MET as a New Therapeutic Target in Lung Cancer:
Current Status & Future Directions
David R. Gandara, MD University of California Davis
Comprehensive Cancer Center
Alex A. Adjei Roswell Park Cancer Institute
Buffalo, NY USA
Apologies from Alex
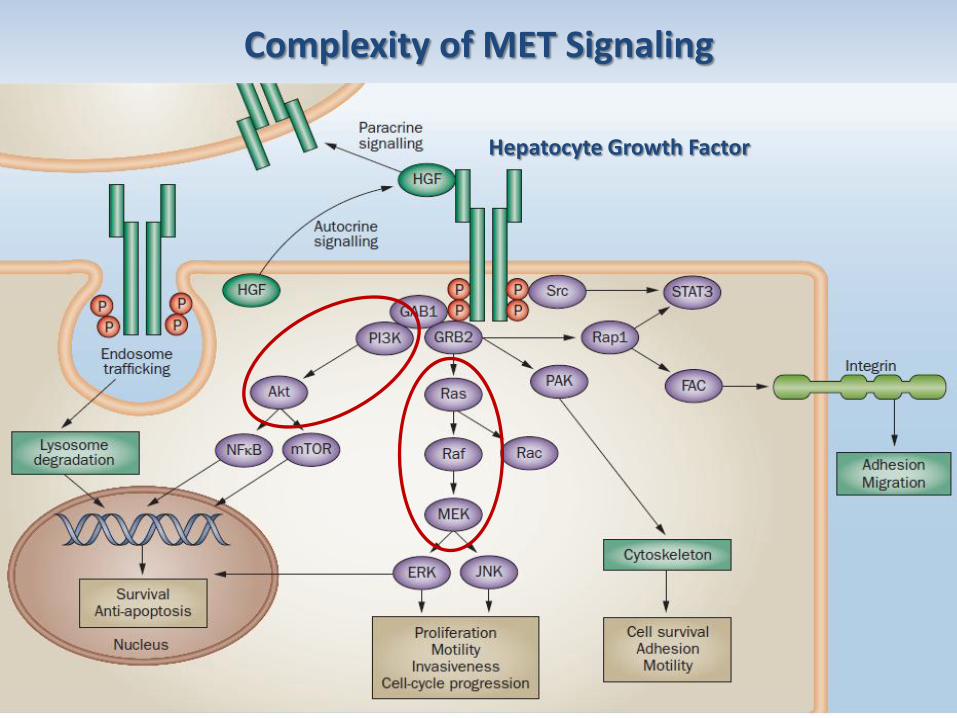
Complexity of MET Signaling
Hepatocyte Growth Factor
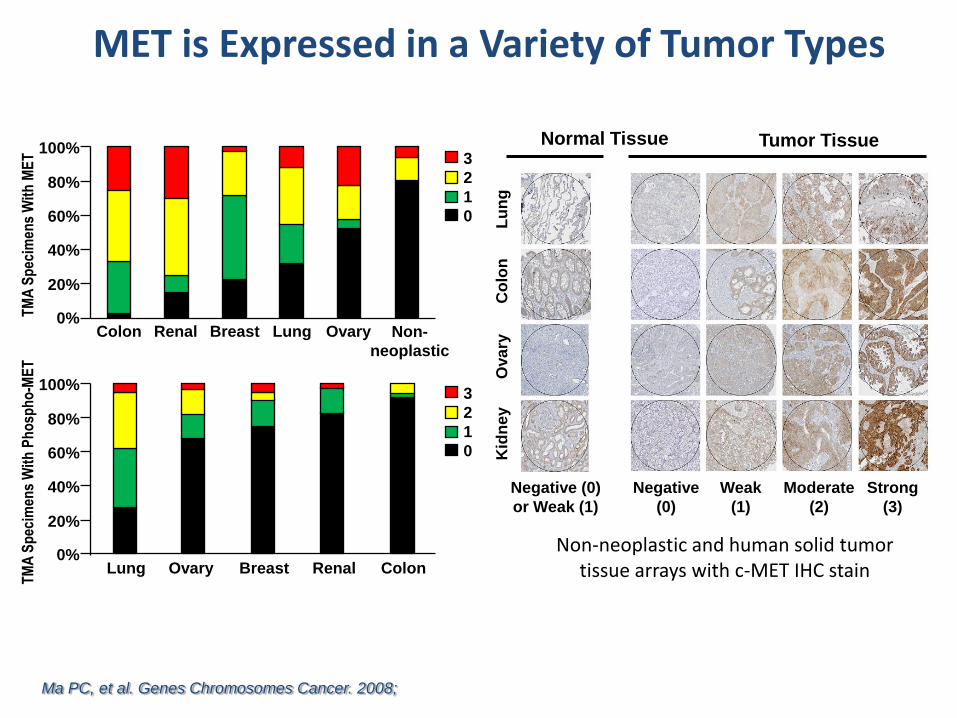
MET is Expressed in a Variety of Tumor Types
Non-neoplastic and human solid tumor tissue arrays with c-MET IHC stain
Ma PC, et al. Genes Chromosomes Cancer. 2008;
100%
80%
60%
40%
20%
0% TM
A S
pec
imen
s W
ith
ME
T
Colon Renal Breast Lung Ovary Non-
neoplastic
3
2
1
0
TM
A S
pec
imen
s W
ith
Ph
osp
ho
-ME
T
100%
80%
60%
40%
20%
0% Lung Ovary Breast Renal Colon
3
2
1
0
Tumor Tissue Normal Tissue
Kid
ney
Ova
ry
Co
lon
L
un
g
Negative (0)
or Weak (1)
Negative
(0)
Weak
(1)
Moderate
(2)
Strong
(3)
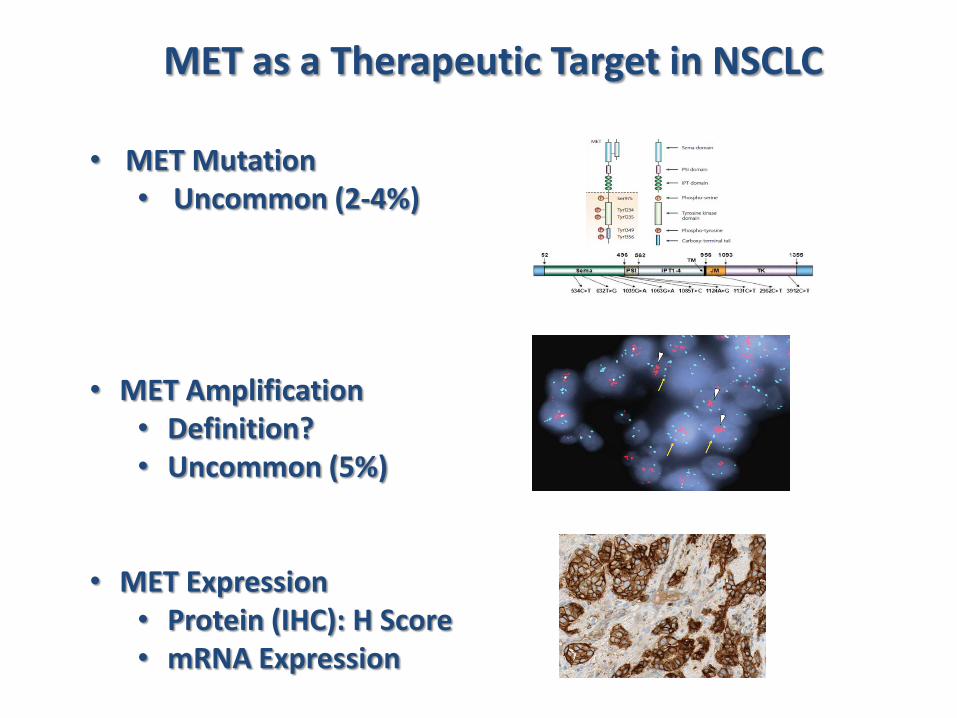
MET as a Therapeutic Target in NSCLC
• MET Mutation • Uncommon (2-4%)
• MET Amplification • Definition? • Uncommon (5%)
• MET Expression
• Protein (IHC): H Score • mRNA Expression
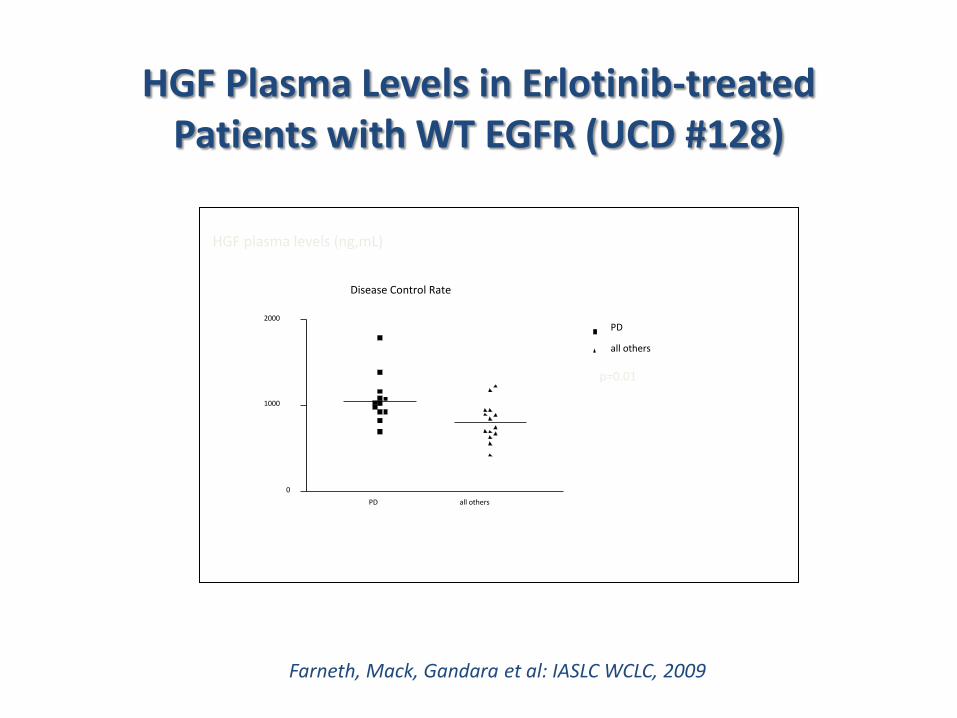
HGF Plasma Levels in Erlotinib-treated Patients with WT EGFR (UCD #128)
HGF plasma levels (ng,mL) p=0.01
Disease Control Rate
PD all others
0
1000
2000 PD
all others
