payments you must present this completed form to the payor. Enter the amount you want wi thheld on line 6.
If you determine the amount of tax being withheld is insufficient, you may reduce the number of exemptions you are claim ing or request add itional taxes be withheld from each payroll period. Enter the add itional amount you want to have withheld on line 6.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - cut here- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
WV/IT-104 Rev. 12/09
WEST VIRGINIA EM PLOYEE'S WITHHOLDING EXEMPTION CERTIFICATE
Social Securily Number ___________ _
Address. ______________________ _____________ _
City ___________ __ _ State ______ _ Zip Code ______ _
1. If SINGLE, and you claim an exemption, enter "1 ", if you do not, enter "O .................................. ..... .. .
2. If MARRIED, one exemption each for husband and wife if not claimed on another certificate. (a) If you claim both of these exemptions, enter "2" j (b) If you claim one of these exemptions, enter "1" ..................... .................. . (c) If you claim neither of these exemptions, enter "O"
3. If you claim exemptions for one or more dependents, enter the number of such exemptions ........... .
4. Add the number of exemptions which you have claimed above and enter the total ........................... .
5. If you are Single, Head of Household, or Married and your spouse does not work, and you are receiving wages from only one job, and you wish to have your tax withheld at a lower rate, check here ....... .. . .
6. Additional withholding per pay period under agreement with employer, enter amount here .............. $
(~) ,,':, ... '
Note that special withholding allowances provided on Federal Form W.4 may not be claimed on your West Virginia Form I/N/IT-104 I CERTIFY, under penalties provided by law, that the number of exemptions claimed in this certificate is not in excess of those to which I am entitled.
Date ________ _ Signature ______________ _
NONRESIDENTS-SEE REVERSE SIDE
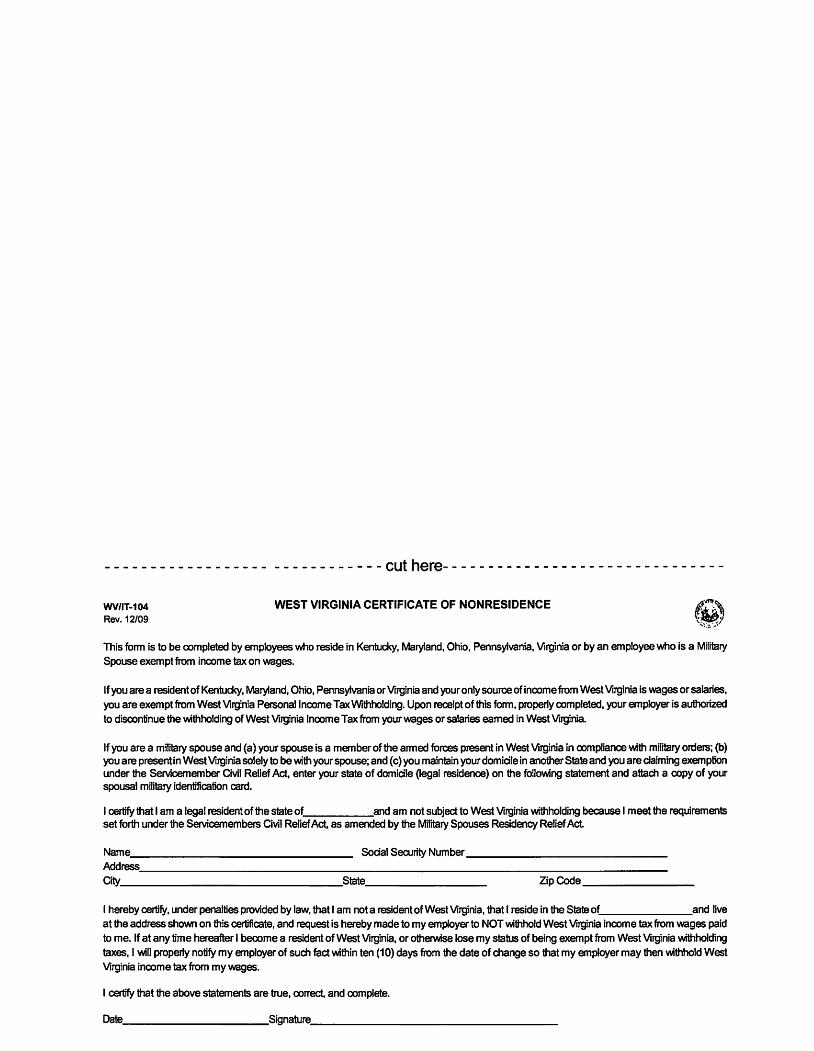
WV/IT-104 Rev. 12/09
------------cuthere-------------------------------
WEST VIRGINIA CERTIFICATE OF NONRESIDENCE
This fonn is to be completed by employees who reside in Kentucky, Maryland, Ohio, Pennsylvania, Virginia or by an employee who is a Military Spouse exempt from income tax on wages.
If you are a resident of Kentucky, Maryland, Ohio, Pennsylvania or Virginia and your only source of income from West Virginia is wages or salaries, you are exempt from West Virginia Personal Income Tax Wrthholding. Upon receipt of this fonn, property completed, your employer is authorized to discontinue the wthholding of West Virginia Income Tax from your wages or salaries earned in West Virginia.
If you are a military spouse and (a) your spouse is a member of the anned forces present in West Virginia in compliance with military orders; (b) you are present in West Virginia solely to be with your spouse; and (c) you maintain your domicile in another State and you are daiming exemption under the Servicemember Civil Relief Act, enter your state of domicile (legal residence) on the following statement and attach a copy of your spousal military identification card.
I certify that I am a legal resident of the state of and am not subject to West Virginia withholding because I meet the requirements set forth under the Servicemembers Civil Relief Act, as amended by the Military Spouses Residency Relief Act
Social Security Number--------------------------Name------------------------------Address'---------------------------------------------------------------------------Oty-------------------------------State_--------------- Zip Code---------
I hereby certify, under penalties provided by law, that I am not a resident of West Virginia, that I reside in the State of and live at the address shown on this certificate, and request is hereby made to my employer to NOT wthhold West Virginia income tax from wages paid to me. If at any time hereafter I become a resident of West Virginia, or otherwise lose my status of being exempt from West Virginia withholding taxes, I will properly notify my employer of such fact within ten (10) days from the date of change so that my employer may then withhold West Virginia income tax from my wages.
I certify that the above statements are true, correct, and complete.
