Empowering Pharmacists asDiabetes Medication Experts
and Educators
In Collaboration with
Objectives
• Quantify the burden of suboptimal management of patients with type 2 diabetes mellitus (T2DM), including rehospitalization, hyperglycemia, and hypoglycemia
• Outline the safety, efficacy, and evidence-based role of newer agents, including incretin-based therapy and sodium glucose cotransporter-2 (SGLT-2) inhibitors in the management of T2DM
• Apply current guidelines and evidence to the review and adjustment of medication regimens in poorly controlled T2DM patients on admission and discharge
• Outline the role of health-system pharmacists as diabetes educators and discuss approaches to optimizing patient counseling
It Is Estimated That…
• 1 in 3 babies born in 2012 will live to 100 years of age
• 1 in 3 babies born in 2000 will develop diabetes
– 2 out of 3 in high-risk ethnic groups
• Therefore, the need for diabetes prevention and education is imperative
– ALL healthcare professionals are needed
Christensen K, et al. Lancet. 2009;374(9696):1196-1208. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/diabetes/news/docs/lifetime.htm. Updated March 12, 2010. Accessed February 23, 2014.
Need for Improved Glycemic Control in the United States
• Glycemic targets must be individualized
• The ADA recommends an A1C of <7% as a reasonable goal for many nonpregnant adults
• Many US adults with diagnosed diabetes do not have an A1C of <7%
ADA = American Diabetes Association.Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379. American Diabetes Association. Diabetes Care. 2013;36(Suppl 11):S11-S66. Cheung BMY, et al. Am J Med. 2009;122:443-453.
Percentage of US Adultswith Diagnosed Diabetes
and AIC <7%70
50
40
30
20
0
10
Pe
rce
nt
(%)
57.1
61.9
44.240.6
Overall
53.960
WhiteNon-
Hispanic
BlackNon-
Hispanic
MexicanAmerican
Other
Suboptimal Glycemic Control Resultsin Hospitalizations
• Individuals with suboptimal glycemic control are at risk for short-term complications that often require hospitalization
• The overall rate of admission for US adults with short-term complications is increasing
*2006 data not available.Agency for Healthcare Research and Quality. National Healthcare Quality Report, 2011. 2012.
70
60
55
50
45
30
35
Ra
te p
er
10
0,0
00
Pe
op
le
Hospital Admissions forShort-Term Complications*
2004
65
2005 2007 2008
Achievable Benchmark
All Patients
40
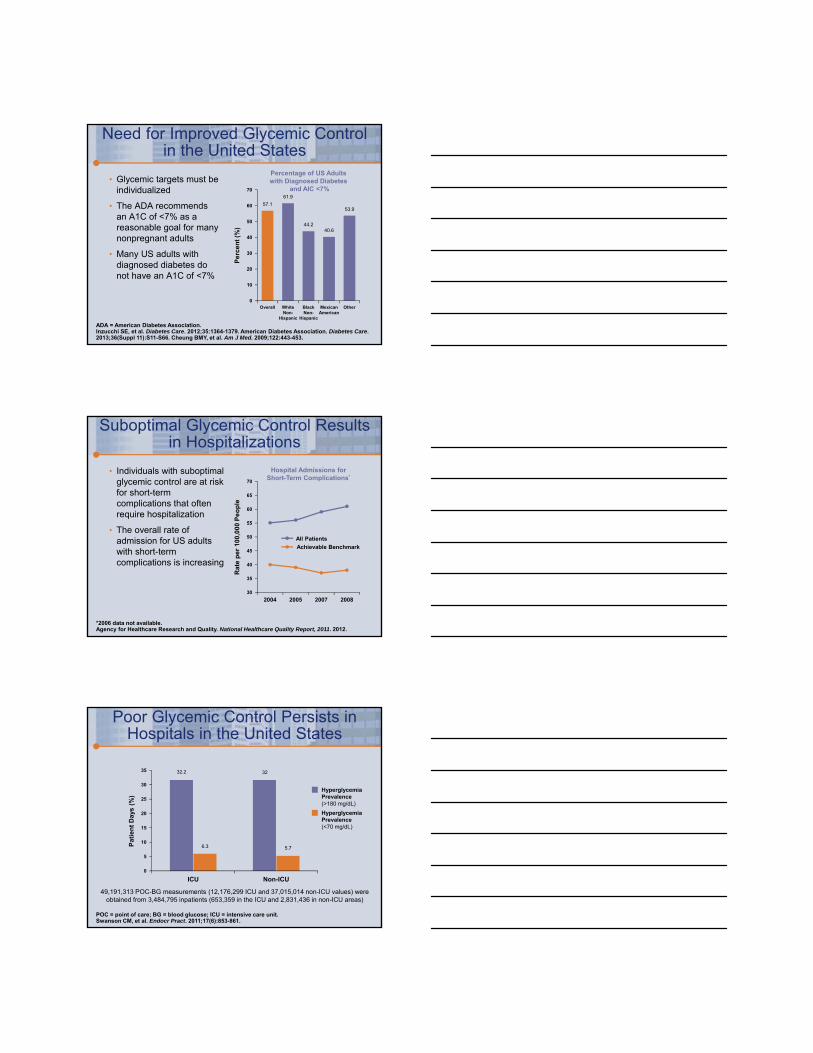
Poor Glycemic Control Persists in Hospitals in the United States
49,191,313 POC-BG measurements (12,176,299 ICU and 37,015,014 non-ICU values) were obtained from 3,484,795 inpatients (653,359 in the ICU and 2,831,436 in non-ICU areas)
POC = point of care; BG = blood glucose; ICU = intensive care unit.Swanson CM, et al. Endocr Pract. 2011;17(6):853-861.
25
15
35
5
0
Pa
tie
nt
Da
ys (
%)
ICU Non-ICU
32.2
6.3
32
5.7
30
20
10
HyperglycemiaPrevalence(<70 mg/dL)
HyperglycemiaPrevalence(>180 mg/dL)
2014 Standards of Medical Care in Diabetes: Revisions (Hospital Specific)
• IX: Diabetes care in the hospital
– Discharge planning should start at admission
• Clear diabetes management instructions provided
– Elimination of the sole use of sliding scale in the inpatient hospital setting
– All diabetes patients have “diabetes” clearly identified in the EMR
– Order for blood glucose monitoring and goals
– Obtain A1C in patients with risk factors for undiagnosed diabetes with hyperglycemia in hospital
American Diabetes Association. Diabetes Care. 2014;37:(Suppl 1):S14-S80.
