fMRI (functional Magnetic Resonance Imaging)
and Optic Neuritis
Recovery from optic neuritis is associated with a change in the distribution of cerebral response to visual stimulation: a fMRI study
Functional magnetic resonance imaging of the cortical response to photic stimulation in humans following optic neuritis recovery
-A.J Thompson et al

MRI studies brain anatomy.Functional MRI (fMRI) studies brain function.
MRI vs. fMRI
Source: Jody Culham’s fMRI for Dummies web site

fMRI Setup
Source: Jody Culham’s fMRI for Dummies web site

% signal change = (point – baseline)/baselineusually 0.5-3%
initial dip-more focal and potentially a better measure-somewhat elusive so far, not everyone can find it
time to rise signal begins to rise soon after stimulus begins
time to peaksignal peaks 4-6 sec after stimulus begins
post stimulus undershootsignal suppressed after stimulation ends
Source: Jody Culham’s fMRI for Dummies web site
Hemodynamic Response Function

MRI vs. fMRI
neural activity blood oxygen fMRI signal
MRI fMRI
one image
many images (e.g., every 2 sec for 5 mins)
fMRI Blood Oxygenation Level Dependent (BOLD) signal
indirect measure of neural activity …
Source: Jody Culham’s fMRI for Dummies web site

The papers…
Both by the same authors and has similar experimental setups
The second paper is a follow up to the results presented in the first paper

Terms and Observations
Myelin: The fatty sheath coating the axons of the nerves; it allows efficient conduction of nerve impulses.
MS (Multiple Sclerosis): Demyelination of the CNS ON (Optic neuritis): An inflammatory disorder of the optic nerve that
usually occurs in only one eye and causes visual loss and sometimes blindness. It is generally temporary.
Temporary: Patients usually regain visual acuity after a period of time. Visual acuity: Sharpness or clearness of vision.
Measured using Snellen charts and Ishihara color plates.
Question: How is visual acuity regained? Given that ON is a common precursor to MS. (Implying that the optic pathways are probably irreparably damaged)

Hypothesis and Study
Possibility of cortical re-adaptation (functional reorganization)
Use fMRI to study patients who have recovered from ON.
Pick patients who had only one eye affected.
Match with equal number of normal subjects
Conduct additional structural scans and VEP (Visual Evoked Potential)
Interpret the fMRI analysis

fMRI experimental setup
1.5 T magnet One volume every 4 seconds, for a duration of 8 minutes (8*60/4 = 120) Each volume has a size 96*96*10 vox (2.5 mm in plane 5mm thick slices)
0 50 100 150 200 250 300 350 400 450 5000
0.5
1
1.5
2
Baseline
AcitvationRed 8hz photic stimulationto one eye 12 cycles of
alteration
5 volumes perstate

Preprocessing: Head motion correction Reference [9] of the first paper: Methods of Diagnosis and treatment
of stimulus-correlated motion in generic brain activation studies using fMRI
Find mean image of time series (base)
Minimize MAD (mean absolute difference) of each with respect to base
Realignment done using tricubic spline interpolation
Difference between SCM (Stimulus Correlated Motion) between the two groups was not significant. (Paper does not mention the actual values for them! ). Hence not accounted for in this study

fMRI data analysis: GBAMGBAM: Generic Brain Activation Map. Reference [13] :Generic brain activation mapping in functional magnetic resonance imaging: a non parametric approach.
Fit a model: Y(t) is the time course of a single
voxel (IMP: slice wise) w is fundamental frequency of
stimulus 2 harmonic components a+bt represents a linear trend rho(t) is the residual
rho(t) is usually a first order autoregressive process.
Pseudogeneralised lest squares fitting Reduce each time course to a single
value reflecting the power at fundamental frequency

fMRI data analysis: GBAM To check the hypothesis that a given
voxel FPQ value is determined by periodic experimental design, authors use Randomization testing Randomly permute the slices (of each
volume with corresponding slice location in another volume) of the time series to obtain 10 random time courses
Another paper asserts that the FPQ sampled this way is indistinguishable from a FPQ derived from image sequences when no stimulus is provided
Calculate the FPQ maps for each of these time courses
Generic analysis: Register these maps into the standard space (Talairach and Tournoux)
GBAM obtained by comparing medians
observed
randomized
Time series FPQ maps
observed
randomized
Subject 1
Subject 2
MedianFPQ maps
*Model fitting and registration
*