Date_------------------S~nature._--------------------------------
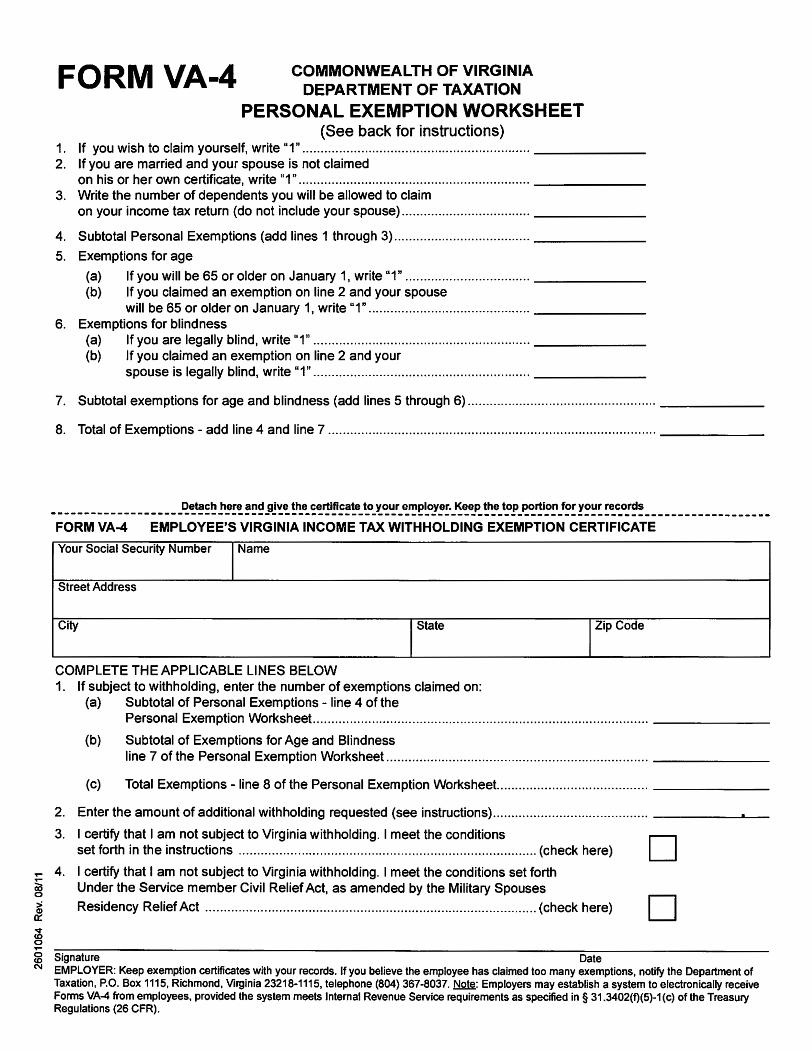
FORM VA-4 COMMONWEALTH OF VIRGINIA DEPARTMENT OF TAXATION
PERSONAL EXEMPTION WORKSHEET (See back for instructions)
1. If you wish to claim yourself, write "1" .............................................................. -------2. If you are married and your spouse is not claimed
on his or her own certificate, write "1" ............................................................... -------3. Write the number of dependents you will be allowed to claim
on your income tax return (do not include your spouse) ................................... -------
4. Subtotal Personal Exemptions (add lines 1 through 3) ..................................... -------
5. Exemptions for age
(a) If you will be 65 or older on January 1, write "1" .................................. -------(b) If you claimed an exemption on line 2 and your spouse
will be 65 or older on January 1, write "1" ............................................ -------6. Exemptions for blindness
(a) If you are legally blind, write "1" ........................................................... -------(b) If you claimed an exemption on line 2 and your
spouse is legally blind, write "1" ........................................................... -------
7. Subtotal exemptions for age and blindness (add lines 5 through 6) ................................................... _____ _
8. Total of Exemptions - add line 4 and line 7 ......................................................................................... ------
___________________ Detach here and give the certificate to your employer. Keep the top portion for your records __________________ _
FORM VA-4 EMPLOYEE'S VIRGINIA INCOME TAX WITHHOLDING EXEMPTION CERTIFICATE
Your Social Security Number Name
Street Address
City State Zip Code
COMPLETE THE APPLICABLE LINES BELOW 1. If subject to withholding, enter the number of exemptions claimed on:
(a) Subtotal of Personal Exemptions - line 4 of the Personal Exemption Worksheet ........................................................................................... ______ _
(b) Subtotal of Exemptions for Age and Blindness line 7 of the Personal Exemption Worksheet ....................................................................... ______ _
(c) Total Exemptions -line 8 of the Personal Exemption Worksheet... ...................................... ______ _
2. Enter the amount of additional withholding requested (see instructions) .......................................... -------
J_ ~::~ht~:~~:~s~~c~~~=~-t-~--~'.'.~'.".i_a_~'.'.~~~'.~i-~-~----'-:~~'._'.~~-~~~'.'.'.~~-~--------- (check here) D ~ 4. I certify that I am not subject to Virginia withholding. I meet the conditions set forth ~ Under the Service member Civil Relief Act, as amended by the Military Spouses
l Residency Relief Act .......................................................................................... (check here) D ~ 0
"'"" g Signature Date N EMPLOYER: Keep exemption certificates with your records. If you believe the employee has claimed too many exemptions, notify the Department of
Taxation, P.O. Box 1115, Richmond, Virginia 23218-1115, telephone (804) 367-8037. Note: Employers may establish a system to electronically receive Forms VA-4 from employees, provided the system meets Internal Revenue Service requirements as specified in§ 31.3402(f)(5)-1(c) of the Treasury Regulations (26 CFR).
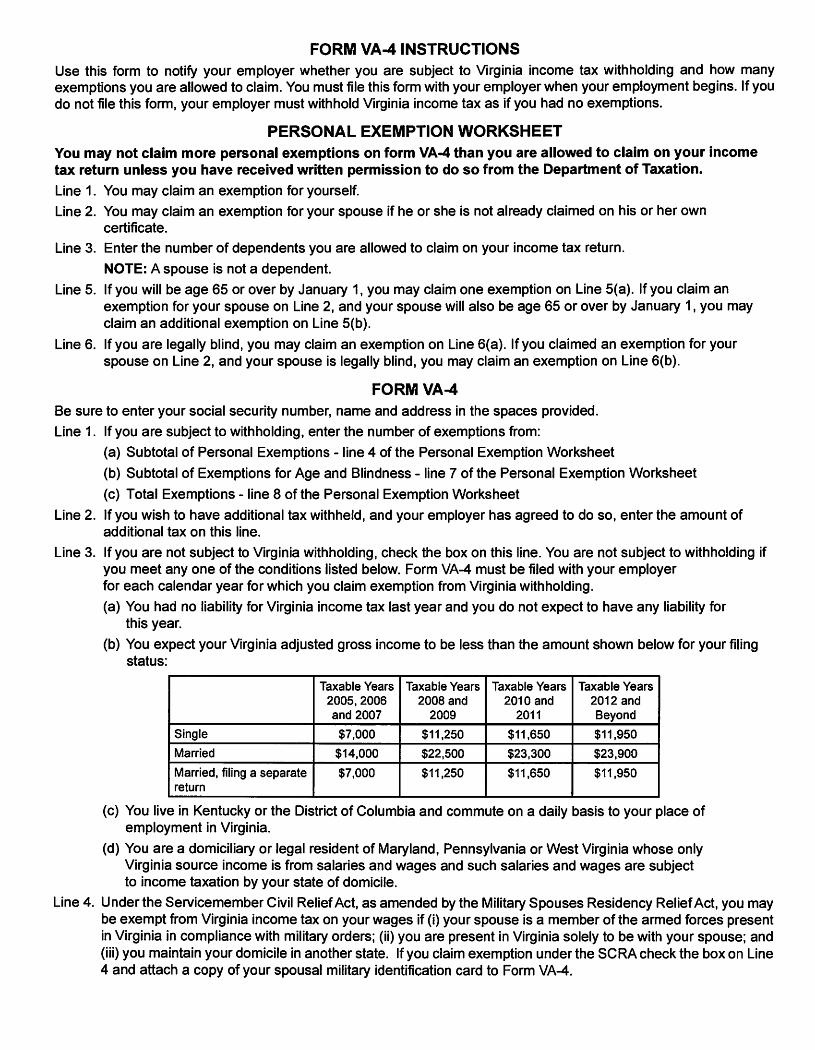
FORM VA-4 INSTRUCTIONS Use this form to notify your employer whether you are subject to Virginia income tax withholding and how many exemptions you are allowed to claim. You must file this form with your employer when your employment begins. If you do not file this form, your employer must withhold Virginia income tax as if you had no exemptions.
PERSONAL EXEMPTION WORKSHEET You may not claim more personal exemptions on form VA-4 than you are allowed to claim on your income tax return unless you have received written permission to do so from the Department of Taxation.
Line 1. You may claim an exemption for yourself.
Line 2. You may claim an exemption for your spouse if he or she is not already claimed on his or her own certificate.
Line 3. Enter the number of dependents you are allowed to claim on your income tax return.