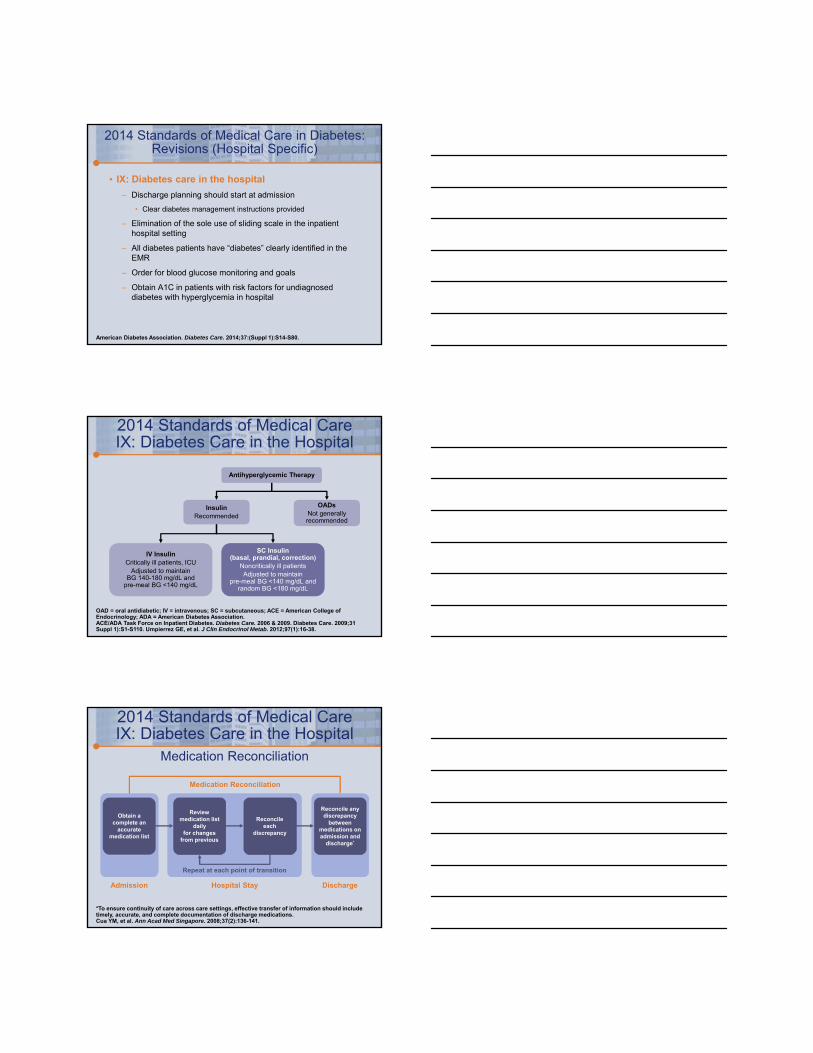
OAD = oral antidiabetic; IV = intravenous; SC = subcutaneous; ACE = American College of Endocrinology; ADA = American Diabetes Association. ACE/ADA Task Force on Inpatient Diabetes. Diabetes Care. 2006 & 2009. Diabetes Care. 2009;31Suppl 1):S1-S110. Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97(1):16-38.
IV InsulinCritically ill patients, ICU
Adjusted to maintain BG 140-180 mg/dL and
pre-meal BG <140 mg/dL
SC Insulin(basal, prandial, correction)
Noncritically ill patientsAdjusted to maintain
pre-meal BG <140 mg/dL andrandom BG <180 mg/dL
2014 Standards of Medical CareIX: Diabetes Care in the Hospital
OADs Not generallyrecommended
Insulin Recommended
Antihyperglycemic Therapy
Medication Reconciliation
Obtain a complete an
accurate medication list
Review medication list
dailyfor changes
from previous
Reconcileeach
discrepancy
Reconcile any discrepancy
between medications on admission and
discharge*
Hospital Stay DischargeAdmission
Repeat at each point of transition
2014 Standards of Medical CareIX: Diabetes Care in the Hospital
*To ensure continuity of care across care settings, effective transfer of information should include timely, accurate, and complete documentation of discharge medications.Cua YM, et al. Ann Acad Med Singapore. 2008;37(2):136-141.
Medication Reconciliation

Medication-Related Patient Care Concerns
• Medication errors cause at least one death every day and injure approximately 1.3 million people annually (United States)
• Delays in treatment and medication nonadherence are the major reasons behind avoidable costs in the healthcare system
– Avoidable costs >$200 billion are incurred each year in the US healthcare system, representing 8% of the country’s total annual healthcare expenditures
• Significant cost to patients
• Unnecessary utilization of healthcare resources
• $400 million hospital visits (annually)
Medication error reports. Food and Drug Administration Web site. http://www.fda.gov/Drugs/ DrugSafety/MedicationErrors/ucm080629.htm. Updated March 5, 2009. Accessed February 28, 2014. Identify those who need adherence help. Modern Medicine Web site. http://managedhealthcareexecutive.modernmedicine.com/managed-healthcare-executive/news/ identify-those-who-need-adherence-help. Published July 15, 2013. Accessed February 28, 2014.
Clinical Inertia
• Delays in evidence-based treatment to patients
– > $40 billion per year in avoidable costs
• Diabetes is the largest avoidable impact to the US healthcare system
– Delays increased outpatient visits and hospitalizations
• Keys to adherence:
– Identifying patients with chronic conditions
– Creating a program that focuses on patients engagement
Identify those who need adherence help. Modern Medicine Web site. http://managedhealthcareexecutive.modernmedicine.com/managed-healthcare-executive/news/ identify-those-who-need-adherence-help. Published July 15, 2013. Accessed February 28, 2014.
Time Since Diabetes DiagnosisIs Key in Adherence
• Less adherent:
– Newly diagnosed T2DM patients
• Possibly due to lack of routine
– Fewer medications
• More adherent:
– Patients with long-standing T2DM
– More medications
– Older
MedPage Today. Time Since Diabetes Dx Key in Adherence. http://www.medpagetoday.com/ MeetingCoverage/ADA/40092. Accessed February 27, 2014.
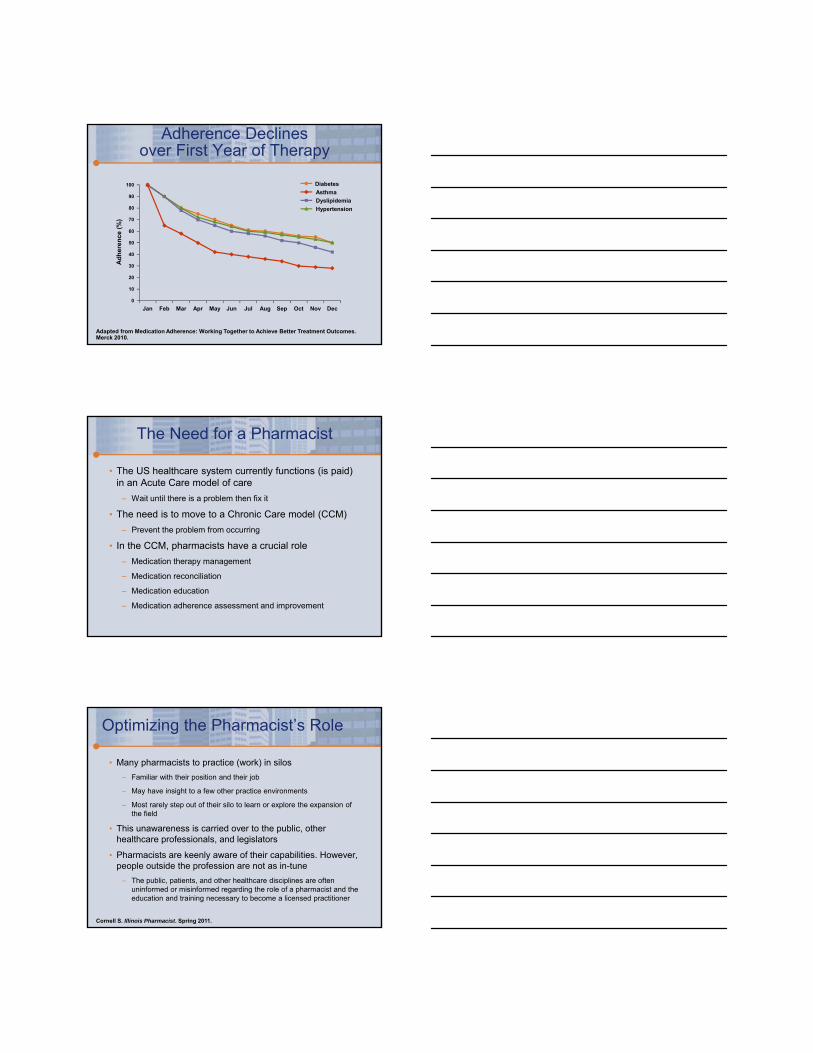
Adherence Declinesover First Year of Therapy
Adapted from Medication Adherence: Working Together to Achieve Better Treatment Outcomes. Merck 2010.