Farneth, Mack, Gandara et al: IASLC WCLC, 2009
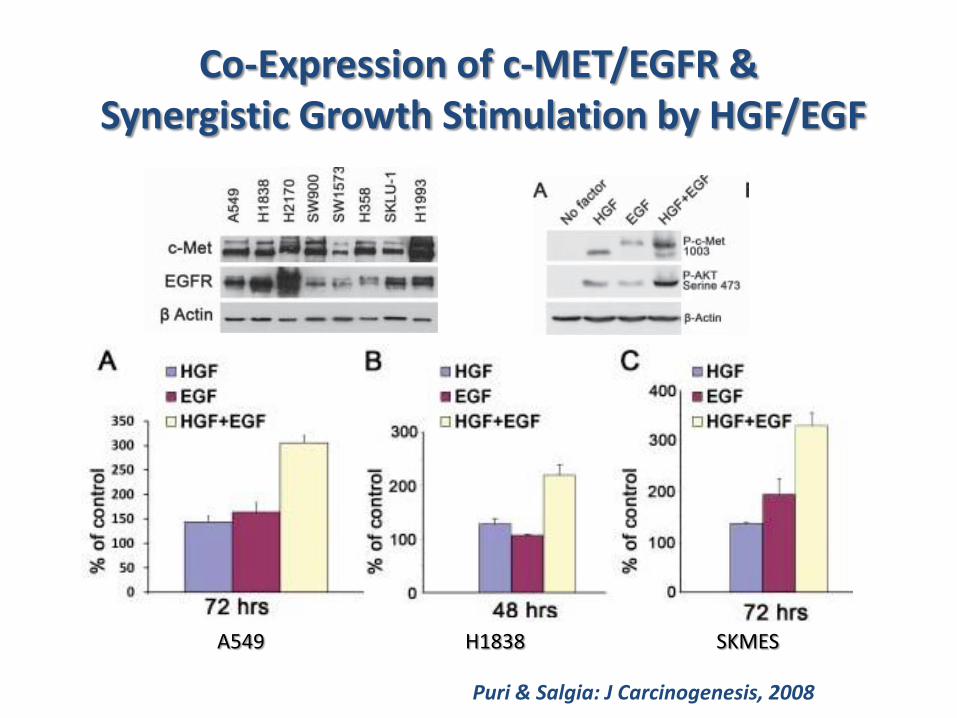
Co-Expression of c-MET/EGFR & Synergistic Growth Stimulation by HGF/EGF
Puri & Salgia: J Carcinogenesis, 2008
A549 H1838 SKMES
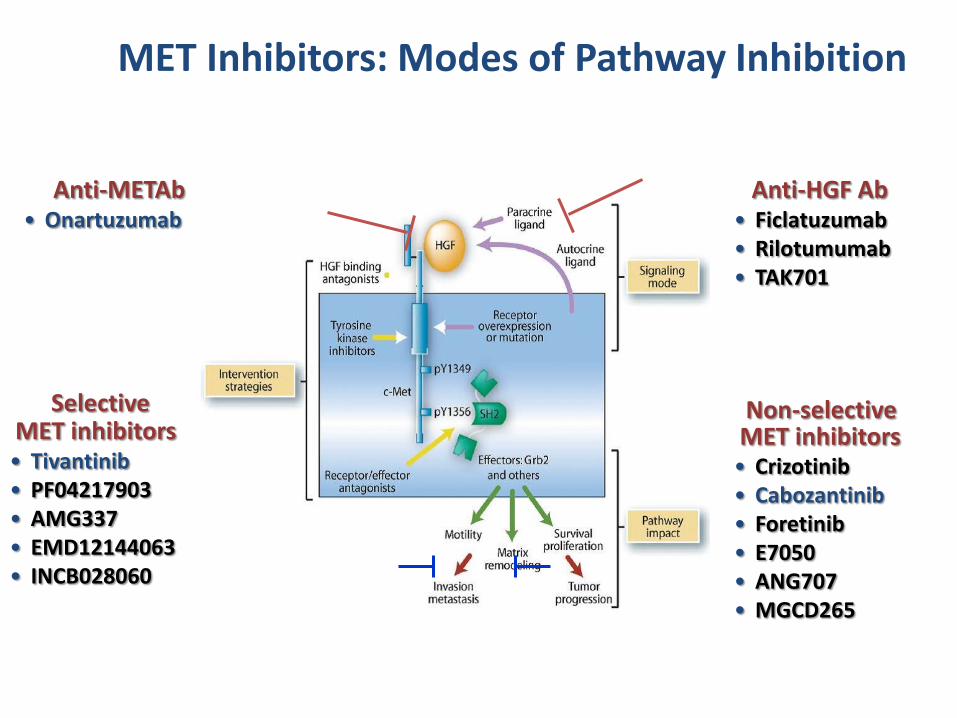
MET Inhibitors: Modes of Pathway Inhibition
Anti-HGF Ab • Ficlatuzumab • Rilotumumab • TAK701
Non-selective MET inhibitors • Crizotinib • Cabozantinib • Foretinib • E7050 • ANG707 • MGCD265
Anti-METAb • Onartuzumab
Selective MET inhibitors • Tivantinib • PF04217903 • AMG337 • EMD12144063 • INCB028060
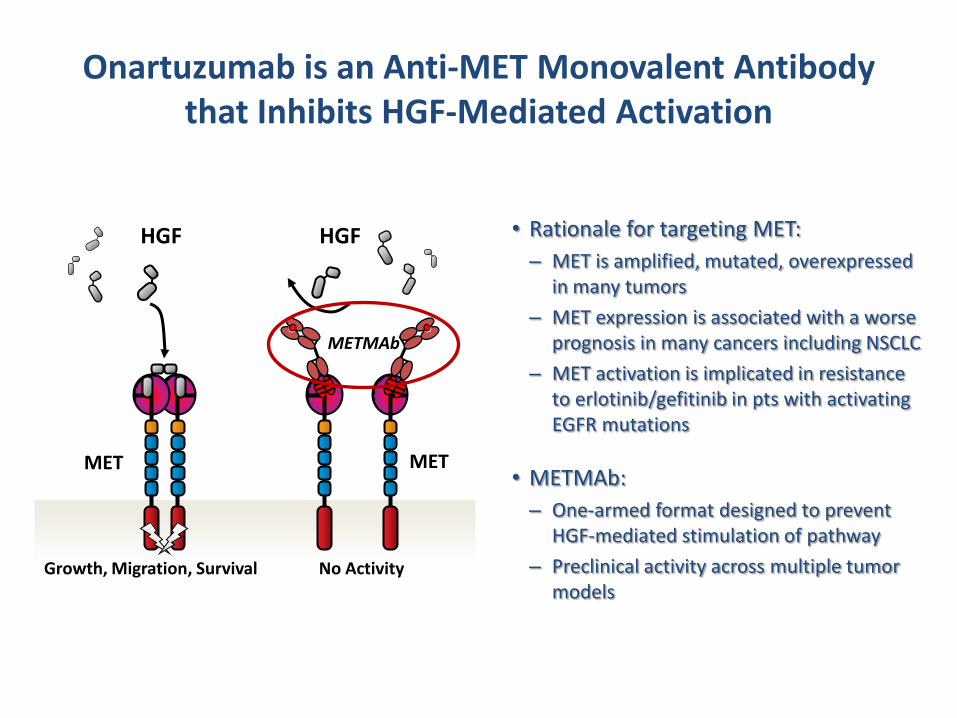
Onartuzumab is an Anti-MET Monovalent Antibody that Inhibits HGF-Mediated Activation
• Rationale for targeting MET:
– MET is amplified, mutated, overexpressed in many tumors
– MET expression is associated with a worse prognosis in many cancers including NSCLC
– MET activation is implicated in resistance to erlotinib/gefitinib in pts with activating EGFR mutations
• METMAb:
– One-armed format designed to prevent HGF-mediated stimulation of pathway
– Preclinical activity across multiple tumor models
METMAb
MET
HGF HGF
MET
Growth, Migration, Survival No Activity
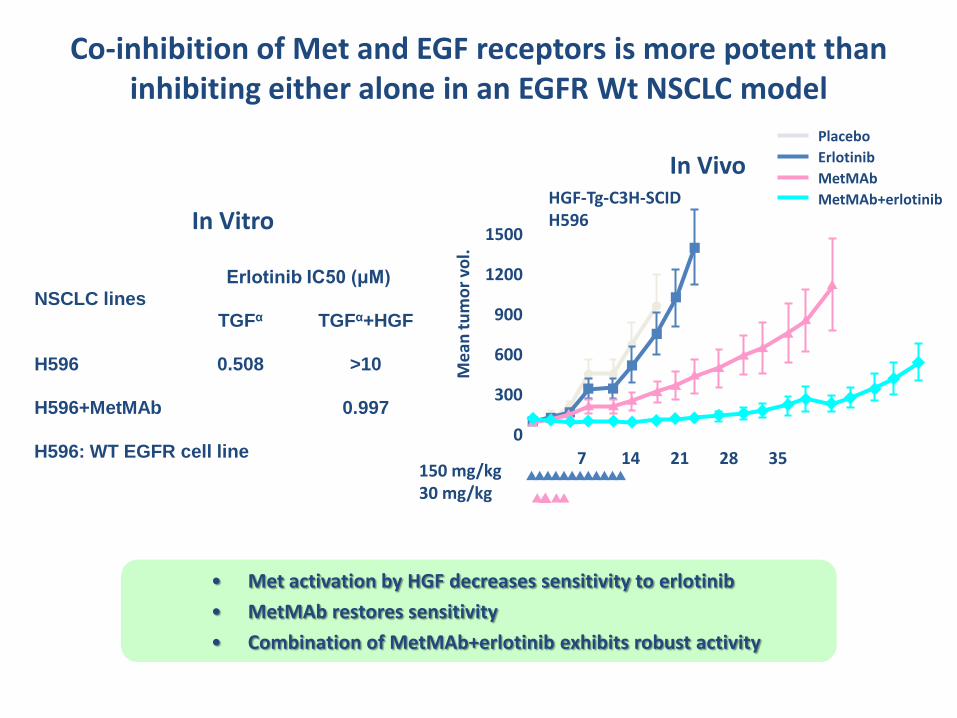
Co-inhibition of Met and EGF receptors is more potent than inhibiting either alone in an EGFR Wt NSCLC model
H596: WT EGFR cell line
In Vivo
