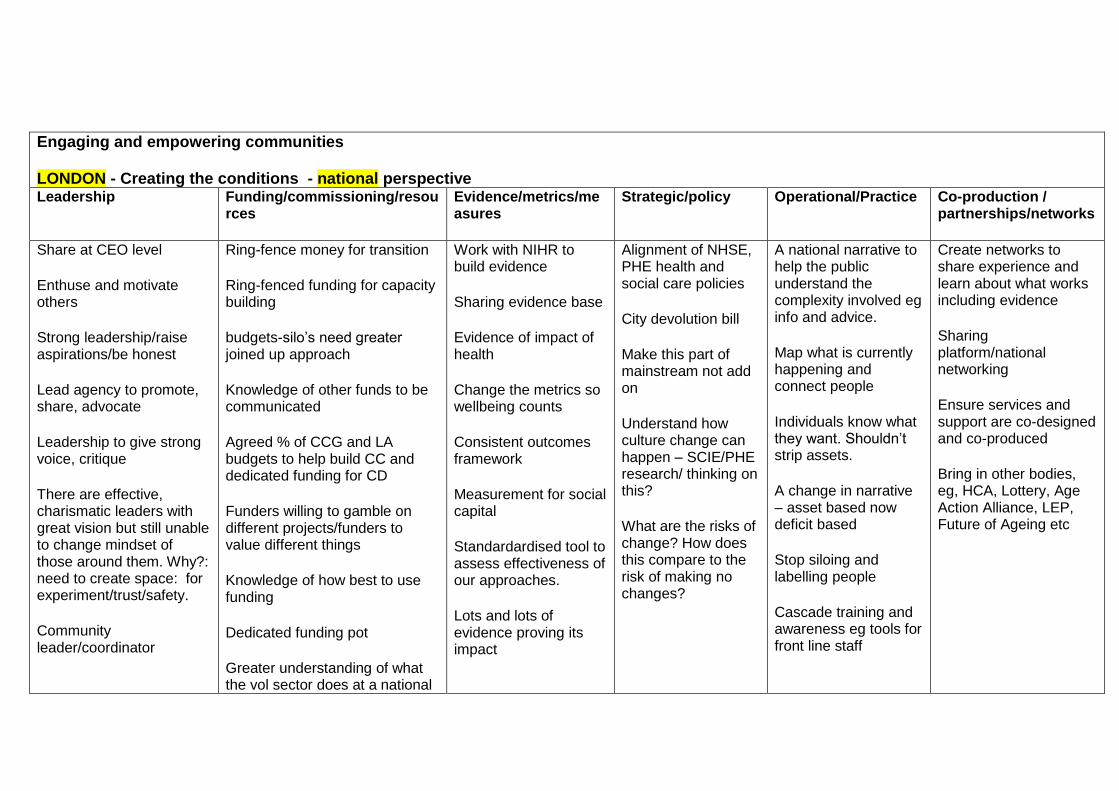
Engaging and empowering communities LONDON - Creating the conditions - national perspective Leadership
Funding/commissioning/resources
Evidence/metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships/networks
Share at CEO level
Enthuse and motivate others
Strong leadership/raise aspirations/be honest
Lead agency to promote, share, advocate
Leadership to give strong voice, critique
There are effective, charismatic leaders with great vision but still unable to change mindset of those around them. Why?: need to create space: for experiment/trust/safety.
Community leader/coordinator
Ring-fence money for transition
Ring-fenced funding for capacity building
budgets-silo’s need greater joined up approach
Knowledge of other funds to be communicated
Agreed % of CCG and LA budgets to help build CC and dedicated funding for CD
Funders willing to gamble on different projects/funders to value different things
Knowledge of how best to use funding
Dedicated funding pot
Greater understanding of what the vol sector does at a national
Work with NIHR to build evidence
Sharing evidence base
Evidence of impact of health
Change the metrics so wellbeing counts
Consistent outcomes framework
Measurement for social capital
Standardardised tool to assess effectiveness of our approaches.
Lots and lots of evidence proving its impact
Alignment of NHSE, PHE health and social care policies
City devolution bill
Make this part of mainstream not add on
Understand how culture change can happen – SCIE/PHE research/ thinking on this?
What are the risks of change? How does this compare to the risk of making no changes?
A national narrative to help the public understand the complexity involved eg info and advice.
Map what is currently happening and connect people
Individuals know what they want. Shouldn’t strip assets.
