Continuity and tension in the definition, perception and enactment of the first-line management role in health care
Colin Hales, Carole Doherty and Mark Gatenby

Outline
•Research questions•What is first-line management•Method•Findings- Ward managers/ward sisters
- Service managers•Comparison of the roles•Implications for practice

Research Questions
How has the FLM role been both shaped and experienced in health care?
1.How is the FLM role in healthcare defined, both formally and in terms of others’ expectations?
2.What is the balance between routine supervision, performance management, team leadership and wider resource management responsibilities and what are the tensions between these?
3.How do FLMs interpret, experience and enact their role?

What is the role of first-line managers?
The first level of management to whom non-managerial employees report. The role is:
- centred on the day to day supervision of a limited organisational operational sub-unit/work group
- responsibility for the key functions of ‘keeping production going’ and translating strategy into operational reality
- Tasks included supervision, monitoring and reporting of operational activities

What is the role of first-line managers?
Changes has been towards
Re-division of managerial labour to produce an expanded FLM role
Downward shift has often been to professionals
Decision making and accountability confined largely to operations
Are they coaches of self managing teams/ mini-general managers of cost centres/business units with commensurate authority over budgeting, staffing decisions and accountability for performance?
or
Has their supervisory core has been strengthened by needed to handle a growth in operational activity or comply with more external regulation?

Method
‘Mixed paradigm’ – combination of critical realism and sense-making
A critical realist lens - focus on the structural conditions which constrain and enable FLMs’ actions and interactions
A sense-making lens - focus on the detailed processes of FLMs’ actions and interaction
•Case study approach: - two types of FLM role (the ward sister/charge nurse as a ‘practitioner-manager’ and one ‘general line manager’) - two hospital trusts (Alpha and Beta) hospitals selected for ‘typicality’

Data collection methods
Organisational documents, in-depth interviews and ethnographic observations.
Data on how the FLM roles are constituted by the connection between others' expectations and FLMs' own role perceptions and interpretations were collected in four stages:
1.Identifying the FLMs’ role sets 2.Eliciting role set members’ expectations of the FLM role3.Eliciting FLMs’ perceptions of their own role4.Investigating FLMs’ sense-making of others’ expectations

Data collection methods
Ethnographic observations took two forms:
Firstly, 7 FLMs, 3 in Alpha and 4 in Beta were work shadowed over the course of one or more working days. 10 days of work shadowing were conducted in total
Secondly, the research team were invited to sit in on and observe a series of training days for Ward Sisters at Beta. These took the form of presentations by senior managers on topics and issues considered to be of relevance to the WS role, followed by small-group and subsequent plenary discussion of these topics

Findings.Expectations of the Ward Sister/Charge Nurse RoleNursing and clinical work – ‘The pure professional role’
Clinical credibility
TeacherDoing ‘fair share’ of nursing work
Mentor
Management within the clinical roleManagement beyond the
clinical role
Being in charge – ‘the captain of the ship’
Human resource management
Conflict resolutionPerformance monitoring/reporting
Shaping the ward environment
Role Model
Supervisor and standard bearer
Managing patient ‘throughput’
Financial management
Formal complaints handling

Tensions

Ward Sister/Charge Nurse interpretation and enactment of their role
In general they re-affirm their identity as senior nurses by holding to the central importance and unchanging nature of patient care and the role of the WS as central to healthcare delivery.
‘The clinical work is still really important to me…. actually hands-on with a patient is [important]- I really like doing that, I wouldn't want to lose that at the moment. ... Obviously my priority is the patients (WS 2, Alpha)
…the job description says twenty-four hour responsibility which, you know, I took the job, I knew what it was about (WS 3, Alpha)

Ward Sister/Charge Nurse interpretation and enactment of their role
They comply with those targets and procedures which they cannot avoid by ‘box ticking’ and sometimes ‘gaming’ the system and falsify audit scores:
‘we lie about some of our audit data because if we didn't lie, then we'd be told off so sometimes it's easier to lie about it rather than do it properly’ (WS 6, Beta)
‘Clinical Governance meeting…it was horrible…I can still feel the palpitations from sitting there! It was horrible really intimidating’.
(WS 12, Beta)