NOTE: A spouse is not a dependent.
Line 5. If you will be age 65 or over by January 1, you may claim one exemption on Line 5(a). If you claim an exemption for your spouse on Line 2, and your spouse will also be age 65 or over by January 1, you may claim an additional exemption on Line 5(b).
Line 6. If you are legally blind, you may claim an exemption on Line 6(a). If you claimed an exemption for your spouse on Line 2, and your spouse is legally blind, you may claim an exemption on Line 6(b).
FORM VA-4 Be sure to enter your social security number, name and address in the spaces provided.
Line 1. If you are subject to withholding, enter the number of exemptions from:
(a) Subtotal of Personal Exemptions - line 4 of the Personal Exemption Worksheet
(b) Subtotal of Exemptions for Age and Blindness - line 7 of the Personal Exemption Worksheet
(c) Total Exemptions - line 8 of the Personal Exemption Worksheet
Line 2. If you wish to have additional tax withheld, and your employer has agreed to do so, enter the amount of additional tax on this line.
Line 3. If you are not subject to Virginia withholding, check the box on this line. You are not subject to withholding if you meet any one of the conditions listed below. Form VA-4 must be filed with your employer for each calendar year for which you claim exemption from Virginia withholding.
(a) You had no liability for Virginia income tax last year and you do not expect to have any liability for this year.
(b) You expect your Virginia adjusted gross income to be less than the amount shown below for your filing status:
Taxable Years Taxable Years Taxable Years Taxable Years 2005,2006 2008 and 2010 and 2012 and and 2007 2009 2011 Beyond
Single $7,000 $11,250 $11,650 $11,950
Married $14,000 $22,500 $23,300 $23,900
Married, filing a separate $7,000 $11,250 $11,650 $11,950 return
(c) You live in Kentucky or the District of Columbia and commute on a daily basis to your place of employment in Virginia.
(d) You are a domiciliary or legal resident of Maryland, Pennsylvania or West Virginia whose only Virginia source income is from salaries and wages and such salaries and wages are subject to income taxation by your state of domicile.
Line 4. Under the Servicemember Civil Relief Act, as amended by the Military Spouses Residency Relief Act, you may be exempt from Virginia income tax on your wages if (i) your spouse is a member of the armed forces present in Virginia in compliance with military orders; (ii) you are present in Virginia solely to be with your spouse; and (iii) you maintain your domicile in another state. If you claim exemption under the SCRA check the box on Line 4 and attach a copy of your spousal military identification card to Form VA-4.
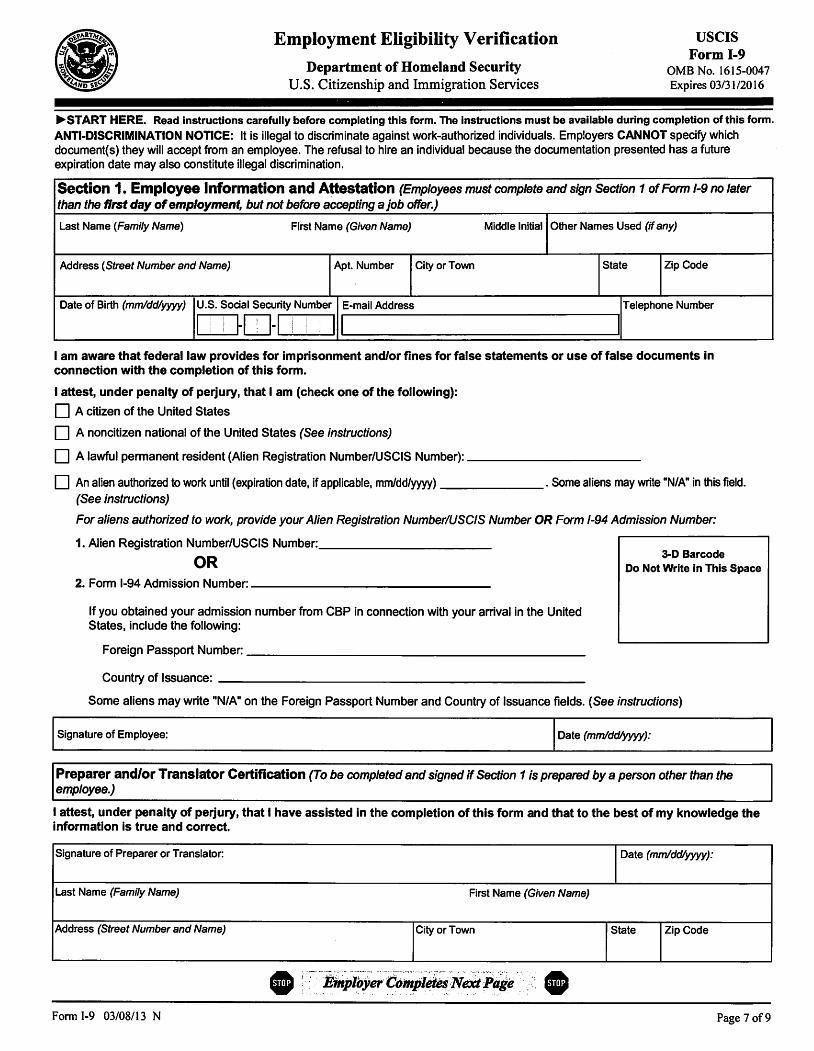
Employment Eligibility Verification
Department of Homeland Security U.S. Citizenship and Immigration Services
USCIS Form 1-9
0MB No. 1615-0047 Expires 03/31/2016
.... START HERE. Read instructions carefully before completing this form. The instructions must be available during completion of this form.
ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document{s) they will accept from an employee. The refusal to hire an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form 1-9 no later than the first day of employment, but not before accepting a job offer.)
Last Name (Family Name) First Name (Given Name) Middle Initial Other Names Used (if any)
Address (Street Number and Name) Apt. Number City or Town State Zip Code
Date of Birth (mmlddlyyyy) U.S. Social Security Number E-mail Address Telephone Number
I I
I ~ITJ-1 ! I ! 11 I I
i I
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.
I attest, under penalty of perjury, that I am (check one of the following):
DA citizen of the United States
D A noncitizen national of the United States (See instructions)
D A lawful permanent resident {Alien Registration Number/USCIS Number):-----------
D An alien authorized to work until (expiration date, if applicable, mm/dd/yyyy) -------. Some aliens may write "N/A" in this field. (See instructions)
For aliens authorized to work, provide your Alien Registration Number/USCIS Number OR Form 1-94 Admission Number:
1. Alien Registration Number/USCIS Number: __________ _
OR 3-D Barcode
Do Not Write in This Space 2. Form 1-94 Admission Number: _______________ _
If you obtained your admission number from CBP in connection with your arrival in the United States, include the following:
Foreign Passport Number:---------------------
Country of Issuance: ------------------------
Some aliens may write "N/A" on the Foreign Passport Number and Country of Issuance fields. { See instructions)
I Signature of Employee: I Date (mmlddlyyyy):
Preparer and/or Translator Certification (To be completed and signed if Section 1 is prepared by a person other than the employee.)
I attest, under penalty of perjury, that I have assisted in the completion of this form and that to the best of my knowledge the information is true and correct.
