Florida Emergency Department Florida Emergency Department CollaborativeCollaborative
June 8, 2011June 8, 2011
Presented by:Howard Pitluk, MD, MPH, FACS, Vice President/Chief Medical OfficerMargaret deHesse, RN, BSN, Executive Director State and Corporate Services
Overview
Goal of the Emergency Department (ED) Collaborative
Objectives of the ED Collaborative Characteristics of ED populations National and Florida ED utilization ED utilization analysis – HMO/PSN Key drivers of inappropriate ED use Conclusions Timeline
Goal of the ED Collaborative
Reduce unnecessary ED utilization among Florida Medicaid managed care recipients through a collaborative effort
Effectiveness of current Florida-specific ED strategies
Challenges in managing consumer and provider
behaviors resulting in inappropriate ED utilization
Need to address ED utilization at a systems level

Goal of the ED Collaborative
Direct managed care consumers to seek care in the most appropriate setting and to reduce ED use in non-emergent situationsLeadership required to direct the effort
Identify the priorities
Identify the stakeholders
Identify possible solutions/strategies

Characteristics of ED Populations
National Hospital Ambulatory Medical Care Study – 2006 Emergency Department Summary, DHHS, CDC, August 2008. Medicaid consumers visit the ER more frequently than
individuals with any other source of payment
Infants under twelve months had the highest utilization
Persons aged 75 and older were the second highest followed by persons living in nursing homes and homeless persons
Black persons visited the ERs approximately twice as often as white persons, regardless of age

National ED Utilization
Florida’s overall ED utilization rates have been consistently comparable to national averages.

Classification of ED Visits
NYU Algorithm:Developed with advice of panel of ED and Primary
Care Physicians (PCPs) after examination of nearly 6,000 full ED records by panel
Grouped ED visits into categories: Non-emergent Emergent Primary Care Treatable Emergent Preventable/Avoidable Emergent Not Preventable/Avoidable
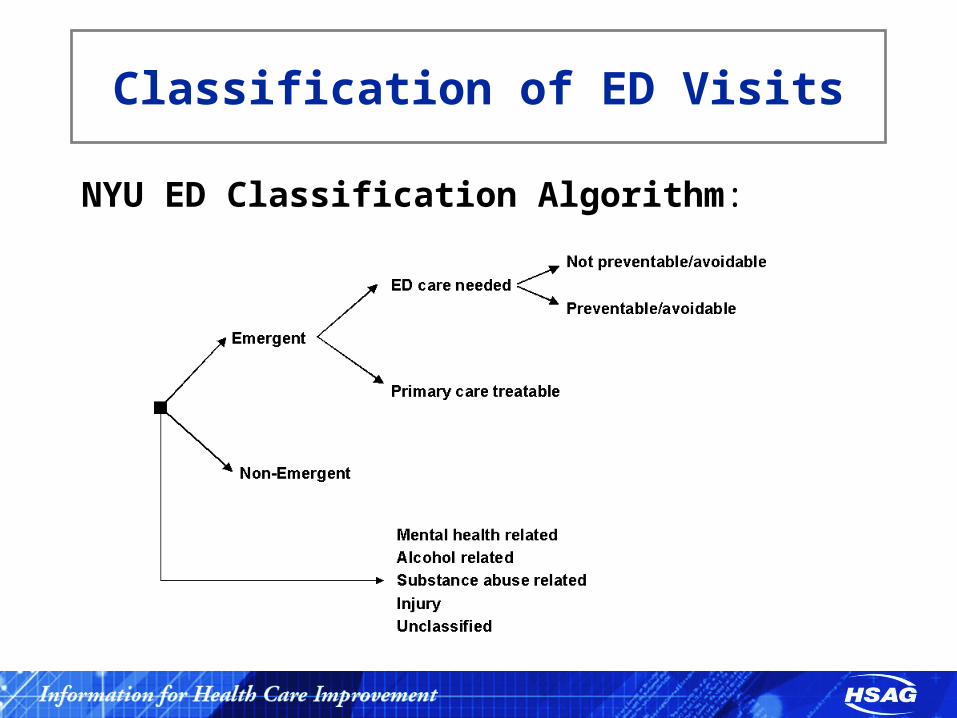
Classification of ED Visits
NYU ED Classification Algorithm:

Florida Medicaid ED Utilization Rates - Methods and Findings
Participating plans included Reform HMOs and PSNs in Broward, Baker, Clay, Duval, and Nassau counties
State fiscal year (SFY) 2010 Claims Data was employed in all ED analyses
Applied NYU algorithm to SFY 2010 ED Visits
ED utilization analysis includes results reported by: Product type by Adult and Child
Top 10 Diagnoses by Adult and Child
Gender
Age

Non-Emergent/PCP Treatable/Preventable ED Visits Demographics
Demographic Categories
Non-Emergent, PCP Treatable, Preventable ED Visits
Number of Visits Percentage of Visits
GenderMale 30,299 53.2%
Female 47,763 58.9%
Age GroupAdult 28,451 57.0%
Child 49,521 56.3%
Age and Gender
Male, 21+ 6,073 49.9%
Male, 0-20 24,226 54.2%
Female, 21+ 22,378 59.3%
Female, 0-20 25,295 58.6%
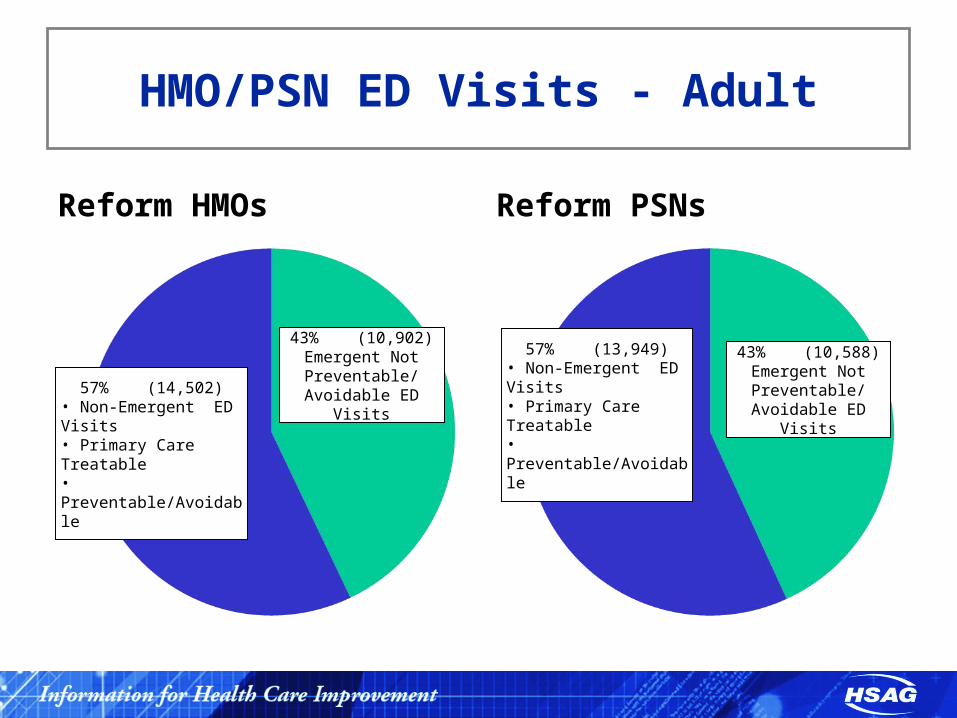
HMO/PSN ED Visits - Adult
Reform HMOs Reform PSNs
43% (10,588)Emergent Not