80
70
100
90
60
50
40
30
20
0
10
Feb
Ad
he
ren
ce
(%
)
Asthma
Dyslipidemia
Diabetes
Hypertension
Jan AprMar JunMay AugJul OctSep DecNov
The Need for a Pharmacist
• The US healthcare system currently functions (is paid) in an Acute Care model of care
– Wait until there is a problem then fix it
• The need is to move to a Chronic Care model (CCM)
– Prevent the problem from occurring
• In the CCM, pharmacists have a crucial role
– Medication therapy management
– Medication reconciliation
– Medication education
– Medication adherence assessment and improvement
Optimizing the Pharmacist’s Role
• Many pharmacists to practice (work) in silos
– Familiar with their position and their job
– May have insight to a few other practice environments
– Most rarely step out of their silo to learn or explore the expansion of the field
• This unawareness is carried over to the public, other healthcare professionals, and legislators
• Pharmacists are keenly aware of their capabilities. However, people outside the profession are not as in-tune
– The public, patients, and other healthcare disciplines are often uninformed or misinformed regarding the role of a pharmacist and the education and training necessary to become a licensed practitioner
Cornell S. Illinois Pharmacist. Spring 2011.
Patients at Risk for Readmission
• Inpatient diabetes education seems to reduce readmissions
– Complex diabetes patients vulnerable to multiple complications
• Retrospective study – 30-day analysis
– 2265 patients with type 1 and type 2
– A1C >9%
– 43% received inpatient diabetes education
• Result
– 34% reduction in readmission at 30 days
ADA 2013 Scientific Sessions.
Transition to Outpatient Status
• Begin discharge planning early
• Stabilize BG prior to discharge
• Obtain A1C for discharge planning if the result is not available from the previous 2 to 3 months
– A1C can now be used as a means to make the diagnosis of diabetes
Moghissi ES, et al. Endocr Pract. 2009;15(4):353-369.
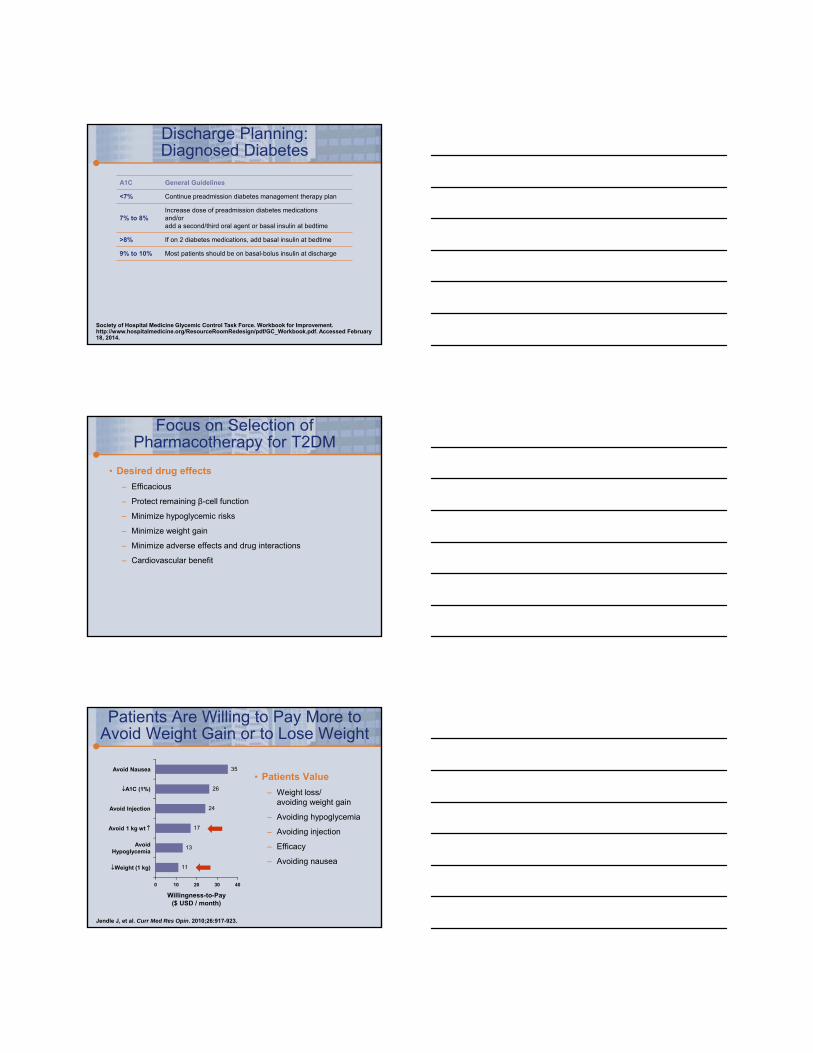
Discharge Planning: New Hyperglycemia
A1C General Guidelines
<5.2% Patient does not have diabetes nor prediabetes
5.2% to 6%Patient has prediabetes (at risk); repeat screening and follow-up advisable; consider diabetes prevention strategies
6.1% to 7%Patient will likely be diagnosed with diabetes in near future; can be treated with lifestyle modifications; discharge on a diabetic diet
7.1% to 9%Patient will likely be diagnosed with diabetes in the future; treat with diet, exercise, and/or a low dose oral agent
>9%Most patients would likely benefit from basal-bolus insulin regimen at discharge
Society of Hospital Medicine Glycemic Control Task Force. Workbook for Improvement.http://www.hospitalmedicine.org/ResourceRoomRedesign/pdf/GC_Workbook.pdf. Accessed February 27, 2014.