In Vitro
NSCLC lines Erlotinib IC50 (μM)
TGFα TGFα+HGF
H596 0.508 >10
H596+MetMAb 0.997
• Met activation by HGF decreases sensitivity to erlotinib
• MetMAb restores sensitivity
• Combination of MetMAb+erlotinib exhibits robust activity
Day
0 14 21 28 35 49 56 63 M
ean
tu
mo
r vo
l.
0
600
900
1200
1500
1800
Placebo
Erlotinib
MetMAb
MetMAb+erlotinib
300
7
HGF-Tg-C3H-SCID H596
150 mg/kg 30 mg/kg
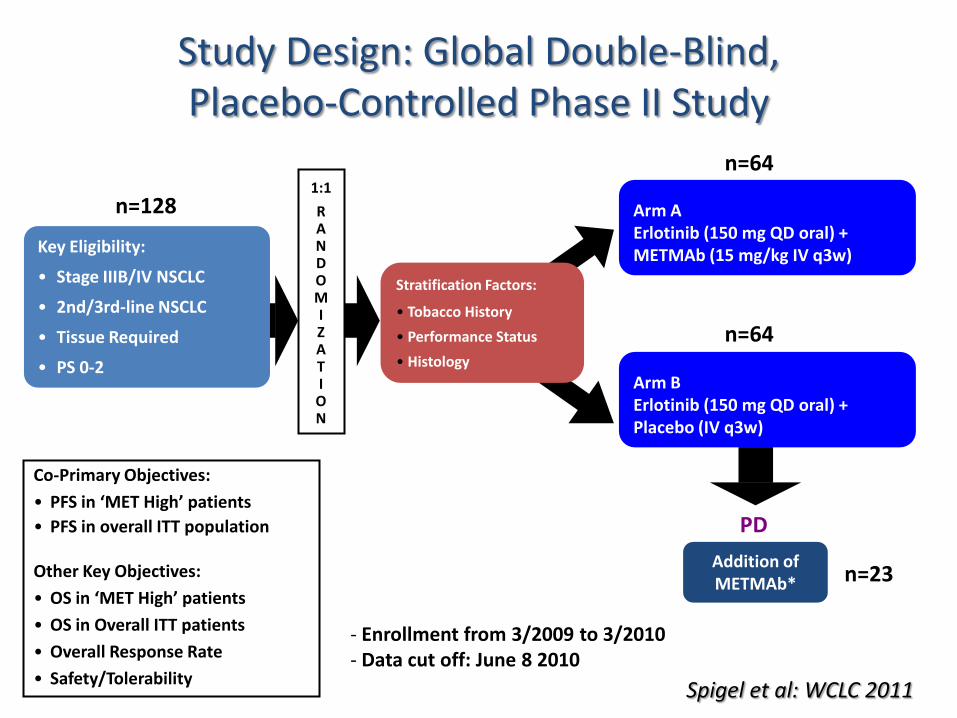
Arm A Erlotinib (150 mg QD oral) + METMAb (15 mg/kg IV q3w)
Addition of METMAb*
PD
*If eligible
Co-Primary Objectives:
• PFS in ‘MET High’ patients
• PFS in overall ITT population
Other Key Objectives:
• OS in ‘MET High’ patients
• OS in Overall ITT patients
• Overall Response Rate
• Safety/Tolerability
Study Design: Global Double-Blind, Placebo-Controlled Phase II Study
Arm B Erlotinib (150 mg QD oral) + Placebo (IV q3w)
Key Eligibility:
• Stage IIIB/IV NSCLC
• 2nd/3rd-line NSCLC
• Tissue Required
• PS 0-2
R A N D O M I Z A T I O N
1:1
n=128
n=64
n=64
n=23
- Enrollment from 3/2009 to 3/2010 - Data cut off: June 8 2010
Stratification Factors:
• Tobacco History
• Performance Status
• Histology
Spigel et al: WCLC 2011
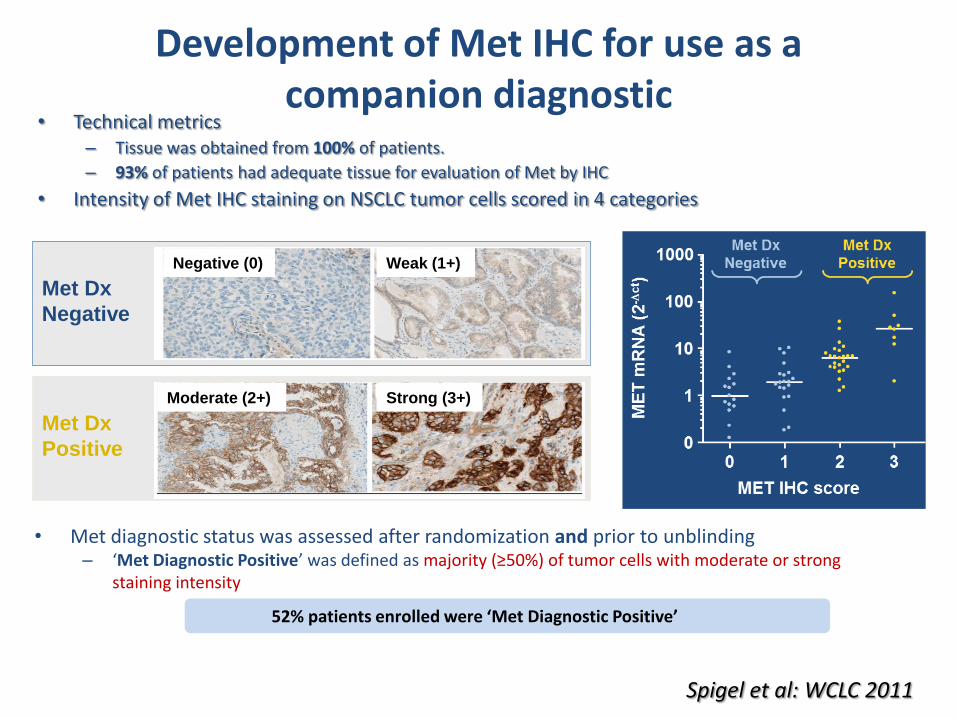
Development of Met IHC for use as a companion diagnostic
• Technical metrics – Tissue was obtained from 100% of patients.