Preventable/ Avoidable ED Visits
57% (13,949)• Non-Emergent ED Visits• Primary Care Treatable• Preventable/Avoidable
43% (10,902)Emergent Not
Preventable/ Avoidable ED Visits57% (14,502)
• Non-Emergent ED Visits• Primary Care Treatable• Preventable/Avoidable
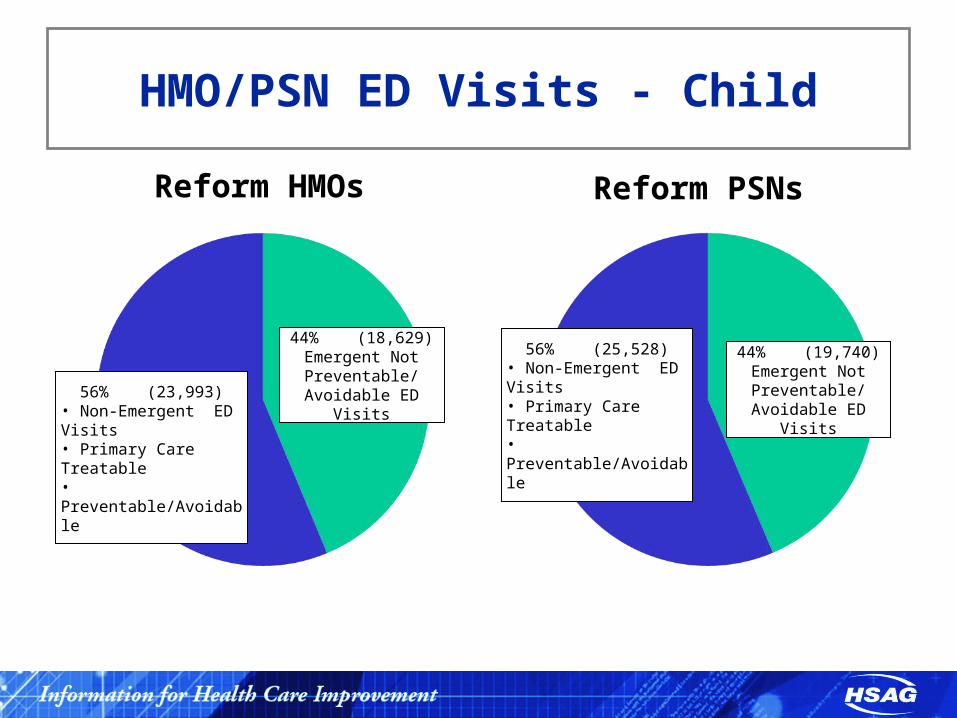
HMO/PSN ED Visits - Child
Reform HMOs Reform PSNs
44% (19,740)Emergent Not
Preventable/ Avoidable ED Visits
56% (25,528)• Non-Emergent ED Visits• Primary Care Treatable• Preventable/Avoidable
44% (18,629)Emergent Not
Preventable/ Avoidable ED Visits56% (23,993)
• Non-Emergent ED Visits• Primary Care Treatable• Preventable/Avoidable
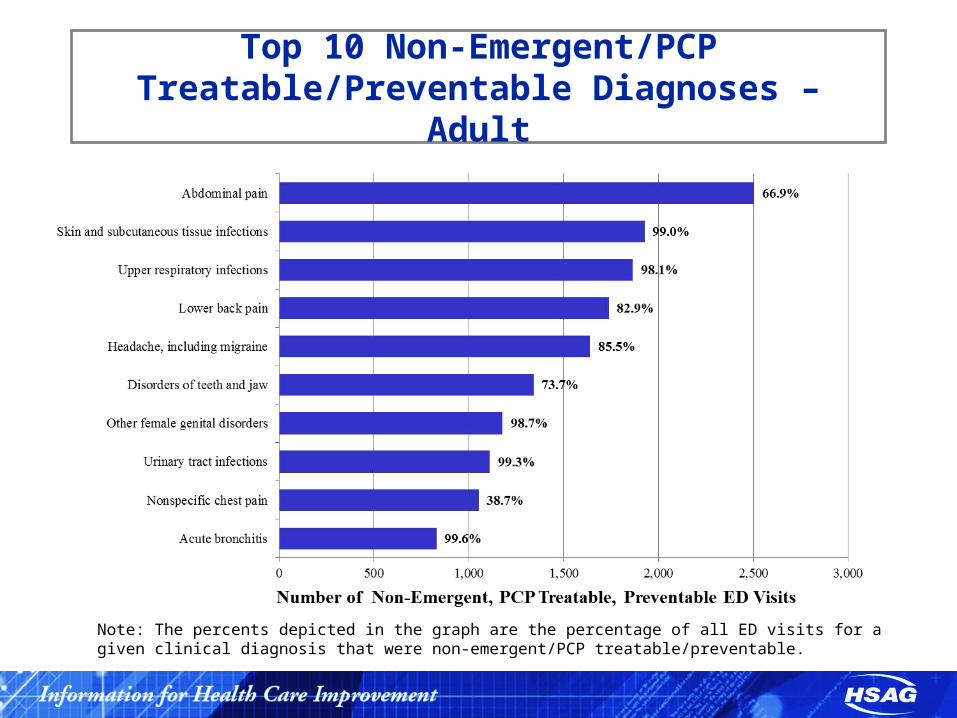
Top 10 Non-Emergent/PCP Treatable/Preventable Diagnoses – Adult
Note: The percents depicted in the graph are the percentage of all ED visits for a given clinical diagnosis that were non-emergent/PCP treatable/preventable.