A change in narrative – asset based now deficit based
Stop siloing and labelling people
Cascade training and awareness eg tools for front line staff
Create networks to share experience and learn about what works including evidence
Sharing platform/national networking
Ensure services and support are co-designed and co-produced
Bring in other bodies, eg, HCA, Lottery, Age Action Alliance, LEP, Future of Ageing etc
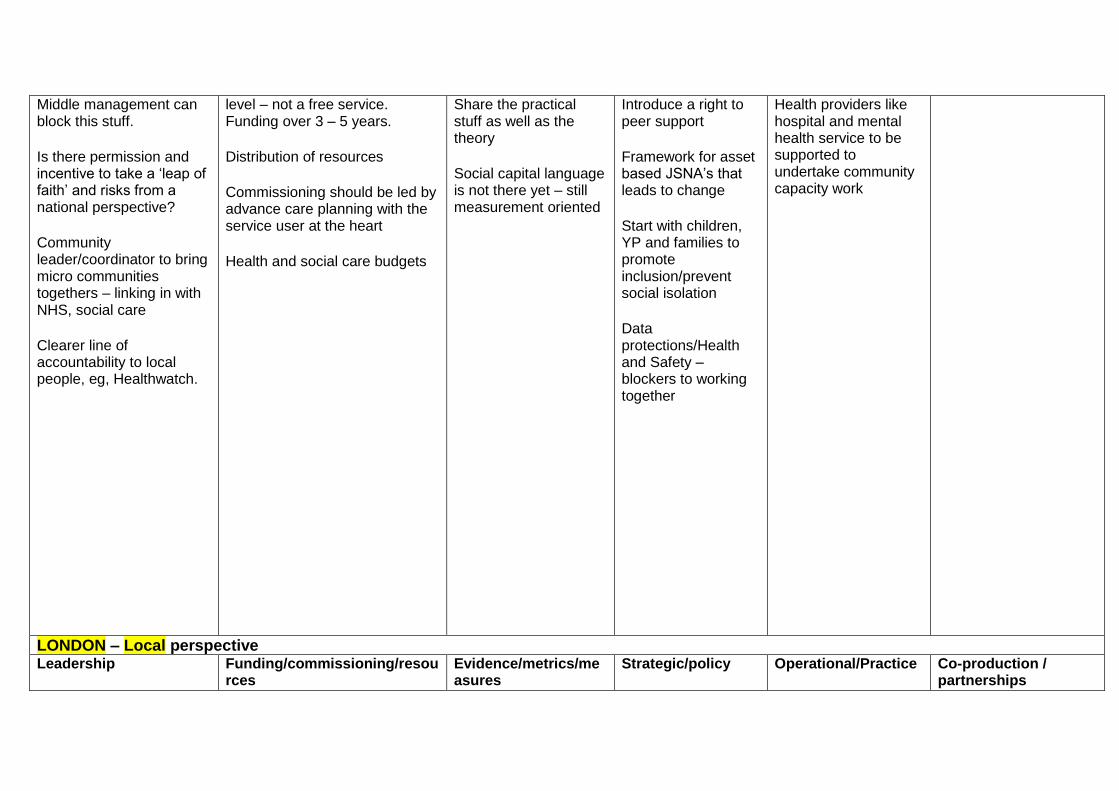
Middle management can block this stuff.
Is there permission and incentive to take a ‘leap of faith’ and risks from a national perspective?
Community leader/coordinator to bring micro communities togethers – linking in with NHS, social care
Clearer line of accountability to local people, eg, Healthwatch.
level – not a free service. Funding over 3 – 5 years.