– 93% of patients had adequate tissue for evaluation of Met by IHC
• Intensity of Met IHC staining on NSCLC tumor cells scored in 4 categories
• Met diagnostic status was assessed after randomization and prior to unblinding – ‘Met Diagnostic Positive’ was defined as majority (≥50%) of tumor cells with moderate or strong
staining intensity
Negative (0) Weak (1+)
Moderate (2+) Strong (3+)
Met Dx
Negative
Met Dx
Positive
MET IHC score
52% patients enrolled were ‘Met Diagnostic Positive’
Spigel et al: WCLC 2011
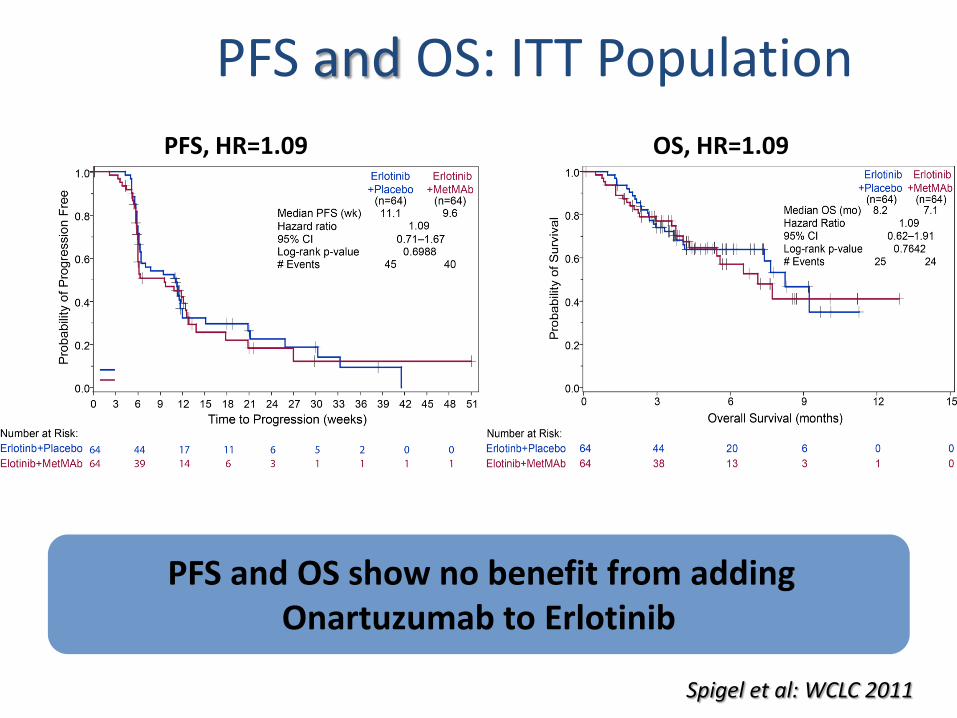
PFS and OS: ITT Population
PFS, HR=1.09 OS, HR=1.09
PFS and OS show no benefit from adding Onartuzumab to Erlotinib
Spigel et al: WCLC 2011
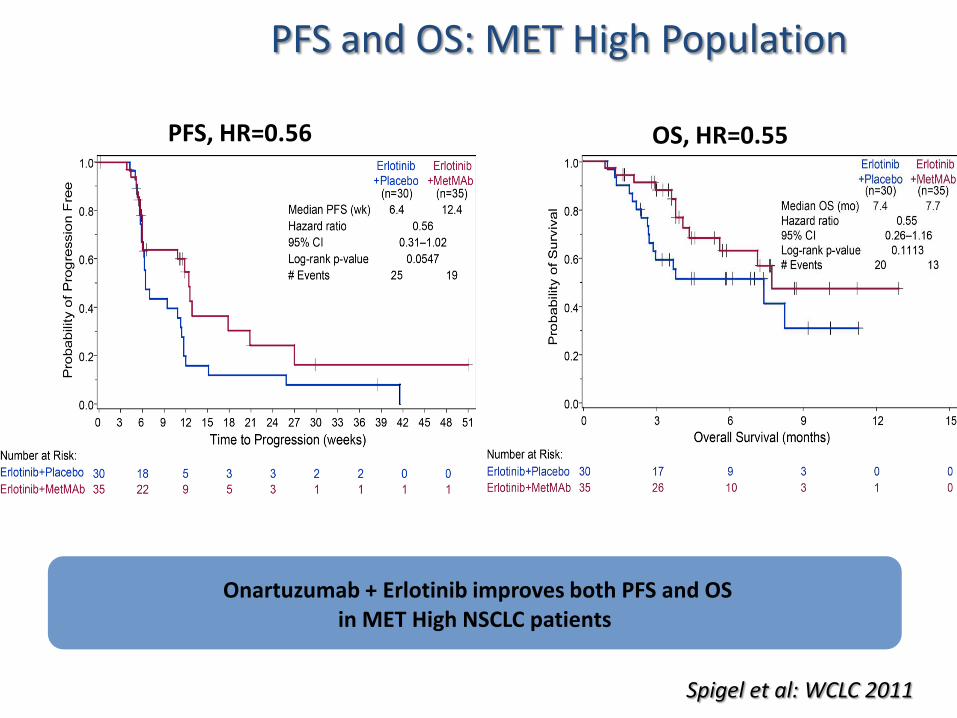
PFS and OS: MET High Population
PFS, HR=0.56 OS, HR=0.55
Onartuzumab + Erlotinib improves both PFS and OS in MET High NSCLC patients
Spigel et al: WCLC 2011
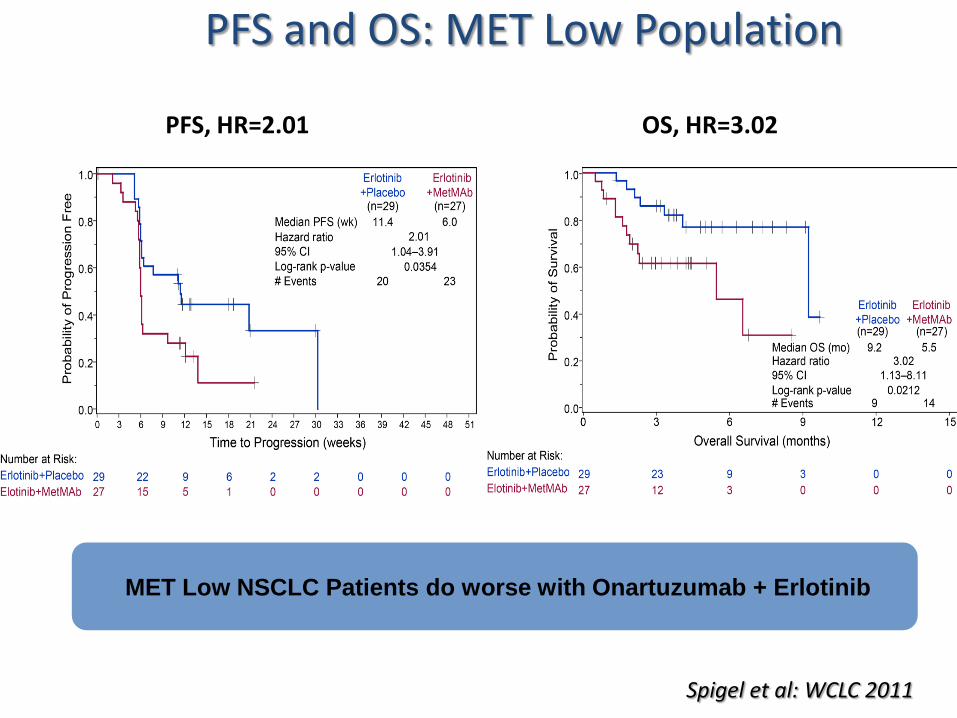
PFS and OS: MET Low Population
PFS, HR=2.01 OS, HR=3.02
MET Low NSCLC Patients do worse with Onartuzumab + Erlotinib
Spigel et al: WCLC 2011
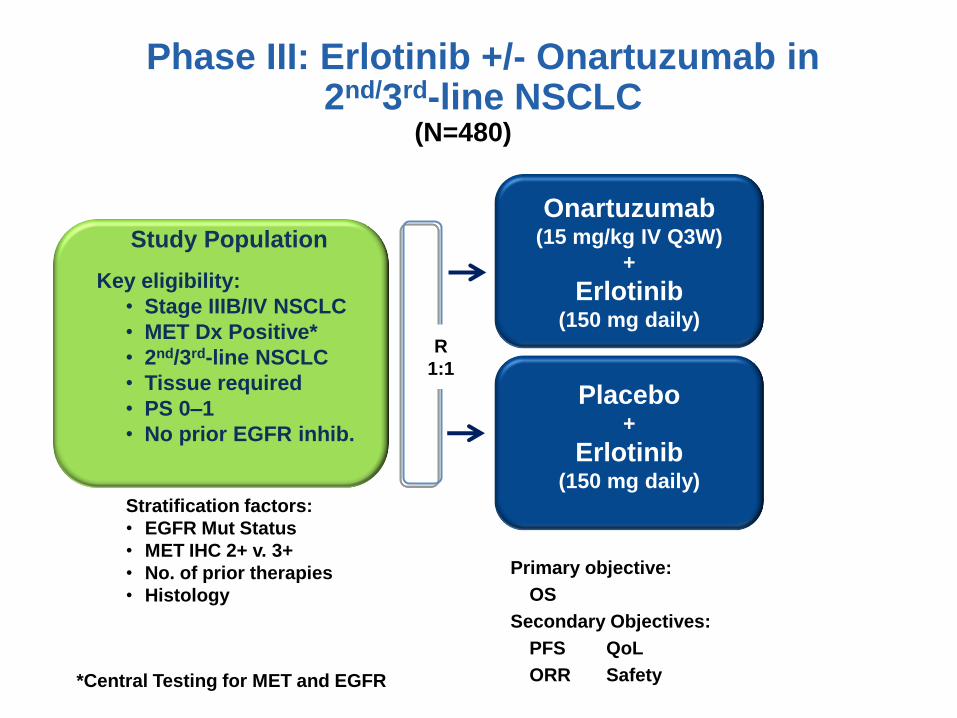
Phase III: Erlotinib +/- Onartuzumab in 2nd/3rd-line NSCLC
16
Placebo +
Erlotinib (150 mg daily)
Onartuzumab
(15 mg/kg IV Q3W)
+
Erlotinib (150 mg daily)
R
1:1
(N=480)
Study Population
Key eligibility:
• Stage IIIB/IV NSCLC
• MET Dx Positive*
• 2nd/3rd-line NSCLC
• Tissue required
• PS 0–1
• No prior EGFR inhib.