Top 10 Non-Emergent/PCP Treatable/Preventable Diagnoses – Child
Note: The percents depicted in the graph are the percentage of all ED visits for a given clinical diagnosis that were non-emergent/PCP treatable/preventable.

Summary of Findings
When evaluating product type (i.e., HMO vs. PSN), there is little to no variation in the percentage of non-emergent, PCP treatable, and preventable/avoidable ED visits for both the adult and child populations
In comparing the top ten diagnoses of non-emergent, PCP treatable, and preventable/avoidable ED visits between the adult and child populations three common diagnosis were identified:Upper respiratory infectionsAbdominal painSkin and subcutaneous tissue infections
Key Drivers of Inappropriate ED Use
Consumers Inadequate logistical access to primary care services
Lack of knowledge about when to use primary care, urgent care, and emergency care
Lack of alternatives to the ER for after-hours health care
Lack of convenient or “open” appointments
Lack of access for specialty and behavioral health services
Lack of disincentive for use of the ER for non-emergency conditions
Key Drivers of Inappropriate ED Use
Primary Care Providers (PCPs)Lack of alternative methods to address and treat
emergency call needs
Lack of member/PCP relationship (educational opp.)
Lack or absence of a provider phone message
Lack of incentives for providers to provide after hours care
Key Drivers of Inappropriate ED Use
Managed Care PlansLack of a consistent approach regarding when to use
primary care, urgent care, and emergency care
Lack of timely communication between the ED and managed care plans
Lack of member education on ED use
Lack of timely information about members accessing care in the ED

Key Drivers of Inappropriate ED Use
Emergency DepartmentHospitals treat consumers who present, citing the
federal Emergency Medical Treatment and Active Labor Act (EMTALA) - 1986
Consumers can receive health care regardless of resources or time of day
Lack of incentives for hospitals to reduce ED utilization
Lack of communication with managed care plans and providers

Conclusions
Geographic factors, chronic health conditions, and primary care access are all predictors of ED utilization patterns for Medicaid recipients
Potentially successful strategies include increased access to primary care and managed care interventions
Reducing avoidable emergency care will require greater coordination among EDs, Health Plans, PCPs, and consumers
There is no “gold standard” regarding initiatives to reduce avoidable visits to the ED

Timeline

Florida Emergency Department Florida Emergency Department CollaborativeCollaborative
Questions







