
Diabetes Insipidus
and SIADH: An
UpdateELI MCKENNA-WEISS, MD
KIDNEY CARE AND TRANSPLANT SERVICES OF NEW ENGLAND

I have no financial/advisory/research
conflicts of interest of any sort




SIADH




Uric acid handling in diagnosis
Uric acid level generally >5 mg/dL in hypovolemia
Uric acid level usually <4 mg/dL in SIADH
No clear pathogenesis of this









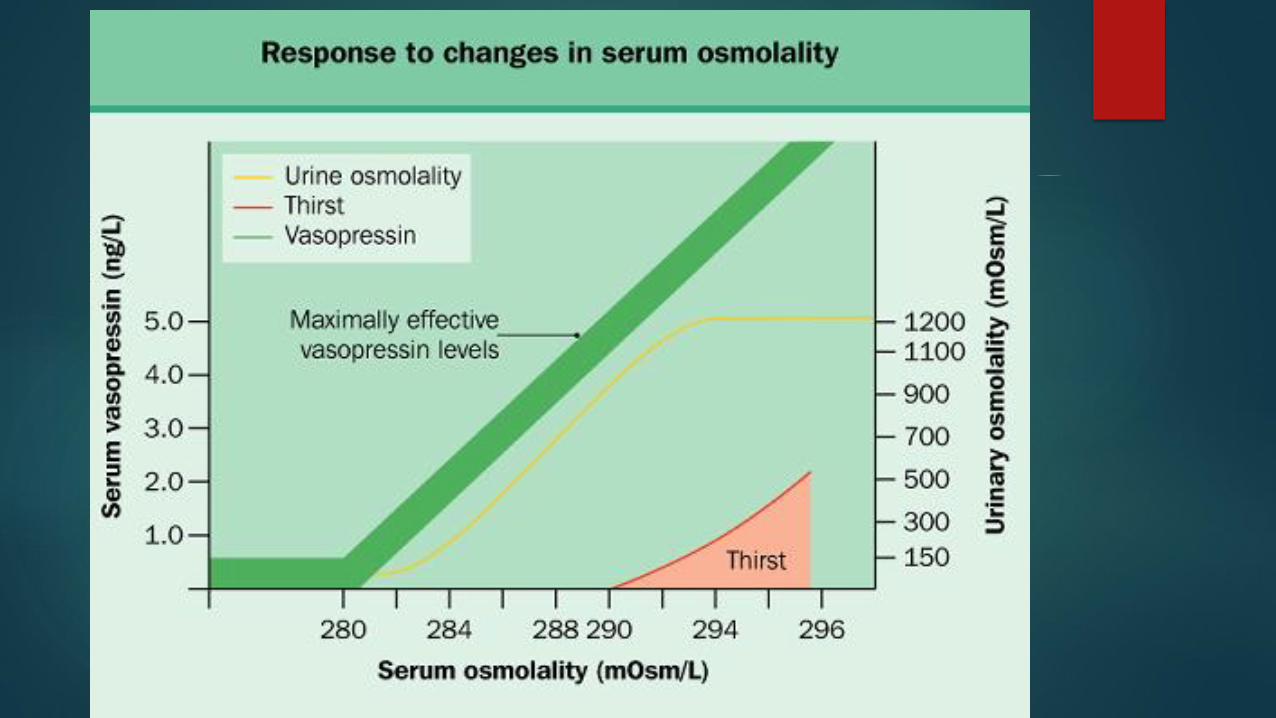
Diabetes Insipidus
Large volumes (>3 liters in 24 hours) of dilute urine (<300 mOsm/kg)
Central, partial central, nephrogenic, primary polydipsia
Gold standard for diagnosis currently the water deprivation test



New Possibilities in Diagnosis
Water deprivation is time consuming and unpleasant for patients
Runs the risk of causing dehydration prior to ddavp administration
In study recently published, this test correctly identified DI vs primary
polydipsia in 73% of patients

Copeptin
Copeptin is the C-terminal segment of argenine vasopressin prohormone
3% Saline administered until SNa was 150 (checked q30 min by POC), copeptin levels measured, then ddavp and free water administered to correct the abnormality
Patients reported this to be a less burdensome test
Equal numbers of adverse events
Correctly distinguished between the two conditions in 95% of the patients
Cases were reviewed after discharge with copeptin levels obscured. Clinical, historical and laboratory data reviewed by two investigators, a third was used in the rare occasion of a split vote


Wave of the future?
3% usually administered in intercare/step-down setting
POC testing expensive
Likely dangerous for a subset of patients (cirrhotics and CHF)
Unclear if copeptin test widely available

References
Boone, M., & Deen, P. M. (2008). Physiology and pathophysiology of the vasopressin-regulated renal water reabsorption. European Journal of Physiology, 456, 1005-1024. https://doi.org/10.1007/s00424-008-0498-1
Burst, V., Grundmann, F., Kubacki, T., Greenberg, A., Becker, I., Rudolf, D., & Verbalis, J. (2017). Thiazide-associated hyponatremia, report of the hyponatremia registry: An observational multicenter international study. American Journal of Nephrology, 45, 420-430. https://doi.org/10.1159/000471493
Farmand, S., Lindh, J. D., Calissendorff, J., Skov, J., Falhammar, H., Nathanson, D., & Mannheimer, B. (2018). Differences in associations of antidepressants and hospitalization due to hyponatremia. The American Journal of Medicine, 131, 56-63. https://doi.org/10.1016/j.amjmed.2017.07.025
Fenske, W., Refardt, J., Chifu, I., Schnyder, I., Winzeler, B., Drummond, J., ... Christ-Crain, M. (2018). A copeptin-based approach in the diagnosis of diabetes insipidus. The New England Journal of Medicine, 379, 428-439. https://doi.org/10.1056/NEJMoa1803760

Fenske, W., Stork, S., Koschker, A., Blechschmidt, A., Lorenz, D., Wortmann, S., & Allolio, B. (2008). Value of fractional uric acid excretion in differential diagnosis of hyponatremic patients on diuretics. The Journal of Clinical Endocrinology and Metabolism, 93, 2991-2997. https://doi.org/10.1210/jc.2008-0330
Hoorn, E. J., & Zietse, R. (2017). Diagnosis and treatment of hyponatremia: Compilation of the guidelines. Journal of the American Society of Nephrology, 28, 1340-1349. https://doi.org/10.1681/ASN.2016101139
Milionis, H. J., Liamis, G. L., & Elisaf, M. S. (2002). The hyponatremic patient: a systematic approach to laboratory diagnosis. Canadian Medical Association Journal, 166(8), 1056-1062. Retrieved from Http://www.cmaj.ca
Soupart, A., Coffernils, M., Couturier, B., Gankam-Kengne, F., & Decaux, G. (2012, May). Efficacy and tolerance of urea compared with vaptans for long-term treatment of patients with SIADH. Clinical Journal of the American Society of Nephrology, 7, 742-747. https://doi.org/ 10.2215/CJN.06990711
Sterns, R. H., Silver, S. M., & Hix, J. K. (2015). Urea for hyponatremia? Kidney International, 87, 268-270. https://doi.org/10.1038/ki.2014.320