Ward Sister/Charge Nurse interpretation and enactment of their role
Juggle tasks - usually by attending to immediate clinical issues at the expense of management tasks
‘I have it all planned in my mind so I come in at half past seven, telephone's ringing, somebody's off sick and then somebody else is off sick and then I think to myself, 'Right, that's those business cases gone today, another day to do those' ...help! What can I do? Knit nurses, that's what I say (WS 10, Beta)
‘We were trying to actively recruit a staff nurse and I knew that we kept missing her during the morning, then a child needed a nebuliser so I assist[ed] the child,…, then the nurse rang up and so I went into the office and discussed briefly, …what the role was about… how to apply… [I] then clicked straight back into taking the nebuliser off and doing the observation on the child again which I found quite weird at first, …so it's difficult to do your clinical and your management and not switch off either …’ (WS 2, Alpha)

Service Manager Role Set Expectations and Tensions
Who are first-line non-clinical managers?- They are variously labelled, Specialty Managers,
Service Managers, Operations Managers and Clinical Business Unit Managers
Common responsibilities and relationships are found in the job descriptions that, at least formally, help to define the role:
working closely with the General Manager, this post will play a key role in ensuring that the Specialist Medicine Directorate meets the requirements of the performance agenda.
The job description reinforces this relationship by outlining the relative responsibilities of the role:
work with the general manager … to ensure junior doctor rosters are compliant and provide the required support for the service
supported by their manager, the role will be responsible for policy implementation, and service development in their area

ConsultantsSenior managers
Junior staff
Operations – ensuring the smooth running of processes by reacting to and attempting to solve day to day problems in the system
Human resource management –
primarily of administrative staff
including medical secretaries, whom
SMs manage on behalf of the consultants
Finance and performance management - monitor breaches, account for breaches
Service Development - to provide the
‘nuts and bolts’ to enable the
implementation of consultants’
ideas for service development

Service Manager Role Set Expectations and Tensions
From the doctors’ perspective, there is a lot of ‘management for management’s sake’ and some aspects of the SMs’ role are seen to reflect this:
…management likes to go in for play …this…TPOT… irritates grown-up people to be honest and there is an awful lot of that so a [SM] has to be, I think, careful not to put the backs up people that have to work and deliver. (General Surgeon, Alpha)
Similarly some Ward Sisters take the view that there are ‘too many managers’:
Business managers have lots of meetings, not sure what about, they don’t decide much or make things happen. (Ward Sister, MHDU, Beta).

Service Manager interpretation and enactment of their role
SMs believe that they are personally responsible and accountable for the performance of ‘their’ SBUs.
They [finance] want to know what I'm going to be spending, is the activity we're doing making us money, how much money, how much activity we're going to put through, how much am I paying my doctors. (SM 1, Alpha)
Ultimately it is the consultants who are the arbiters of the cost-efficiency and effectiveness of the SBUs’ work performance and they make this clear to the SMs:
I've been told ... 'I will make sure that the operations are done but …if you haven't got enough capacity that's down to you rather than down to me.' …they're there to treat the patients, you're there to be the bureaucrat and see the numbers. (SM 4, Alpha)
There are a few really nasty bullies that are consultants but that's just because they think they're God. (SM, 6 Alpha)

Service Manager interpretation and enactment of their roleSMs enact their environment to manage the role pressure by constructing an
identity as dedicated, responsible individuals holding things together at the centre of their respective SBUs, cajoling, fixing and juggling both people and processes to maintain the unit’s functional integrity on a daily basis:
‘The minute I'm off on holiday, everything kind of falls apart, and I come back to over a thousand emails’. (SM 9, Beta)
They work long hours and ‘don’t do lunch’
‘I work part-time four days which means I work usually 40 hours a week, and that gives me some child care flexibility. If I was full time I would have to work a least 45 hours a week.’ (SM 4, Alpha)