Primary objective:
• OS
Secondary Objectives:
PFS QoL
ORR Safety
Stratification factors:
• EGFR Mut Status
• MET IHC 2+ v. 3+
• No. of prior therapies
• Histology
*Central Testing for MET and EGFR
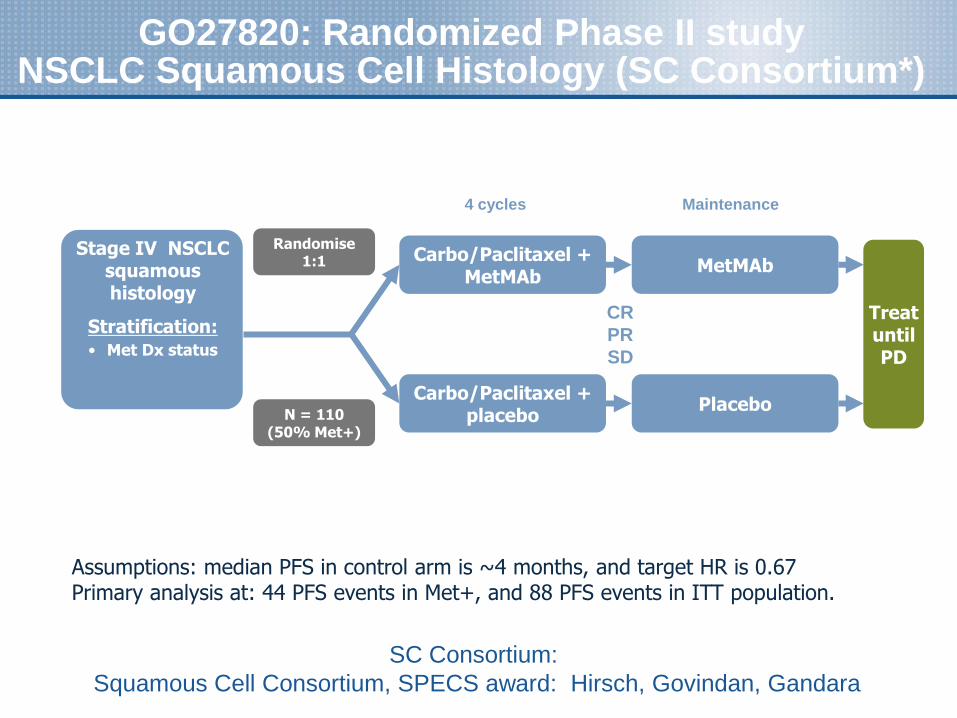
GO27820: Randomized Phase II study NSCLC Squamous Cell Histology (SC Consortium*)
Treat until PD
Carbo/Paclitaxel + MetMAb
Carbo/Paclitaxel + placebo
Randomise 1:1
Stage IV NSCLC squamous histology
Stratification: • Met Dx status
Maintenance
CR
PR
SD
4 cycles
MetMAb
Placebo N = 110
(50% Met+)
Assumptions: median PFS in control arm is ~4 months, and target HR is 0.67 Primary analysis at: 44 PFS events in Met+, and 88 PFS events in ITT population.
SC Consortium:
Squamous Cell Consortium, SPECS award: Hirsch, Govindan, Gandara
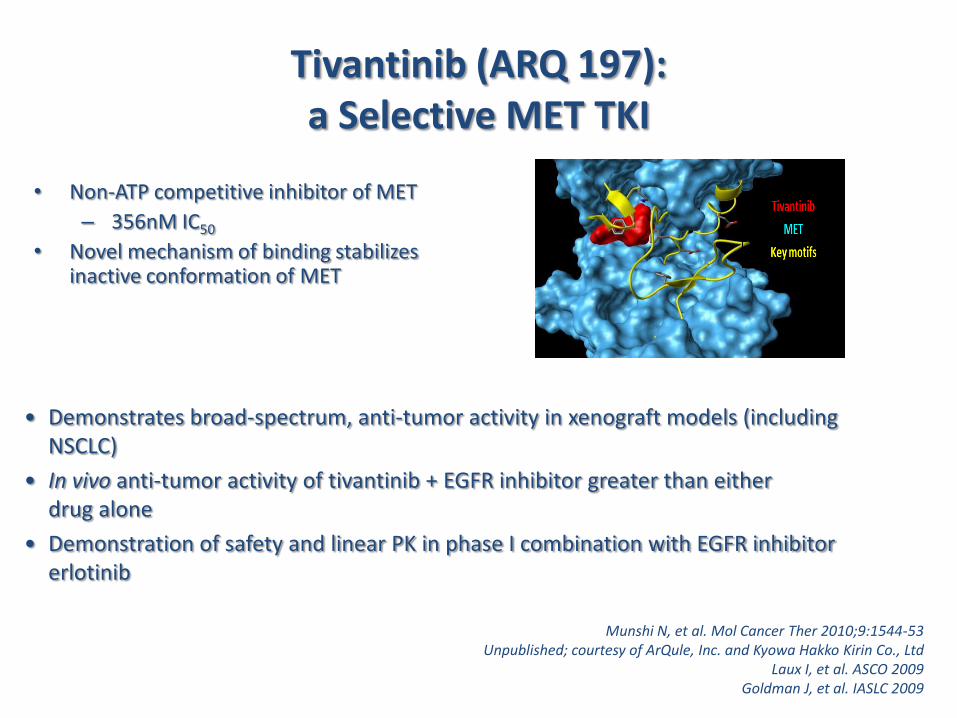
Tivantinib (ARQ 197): a Selective MET TKI
• Non-ATP competitive inhibitor of MET
– 356nM IC50
• Novel mechanism of binding stabilizes inactive conformation of MET
• Demonstrates broad-spectrum, anti-tumor activity in xenograft models (including NSCLC)
• In vivo anti-tumor activity of tivantinib + EGFR inhibitor greater than either drug alone
• Demonstration of safety and linear PK in phase I combination with EGFR inhibitor erlotinib
Munshi N, et al. Mol Cancer Ther 2010;9:1544-53 Unpublished; courtesy of ArQule, Inc. and Kyowa Hakko Kirin Co., Ltd
Laux I, et al. ASCO 2009 Goldman J, et al. IASLC 2009
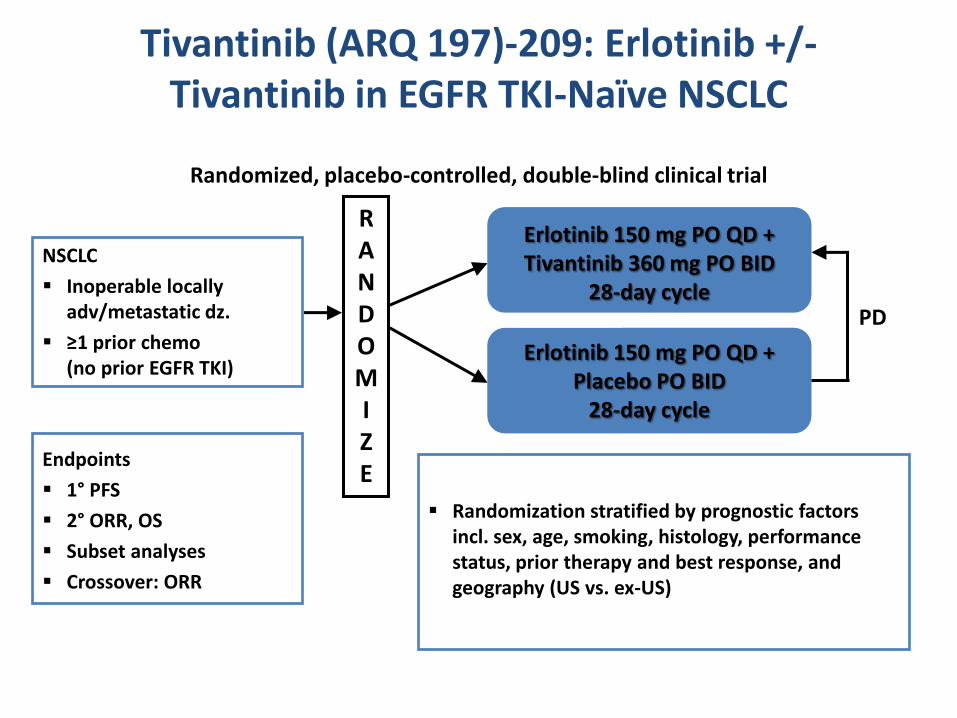
Tivantinib (ARQ 197)-209: Erlotinib +/- Tivantinib in EGFR TKI-Naïve NSCLC
Randomized, placebo-controlled, double-blind clinical trial
NSCLC
Inoperable locally adv/metastatic dz.