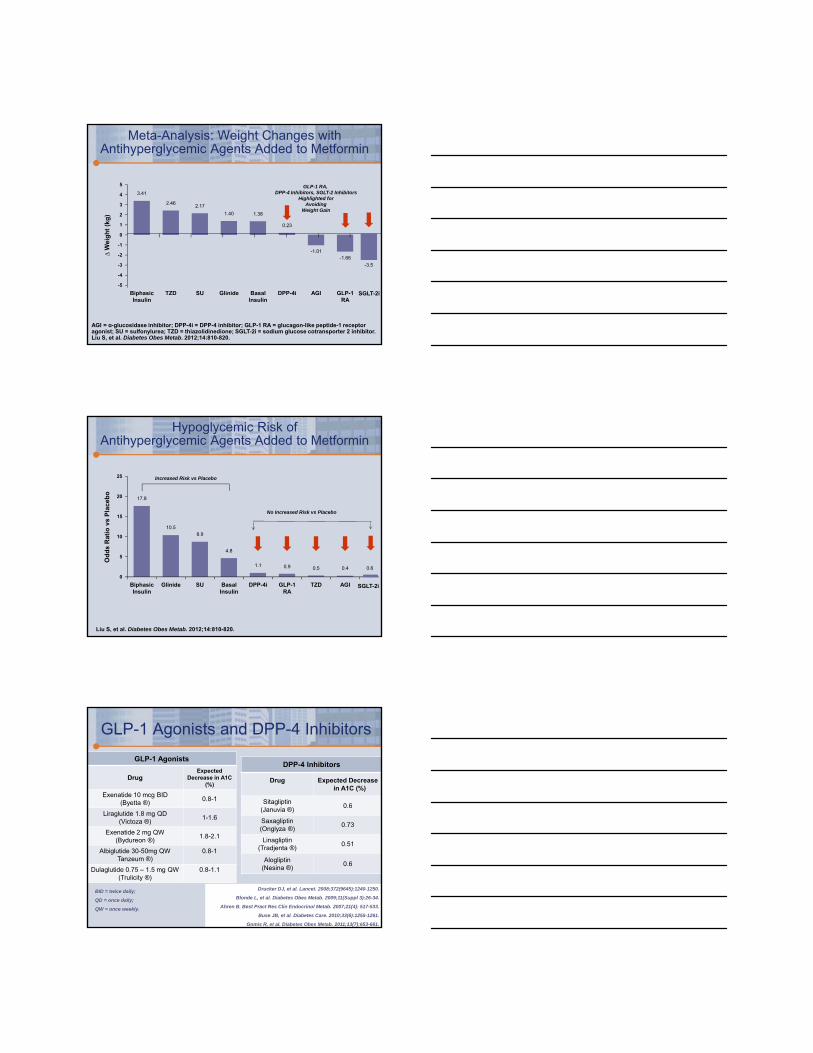
Discharge Planning: Diagnosed Diabetes
A1C General Guidelines
<7% Continue preadmission diabetes management therapy plan
7% to 8%Increase dose of preadmission diabetes medications and/oradd a second/third oral agent or basal insulin at bedtime
>8% If on 2 diabetes medications, add basal insulin at bedtime
9% to 10% Most patients should be on basal-bolus insulin at discharge
Society of Hospital Medicine Glycemic Control Task Force. Workbook for Improvement.http://www.hospitalmedicine.org/ResourceRoomRedesign/pdf/GC_Workbook.pdf. Accessed February 18, 2014.
Focus on Selection of Pharmacotherapy for T2DM
• Desired drug effects
– Efficacious
– Protect remaining β-cell function
– Minimize hypoglycemic risks
– Minimize weight gain
– Minimize adverse effects and drug interactions
– Cardiovascular benefit
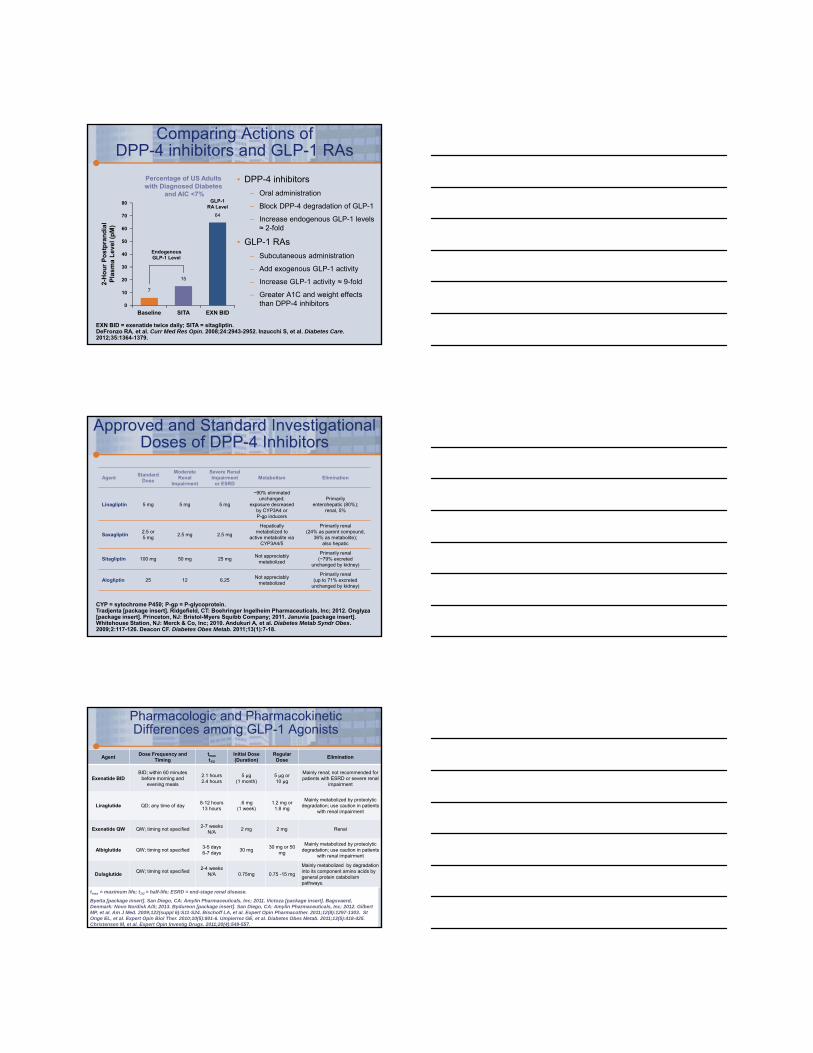
Patients Are Willing to Pay More to Avoid Weight Gain or to Lose Weight
• Patients Value
– Weight loss/avoiding weight gain
– Avoiding hypoglycemia
– Avoiding injection
– Efficacy
– Avoiding nausea
Jendle J, et al. Curr Med Res Opin. 2010;26:917-923.
Willingness-to-Pay($ USD / month)
A1C (1%)
Avoid Injection
Avoid Nausea
Avoid 1 kg wt
AvoidHypoglycemia
Weight (1 kg)
20 400 10 30
35
11
13
17
24
26
Meta-Analysis: Weight Changes with Antihyperglycemic Agents Added to Metformin
AGI = ɑ-glucosidase inhibitor; DPP-4i = DPP-4 inhibitor; GLP-1 RA = glucagon-like peptide-1 receptor agonist; SU = sulfonylurea; TZD = thiazolidinedione; SGLT-2i = sodium glucose cotransporter 2 inhibitor.Liu S, et al. Diabetes Obes Metab. 2012;14:810-820.
1
5
-3
-5
∆ W
eig
ht
(kg
)
3
-1
BiphasicInsulin
3.41
TZD Glinide DPP-4i GLP-1RA
SU BasalInsulin
AGI
2.462.17
1.40 1.38
0.23
-1.01-1.66
GLP-1 RA, DPP-4 Inhibitors, SGLT-2 Inhibitors
Highlighted forAvoiding
Weight Gain
0
4
-4
2
-2
-3.5
SGLT-2i
Hypoglycemic Risk ofAntihyperglycemic Agents Added to Metformin
Liu S, et al. Diabetes Obes Metab. 2012;14:810-820.