Signature of Preparer or Translator: Date (mmldd/ym):
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State Zip Code
Fonn 1-9 03/08/13 N Page 7 of9
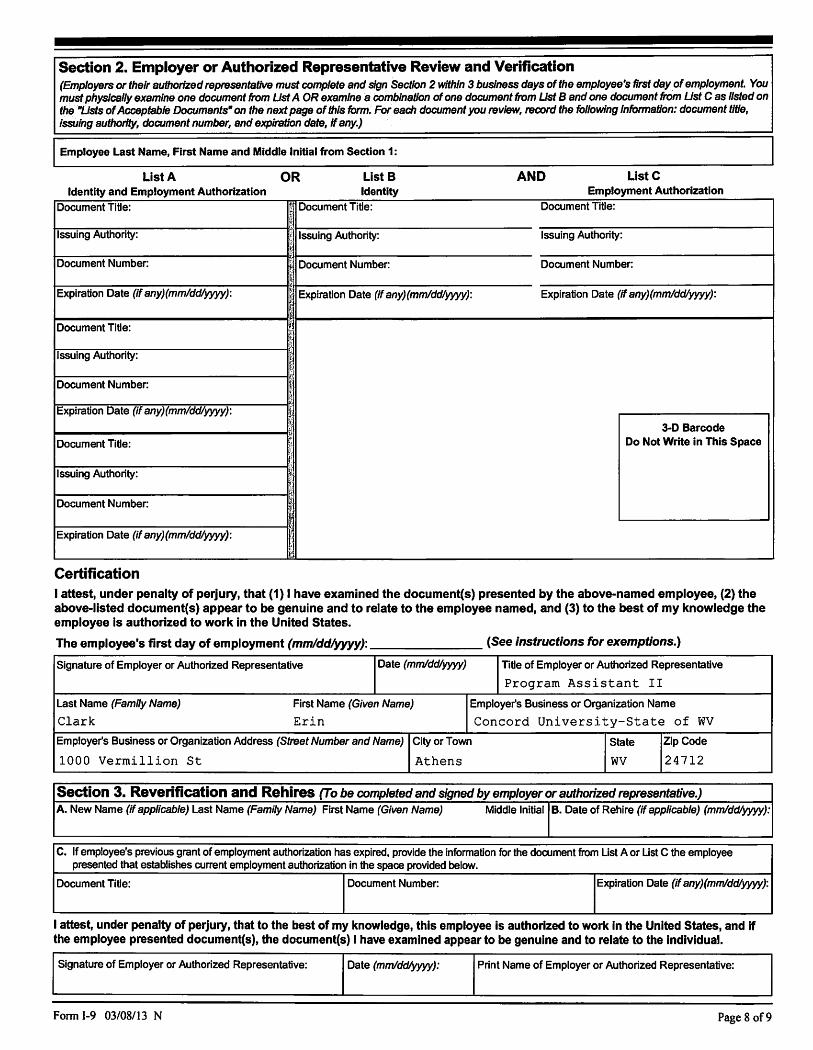
Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day.of employment. You must physically examine one document from Ust A OR examine a coinbinatlon of one document from Ust B and one document from Ust C as fisted on the "Usts of Acceptable Documents" on the next page of this form. For each document you review, record the following Information: document title, Issuing authority, document number, and expiration date, If any.)
Employee Last Name, First Name and Middle Initial from Section 1:
List A Identity and Employment Authorization
Document Title:
Issuing Authority:
Document Number:
Expiration Date (if any)(mm/ddlwyy):
Document Title:
Issuing Authority:
Document Number:
Expiration Date (If any)(mmlddlwyy):
Document Title:
Issuing Authority:
Document Number:
Expiration Date (if any)(mm/ddlyyyy):
Certification
OR List B Identity
% Document Title:
I Issuing Authority; .1
t J Document Number:
Expiration Date (if any)(mmlddlwyy):
~ ~I ,1
l !
V.
1: t
I {:f cl
AND ListC Employment Authorization
Document Title:
Issuing Authority:
Document Number:
Expiration Date (if any)(mmlddlYWY):
3-D Barcode Do Not Write in This Space
I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States.
The employee's first day of employment (mmldd/yyyy): (See instructions for exemptions.)
Signature of Employer or Authorized Representative Date (mrnlddlyyyy) Title of Employer or Authorized Representative
Program Assistant II
Last Name (Family Name) First Name (Given Name) Employer's Business or Organization Name
Clark Erin Concord University-State of WV Employer's Business or Organization Address (Street Number and Name) City or Town State Zip Code
1000 Vermillion St Athens WV 24712
Se~ion 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.) A. New Name (If applicable) Last Name (Family Name) First Name {Given Name) Middle lnltlal I B. Date of Rehire {If applicable) (mmlddlyyyy):
C. If employee's previous grant of employment authorization has expired, provide the information for the document from List A or List C the employee presented that establishes current employment authorization in the space provided below.
Document Title: Document Number: Expiration Date (if any)(mmlddlyyyy):
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual.
Signature of Employer or Authorized Representative: Date (mmldd/yyyy): Print Name of Employer or Authorized Representative:
Form 1-9 03/08/13 N Page 8 of9
1.
2.
3.
4.
5.
6.
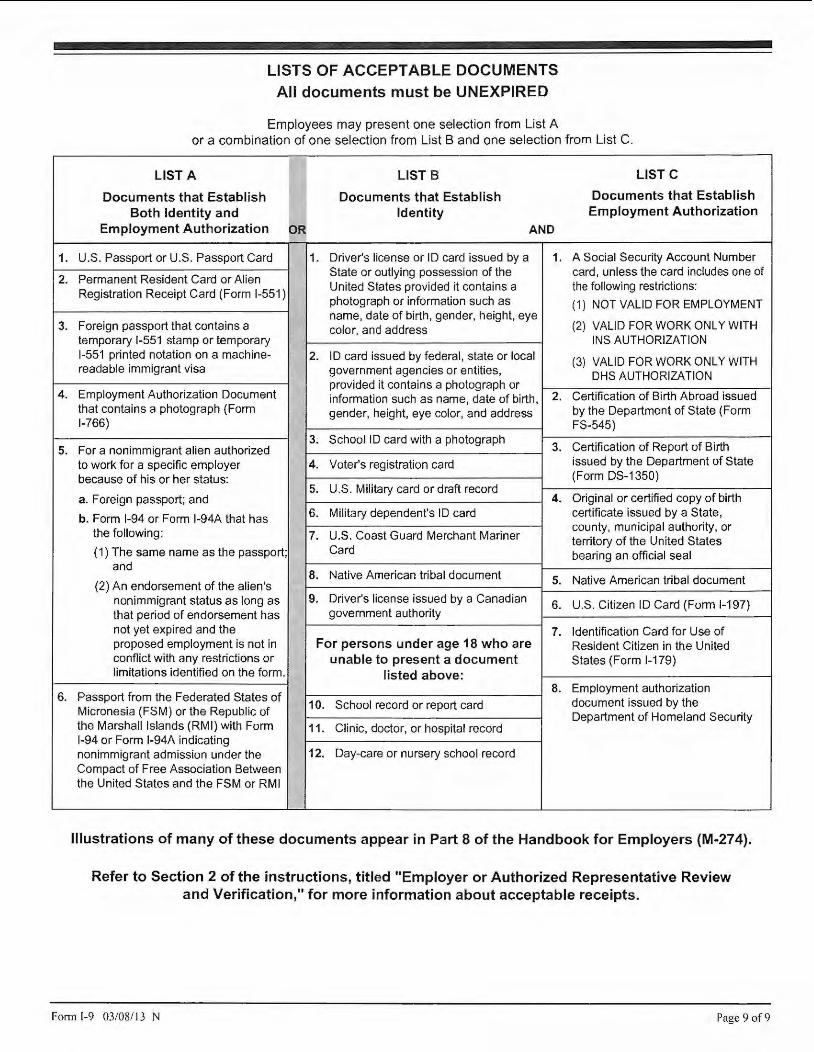
LISTS OF ACCEPTABLE DOCUMENTS All documents must be UNEXPIRED
Employees may present one selection from List A or a combination of one selection from List B and one selection from List C.