Distribution of resources
Commissioning should be led by advance care planning with the service user at the heart
Health and social care budgets
Share the practical stuff as well as the theory
Social capital language is not there yet – still measurement oriented
Introduce a right to peer support
Framework for asset based JSNA’s that leads to change
Start with children, YP and families to promote inclusion/prevent social isolation
Data protections/Health and Safety – blockers to working together
Health providers like hospital and mental health service to be supported to undertake community capacity work
LONDON – Local perspective Leadership Funding/commissioning/resou
rces Evidence/metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships
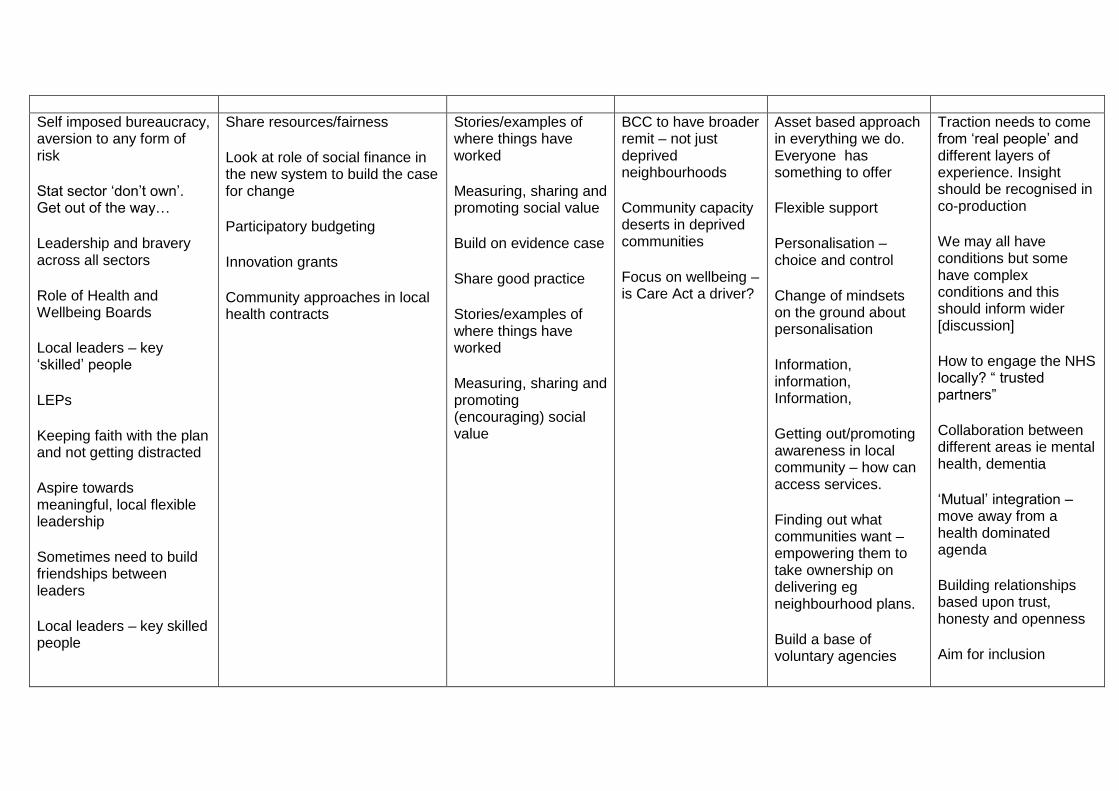
Self imposed bureaucracy, aversion to any form of risk
Stat sector ‘don’t own’. Get out of the way…
Leadership and bravery across all sectors
Role of Health and Wellbeing Boards
Local leaders – key ‘skilled’ people
LEPs
Keeping faith with the plan and not getting distracted
Aspire towards meaningful, local flexible leadership
Sometimes need to build friendships between leaders
Local leaders – key skilled people
Share resources/fairness
Look at role of social finance in the new system to build the case for change
Participatory budgeting
Innovation grants
Community approaches in local health contracts
Stories/examples of where things have worked
Measuring, sharing and promoting social value
Build on evidence case
Share good practice
Stories/examples of where things have worked
Measuring, sharing and promoting (encouraging) social value
BCC to have broader remit – not just deprived neighbourhoods
Community capacity deserts in deprived communities
Focus on wellbeing – is Care Act a driver?
Asset based approach in everything we do. Everyone has something to offer
Flexible support
Personalisation – choice and control
Change of mindsets on the ground about personalisation
Information, information, Information,
Getting out/promoting awareness in local community – how can access services.
Finding out what communities want – empowering them to take ownership on delivering eg neighbourhood plans.
