
How to perform epicardial ablation of VT
Richard SchillingSt. Bartholomew’s Hospital
London, UK

Why epicardial ablation of VT?
Koa-Wing et al JCE 2007

Epicardial approaches
• Transarterial (ethanol)• Tranvenous (Coronary sinus)• Transpericardial

Epicardial Guide Wire Mapping
• Used with ethanol or venous ablation
• Useful for identification of target vessel

Ethanol ablation - Region identified with conventional
catheter

Relevant vessel identified at angiography

Guide wire mapping

Guide wire mapping

Balloon inserted into vessel
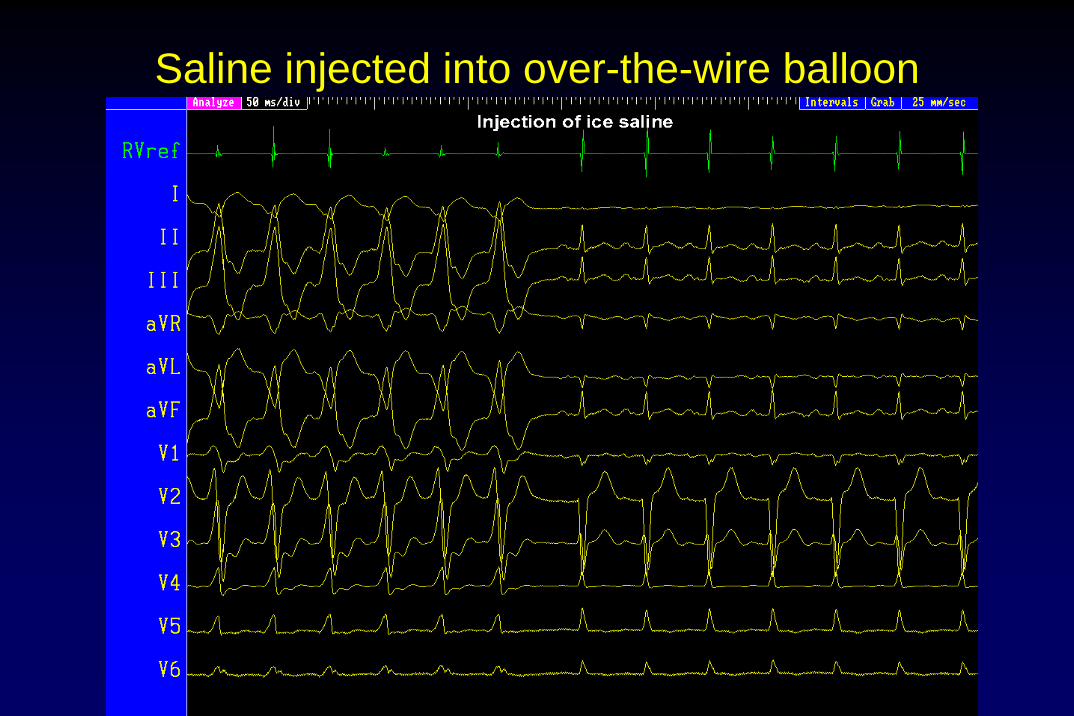
Saline injected into over-the-wire balloon
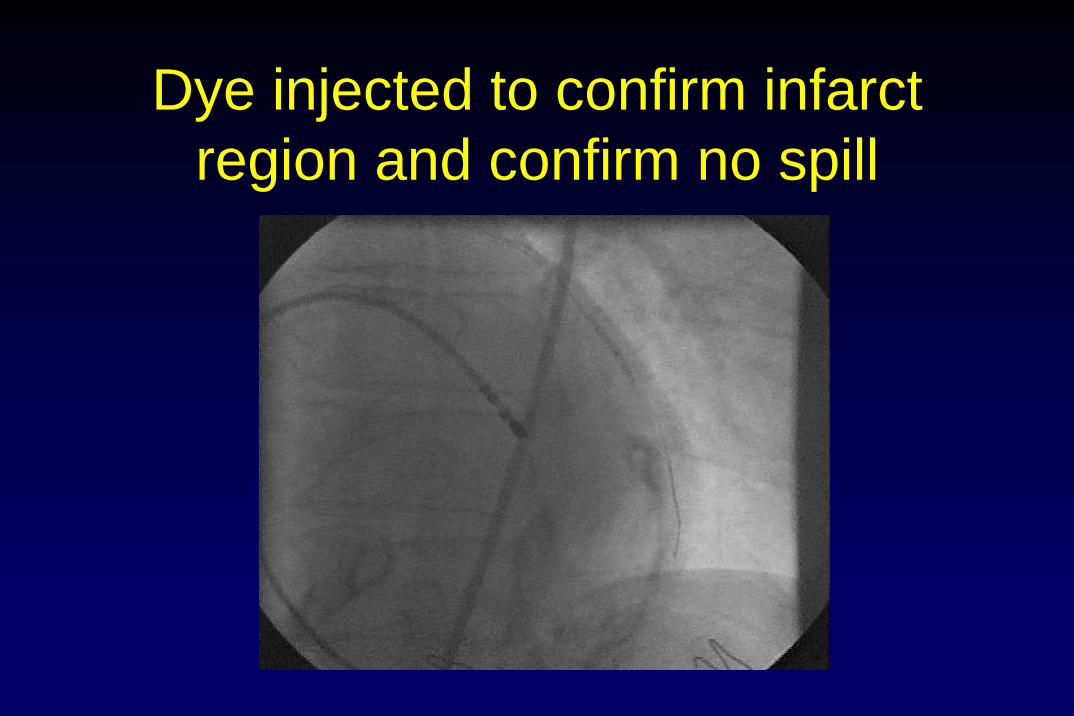
Dye injected to confirm infarct region and confirm no spill
Post op
• CK 300• 6 minutes on ex test no VT off drugs• EP study no VT• Discharged well no further VT