15
25
5
0
Od
ds
Ra
tio
vs
Pla
ce
bo 20
10
BiphasicInsulin
17.8
Glinide BasalInsulin
GLP-1RA
AGISU DPP-4i TZD
10.58.9
4.8
1.1 0.9 0.5 0.4
Increased Risk vs Placebo
No Increased Risk vs Placebo
SGLT-2i
0.6
GLP-1 Agonists and DPP-4 Inhibitors
DPP-4 Inhibitors
Drug Expected Decreasein A1C (%)
Sitagliptin(Januvia ®)
0.6
Saxagliptin(Onglyza ®)
0.73
Linagliptin(Tradjenta ®)
0.51
Alogliptin(Nesina ®)
0.6
GLP-1 Agonists
DrugExpected
Decrease in A1C (%)
Exenatide 10 mcg BID(Byetta ®)
0.8-1
Liraglutide 1.8 mg QD(Victoza ®)
1-1.6
Exenatide 2 mg QW(Bydureon ®)
1.8-2.1
Albiglutide 30-50mg QWTanzeum ®)
0.8-1
Dulaglutide 0.75 – 1.5 mg QW(Trulicity ®)
0.8-1.1
Drucker DJ, et al. Lancet. 2008;372(9645):1240-1250.
Blonde L, et al. Diabetes Obes Metab. 2009;11(Suppl 3):26-34.
Ahren B. Best Pract Res Clin Endocrinol Metab. 2007;21(4): 517-533.
Buse JB, et al. Diabetes Care. 2010;33(6):1255-1261.
Gomis R, et al. Diabetes Obes Metab. 2011;13(7):653-661.
BID = twice daily;
QD = once daily;
QW = once weekly.
Comparing Actions of DPP-4 inhibitors and GLP-1 RAs
• DPP-4 inhibitors
– Oral administration
– Block DPP-4 degradation of GLP-1
– Increase endogenous GLP-1 levels ≈ 2-fold
• GLP-1 RAs
– Subcutaneous administration
– Add exogenous GLP-1 activity
– Increase GLP-1 activity ≈ 9-fold
– Greater A1C and weight effects than DPP-4 inhibitors
EXN BID = exenatide twice daily; SITA = sitagliptin.DeFronzo RA, et al. Curr Med Res Opin. 2008;24:2943-2952. Inzucchi S, et al. Diabetes Care. 2012;35:1364-1379.
80
70
50
30
20
0
10
2-H
ou
r P
os
tpra
nd
ial
Pla
sm
a L
ev
el (
pM
)
15
Percentage of US Adultswith Diagnosed Diabetes
and AIC <7%
Baseline SITA EXN BID
64
7
EndogenousGLP-1 Level
GLP-1RA Level
60
40
Approved and Standard Investigational Doses of DPP-4 Inhibitors
AgentStandard
Dose
ModerateRenal
Impairment
Severe Renal Impairment
or ESRDMetabolism Elimination
Linagliptin 5 mg 5 mg 5 mg
~90% eliminated unchanged;
exposure decreasedby CYP3A4 orP-gp inducers
Primarilyenterohepatic (80%);
renal, 5%
Saxagliptin2.5 or 5 mg
2.5 mg 2.5 mg
Hepaticallymetabolized to
active metabolite via CYP3A4/5
Primarily renal(24% as parent compound,
36% as metabolite);also hepatic
Sitagliptin 100 mg 50 mg 25 mgNot appreciably
metabolized
Primarily renal(~79% excreted
unchanged by kidney)
Alogliptin 25 12 6.25Not appreciably
metabolized
Primarily renal(up to 71% excreted
unchanged by kidney)
CYP = sytochrome P450; P-gp = P-glycoprotein.Tradjenta [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc; 2012. Onglyza[package insert]. Princeton, NJ: Bristol-Myers Squibb Company; 2011. Januvia [package insert]. Whitehouse Station, NJ: Merck & Co, Inc; 2010. Andukuri A, et al. Diabetes Metab Syndr Obes. 2009;2:117-126. Deacon CF. Diabetes Obes Metab. 2011;13(1):7-18.
Pharmacologic and Pharmacokinetic Differences among GLP-1 Agonists
AgentDose Frequency and
Timingtmax
t1/2
Initial Dose (Duration)
Regular Dose
Elimination
Exenatide BIDBID; within 60 minutes
before morning and evening meals
2.1 hours2.4 hours
5 µg (1 month)
5 µg or 10 µg
Mainly renal; not recommended for patients with ESRD or severe renal
impairment
Liraglutide QD; any time of day8-12 hours13 hours
.6 mg (1 week)
1.2 mg or 1.8 mg
Mainly metabolized by proteolytic degradation; use caution in patients
with renal impairment
Exenatide QW QW; timing not specified2-7 weeks
N/A2 mg 2 mg Renal
Albiglutide QW; timing not specified3-5 days6-7 days
30 mg30 mg or 50
mg
Mainly metabolized by proteolyticdegradation; use caution in patients
with renal impairment
DulaglutideQW; timing not specified
2-4 weeksN/A 0.75mg 0.75 -15 mg
Mainly metabolized by degradation into its component amino acids by general protein catabolismpathways.
tmax = maximum life; t1/2 = half-life; ESRD = end-stage renal disease.
Byetta [package insert]. San Diego, CA: Amylin Pharmaceuticals, Inc; 2011. Victoza [package insert]. Bagsvaerd, Denmark: Novo Nordisk A/S; 2013. Bydureon [package insert]. San Diego, CA: Amylin Pharmaceuticals, Inc; 2012. Gilbert MP, et al. Am J Med. 2009;122(suppl 6):S11-S24. Bischoff LA, et al. Expert Opin Pharmacother. 2011;12(8):1297-1303. St Onge EL, et al. Expert Opin Biol Ther. 2010;10(5):801-6. Umpierrez GE, et al. Diabetes Obes Metab. 2011;13(5):418-425. Christensen M, et al. Expert Opin Investig Drugs. 2011;20(4):549-557.
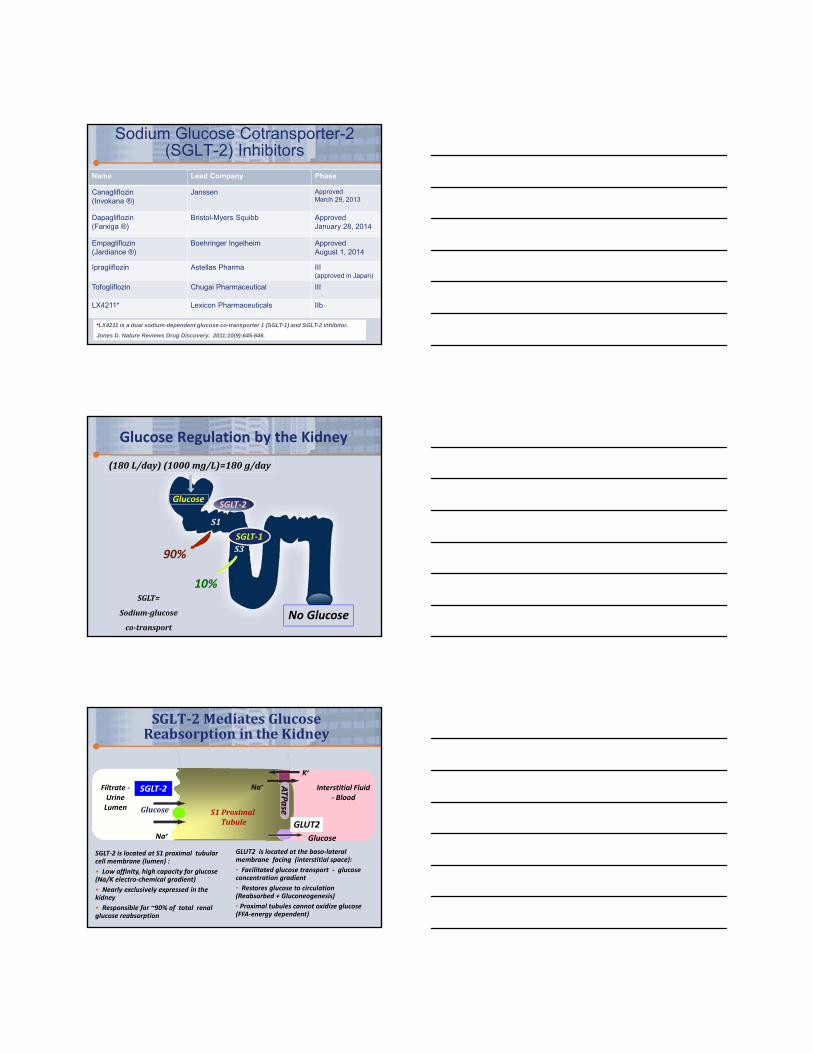
Sodium Glucose Cotransporter-2 (SGLT-2) Inhibitors
Name Lead Company Phase
Canagliflozin(Invokana ®)
Janssen Approved March 29, 2013
Dapagliflozin(Farxiga ®)
Bristol-Myers Squibb Approved January 28, 2014
Empagliflozin(Jardiance ®)
Boehringer Ingelheim Approved August 1, 2014
Ipragliflozin Astellas Pharma III(approved in Japan)
Tofogliflozin Chugai Pharmaceutical III
LX4211* Lexicon Pharmaceuticals IIb
*LX4211 is a dual sodium-dependent glucose co-transporter 1 (SGLT-1) and SGLT-2 inhibitor.