Build a base of voluntary agencies
Traction needs to come from ‘real people’ and different layers of experience. Insight should be recognised in co-production
We may all have conditions but some have complex conditions and this should inform wider [discussion]
How to engage the NHS locally? “ trusted partners”
Collaboration between different areas ie mental health, dementia
‘Mutual’ integration – move away from a health dominated agenda
Building relationships based upon trust, honesty and openness
Aim for inclusion
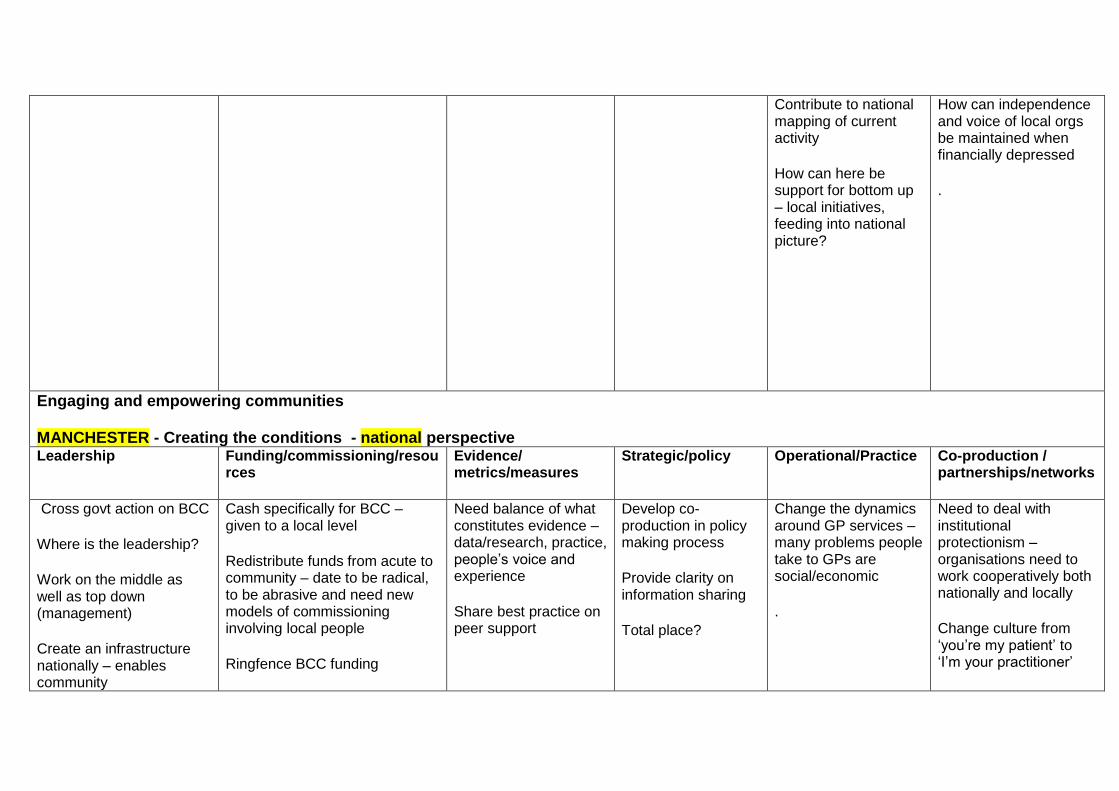
Contribute to national mapping of current activity
How can here be support for bottom up – local initiatives, feeding into national picture?
How can independence and voice of local orgs be maintained when financially depressed
.
Engaging and empowering communities MANCHESTER - Creating the conditions - national perspective
Leadership
Funding/commissioning/resources
Evidence/ metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships/networks
Cross govt action on BCC
Where is the leadership?
Work on the middle as well as top down (management)
Create an infrastructure nationally – enables community
Cash specifically for BCC – given to a local level
Redistribute funds from acute to community – date to be radical, to be abrasive and need new models of commissioning involving local people
Ringfence BCC funding
Need balance of what constitutes evidence – data/research, practice, people’s voice and experience
Share best practice on peer support
Develop co-production in policy making process
Provide clarity on information sharing
Total place?
Change the dynamics around GP services – many problems people take to GPs are social/economic
.
Need to deal with institutional protectionism – organisations need to work cooperatively both nationally and locally
Change culture from ‘you’re my patient’ to ‘I’m your practitioner’

….(Procurement, regs – cqc /risk)
Emphasis on employers contribution (Tesco example)
Leadership and monitoring
Where have community budgets gone?
Change focus form balancing books to commissioning for outcomes for local people
Tie into funding (BCC?)
Incentivise collaboration rather than competition
Commissioning deadlines can be a barrier/new model of commissioning involving local people/commissioning for outcomes/
Need smaller more community focused approach to commissioning/need longer term approach
Invest in creative housing solutions, self build, co-housing etc
Invest in peer support
Act in a way that is true to the evidence base
Need new metrics
Needs to think about what is being measured and how-real quality.