Transvenous ablation

Epicardial - transvenous

Epicardial - transvenous

Epicardial - transvenous

Transpericardial Technique - Best endocardial position
• punctures -heparinisation
• Puncture site adjusted to region of interest
• Obesity• Post-surgical patients
fail if not inferior origin
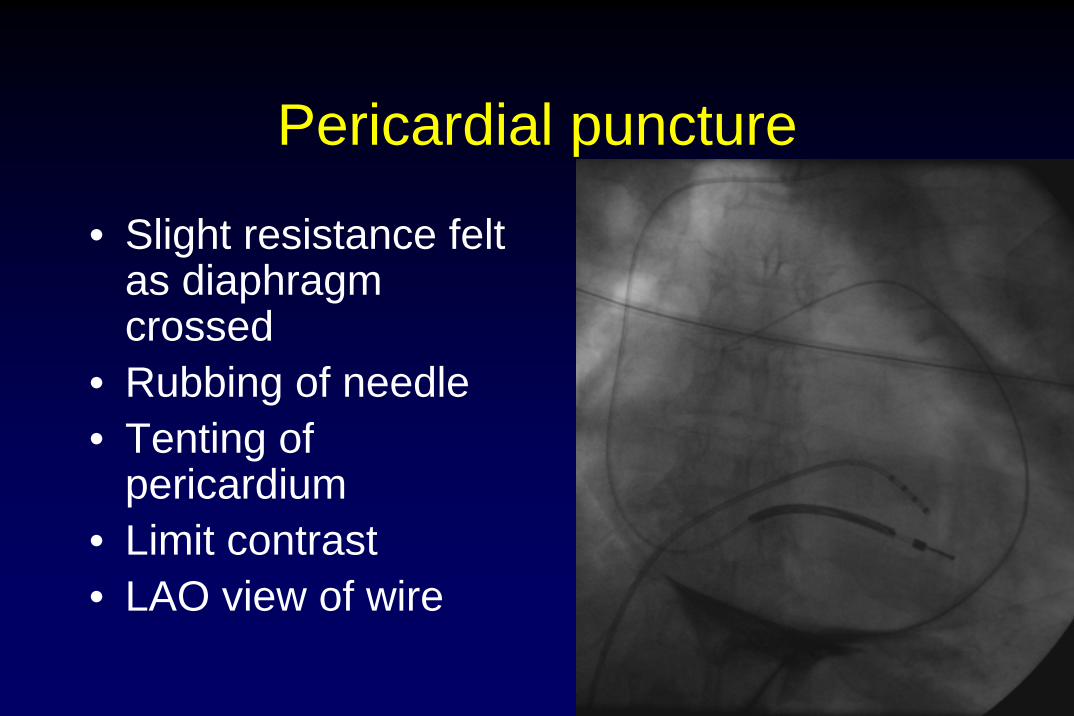
Pericardial puncture
• Slight resistance felt as diaphragm crossed
• Rubbing of needle• Tenting of
pericardium• Limit contrast• LAO view of wire

Pericardial mapping

Complications of epicardial approach8% RV perf and haemopericardium
Sosa et al JACC 2000
0% Cesario Heart Rhythm 2006
6% transient pericarditis
Schweikert et al Circ 2003
5% transient pericarditis
Personal data
Coronary vessel puncture/transient bleeding
Tedrow et al JCE 2009
Pericardial access
• May be limited in redos• Not usually a problem in post MI• Usually not worth trying in post CABG

NICE Guidelines
• No review by advisors prior to publication• Procedures should only be carried out in
units with cardiothoracic surgery

74 yr male frequent ICD shocks
• VT1 – clinical VT– Tolerated– ATP accelerated– Terminated and
non-inducible after RF at first procedure