LIST A LIST B LISTC
Documents that Establish Documents that Establish Documents that Establish Both Identity and Identity Employment Authorization
Employment Authorization OR AND
U.S. Passport or U.S. Passport Card 1. Driver's license or ID card issued by a 1. A Social Security Account Number
Permanent Resident Card or Alien State or outlying possession of the card, unless the card includes one of
Registration Receipt Card (Form 1-551) United States provided it contains a the following restrictions: photograph or information such as (1) NOT VALID FOR EMPLOYMENT
Foreign passport that contains a name, date of birth, gender, height, eye
(2) VALID FOR WORK ONLY WITH color, and address temporary 1-551 stamp or temporary INS AUTHORIZATION 1-551 printed notation on a machine- 2. ID card issued by federal, state or local (3) VALID FOR WORK ONLY WITH readable immigrant visa government agencies or entities, OHS AUTHORIZATION
Employment Authorization Document provided it contains a photograph or information such as name, date of birth, 2. Certification of Birth Abroad issued
that contains a photograph (Form gender, height, eye color, and address by the Department of State (Form 1-766) FS-545)
3. School ID card with a photograph 3. Certification of Report of Birth For a nonimmigrant alien authorized
to work for a specific employer 4. Voter's registration card issued by the Department of State
because of his or her status: (Form DS-1350) 5. U.S. Military card or draft record
a. Foreign passport; and 4. Original or certified copy of birth
b. Form 1-94 or Form l-94A that has 6. Military dependent's ID card certificate issued by a State,
the following: 7. U.S. Coast Guard Merchant Mariner county, municipal authority, or territory of the United States
(1) The same name as the passport; Card bearing an official seal and
8. Native American tribal document (2) An endorsement of the alien's 5. Native American tribal document
nonimmigrant status as long as 9. Driver's license issued by a Canadian 6. U.S. Citizen ID Card (Form 1-197) that period of endorsement has government authority not yet expired and the 7. Identification Card for Use of proposed employment is not in For persons under age 18 who are Resident Citizen in the United conflict with any restrictions or unable to present a document States (Form 1-179) limitations identified on the form . listed above:
8. Employment authorization Passport from the Federated States of
10. School record or report card document issued by the Micronesia (FSM) or the Republic of Department of Homeland Security the Marshall Islands (RMI) with Form 11. Clinic, doctor, or hospital record 1-94 or Form 1-94A indicating nonimmigrant admission under the 12. Day-care or nursery school record Compact of Free Association Between the United States and the FSM or RMI
Illustrations of many of these documents appear in Part 8 of the Handbook for Employers (M-274).
Refer to Section 2 of the instructions, titled "Employer or Authorized Representative Review and Verification," for more information about acceptable receipts.
Fonn 1-9 03/08/1 3 N Page 9 of9
wvOASIS PAYROLL DIRECT DEPOSIT FORM INSTRUCTIONS
In order to process a Payroll Direct Deposit request the employee must do the following:
1. Provide First and Last Name 2. Provide wvOASIS Employee ID - (Can be provided by your payroll department.) 3. Provide Social Security Number 4. Complete, Sign, and Date the fom1. 5. Deliver the form with your account documentation to your State Agency Payroll Department for completion.
Payroll Primary Account
l. List the Financial Institution Name. Your net pay will be going to the Financial Institution Name listed.
2. Indicate whether the account is checking or savings. Mark one box ONLY!
a. Checking Attach a voided check, Financial Institution statement, or a letter from the Financial Institution (on FI letterhead) listing the account information, printed name, and signature of the Financial Institution representative, title and contact information.
b. Savings Attach a Financial Institution statement or letter from the Financial Institution (on FI letterhead) listing the account information, printed name, and signature of the Financial Institution representative, title and contact infonnation.
3. Indicate by marking the appropriate box. Mark one box ONLY!
a. Start Direct Deposit Net pay is currently not setup for direct deposit.
b. Change Net pay is currently setup for direct deposit and you want to send your net pay to a different account or Financial Institution. Do not close your old account until you have received a payment in the new account. This will help prevent a delay in receiving your pay.
c. No Change Continuing with the current direct deposit for your net pay. Mark this box only if you are requesting an add, change or cancel to a secondary account.
Payroll Secondary Account(s)
1. List the Financial Institution Name. Your secondary account will be going to the Financial Institution Name listed.
wvOASIS PAYROLL DIRECT DEPOSIT FORM INSTRUCTIONS
Payroll Secondary Account(s) - Continued
2. Indicate whether the account is checking or savings. Mark one box ONLY!
a. Checking Attach a voided check, Financial Institution statement, or a letter from the Financial Institution ( on FI letterhead) listing the account information, printed name, and signature of the Financial Institution representative, title and contact information.
b. Saving Attach a Financial Institution statement or letter from the Financial Institution ( on FI letterhead) listing the account information, printed name, and signature of the Financial Institution representative, title and contact information.
3. Indicate by marking the appropriate box. Mark one box ONLY!
a. Start Direct Deposit A secondary account that is currently not setup for direct deposit.
b. Change A secondary account is currently setup for direct deposit and you want to send your set amount to a different account, Financial Institution, or wish to change your set amount. Do not close your old account until you have received a payment in the new account. This will help prevent a delay in receiving your pay.
c. Cancel No longer want your secondary account(s) direct deposited.
d. No Change Continuing with the current direct deposit for your secondary account(s). Mark this box only if you are requesting an add, change, or cancel of the Primary Account and/or requesting an add, change or cancel to another secondary account.
4. The dollar amount must be the same for each pay period.
5. More than two secondary accounts will require an additional form to be completed and signed.
To complete the employee's Payroll Direct Deposit request, the State Agency Payroll Department must do the following:
1. Provide the State Agency Name. 2. Provide a Phone Number. 3. Sign and Date the fonn. 4. Review the form and make sure it has been completed. 5. Attach the form along with the documentation to the NPD document prior to submitting into the workflow.
wvOASIS Payroll Direct Deposit Form West Virginia State Auditor's Office, ePayments Division - 1900 Kanawha Blvd., E., Bldg. I, Room W- 121, Charleston, WV 25305
Telephone: 1-800-500-4079 Fax: (304) 340-5084 www.wvsao.gov
- PLEASE f OR\V ARD TO YOUR STATE ACE>JCY PAYROLL DEPARTMENT ():',JC£ COM PLETED -
First Name: I Ml: I Last Name: I
wvOASIS I Employee ID: I I I I I I I I I
SSN: I I I -- I I - - I I I I PAYROLL PRIMARY ACCOUNT:
Bank Name: I 1 Start Direct Deposit 1 Change 1 No Change
1 Checking - Attach a voided check.
Routing #: I 1 Saving
Account #: I
PAYROLL SECONDARY ACCOUNT(S): If you have more than two secondary accounts, please complete an additional form.
Bank Name:I r Start Direct Deposit 1 Change 1 Cancel I No Change
r Checking - Attach a voided check.
Routing #: I r Saving
Account #:! Dollar Amount: I I I I • I I 1 NoChange
Bank Name:! r Start Direct Deposit 1 Change 1 Cancel
r Checking - Attach a voided check.
Routing #: I r Saving
Account #:! Dollar Amount: I I I I • I I I hereby authorize t he State of West Virg inia, hereinafter ca lled STATE, to initiate credit entries to the account(s) as indicated above and to in itiate debit entries as adjust ments for credit entries made in error. The STATE w il l not be responsible for any loss that may arise solely by reason of error, mistake or fraud regarding information provided on this form. This aut hority is to remain in fu ll force and effect until I have filed a new payroll form in a t imely manner so as to afford t he STATE a reasonable opportunity to act. I furth er acknow ledge that my employee pay stub w ill be made avai lable t o me through a secure internet web site.
Employee's Signature: Date:
To be completed by the State Agency Payroll Department.
State Agency:jconcord University-State of WV Phone #~304-384-5272
I hereby certify I am a payroll representative of the herein named State Agency and that being so authorized I do certify the information listed and attached w ith this authorization has been received from the employee indicated above.