National data systems that include social and community social and community factors, wellbeing
Easy to adapt the language but not change practice
MANCHESTER – Local Perspective
Leadership
Funding/commissioning/resources
Evidence/metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships
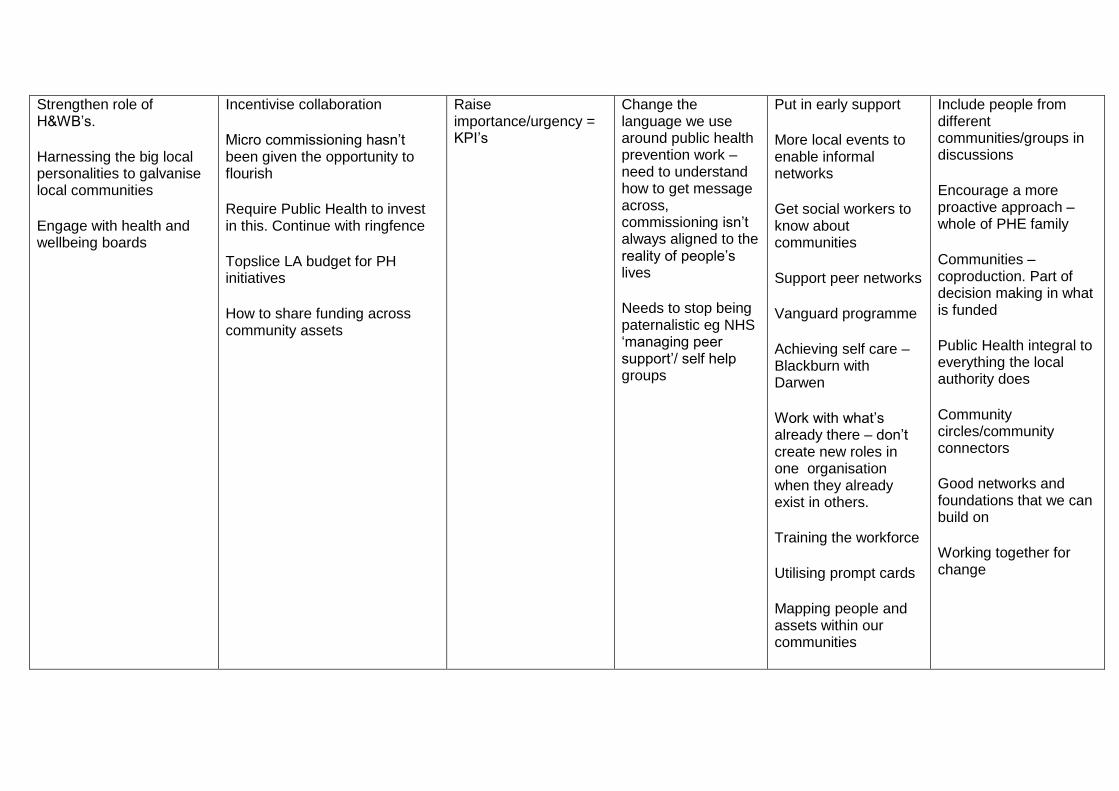
Strengthen role of H&WB’s.
Harnessing the big local personalities to galvanise local communities
Engage with health and wellbeing boards
Incentivise collaboration
Micro commissioning hasn’t been given the opportunity to flourish
Require Public Health to invest in this. Continue with ringfence
Topslice LA budget for PH initiatives
How to share funding across community assets
Raise importance/urgency = KPI’s
Change the language we use around public health prevention work – need to understand how to get message across, commissioning isn’t always aligned to the reality of people’s lives
Needs to stop being paternalistic eg NHS ‘managing peer support’/ self help groups
Put in early support
More local events to enable informal networks
Get social workers to know about communities
Support peer networks
Vanguard programme
Achieving self care – Blackburn with Darwen
Work with what’s already there – don’t create new roles in one organisation when they already exist in others.
Training the workforce
Utilising prompt cards
Mapping people and assets within our communities
Include people from different communities/groups in discussions
Encourage a more proactive approach – whole of PHE family
Communities – coproduction. Part of decision making in what is funded
Public Health integral to everything the local authority does
Community circles/community connectors
Good networks and foundations that we can build on
Working together for change

Need to stop seeing things as public service provision ‘no luncheon club’ but ‘weatherspoons meet up’. Language
Engaging and empowering communities NEWCASTLE - Creating the conditions - national perspective
Leadership
Funding/commissioning/resources
Evidence/ metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships
Do it because it matters not because you think it will save £’s
It isn’t a tokenistic project by project agenda- it is about culture change (including new ways for org/people development
Use localism to challenge central decisions and drive action in communities and local areas
Vital to shift the power held by organisations esp. NHS and professional structure/hierarchies.
No investment at local level. Asset mapping leads to people getting connected and current resources full.