• VT2 repeatedly induced at first procedure
• Poorly tolerated• ATP unreliable

Second ablation attempt
• VT1 endocardial mapping

Site of RF1

VT1 endocardial RF1

VT3 induced - Epicardial site

Myocardial thickness

RF 2 epicardial VT3 to VT4 390 to 330 ms

VT4 recurrently initiated and poorly tolerated
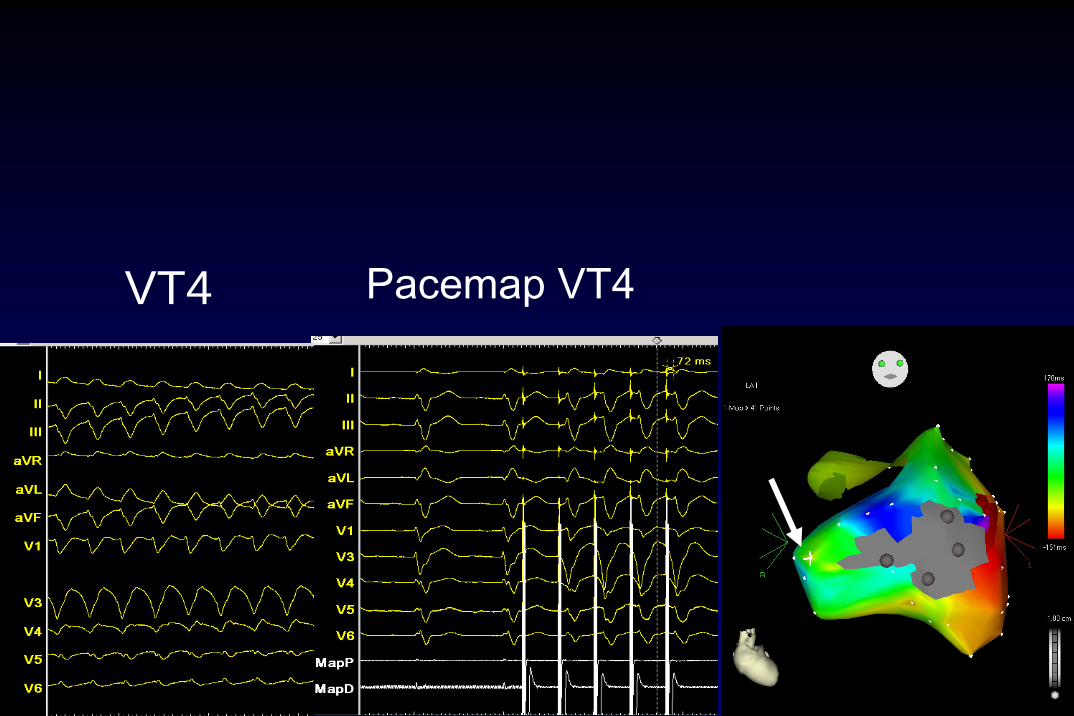
Pacemap VT4VT4

Pacemap poor match for VT4

VT 4 non-inducible

18 year old incessant
• Endocardial
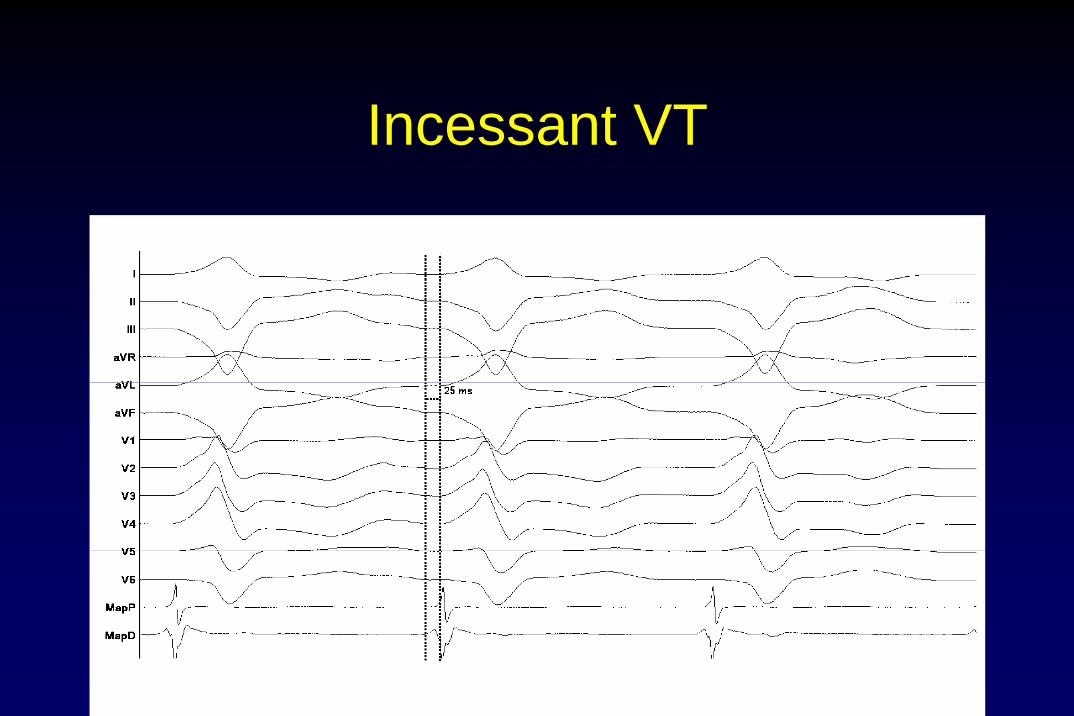
Incessant VT

18 year old incessant VT

Barts VT protocol

Conclusions
Epicardial ablation possible from a number of approachesProbably necessary in 10% of VT (higher in DCM and idiopathic)Safe but requires experience