Payroll Representative's Signature: Dat e: I
Pursuant to Section 7 o f the Privacy Act of 1974, the disclosure of your Social Security Number is mandatory. Social Secu rity Numbers are necessary to properly maintain records concerning your
direct deposi t payments as is requ ired and authorized by the federal government for tax administration purposes. See generally, 42 U.S.C. § 40S(c). Fai lure to provide a Social Securi ty Number will prevent us from processing your di rect deposit request. Version 1 .0
WV PAY CARD FORM INSTRUCTIONS
In order to process a WV Pay Card request, the following employee information must be provided:
I. First and Last Name 2. EPICS Number & wvOASIS Employee ID (This can be provided by your State Agency PayrollDepartment.)
(Phase one employees must supply both numbers!) 3. Social Security Number 4. Home Phone Number 5. Mailing Address {This address must match the address on file in EPICS.) 6. Date of Birth 7. Employee's Signature and Date
Once the information above has been provided, forward request to your State Agency Payroll Departmentfor completion.
To complete a WV Pay Card request, the State Agency Payroll Department must do the following:
1. Provide the State Agency Name 2. Provide Phone Number 3. Review the form and make sure it has been completed properly. 4. Sign and Date the form.
Once the information above has been completed, forward the form to the West Virginia State Auditor's Office, ePayments Division.
WV Pay Card Form West Virgin ia State Auditor's O ffice, ePayments Division - I 900 Kanawha Blvd., E., Stale Capito l, Bldg. I , Room W-12 1, Charleston, WV 25305
Telephone: J-800-500-4079 Fax: (304) 340-5084 www.wvsao.gov
Pursuant to Section 7 of the Privacy Act of 1974, the disclosure of your Social Security Number is mandatory. Social Security Numbers are necessary to properly maintain records concerning your
direct deposit payments as is required and authorized by the federal government for tax administration purposes. See generally, 42 U.S.C. § 40S(c). Failure to provide a Social Security Number w i ll prevent us from processing your request. The information below will be used by Citi to verify identification in order to be in compliance with the USA Patriot Act and the Of AC verification.
~l':'.''.1-i/-- EMPLOYEE INFORMATION " !a ·.·•:,-c~
First Name: I Ml:D Last Name:I I
EPICS #: I wvOASIS Employee ID: I
SSN:DDD- DD- DODD
Home I Phone#: I Mailing Address:
City: State:! I Zip Code:! I
DateofBirth:D D DD DODD M M D D y y y y
I hereby authorize the State of West Virgin ia, hereinafter cal led STATE, to initiate credit entries to my WV Paycard as indicated, and to initiate debit entries as adjustments for credit entries made in error. The State w ill not be responsible for any loss that may arise so lely by reason of error, mistake or fraud regarding information provided on this form. Th is authority is to remain in full force and effect until I have filed a new payroll form in a timely manner so as to afford the STATE a reasonable opportunity to act. I further acknowledge that my employee pay stub will be made available to me th rough a secure internet web site.
Employee's Signature: --- - - - ------ ----------- --------Date: IL._ ______ _,
To be completed by the State Agency Payroll Department.
State Agency:IConcord University-State of WV I Phone #:,304-384-5272
I hereby certify that I am a payroll representative of the herein named agency and being so authorized I do certify the information listed and attached has been received from the named employee.
Payroll Representative's Signature: Date:._! _ _ _ __ __,
New Health Insurance Marketplace Coverage Options and Your Health. Coverage
SMWWi&SWffiwtMiA\N#Bdi&i ie&--Q CA #AS&tiW f &RB MWiNilb&RPA 1 t&Neree 'Ri+ 1i11Hm@tN1
PART A: General Information
Form Approved 0MB No. 1210-0149 (expires 1-31 -2017)
ff¥Mif&&f8¥9MM E&GP l6EWS¥U
When key parts of the health care law tak e effect In 2014 , there will be a new way to buy health insurance: the Health Insuranc e M arketplace . To assist you as you evaluate options for you and your family, this notice provides some basic Information abou! _the new Marketplace and employment-based health coverage offered by your employer.
,.
· What is the Health Insurance Marketplace?
The Marketplace !s designed to help you find health Insurance that meets your needs and fits your budget. The
Marketplace o ffers "one-stop shopping " to f ind and com pare private health lnsurnnce options. You may also be eligible
for a new kind of ta x credit that lowers your m onthly prem ium right away. Open enrollment for health Insurance coverage throuqh the Marketplace begins In October 2013 for coverage starting as early as January 1, 2014.
Can. I Save Money on my Health Insurance Premiums in the Marketplace?
You may qualify to save money and lower your monthly prem ium, but only If your employer does not offer coverage , or offers coverage that doesn't meet certain standards. The savings on your premium that you' re ellglble for depends on your household Income.
Does Employer Health Coverage Affect Eligibility for Premium Savings through the Marketplace?
Yes. If you have a n offer of health coverage from your employer that meets certain standards, you will not be eligible
for a tax c redit through the Marketplace and may wish to enroll In your employer's health p lan. However, you may be
ellglbie for a tax credit that lowers your monthly prem ium, or a reduction In certain cost-sharing If your employer does not offer coverag·e to you at all or does not offer coverage that meets certain standards. If the cost of a plan from your employer that would cover you (and not any other members of your family) Is more than 9.5% of your household
Income f or the year , o r If the ·coverage your employer provides does not meet the "m inimum value" standard set by the Affordable Care A c t , you may be eligible for a tax credit. 1
Note: If you purchase a health plan through the Marketplace Instead of accepting health co"'.erage offered by your
employer, then you may lose the employer contribution (if any) to the employer-offered coverage. Also, this employer contribution -as well as your employee contribution to employer-offered coverage- Is often excluded from Income for
Federal and State Income tax purposes. Your payments fo r coverage through the Marketplace are made on an aftertax basis.
How Can I Get More Information?
For mor e Inform ation about your coverage offered by your employer, please check your summary plan description or
contact Concord University Human Resources at 304-384-SJ 21. -----------------------
The Marketplace can help you evaluate your coverage options, Including your eligibility for coverage through the
Marketplace and Its cost. Please visit HealthCare.gov f or more Inform ation, Including an onllne application for health
Insurance coverage and contact Information for a Health Insurance Marketplace In your a rea.
· l An employer-spo~sor.ed health plan meets the. 'm inimum value stand ard ' If lhe plan's share of the total allowed benefit costs covered by the plan Is no less tha n 60 percenl of such costs .
PART B: Information About Health Coverage Offered by Your Employer This section contains Information about any health coverage offered by your employer. If you decide to complete an appllcatlon for coverage In the Marketplace, you wlll be asked to provide this Information. This Information Is numbered to correspond to the Marketplace appllcatlon.
Here Is some basic Information about J:lealth coverage offered by this employer: •As your employer. we offer a health plan to: •
D Al.I employees. Ellglble employees are:
. ", ·� ..··.·. : . . ·,·
[i] Some emplqyees. Ellalble ernployees are: .. · . Permanent.. full-time employees working regularly at least 20 hours per week (�ludes �ontrac� tenn. and ��n-p�encnip�iti;� . .. -''.:. ·.. such a adjunct faculty. student employees and tempormy / casual employees �O � expected to WO� less than �9 _ho� p
0
f!!�}::--:: . .
·. .. . . . . .
.·. ; .. i }i;�fa{/;;'' • With respect to dependents:
[iJ We do offer coverage. Ellglbfe dependents are: . . : .: : . . .
. :· .. ' ' . � . . .
.. .,. D We do not offer coverage.
.. · ....
