
Hemiplegic Foot
in Children and Teenagers:
When to consider surgery?
Antoine de Gheldere, MD
Consultant in Children’s Orthopaedics and Trauma
GNCH – Royal Victoria Infirmary
Newcastle upon Tyne, UK
Peacocks meeting, Saturday 9th January 2016

3 principles to remember
1. Nobody can cure Hemiplegia (CP)
2. A “neurological deformity” doesn’t get
better with the growth
3. The foot is in continuity with the leg

Common Gait Patterns

Motor Cortex Lesion

Motor Cortex Lesion

Common Hemiplegic
• Walking (GMFCS 1 or 2)
• Distal disorder (hand and foot/ankle)
• Weak ankle extensors (dorsal flexion)
• GCS/S increased tone

Natural History
Worsen without treatment

Worsen without treatment
Natural History
EQUINUS (Triceps tone ++)
Plano-valgus (Talus subluxation)
Cavovarus (TP/TA tone ++)

Reasons for referral
• Gait difficulty: foot – knee – hip – trunk
• Foot pain/discomfort
– Medial or Lateral
– Fixed deformity
– Bunion (teenagers)
• Instability (teenagers)

Clinical Assessment (1)
1st Question: How is the foot position?
• Static
• Dynamic

2nd Question: How many joints affected?
• Knee, hip, trunk, (upper limb)
• Dynamic deformity (spasticity)
• Video recording or gait analysis
Clinical Assessment (2)

3rd Question: Active foot control?
• Selectivity
• Foot “balance”
• Weak agonist vs. antagonist contracture
Clinical Assessment (3)

Active force
Spasticity
Contracture




• Physiotherapy
• Orthotic
• Botulinum toxin
• Serial cast
…
• Surgery
Treatment options

Surgical Indications
• Fixed deformity
• Uncomfortable flexible
deformity
• Compensation deformity
• Gait deterioration
“Do not wait the end of the growth”

Type of Foot Deformity
Equinus: 35%
Cavovarus: 35%
Planus: 12%
Valgus: 6%
Bunion: 12%
Planus Valgus
Equinus Cavovarus

Equinus
Normal initial contact
- Foot in neutral position
- 30 degrees with ground
No more Achilles lengthening!

Normal foot
1st Rocker = Heel
Ex moment = PF
Tib Ant
Eccentric
Absorb impact
2nd Rocker = Ankle
Ex moment = DF
Soleus
Eccentric
Ankle trunk forward
3rd Rocker = Toes
Ex moment = DF
GCN
Concentric
Propulsion


Cavovarus
• Triceps (GCN/S) tone ++ or contracture ?
• Weak DF: TA? EDL? EHL?
• TA or TP ?
• Weak Peronei ?

E (girl), 10yo.
Cavovarus deformity
(+supination)

+5 years
Split TB to PB
GCN lengthening
Calcaneus VgO
M1 closing wedge

H (girl), 8yo.
Cavovarus deformity
(+ADD)

+4 years
Split TP to PB
Calcaneum VgO
C1 open wedge

Planovalgus
MILD PV
• Similar to idiopathic
SEVER PV
• Similar to diplegic
• Work on the bone!

J (boy), 9yo.
Planus deformity (mild)

+3 years
Calcaneum open wedge
GCN lengthening
TP shorthening
TN joint repair

J (boy), 9yo.
Planus deformity
External rotation
Genu valgum

+2 years
AA medial derot. O.
Calcaneus double O.
GCN lengthening
PB lengthening
TP shortening
TN capsule repair