Stop financial cuts – invest in communities (first area where services are cut)
Funding that considers assets/protective factors not just need and programmes that address assets not just need
More funding! (for the right things)
Holistic funding streams
More balance of what constitutes evidence- data/research, practice, people’s voice and experience
Joint dots to evidence and outcomes to value assets
Measuring /targets for evidence of quality process not just narrative
Prioritise equity for all regional outcomes
National data systems that include social and community factors,
Private sector businesses (employers) need to understand and utilise employment of those with disabilities and support needs as PR opportunity. (B&Q and older people.) Invest/incentivise a more diverse workforce.
Language – ‘life package’ NOT ‘care package’
Stop our ‘voluntarising’ day to day good neighbourliness into a service
Build the skills of capacity builders. ABCD is more than change of job title
Develop and think about geographic work to develop ‘community capacity’
Community development to be includes in GP, nursing etc training?
Be informed from local expertise

NEED TO CHALLENGE THEIR EVIDENCE.
Work on the middle as well as top down and bottom up. This is where the blocks are
Reverse austerity – be clear, don’t abuse the terms.
Collective national commitment (vision, guidance, outcomes, evidence, policy, programmes, strategy,insight, marketing with all sectors)
Political will for true social justice
Could CCG’s be more ‘mandated’ to do community development?
Integration messages should be broader than health and social care (eg housing, 3rd sector)
Longer time than 5 year cycles – takes time
Investment in community development
Put health and social care budgets together
Focus on prevention/shift from acute – 5 -10 year transformation fund, sign off %
Commissioning is moving to larger more formal contracts. Should be smaller more community focused.
Commissioning is too short term. Need long term settlement/outcomes measurements
Fair timescales and expectation
Levers with CCG’s: what they commission/voice in commissioning groups/relationship with providers and CVS
Reverse austerity – be clear, don’t abuse the terms
wellbeing not just resilience
Need to think about what is being measured and how – real quality
Could we/should we legislate/enforce voting?
Take the risk out volunteering and social actions eg litigation. In US, volunteering gives you points towards college entrance and employment
Help to translate evidence to all audiences in the narrative
Policy context already appears supportive
Raising awareness of ALL agencies responsibilities under Care Act

NEWCASTLE – Local perspective
Leadership
Funding/commissioning/resources
Evidence/metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships
Local politicians becoming more collaborative – eg, training programme for elected members in ABCD
H&WB Board participation and CVS
Flavour of the month prioritising
Devolution
Build collaboration into commissioning
Bottom up approach rather than commissioners determination
Closer work with LA commissioning on asset based approaches
Building relationships so commissioners know the people/orgs affected
Invest! Stat agencies starting to act as enablers.
Use data based on assets/positive, protective factors for health and wellbeing
Process of local evidence-base creation
Tension between organisation sustainability and immediate priority/targets
Prevention – VCS save PHC work
Use localism BUT choose reps carefully and avoid the usual suspects
Translate evidence into local narrative for different audiences
Quality improvement build in
Who helps and who should navigate the system? Continual process
Lots of different initiatives that we are all trying to develop drive the same directions ‘capacity building’ ‘localism’ etc. Why are people not getting together?
Consider different way to engage communities with democratic processes eg devolution in Scotland
Only the minority vote in the current system

Inconsistency of services drive by short –term funding
Awareness raising of what is already out there – professionals and public
Education for communities – bring back community development workers
Less about party politics more about causes and what local commissioners care about
Reach those who don’t need/won’t/use services – no relationship with commissioners
Encourage communities to coalesce around issues eg HS2 in West Midlands
Genuine professional and community consultation
Genuine CCG engagement needs to happen
Competing agendas from different agencies
Ask, listen and involve local communities

Better communication: CCG=VCS=SSD
VCS Alliance to be the partner
Engaging and empowering communities BIRMINGHAM - Creating the conditions - national perspective
Leadership
Funding/commissioning/resources
Evidence/metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships
Mandate HWB’s to map and support community centres
Mandatory that 3rd sector sit on HWB’s
How can people volunteer without affecting benefits?
Cross party discussion
Identify/remove barriers
Citizen expert
Leaders have genuine conversations (not test own ideas) that enable communities to set
Securing investment in “places to meet” community centres, libraries etc
Consider ring fenced budget
Invest in communities
Money to follow the rhetoric (outside established mechanism)
Recognition that volunteers have a cost attached, eg training
Mandate CCG’s to commission this type of work
Longer term contracts
Flexibility within contracts
Evidence that would make co-production work
Methodology = coproduction - how it would look
Create proportionate/effective measurement systems of community centred activity – value stories
Light touch Assurance
Continue national programme to collect evidence/support development
Right language
Common messages – explore at national level
National platform for standardised information useful to local community leaders eg rural community council, village hall advisor, funding advisors.