Service Manager interpretation and enactment of their role
However, by enacting their environment in this way, SMs create the very conditions that they then have to manage. This can come at a cost to their health and emotional wellbeing:
I don't sleep very well , I dream about it all the time- I think about- it's absolutely completely taken over my entire life, my personal life, everything, I don't think about anything else… I wake up thinking about it. (SM 8, Beta)
I'm starting to feel it now, I've been unwell for about two weeks with colds and things … and I've been working like that since December and the minute you're off sick you're bullied. (SM 6, Alpha)
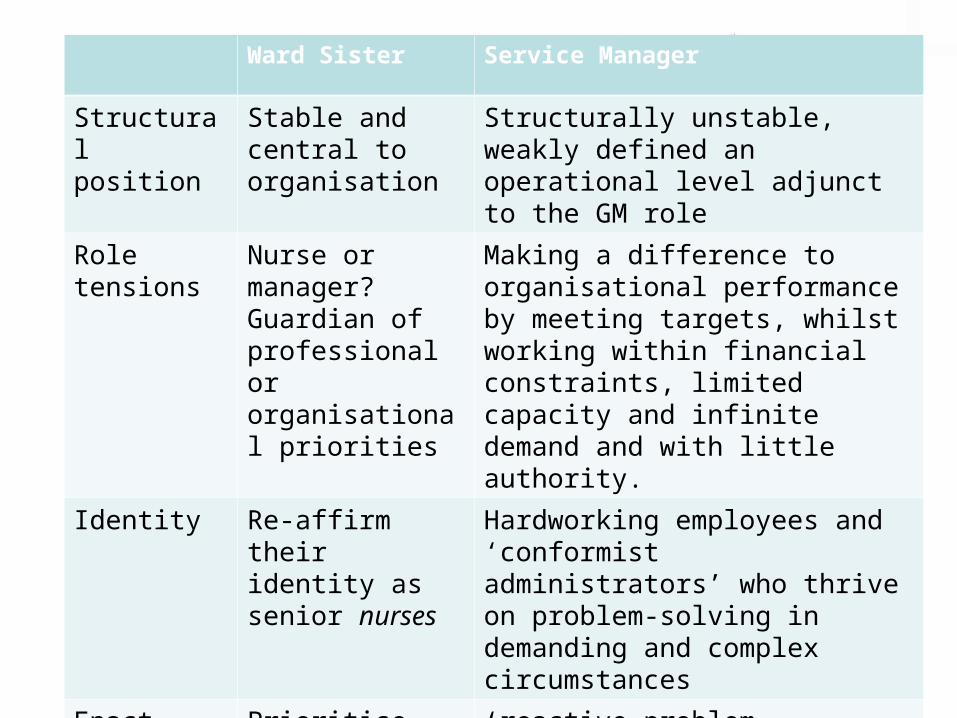
Ward Sister Service Manager
Structural position
Stable and central to organisation
Structurally unstable, weakly defined an operational level adjunct to the GM role
Role tensions
Nurse or manager?Guardian of professional or organisational priorities
Making a difference to organisational performance by meeting targets, whilst working within financial constraints, limited capacity and infinite demand and with little authority.
Identity Re-affirm their identity as senior nurses
Hardworking employees and ‘conformist administrators’ who thrive on problem-solving in demanding and complex circumstances
Enact environment by:
Prioritise clinical work reduce management to technique and box ticking
‘reactive problem-solving’, constantly monitoring waiting lists and waiting times, juggling and negotiating. They ‘walk the job’ and aim to be constantly available

Theory and Practice Implications
First-line management is a crucial for delivering and monitoring of healthcare services
•Ward Sisters have the clinical expertise, status and credibility to leverage nursing staff into undertaking changes to practice that will deliver cost-savings and meet performance targets, but may be loath and reluctant to do so since these changes clash with their professional orientations and values
•Management is a technique ‘need to learn the tricks of the trade’ rather than a political matter of confronting competing priorities.
•Service Managers are more comfortable with managerial values and priorities, and, hence, more sympathetic to a cost-saving, performance management project, lacking a clear role, credibility and authority and, therefore, leverage over the clinicians upon whom they must rely to implement change they will struggle to deliver on this.

Thank you for listening.
This project was funded by the National Institute for Health Research Service Delivery and Organisation (NIHR SDO) programme . Award number 08/1808/246. Department of Health disclaimer: The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NIHR SDO programme or the Department of Health.