Jones D. Nature Reviews Drug Discovery. 2011;10(9):645-646.
(180L/day)(1000mg/L)=180g/day
10%
Glucose
No Glucose
S1
S3
Glucose Regulation by the Kidney
SGLT‐2
90%
SGLT=
Sodium‐glucose
co‐transport
SGLT‐1
SGLT‐2 is located at S1 proximal tubular cell membrane (lumen) :
• Low affinity, high capacity for glucose (Na/K electro‐chemical gradient)
• Nearly exclusively expressed in the kidney
• Responsible for ~90% of total renal glucose reabsorption
S1ProximalTubule
Na+
K+
ATPase
Glucose
GLUT2
Glucose
SGLT‐2 Interstitial Fluid ‐ Blood
Filtrate ‐Urine Lumen
Na+
SGLT‐2MediatesGlucoseReabsorption intheKidney
GLUT2 is located at the baso‐lateral membrane facing (interstitial space):
• Facilitated glucose transport ‐ glucose concentration gradient
• Restores glucose to circulation (Reabsorbed + Gluconeogenesis)
• Proximal tubules cannot oxidize glucose (FFA‐energy dependent)
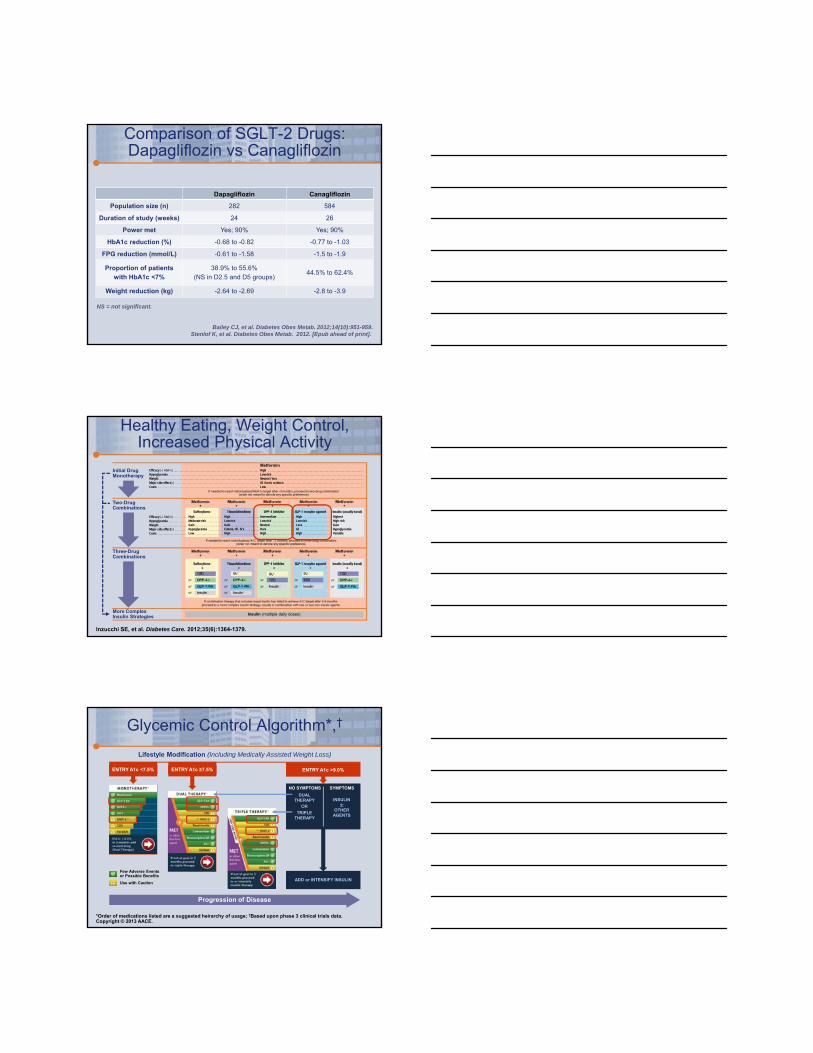
Comparison of SGLT-2 Drugs: Dapagliflozin vs Canagliflozin
Dapagliflozin Canagliflozin
Population size (n) 282 584
Duration of study (weeks) 24 26
Power met Yes; 90% Yes; 90%
HbA1c reduction (%) -0.68 to -0.82 -0.77 to -1.03
FPG reduction (mmol/L) -0.61 to -1.58 -1.5 to -1.9
Proportion of patients with HbA1c <7%
38.9% to 55.6%(NS in D2.5 and D5 groups)
44.5% to 62.4%
Weight reduction (kg) -2.64 to -2.69 -2.8 to -3.9
NS = not significant.
Bailey CJ, et al. Diabetes Obes Metab. 2012;14(10):951-959.Stenlof K, et al. Diabetes Obes Metab. 2012. [Epub ahead of print].
Inzucchi SE, et al. Diabetes Care. 2012;35(6):1364-1379.
Healthy Eating, Weight Control, Increased Physical Activity
HighModerate riskGainHypoglycemiaLow
HighLow riskGainEdema, HF, fx’sHigh
IntermediateLow riskNeutralRareHigh
HighLow riskLossGIHigh
HighestHigh riskGainHypoglycemiaVariable
HighLow riskNeutral / lossGI / lactic acidosisLow
Metformin
If needed to reach individualized HbA1c target after~3 months, proceed to two-drug combination(order not meant to denote any specific preference)
Efficacy (HbA1c)HypoglycemiaWeightMajor side effect(s)Costs
Efficacy (HbA1c)HypoglycemiaWeightMajor side effect(s)Costs
More ComplexInsulin Strategies
Three-DrugCombinations
Two-DrugCombinations
Initial DrugMonotherapy
Insulin (multiple daily doses)
*Order of medications listed are a suggested heirarchy of usage; †Based upon phase 3 clinical trials data.Copyright © 2013 AACE.