Good practice guide
Better communication of key messages and support
Work bottom up not top down
Listen!!
Are we over professionalising life? More affluent areas to get involved. Are we storing up huge health problems for the future?
Campaign to encourage people to help others
People volunteer (5 days) per year to help others
More skills sharing

agenda of what is important to them
Leaders accept the solutions communities create
Allow creativity
More trusting
Joined up government departments/agenda
Building community capacity not a substitute for services
Right representation on HWB’s
FYFV community engagement a priority
There are the right words, eg, localism but they don’t release the power for implementation
Politicians to really understand their communities
Relax how we measure outcomes – be more creative
Share stories – what works
Education (PHSE)
Encourage volunteering nationally
Support available for everyone
Encourage community support
Other currency to support (timebanking)
Stop measures that determine/direct intervention
Embed as integral to behaviour – not an add on to business
More trusting
Less jargon
Don’t duplicate
Recognise lead in time/planning
National bodies need to get connected with communities
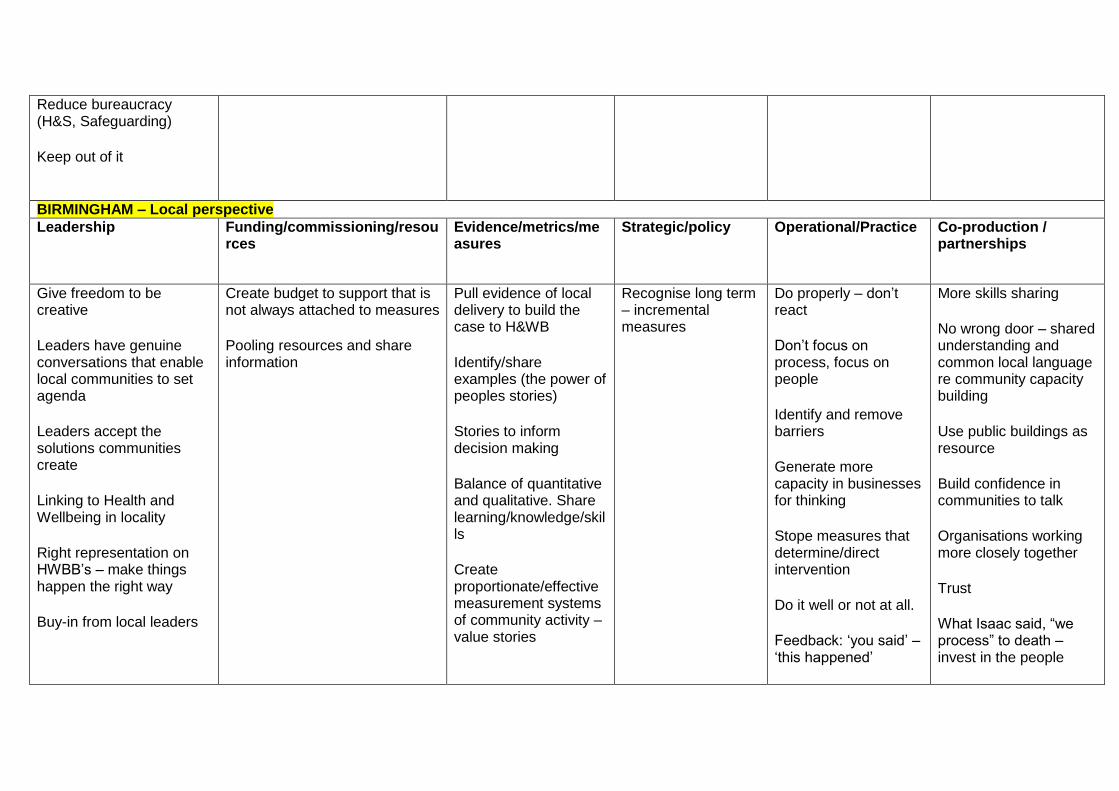
Reduce bureaucracy (H&S, Safeguarding)
Keep out of it
BIRMINGHAM – Local perspective
Leadership
Funding/commissioning/resources
Evidence/metrics/measures
Strategic/policy Operational/Practice
Co-production / partnerships
Give freedom to be creative
Leaders have genuine conversations that enable local communities to set agenda
Leaders accept the solutions communities create
Linking to Health and Wellbeing in locality
Right representation on HWBB’s – make things happen the right way
Buy-in from local leaders
Create budget to support that is not always attached to measures
Pooling resources and share information
Pull evidence of local delivery to build the case to H&WB
Identify/share examples (the power of peoples stories)
Stories to inform decision making
Balance of quantitative and qualitative. Share learning/knowledge/skills
Create proportionate/effective measurement systems of community activity – value stories
Recognise long term – incremental measures
Do properly – don’t react
Don’t focus on process, focus on people
Identify and remove barriers
Generate more capacity in businesses for thinking
Stope measures that determine/direct intervention
Do it well or not at all.