≥1 prior chemo (no prior EGFR TKI)
Endpoints
1° PFS
2° ORR, OS
Subset analyses
Crossover: ORR
R A N D O M I Z E
Randomization stratified by prognostic factors incl. sex, age, smoking, histology, performance status, prior therapy and best response, and geography (US vs. ex-US)
Erlotinib 150 mg PO QD + Tivantinib 360 mg PO BID
28-day cycle
Erlotinib 150 mg PO QD + Placebo PO BID
28-day cycle
PD
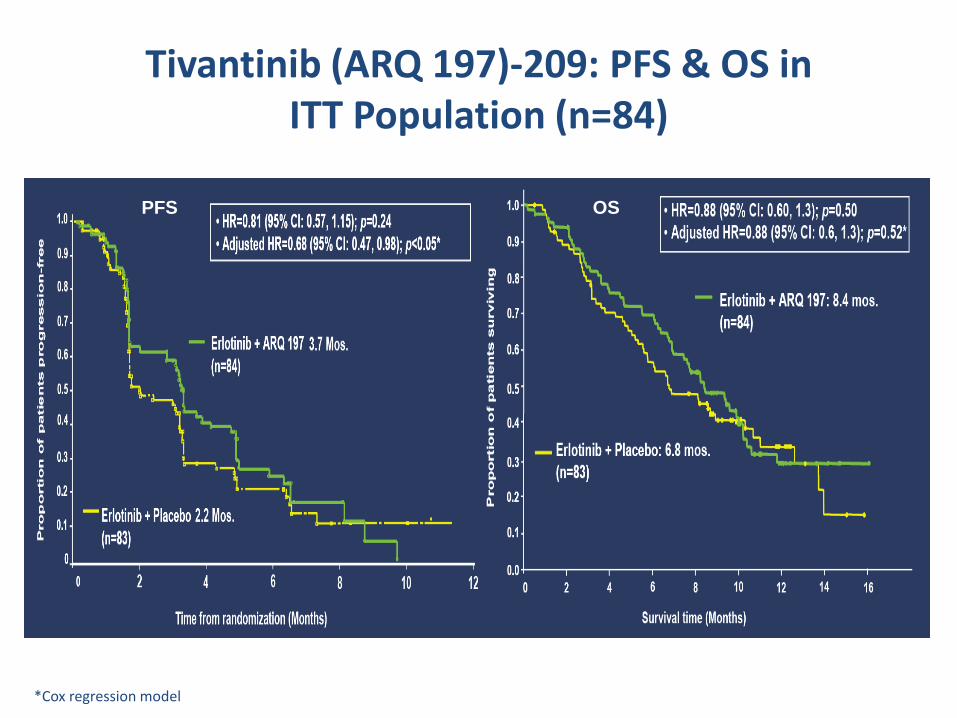
Tivantinib (ARQ 197)-209: PFS & OS in ITT Population (n=84)
*Cox regression model
PFS OS
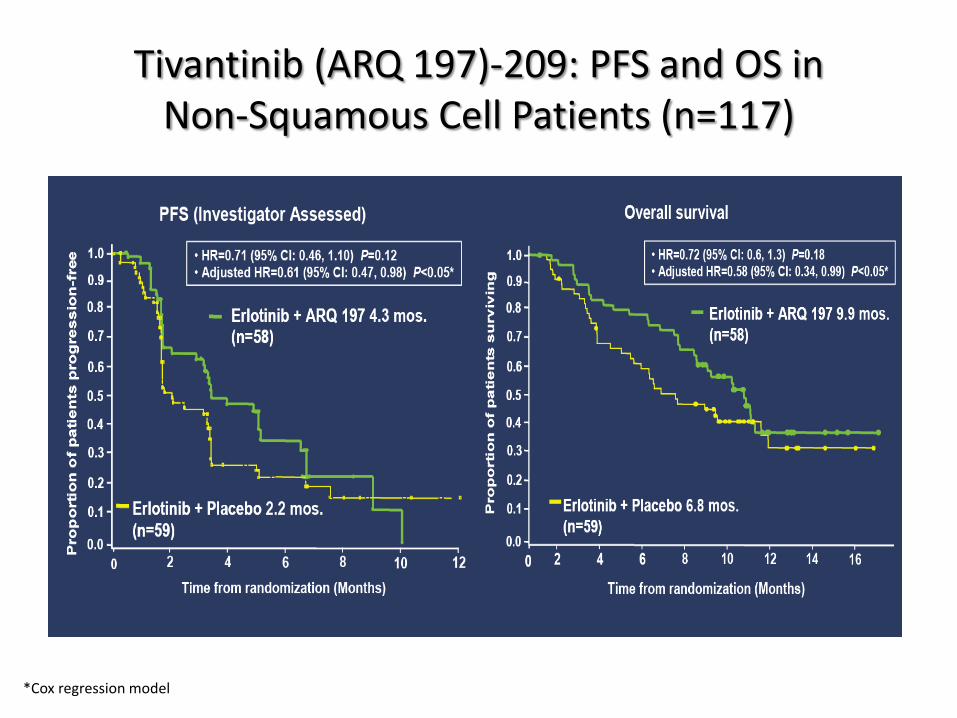
Tivantinib (ARQ 197)-209: PFS and OS in Non-Squamous Cell Patients (n=117)
*Cox regression model
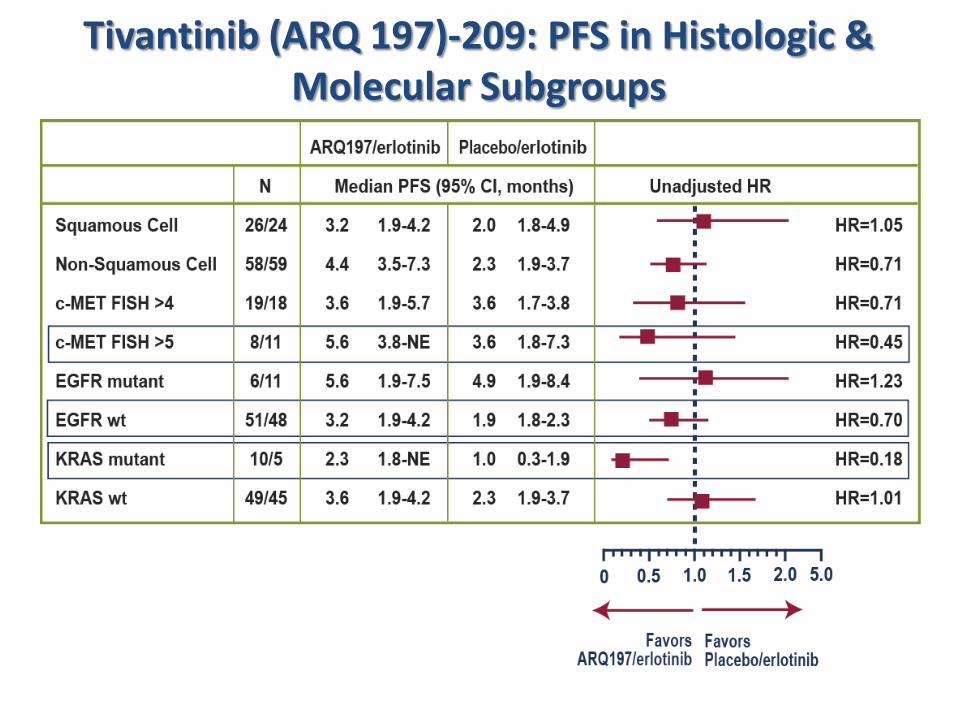
Tivantinib (ARQ 197)-209: PFS in Histologic & Molecular Subgroups
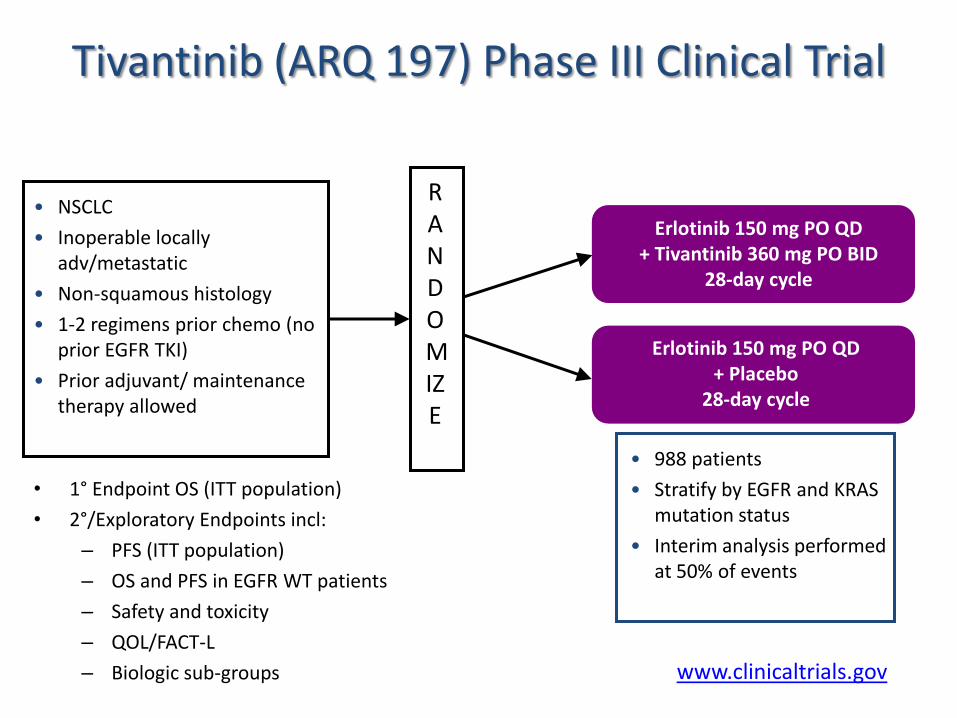
Tivantinib (ARQ 197) Phase III Clinical Trial
• 1° Endpoint OS (ITT population)
• 2°/Exploratory Endpoints incl:
– PFS (ITT population)
– OS and PFS in EGFR WT patients
– Safety and toxicity
– QOL/FACT-L
– Biologic sub-groups
• NSCLC
• Inoperable locally adv/metastatic
• Non-squamous histology
• 1-2 regimens prior chemo (no prior EGFR TKI)
• Prior adjuvant/ maintenance therapy allowed
RANDOMIZE
• 988 patients
• Stratify by EGFR and KRAS mutation status
• Interim analysis performed at 50% of events