· -:: ', · ... ·)\t1t.Jtft· ,·· . •:..\ ••• • *·
· :· .. c . ;, .·. , ·:. ··-
[i] If checked, this coverage meets the minimum value standard, and the cost of this coverage to you Is Intended to be affordable. based on employee wages.
u Even ·1r your employer Intends your coverage to be affordable. you may stlll be ellglble for a premium discount through the Marketplace. The Marketplace wlll use your household Income, along with other factors, to determine whether you may be eltgfble for a premium discount. If, for example, your wages vary from week to week (perhaps you are an hourly employee or you work· on a com mission basis), If you are newly emplayed mid-year, or If you have other Income losses, you may still qualify for a premium discount.
If you decide to shop for coverage In the Marketplace, HealthCare.gov will guide you through the process. Here's the employer Information you'll enter when you visit HealthCare.gov to find out If you can get a tax credit to lower your monthly premiums.
Printed Name:
EMPLOYEE RECEIPT AND ACKNOWLEDGEMENT OF AFFORADABLE CARE ACT MARKETPLACE NOTICE
I hereby state that I have received a copy of the Affordable Care Act Insurance Marketplace Notice.
Signature: Date:
The Information below corresponds to the Marketplace Employer Coverage Tool. Co1T1pletlng this section Is optional for employers, but will help ensure employees understand their coverage choices.
13. Is the employee currently eligible for coverage offered _by this employer, or will the employee be eligible in the next 3 months? ·
D Yes (Continue) · · 13a. If the employee Is not eligible today, Including as a result of a waiting or probationary period, wh·en Is the
employee ellglble for coverage? (mm/dd/yyyy) (Continue) · D No (STOP and r~turn this form to employee)
If the plan year wlli end soon and you know that the health plans offered will change, go to question 16. If you doh't know, STOP and .return form to employee."
16. What change will the employer make for the new plan year? _____ _
B EmP.loyer won't offer health coverage . · Employer will start offering health coverage to employees or change the premium for the lowest-cost plan available only to the employee that meets the minimum value. standard.* (Premium should reflect. the discount for wellness programs. See question 15.)
a. How much would the emp!f!Yee have to pay In premiums for this plan? $=....------.:::=-b. How often? Oweekly LJEyery 2 weeks 0Twlce a month D Monthly D Quarterly .OYearfy
• An employer-sponsored health plan meets the •minimum value standard• If the plan's share of the total allowed benefit costs covered by the plan Is no less .than 60 percent of such costs (Section 36B(c)(2)(C)(II) of the Internal Revenue Code of 1986)
KRONOS Information
1. If you have one job, you will be clocking in on the
KRONOS system and approving your time in KRONOS.
You and your supervisor must approve your time in
KRONOS every other Friday.
2. If you have more than one job, you will be clocking in on
the KRON OS system for your primary job. You and your
supervisor must approve your time in KRONOS every oth
er Friday. Your supervisor will be turning in a paper time
card to the Student Payroll Office for your secondary job.
You will be clocking in for ________ _
You will fill out a timecard for --------
Your Oasis employee ID is ________ . You will
use this number to clock in with.
If you were awarded Federal Work Study, you may work an
average of ___ hours a week during the semester.
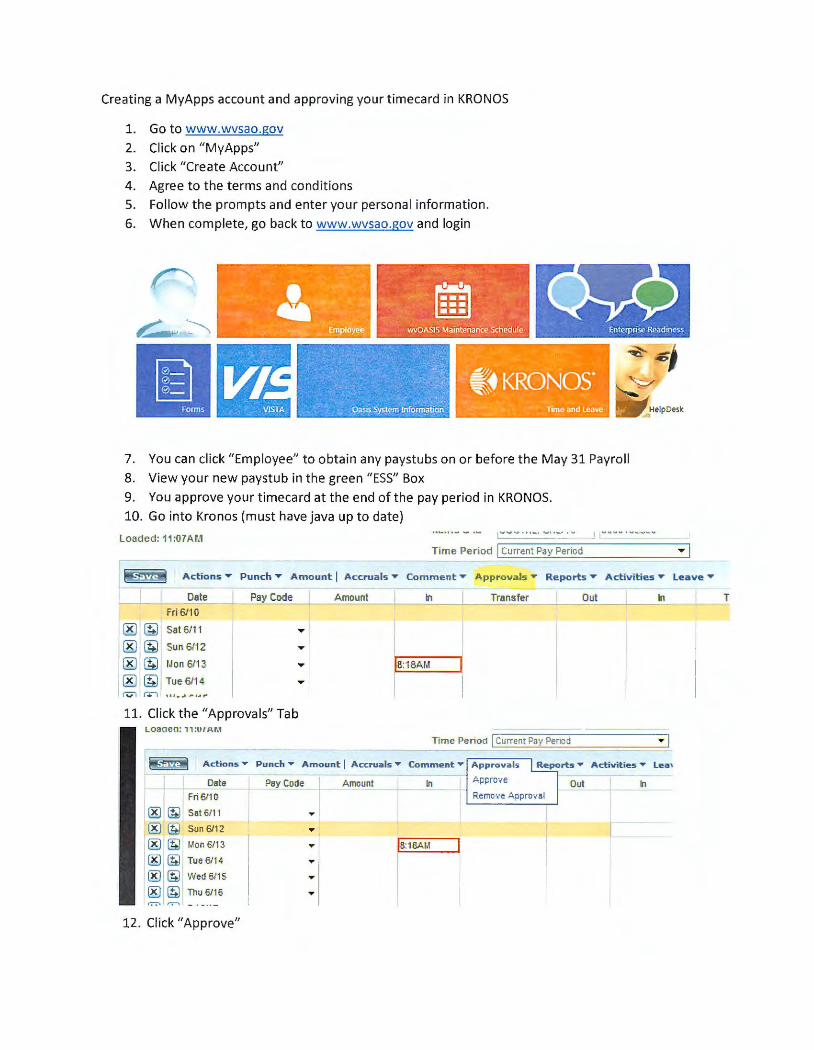
Creating a MyApps account and approving your timecard in KRONOS
1. Go to www.wvsao.gov
2. Click on "MyApps"
3. Click "Create Account"
4. Agree to the terms and conditions
5. Follow the prompts and enter your personal information.
6. When complete, go back to www.wvsao.gov and login
. - -. . .
. . ... ~ , .. ·~·.• . ..:;) ~ . . ~ , .
,. .. ~-·:._~·-~mpl5y~e:·
. - ·. ..· ,;. .
i ~•KRON05 ~~ . '
.,o. .• ~ ~ ..
. ::'~~~:~ •• .. 11~eandleave
7. You can click "Employee" to obtain any paystubs on or before the May 31 Payroll
8. View your new paystub in the green "ESS" Box
9. You approve your timecard at the end of the pay period in KRONOS.
10. Go into Kronos (must have java up to date)
Loaded: 11 :07 AM Time Period I Current Pi!)' Period
8$.M Actions .,.. Punch ,.. Amount I Accruals .,.. Comment .,.. Appr ovals .,.. Reports .,.. Activities .,.. Leave .,..