Glycemic Control Algorithm*,†
Lifestyle Modification (Including Medically Assisted Weight Loss)
Progression of Disease
ENTRY A1c <7.5% ENTRY A1c ≥7.5%
Few Adverse Eventsor Possible Benefits
Use with Caution
ENTRY A1c >9.0%
DUALTHERAPY
SYMPTOMS
TRIPLETHERAPY
NO SYMPTOMS
OR
INSULIN±
OTHERAGENTS
ADD or INTENSIFY INSULIN
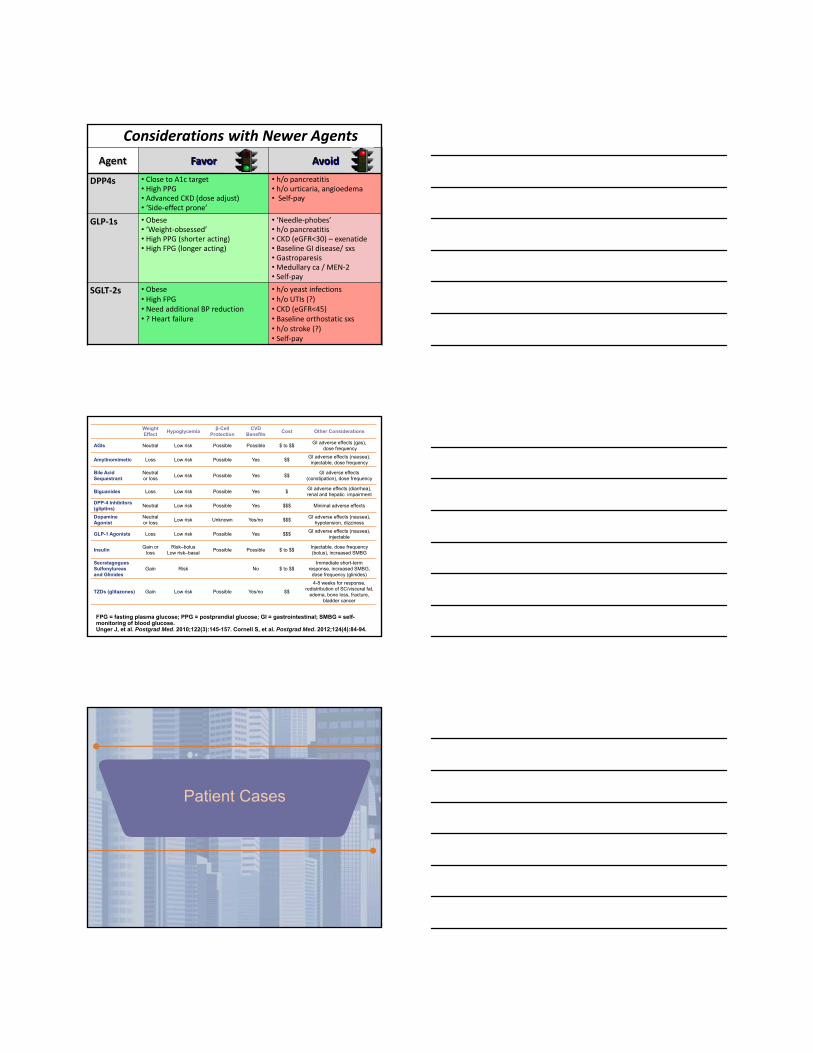
Agent Favor Avoid
DPP4s • Close to A1c target • High PPG• Advanced CKD (dose adjust)• ‘Side‐effect prone’
• h/o pancreatitis• h/o urticaria, angioedema • Self‐pay
GLP‐1s • Obese• ‘Weight‐obsessed’ • High PPG (shorter acting)• High FPG (longer acting)
• ‘Needle‐phobes’• h/o pancreatitis• CKD (eGFR<30) – exenatide• Baseline GI disease/ sxs• Gastroparesis• Medullary ca / MEN‐2• Self‐pay
SGLT‐2s • Obese• High FPG• Need additional BP reduction • ? Heart failure
• h/o yeast infections• h/o UTIs (?)• CKD (eGFR<45)• Baseline orthostatic sxs• h/o stroke (?)• Self‐pay
Considerations with Newer Agents
Weight Effect
Hypoglycemiaβ-Cell
ProtectionCVD
BenefitsCost Other Considerations
AGIs Neutral Low risk Possible Possible $ to $$GI adverse effects (gas),
dose frequency
Amylinomimetic Loss Low risk Possible Yes $$GI adverse effects (nausea), injectable, dose frequency
Bile Acid Sequestrant
Neutral or loss
Low risk Possible Yes $$GI adverse effects
(constipation), dose frequency
Biguanides Loss Low risk Possible Yes $GI adverse effects (diarrhea), renal and hepatic impairment
DPP-4 Inhibitors (gliptins)
Neutral Low risk Possible Yes $$$ Minimal adverse effects
Dopamine Agonist
Neutral or loss
Low risk Unknown Yes/no $$$GI adverse effects (nausea),
hypotension, dizziness
GLP-1 Agonists Loss Low risk Possible Yes $$$GI adverse effects (nausea),
injectable
InsulinGain or
loss Risk–bolus
Low risk–basalPossible Possible $ to $$
Injectable, dose frequency (bolus), increased SMBG
SecretagoguesSulfonylureas and Glinides
Gain Risk No $ to $$Immediate short-term
response, increased SMBG, dose frequency (glinides)
TZDs (glitazones) Gain Low risk Possible Yes/no $$
4-8 weeks for response, redistribution of SC/visceral fat,
edema, bone loss, fracture, bladder cancer
FPG = fasting plasma glucose; PPG = postprandial glucose; GI = gastrointestinal; SMBG = self-monitoring of blood glucose. Unger J, et al. Postgrad Med. 2010;122(3):145-157. Cornell S, et al. Postgrad Med. 2012;124(4):84-94.