Erlotinib 150 mg PO QD + Tivantinib 360 mg PO BID
28-day cycle
Erlotinib 150 mg PO QD + Placebo
28-day cycle
www.clinicaltrials.gov
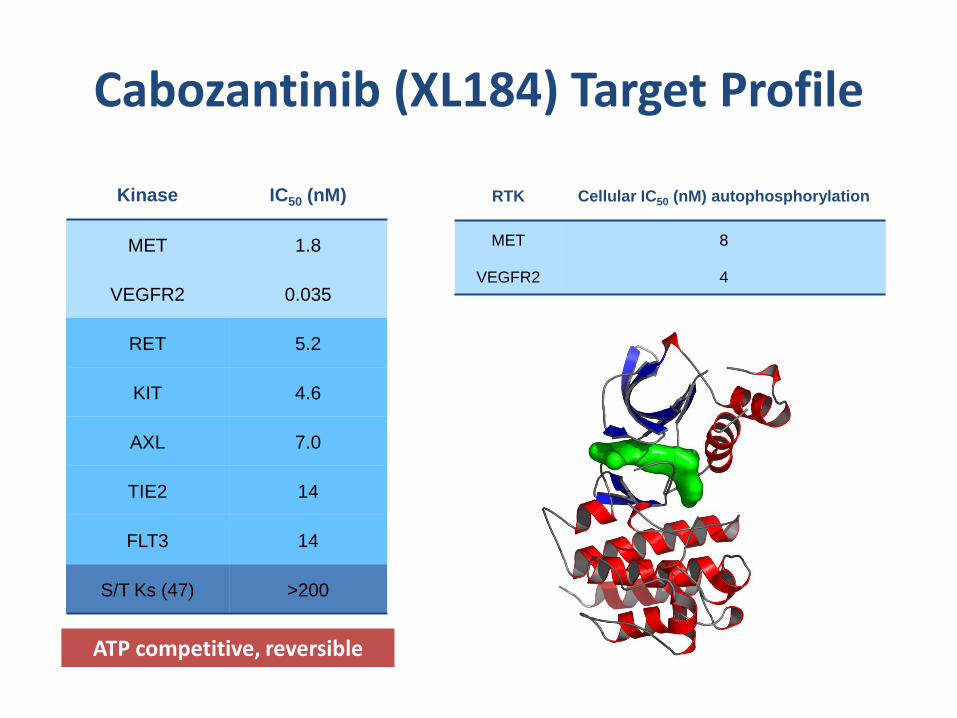
Cabozantinib (XL184) Target Profile
ATP competitive, reversible
RTK Cellular IC50 (nM) autophosphorylation
MET 8
VEGFR2 4
Kinase IC50 (nM)
MET 1.8
VEGFR2 0.035
RET 5.2
KIT 4.6
AXL 7.0
TIE2 14
FLT3 14
S/T Ks (47) >200
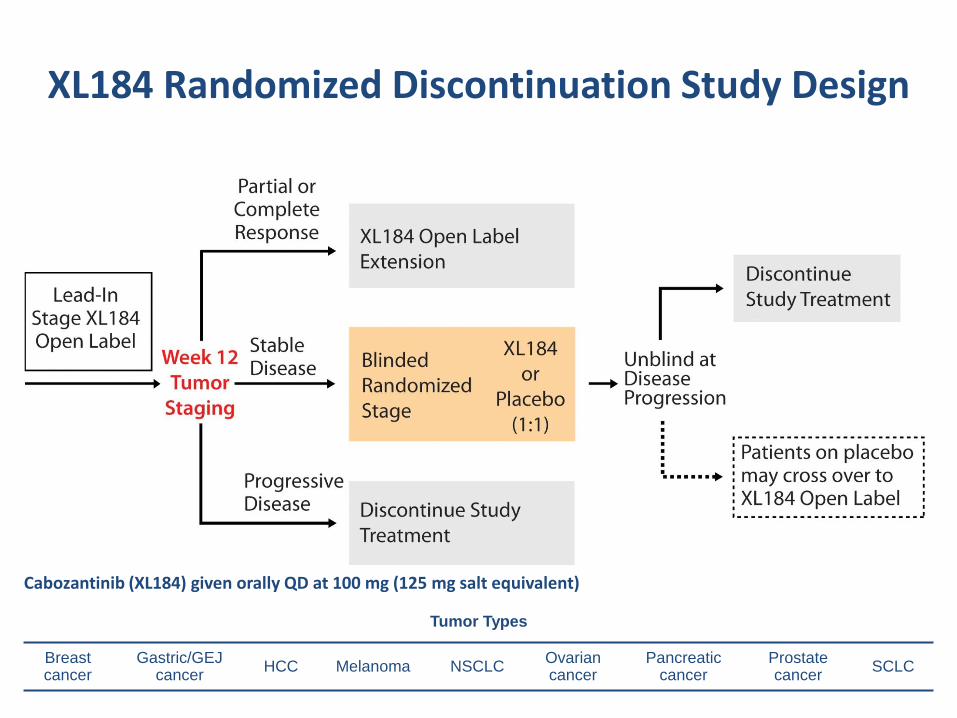
XL184 Randomized Discontinuation Study Design
Tumor Types
Breast cancer
Gastric/GEJ cancer
HCC Melanoma NSCLC Ovarian cancer
Pancreatic cancer
Prostate cancer
SCLC
Cabozantinib (XL184) given orally QD at 100 mg (125 mg salt equivalent)
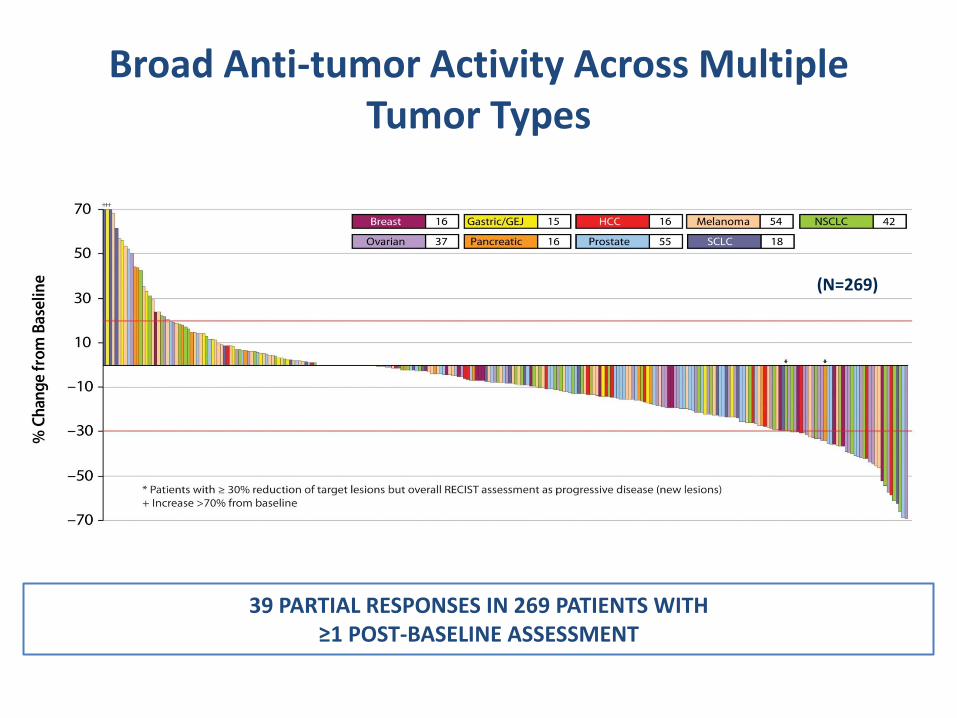
Broad Anti-tumor Activity Across Multiple Tumor Types
Effects in bone
(N=269)
39 PARTIAL RESPONSES IN 269 PATIENTS WITH ≥1 POST-BASELINE ASSESSMENT
Interim RDT data presented at 2010 EORTC-NCI-AACR Symposium
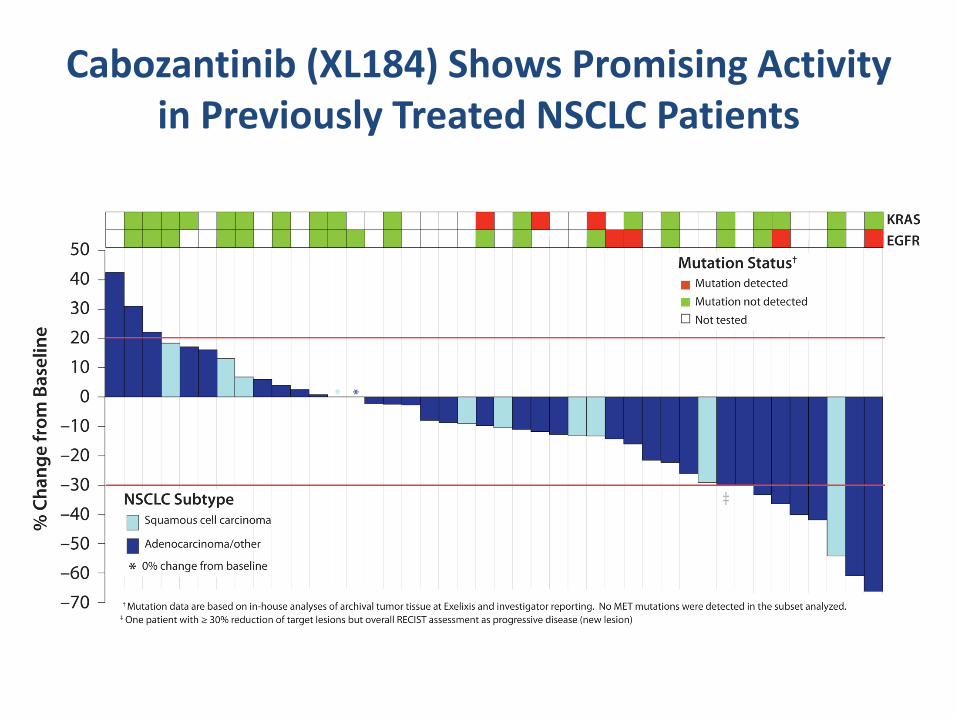
Cabozantinib (XL184) Shows Promising Activity in Previously Treated NSCLC Patients
Best Radiologic Time Point Response of Patients with >1 Post-baseline Tumor Assessment
Interim RDT data presented at 2010 EORTC-NCI-AACR Symposium
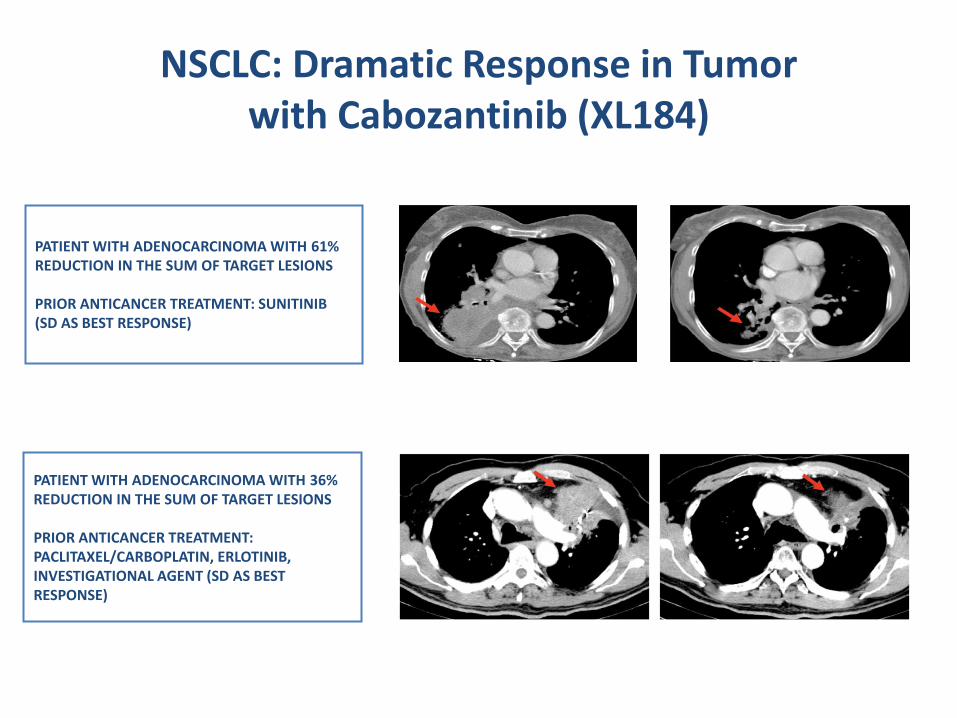
NSCLC: Dramatic Response in Tumor with Cabozantinib (XL184)
Radiographic Images from a 72-Year-Old Male with Metastatic NSCLC
