Download - GENERAL MEDICAL SERVICES

GENERAL MEDICAL SERVICES
GENERAL PRACTICE MANAGEMENT GENERAL PRACTICE MANAGEMENT

Learning OutcomesUNDERSTAND:
The Scope of General Practice Management
The various means by which GPs are contracted
Key features of the Contractual and Partnership
Agreements and the Business Plan
General Practice funding streams

Important History of General Practice1948: Lord Beveridge, NHS is established, providing free health care for everyone
1952: College of General Practitioners is founded
1966: Family doctor charter facilitates payments for nursing staff and buildings
1976: Primary Care Act requires general practice principals to do vocational training
Mid 80s: Cost /Notional Rent Scheme, Practice Nurses and Practice Managers started to appear
1990: General practice contract – Health Promotion Clinics. Fundholding introduced
1997: New contract enables general practitioners to choose to be salaried rather than self employed Personal Medical Services. Money ran out
1999: Fundholding is replaced by Primary Care Groups and Trusts
2004: nGMS Contract - Doctors are allowed to stop providing out of hours care

Private trader at WorkBefore the 20th century general practitioners worked as private traders, treating patients only if they had the means to pay

Yesterday v Today 2 groups

GENERAL PRACTICE IS A BUSINESS
General Practice is a small people-centred business
The business is owned by the practice partnership
GPs are “independent contractors”

WHAT DO YOU EXPECT
THE PRACTICE MANAGER
TO KNOW
AND BE
CAPABLE OF DOING?

NES GPMVTS MENU for LEARNING LEARNING NEEDS ANALYSIS D
General Medical Services Contract (2003) Annex C: Competency Framework For Practice Management
Practice Operation and Development Risk management and assessment Partnership Issues Patient and Community Service Finance Human Resources Premises and Equipment IM&T Population Care

“IN A TIME OF TURBULENCE AND CHANGE, IT IS MORE TRUE THAN EVER THAT
KNOWLEDGE IS POWER”
Sir Francis Bacon and J F Kennedy

IMPORTANT DOCUMENTS to know about and use
• Practice GMS Contract
• Statement of Fees and Entitlements (SFE)
• NHS Circulars
• Partnership Agreement
GENERAL PRACTICE CONTRACTING ARRANGEMENTS
LOCAL ADMINISTRATION LEVEL:
◦ Scotland – PCO - Primary Care Organisations ◦ England - PCT - Primary Care Trusts ◦ Wales - HB - Local Health Boards
4 CONTRACTUAL METHODS:
◦ General Medical Services Contract (GMS) – (a new GMS contract has been in place since April 2004)
◦ Personal Medical Services agreements (PMS) ◦ Alternative Provider Medical Services (APMS), and ◦ Primary Care Led Medical Services (PCTMS).
A CONTRACT BETWEEN WHOM?
• Contract between a practice and a PCO– all practice partners will enter contract with PCO
• Individual practice contractual terms come from national “menu”


A PARTNERSHIP AGREEMENT • A contract between the partners and should be kept up to date at all
times in order to be valid and thus effective.
• Although an oral partnership is a valid one, it is not to be recommended.
• In a PARTNERSHIP AT WILL, relations between partners are governed by the Partnership Act 1890, unless some agreement to the contrary can be proved.
• The Partnership Act was designed to cover all partnerships and does not meet the specific needs of individual professions.

Partnership Act 1890.Some consequences of being a partnership 'at will';
• Any partner may dissolve it at any time with no formal procedure
• Death or bankruptcy of a partner will automatically dissolve the partnership
• No partner(s) has the right to expel another for any reason
• No partner(s) has the automatic right to carry on the partnership
• The assets will be frozen immediately on dissolution
• Staff will be made redundant on dissolution
• All partners are entitled to an equal share of the assets
• All partners have equal liability for the debts
• No new partner may be appointed without a unanimous decision
• All partners may take part in the management of the partnership

Partnership Agreements

Document Hierarchy

GMS CONTRACTPractice Based Lists
• Patients Registered with Practice not GP• New Patient Right to See GP of Choice
» Wait longer
• New Rules on Registering Patients» Clinician can refuse (violent patient) » Refer to another clinician if doesn’t provide service» New Rules Removing Patients

WHO are our PATIENTS?
Must provide primary medical services to the following:
REGISTERED PATIENTS & TEMPORARY RESIDENTS• provide appropriate ongoing treatment/care • including provision of advice re patients health
(including health promotion) and referral to other services.

IMMEDIATE NECESSARY TREATMENT
Must also provide primary medical services required in core hours for any person (to whom the practice has been requested to provide treatment) owing to accident or emergency at any place in practice area
This includes any medical emergency not just services provided under this contract.

THE CONTRACT “MENU”FIVE TYPES OF SERVICE
“Normal” services:
1.Essential
2.Additional
“ Supplementary” services:
1.Directed Enhanced2.National Enhanced3.Local Enhanced

ESSENTIAL SERVICES - MANDATORY
Practices must provide the following services during core hours (8am-6.30pm)
Management of its registered patients & temporary residents (TR) who are:(a) ill, or believe themselves to be ill, with conditions from which recovery in generally expected(b) terminally ill (c) suffering from chronic diseasedelivered in the manner determined by the practice in discussion with the patient.