Patient Cases
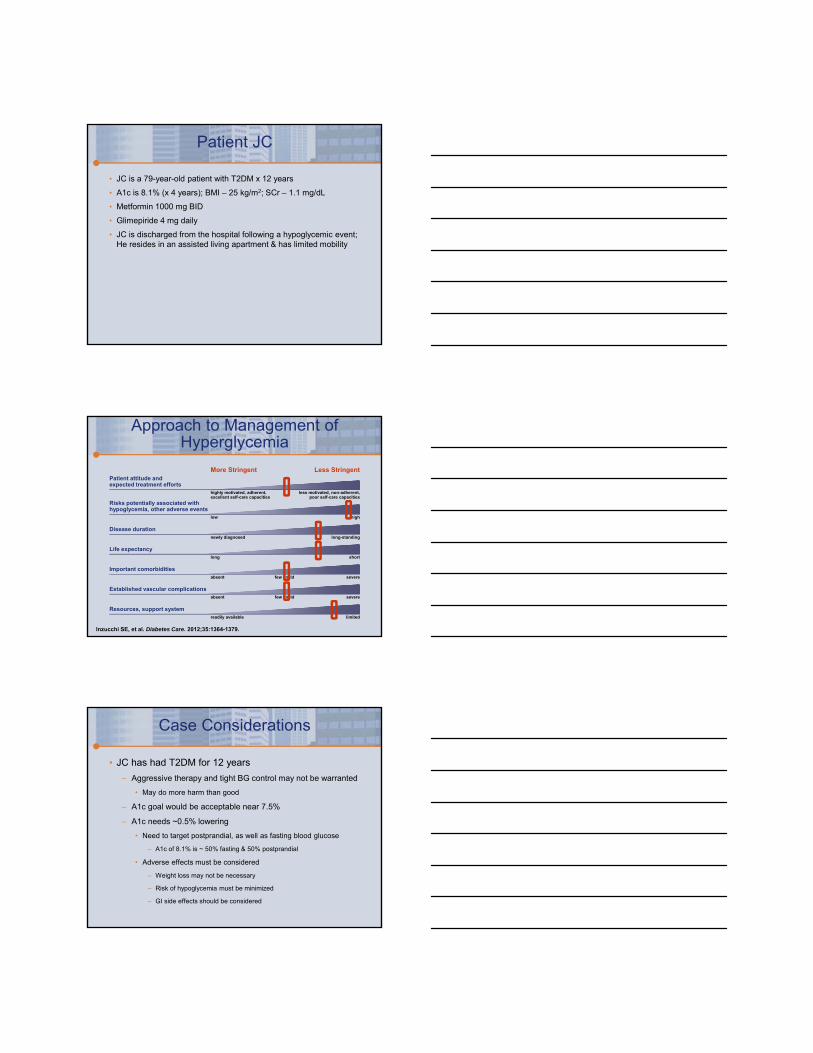
Patient JC
• JC is a 79-year-old patient with T2DM x 12 years
• A1c is 8.1% (x 4 years); BMI – 25 kg/m2; SCr – 1.1 mg/dL
• Metformin 1000 mg BID
• Glimepiride 4 mg daily
• JC is discharged from the hospital following a hypoglycemic event; He resides in an assisted living apartment & has limited mobility
absent
absent
severe
severe
few / mild
few / mild
Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379.
More Stringent Less StringentPatient attitude andexpected treatment efforts
highly motivated, adherent,excellent self-care capacities
less motivated, non-adherent,poor self-care capacities
Risks potentially associated with hypoglycemia, other adverse events
low high
Disease durationnewly diagnosed long-standing
Life expectancylong short
Important comorbidities
Resources, support systemreadily available limited
Established vascular complications
Approach to Management of Hyperglycemia
Case Considerations
• JC has had T2DM for 12 years
– Aggressive therapy and tight BG control may not be warranted
• May do more harm than good
– A1c goal would be acceptable near 7.5%
– A1c needs ~0.5% lowering
• Need to target postprandial, as well as fasting blood glucose
– A1c of 8.1% is ~ 50% fasting & 50% postprandial
• Adverse effects must be considered
– Weight loss may not be necessary
– Risk of hypoglycemia must be minimized
– GI side effects should be considered
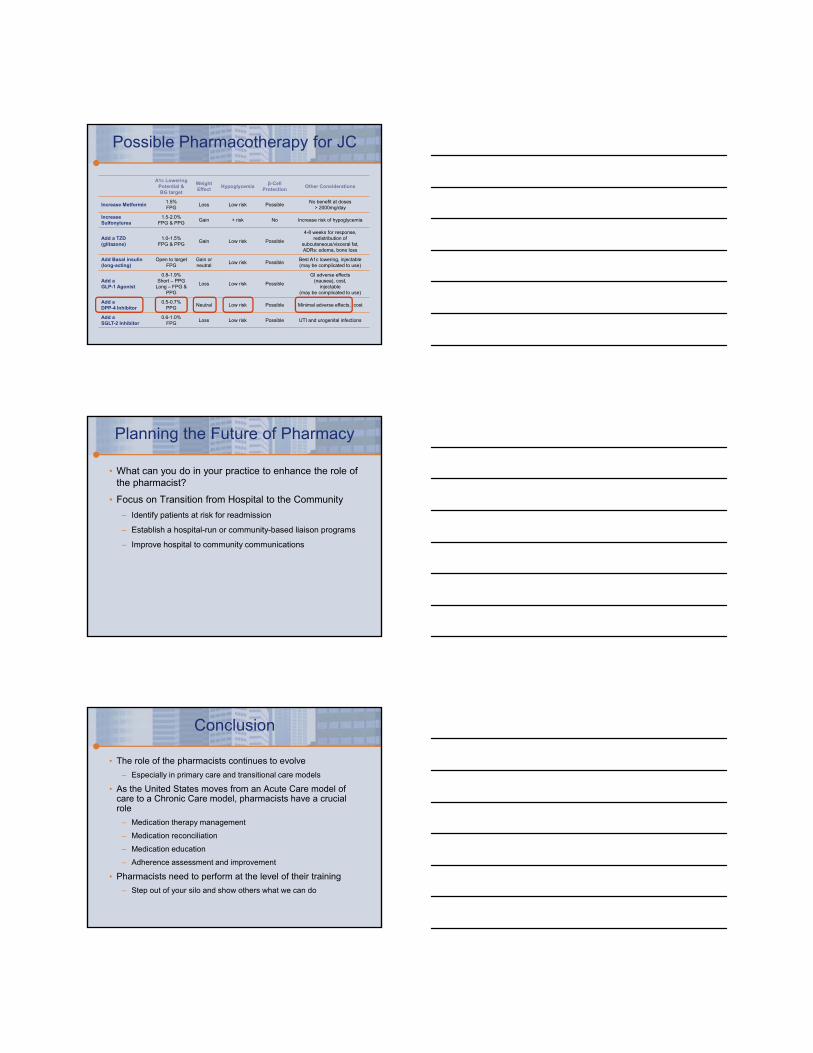
Possible Pharmacotherapy for JC
A1c Lowering Potential &BG target
Weight Effect
Hypoglycemiaβ-Cell
ProtectionOther Considerations
Increase Metformin1.5%FPG
Loss Low risk PossibleNo benefit at doses
> 2000mg/day
IncreaseSulfonylurea
1.5-2.0%FPG & PPG
Gain + risk No Increase risk of hypoglycemia
Add a TZD (glitazone)
1.0-1.5%FPG & PPG
Gain Low risk Possible
4-8 weeks for response, redistribution of
subcutaneous/visceral fat, ADRs: edema, bone loss
Add Basal insulin(long-acting)
Open to targetFPG
Gain or neutral
Low risk PossibleBest A1c lowering, injectable (may be complicated to use)
Add a GLP-1 Agonist
0.8-1.9%Short – PPG
Long – FPG & PPG
Loss Low risk Possible
GI adverse effects(nausea), cost,
injectable(may be complicated to use)
Add a DPP-4 Inhibitor
0.5-0.7%PPG
Neutral Low risk Possible Minimal adverse effects, cost
Add aSGLT-2 Inhibitor
0.6-1.0%FPG
Loss Low risk Possible UTI and urogenital infections
Planning the Future of Pharmacy
• What can you do in your practice to enhance the role of the pharmacist?
• Focus on Transition from Hospital to the Community
– Identify patients at risk for readmission
– Establish a hospital-run or community-based liaison programs
– Improve hospital to community communications
Conclusion
• The role of the pharmacists continues to evolve
– Especially in primary care and transitional care models
• As the United States moves from an Acute Care model of care to a Chronic Care model, pharmacists have a crucial role
– Medication therapy management
– Medication reconciliation
– Medication education
– Adherence assessment and improvement
• Pharmacists need to perform at the level of their training
– Step out of your silo and show others what we can do