Radiographic Images from a 88-Year-Old Female with Metastatic NSCLC
PATIENT WITH ADENOCARCINOMA WITH 61% REDUCTION IN THE SUM OF TARGET LESIONS PRIOR ANTICANCER TREATMENT: SUNITINIB (SD AS BEST RESPONSE)
PATIENT WITH ADENOCARCINOMA WITH 36% REDUCTION IN THE SUM OF TARGET LESIONS PRIOR ANTICANCER TREATMENT: PACLITAXEL/CARBOPLATIN, ERLOTINIB, INVESTIGATIONAL AGENT (SD AS BEST RESPONSE)
Screening Week 12
Screening Week 12
Interim RDT data presented at 2010 EORTC-NCI-AACR Symposium
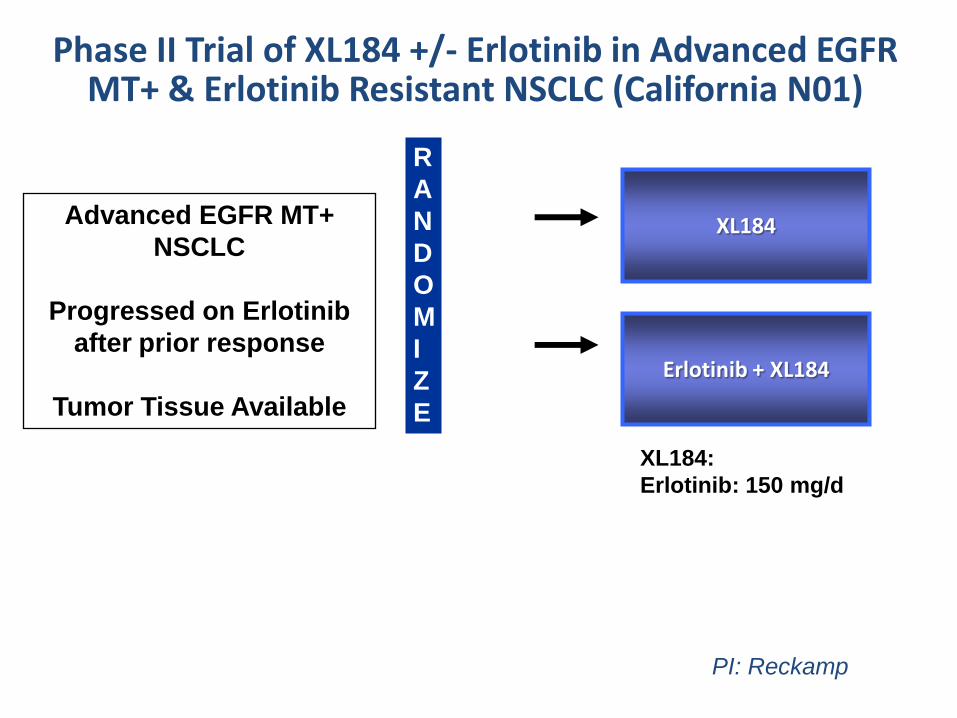
Phase II Trial of XL184 +/- Erlotinib in Advanced EGFR MT+ & Erlotinib Resistant NSCLC (California N01)
R
A
N
D
O
M
I
Z
E
XL184 Advanced EGFR MT+
NSCLC
Progressed on Erlotinib
after prior response
Tumor Tissue Available
PI: Reckamp
Erlotinib + XL184
XL184:
Erlotinib: 150 mg/d
Summary and Conclusions
HGF & MET are good targets for cancer therapy:
• MET is (over)expressed in multiple tumor types
• HGF & MET control multiple biologic functions of cancer cells including proliferation, survival, and angiogenesis
• MET activation confers resistance to chemo- & radiotherapy
• HGF & MET mediate resistance to target therapies against other receptors including EGFR and VEGFR
• Targeted agents against METPredictive biomarkers need to be defined
• Rational Combinations are being explored