Date Pay Code Amount Ill Transfer Out In Fri 6/10
® (!;) Sat 6/11 .... ® (!;) Sun 6/12 .... ® (!;) l,lon 6/13 .... !8:18Al,1
®@ Tue6/1 4 .... (v"I r..:-, , .. , • .,. ,.. , ., r
11. Click the "Approvals" Tab LOaaea: 11:U I AM
Time Penod I Current Pe\• Period
~ Actions• Punch ... Amount I A ccrua ls • Comme nt • Approva l s Activities • Lea,
Date Pay Code Amount In A pprove Out In Fri6110 Remo·,e A pproval
® @ Sat 6/11 ... ®@ Sun 6112 ... ® @ l,l on 6113 !8:18Ar.l
®@ Tue 6114 ... ®@ Wed6115 ... ®@ Thu 6/16 ... I":"":"\ r.-'\
12. Click "Approve"
T
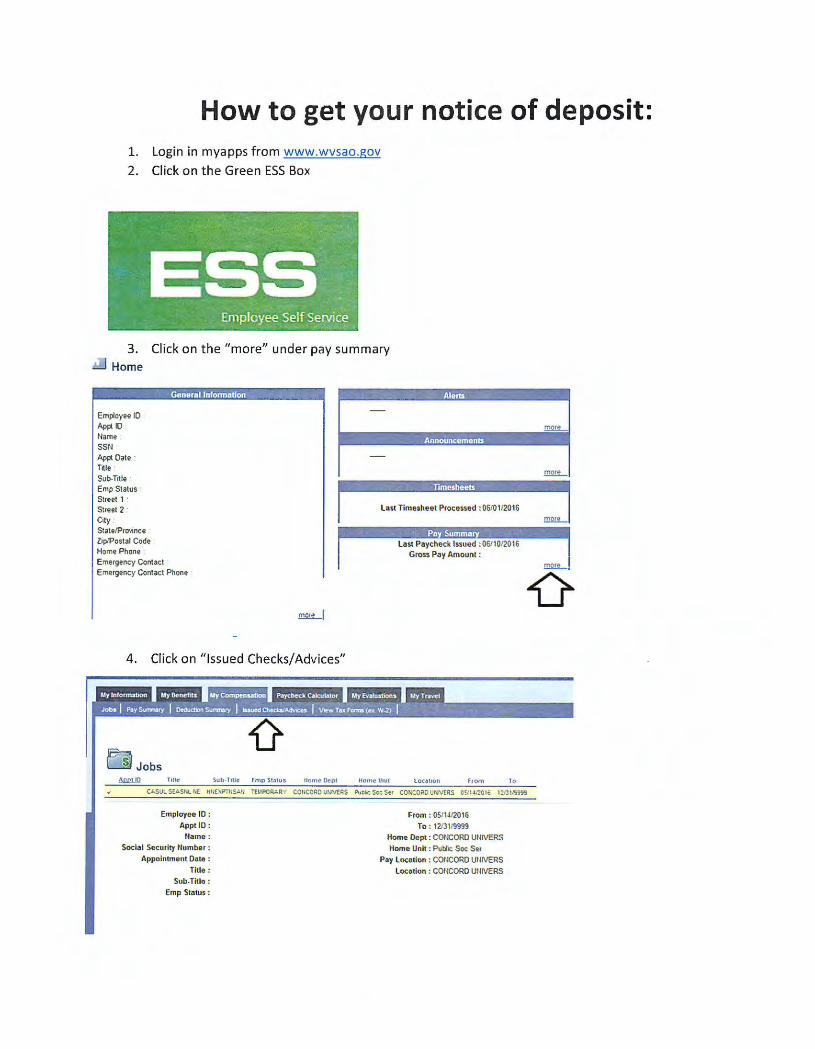
How to get your notice of deposit: 1. Login in myapps from www.wvsao.gov
2. Click on the Green ESS Box
3. Click on the "more" under pay summary .!:!...l Home
Employee 10 Appl 10 Name SSN Appl Date l"rtle Sub-Title Emp Status Streel 1 Street 2 C,ty S1a1e/Pr0\1nce Z1p/Postal Code Home Phone
Goner11l lnform111fon
Emergency Contact Emergency Contact Phone
!!l2.!LI
4. Click on "Issued Checks/Advices"
Ei Jobs Tille Sub-Tille [ mp S1.stu s ttomc~pt
Employee 10 : Appl ID :
Name :
Social Security llumber :
Appoinlment Onto :
Ti tle:
Sub-Ti tle:
Emp Status:
Last Timeshoet Proce .. ed :06/0 1/20 16
Last Paycheck l$SUOd :06/10/20 16 Gross Pay Amount :
HomcUm1 from
From : OS/lJ/2016
To: 1213 119999
Home Dept : CONCORD UNIVERS
Home Uni t : Pubic Soc Str
Pay Location : CONCORD UlllVERS
Location : CONCORD UNIVERS
l o
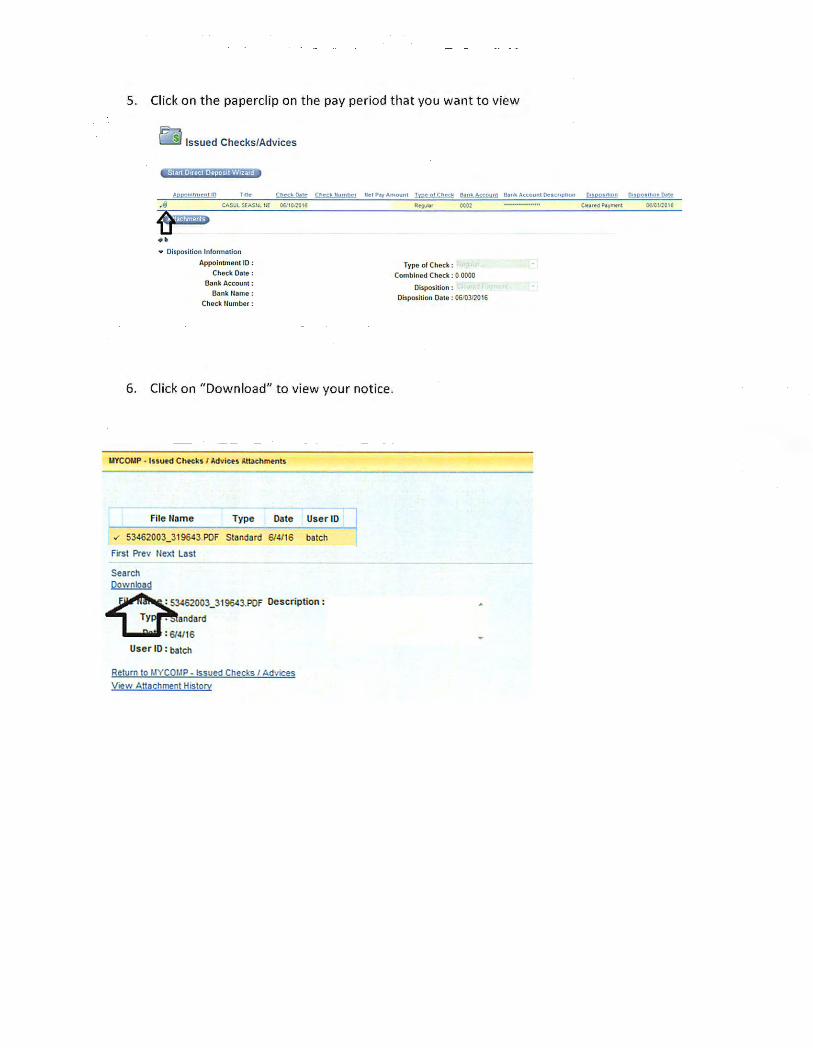
5. Click on the paperclip on the pay period that you want to view
~ Issued Checks/Advices
.,~ C.t.SULSUSULUE w 1cnc18
•• • Oispot ltion Information
Appointment 10 :
Chec.k Dote : Bilnk Ac:counl :
~nk Name:
Chock Uumber :
6. Click on "Download" to view your notice.
UYCOI.IP · lnutd Chtek• I Advi~• Amchmt nts
file Harne Type Date User lD
.,, 53462003_319643.POf Standard 6/4/16 batch
f irst Prev Next Last
Search
~
3462003_319643.POf
andard
6/4/16
User ID : batch
Description :
Return to MYCOl,IP - Issued Checks / Advices V,ew Attachment History
fyv. 0 1 r.htctr t\1111!,_A,:counJ &nk >.ccounl Oea c11s:i1ioo
Type of Chock : Combined Chock : 0 0000
Oisposilion : Dispositio n Doto : 06/03/2016