Feedback: ‘you said’ – ‘this happened’
More skills sharing
No wrong door – shared understanding and common local language re community capacity building
Use public buildings as resource
Build confidence in communities to talk
Organisations working more closely together
Trust
What Isaac said, “we process” to death – invest in the people
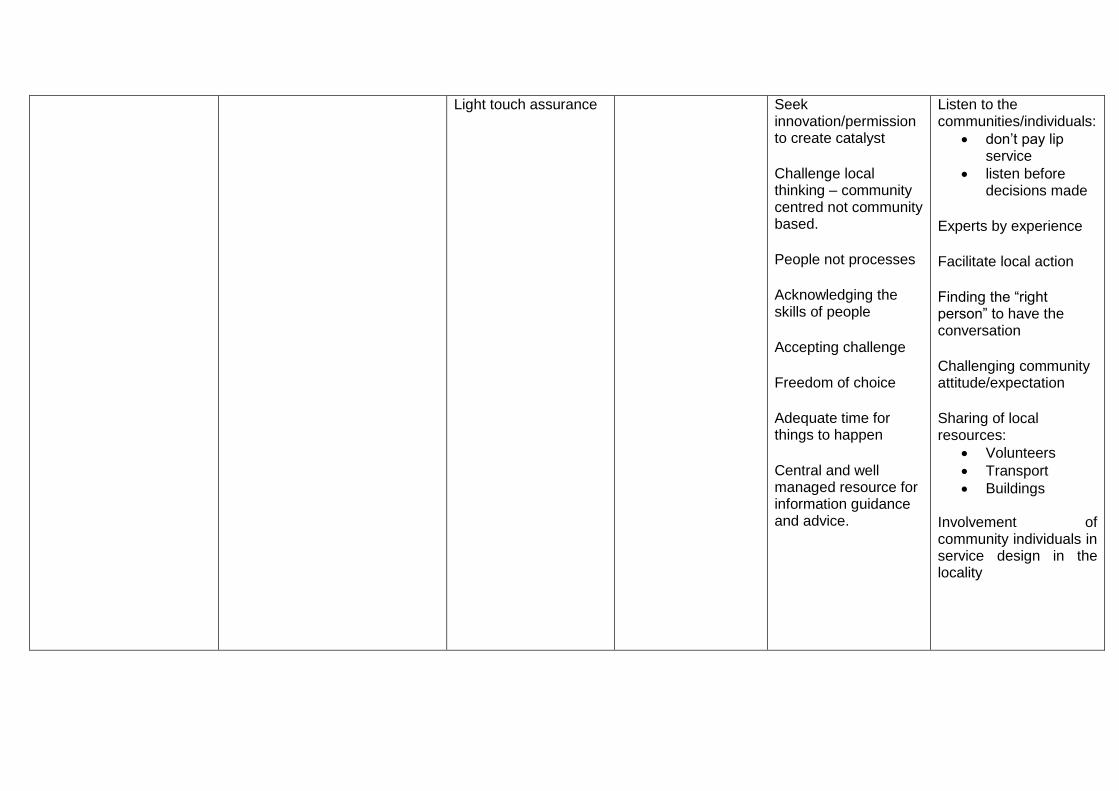
Light touch assurance
Seek innovation/permission to create catalyst
Challenge local thinking – community centred not community based.
People not processes
Acknowledging the skills of people
Accepting challenge
Freedom of choice
Adequate time for things to happen
Central and well managed resource for information guidance and advice.
Listen to the communities/individuals:
don’t pay lip service
listen before decisions made
Experts by experience
Facilitate local action
Finding the “right person” to have the conversation
Challenging community attitude/expectation
Sharing of local resources:
Volunteers
Transport
Buildings
Involvement of community individuals in service design in the locality