ADDITIONAL SERVICES
• Normally expected of all practices but OPT-OUT possible
• These will mainly include services which are preventative:– CHS– Non-IUD contraception– Non-intra partum maternity– Childhood vaccinations and immunisations– Cervical screening– Curettage, cautery and cryocautery
OPTING-OUT Either:
• temporary (emergencies)• permanent (long-term problems)
PCOs and practices working togetherMaximum 9-month process
Alternatives – other practices, PCO, other providers e.g. walk-in centres
Money removed from practice global sum
Patient access to services protected
LIST CLOSURE process
DIRECTED ENHANCED SERVICES• OPT-IN for practice
• Obligatory for each PCO
• National specifications
• No one practice has to do but someone has to– Services to violent patients
– Childhood vaccinations and immunisations financial incentives
– Minor surgery
– Flu immunisations

NATIONAL ENHANCED SERVICES
OPT-IN - national terms and conditionse.g.
Anticoagulant monitoring IUCD Sexual health MSDrug and alcohol misuse Terminally illDepression Learning
disabilitiesIntra partum care Minor injuriesNear-patient testing Homeless Immediate/first response care

LOCAL ENHANCED SERVICES
OPT-IN
• Response to specific local requirements
• Local terms, conditions and standards
• Possibly, innovative services for piloting and evaluation

PaymentsHow can the practice income be increased?
3
Global Sum or
Minimum Practice Income Guarantee
Enhanced Services
Quality & Outcome Framework
Seniority & Other Payments eg maternity, sickness
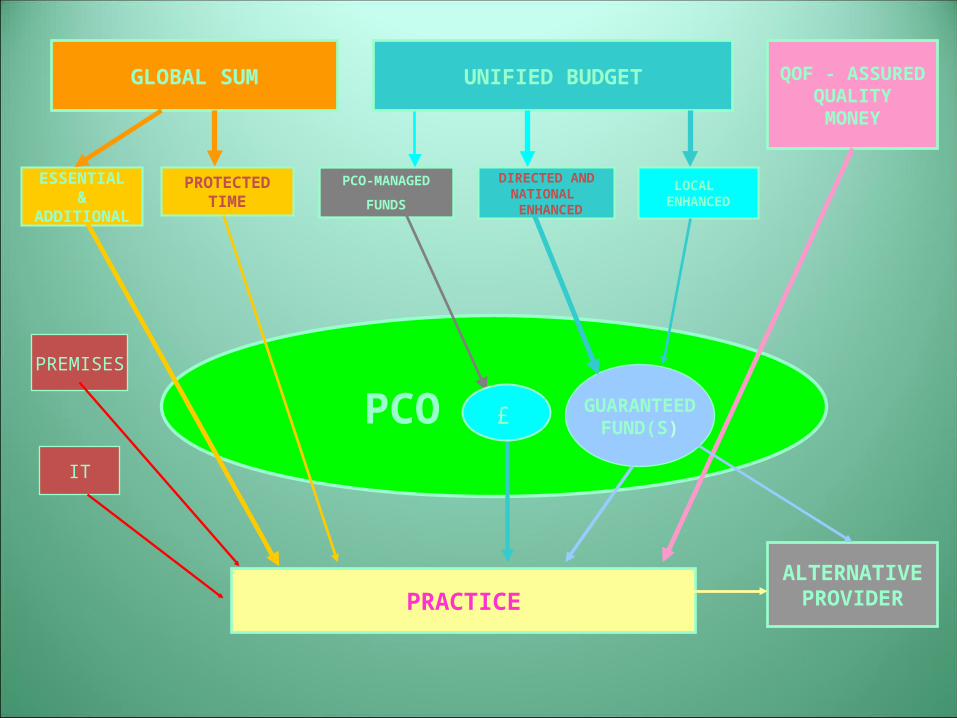
PRACTICE
GLOBAL SUM
PCO
UNIFIED BUDGET
ESSENTIAL&
ADDITIONAL
PROTECTEDTIME
DIRECTED ANDNATIONAL ENHANCED
LOCAL ENHANCED
GUARANTEEDFUND(S)
QOF - ASSUREDQUALITYMONEY
ALTERNATIVEPROVIDER
PCO-MANAGED
FUNDS
PREMISES
IT
£
2011-2012 GMS CONTRACT AGREEMENT
Practice Expenses
For 2011-12, in order to reduce the risks of a further net pay cut for GPs, we have agreed to an increase to the overall value of GMS contract payments by 0.5 per cent, to support practices in meeting the costs of increased expenses, including the pay award for employed staff with a full time equivalent salary of less than £21,000. This increase will be delivered in through a 2.53 per cent increase in the value of a QOF point from £127.29 to £130.51.
This increase in the value of a QOF point is intended to deliver the full 0.5 per cent expenses increase agreed with NHS Employers.
Increased expenses – no reimbursement for Commercial waste disposal

BUSINESS PLANNING“Alice's Adventures in Wonderland”
Alice comes to a fork in the road and asks the cat:
• “Would you tell me, please, which way I ought to go from here?”
• “That depends a good deal on where you want to get to”, said the Cat.
• “I don't much care where”, said Alice.
• “Then it doesn't matter which way you go”, said the Cat.
Rudderless, haphazard, reactive, poor communication and teamwork

BUSINESS PLANNeeds:
• People – Personnel & Patients• Organisational • Operational
Plan:• Vision and the Mission• Practice Profile• Running the Business• Finance
ACTIVITYThe Practice Merger
The Task
In groups of 5-6, consider the scenario
Before commencing the exercise, nominate a spokesperson and
a scribe.
You have 20 minutes to brainstorm the issues
You are not expected to solve the problems but to identify the
issues
The issues may be suitable tutorial topics







