Download - Headaches and Children - umem.org

Headaches and Children
Mimi Lu, MD, FAAEM Clinical Assistant Professor
Assistant Residency Program Director
Director, Pediatric Emergency Medicine Education
University of Maryland School of Medicine
Baltimore, Maryland
No relevant financial disclosures


Headaches and Children
Mimi Lu, MD, FAAEM Clinical Assistant Professor
Assistant Residency Program Director
Director, Pediatric Emergency Medicine Education
University of Maryland School of Medicine
Baltimore, Maryland

Outline
Meningitis
Trauma
Migraines
Questions? [email protected]
For a PDF copy of all slides, go to:
lectures.umem.org/AAEM [will be posted after AAEM for 1 month]

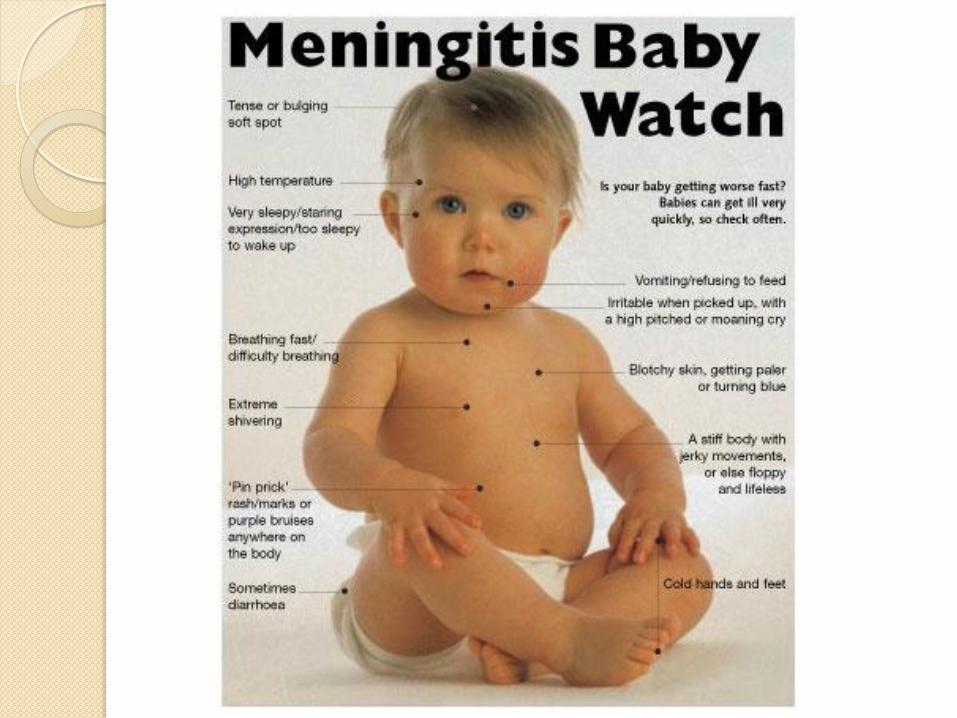
Meningitis

McAbee, Pediatrics 2008

McAbee, Pediatrics 2008

McAbee, Pediatrics 2008

McAbee, Pediatrics 2008

Epidemiology
Historic lows in the U.S.
Highest among infants < 1 year
Decreasing incidence and mortality
N meningitidis serotypes B, C, Y
Vaccines not routine
Castelblanco, Lancet Infect Dis, 2014
MacNeil et al, Pediatrics, 2015

© 2014 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.
2
Acute Meningitis in the Pediatric Emergency Department: Diagnostic Yield of Procalcitonin and C-Reactive Protein.
Casado, Pediatr Emerg Care, 2014

CT before LP
New seizures
Altered mental status
Immunocompromise
Papilledema
Focal neurologic signs
LP pearls
Local anesthetic
◦ Kaur, Arch Pediatr Adolesc Med, 2003
Early stylet removal
◦ Baxter et al, Pediatrics, 2010
◦ Nigrovic, Ann Emerg Med, 2007
Positioning
◦ Abo et al, Pediatrics, 2010
◦ Hanson et al, Pediatr Emerg Care, 2014

Meningitis treatment
Anti-infective agents
◦ Ampicillin (100 mg/kg) + cefotaxime (50 mg/kg)
in neonates
◦ Ceftriaxone (100 mg/kg) infants >1 month of age.
◦ Vancomycin if streptococcal infection is
suspected (e.g. cloudy spinal fluid).
◦ Add acyclovir if neonate, focal seizure