Teenagers Hemiplegic Foot
Problem No.1: Doesn’t like splints
• Stretching self-teaching (gym)
• Shoe compensation
– “high heel”
– Boots
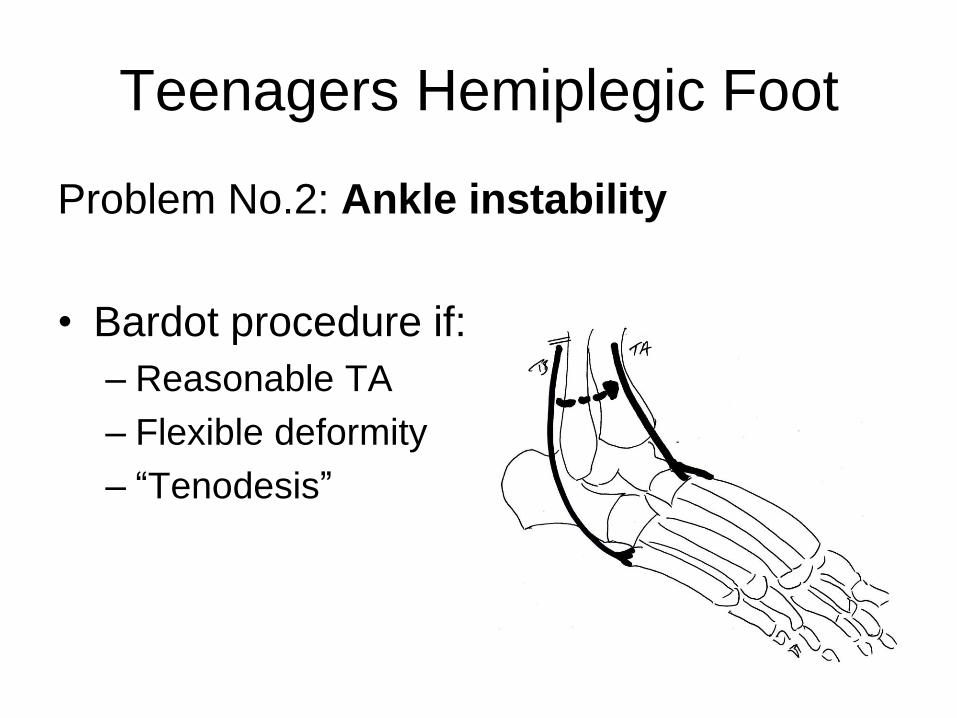
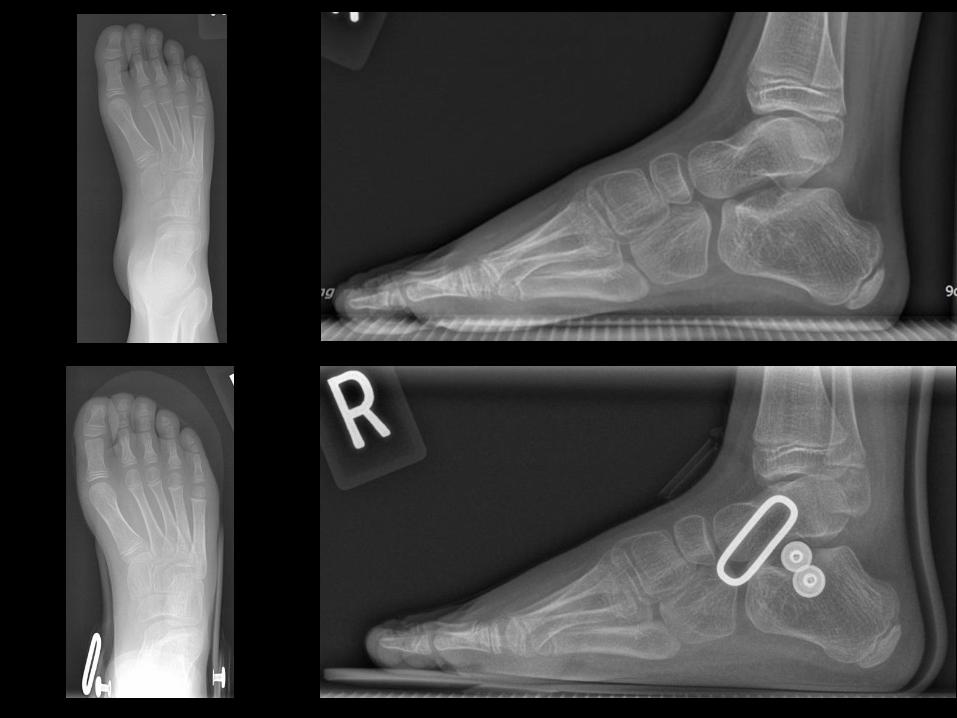
Teenagers Hemiplegic Foot
Problem No.2: Ankle instability
• Bardot procedure if:
– Reasonable TA
– Flexible deformity
– “Tenodesis”

Bunion – Hallux Valgus
• More frequent with planovalus foot
• Osteotomy and ADH release
• Aim M1P1 at 0
• Fusion only if (symptomatic) failure

D (boy), 12yo.
Hallux Valgus (mild)

+3 years
M1 osteotomy
P1 osteotomy
PM1 lat. Hemi-epiphysiodesis

Take Home Message
• Conservative treatment first
• Don’t wait end of growth for surgery
• Understand the deformity
• Avoid fusion
• Osteotomy(ies) and soft tissues