ResultsLeft: 3 selected slices for controls (A and B), unaffectedpatient eye (C) and ON affected patient eye (D)Bottom: Comparison of VEP delay in affected patient eye
Key observations: Extra occipital response and phase of this response

Results
The identified extra occipital areas are known to have extensive connections with the visual processing system
Unaffected eye also displayed extra cortical activation areas. Possibly due to clinically silent abnormality
During an episode of ON VEP amplitude decreases and latency increases. After recovery, amplitude more or less returns back to normal but latency persists
The result of reduced volume in the visual cortex correlates with previous studies
But did not report extra occipital response (due to methodological differences?)
Strengths the hypothesis of possible cortical reorganization
Results
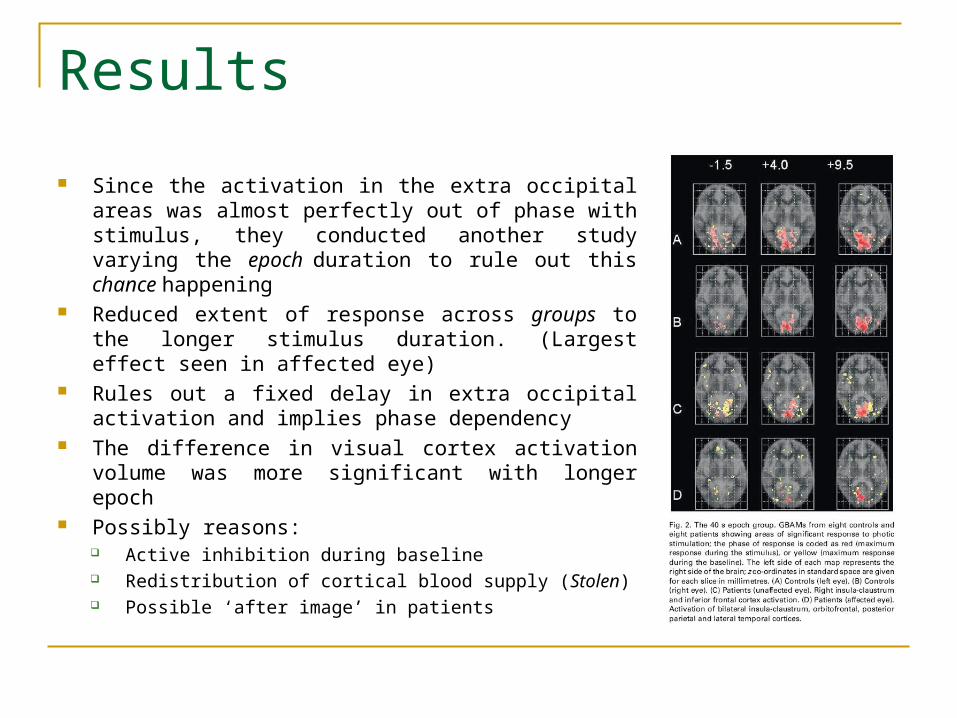
Since the activation in the extra occipital areas was almost perfectly out of phase with stimulus, they conducted another study varying the epoch duration to rule out this chance happening
Reduced extent of response across groups to the longer stimulus duration. (Largest effect seen in affected eye)
Rules out a fixed delay in extra occipital activation and implies phase dependency
The difference in visual cortex activation volume was more significant with longer epoch
Possibly reasons: Active inhibition during baseline Redistribution of cortical blood supply (Stolen) Possible ‘after image’ in patients

And….
Am Done…
Qs?