Steroids in meningitis
Beneficial effect in acute bacterial meningitis
◦ Reduction hearing loss
◦ Reduction short-term neurologic sequelae
◦ Reduction in mortality for S. Pneumo
High-income countries
Before or after antibiotics
Mongelluzo, JAMA, 2008
Brouwer et al, Cochrane Review. 2013

Meningitis pearls
Toxic patients should have antibiotics
administered as soon as possible.
Do not withhold antibiotics for LP or CT
LP all febrile neonates
Strongly consider LP for children 1-2 months of
age who are to be given antibiotics for another
reason

Meningitis pearls
Simple febrile seizures do NOT require CT or
LP unless history or physical exam directs
otherwise
◦ concern for non-accidental trauma
◦ localizing neurologic findings
Complex febrile seizures probably do not
require “routine” work up, especially if due to
recurrence

Meningitis pitfalls
Beware atypical presentations
◦ Previous antibiotics
◦ Immunocompromised
incompletely immunized
◦ Complex febrile seizure
◦ Afebrile
Do not rely on WBC to decide on LP
◦ 50% normal

Meningitis pitfalls
Describe general appearance
Beware “age-appropriate” and “nonfocal”
Physical exam limited reliability in infants
◦ Minority present with meningeal irritation
◦ Paradoxical irritability

Head Injury

Case
8 yo male head injury
VS: HR 96, RR 18, BP 110/85, 97%
Exam: awake, alert
◦ LOC?
◦Vomited?
15 mo
HR 130, RR 26, BP 75/40, 97%

PECARN vs CATCH vs CHALICE
Conclusion:
Physician practice and PECARN identified
all clinically important traumatic brain
injuries
Easter et al, Ann Emerg Med, 2014

Kupperman et al, Lancet, 2009
Age < 2 years

Kupperman et al, Lancet, 2009
Age ≥ 2 years

Image gently

Case
8 yo male head injury
VS: HR 96, RR 18, BP 110/85, 97%
Exam: awake, alert
◦Ondansetron?

Ondansetron?
Sturm et al, AJEM, 2013
Retrospective cross-sectional study
Lower likelihood of 72 hour return
Use: no effect on admission or returns
Rx: no effect on returns or readmissions

Ondansetron and head injury
Conclusion:
Ondansetron did not mask symptoms and
decreased return visits to ED in children
who underwent CT and were discharged
home.

Hypertonic saline
Lumba-Brown et al, Pediatr Emerg Care, 2014
◦ Prospective, randomized, blinded
◦ Self-reported pain
Conclusion
◦ Three percent HTS more effective than NS in
acutely reducing concussion pain


Migraines
Post-traumatic headaches
Leung et al, Headache, 2013
◦ Retrospective
◦ 14 days of ED visit
◦ IV migraine therapy
ketorolac, prochlorperazine, metoclopramide,
chlorpromazine, and ondansetron
◦ Reduction of post-traumatic headache
Leung et al, Headache, 2013

Migraine cocktail?
NS, ketorolac, prochlorperazine,/
metoclopramide, diphenhydramine
Conclusion:
Standardized combination therapy is
effective for acute pediatric migraine
therapy in the ED
Reduces headache pain scores, length of
ED stay, and hospital admission rates.
Leung et al, Headache, 2013

Opioids
DeVries et al, J Adolesc Health, 2014
◦ 46% received opioids
◦ 48% Rx opioids during follow up
◦ 29% received > 3 Rx opioids
Conclusion:
◦ A large proportion of adolescents with headache were prescribed opioids.
◦ ED visits were strongly correlated with opioid prescriptions.

Retrospective ED
32,124 children with migraines
Medications
◦ Nonopioid analgesics 66%
◦ Dopamine antagonist 50%
◦ Diphenhydramine 33%
◦ Ondansetron 21%
◦ Triptans and opiates 3%
Bachur et al, Pediatrics, 2015

Results
◦ Metoclopramide 31% increased odds for ED
revisit vs prochlorperazine
◦ Diphenhydramine + DA antagonist 27%
increased odds vs DA antagonist alone
Bachur et al, Pediatrics, 2015

Summary
Early antibiotics and steroids in meningitis
Symptom control for post-traumatic HA
◦ Ondansetron
◦ Hypertonic saline
Symptom control for migraine
◦ Avoid opioids!
◦ Diphenhydramine ?
◦ Prochlorperazine over metoclopramide

Questions?
For a PDF copy of all slides, go to:
lectures.umem.org/AAEM [will be posted after AAEM for 1 month]







