Download - I M lec #3

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 1/25
1 | P a g e
-

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 2/25
2 | P a g e
Dr Musa Almakawi
-COPD
In the name of Allah the most gracious and merciful.
Today we’re going to talk about COPD. Before starting the lecture,
COPD is smoke related disease, probably 85 % of COPD patients are
smoker ( this is in west) But in Jordan, It might be 90% or 95% becausehere we don’t have mining or other industrial exposure.
Smoking Related Death
In a worldwide, it is about 5.4 millions per year, one death every
seconds due to smoking, out of this amount, there are 1.7 millions died
due to Cardiovascular Diseases (CVD), 1 million due to COPD, and
80,000 due to lung cancer. In United States, about 443,000 died every
year because of smoking.
Smokers generally die 15 years earlier than non-smoker. So if anyone of
you smoking, you have to take back this survival rate point as
consideration . And a diabetic patients usually die 10 years earlier
compared to non-diabetic patients. So, a smoker die earlier than adiabetic patient.
Chronic Obstructive Pulmonary Disease (COPD)

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 3/25
3 | P a g e
Chronic Obstructive Pulmonary Disease (COPD) it means that there is
an airway obstruction and chronic disease. It comprises of 2 diseases,
and we’ll start by definition,
COPD is a disease state characterized by airflow limitation or airflow
obstruction that is not fully reversible ( DD: Bronchial Asthma - Chronic
Obstruction but reversible with Tx. Majority of them have normal
pulmonary function, they can lead a normal life) and it usually
progressive (DD: Bronchial Astma – Intermittent) and associated with
abnormal inflammatory response of the lungs to noxious particles or
gases (from cigarette). It is preventable and treatable but not cureable.There is Tx to reduce the symptoms indicated because the disease is
irreversible, you cannot return the patient into normal after tx. The Tx
is usually a symptomatic treatment. It gives some quality of life, but It
cannot be cured.
So we have two type of COPD which is
1) Chronic Bronchitis
2) Emphysema (Both are smoke related)
Chronic Bronchitis is defined clinically by the presence of cough and
sputum production for at least 3 months in each year for two
consecutive years without underline lung disease for example to those
who have (5.33) will have cough and sputum but this is not COPD.
When you have a patient that have a chronic bronchitis but he don’t
have any obstruction in airway. This is not COPD, He does have the
symptoms but the pulmonary function is normal. So to diagnose COPD,
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 4/25
4 | P a g e
you have to check pulmonary function regarding any obstruction in
aiwarys.
The other disease is Emphysema, which is a permanent airspaceenglargement beyond the terminal bronchioles with destruction of
alveolar septa.
If you go back to anatomy of bronchiole tree, you have conducting
airways starting from trachea down to 17 generations because each
one in a dichotomous way , will give two branches. This is a conducting
airway from here to here. And this is the part where Chronic Bronchitisusually occur. But majority of inflammation happen small airways
which are about 2mm of diameter. While emphysema is related in
transitional and respiratory zone (including some part of terminal
bronchioles until alveolar sacs) where the gas exchange unit started. So
in Emphysema, it is the destruction of alveolar wall, while Chronic
Bronchitis is the inflammation of conduting airways.

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 5/25
5 | P a g e

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 6/25
6 | P a g e
Comparisons between Asthma and COPD
COPD in USA
Asthma
• Caused by SensitizingAgent(Grass pollen, tree polen,animal fur)
• Inflammation:--CD4+ T Lymphocytes
- Eosinophils (goodresponse towards steroideither inhale or systemic -good in tx)
• Completely / Partiallyreversible
COPD
• Caused by Noxious Agent( toxin in smoker)
• Inflammation:--CD8+ Lymphocytes- Macrophages
-Neutrophils ( no responsetowards steroid- difficult intx)
• Completely irreversible
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 7/25
7 | P a g e
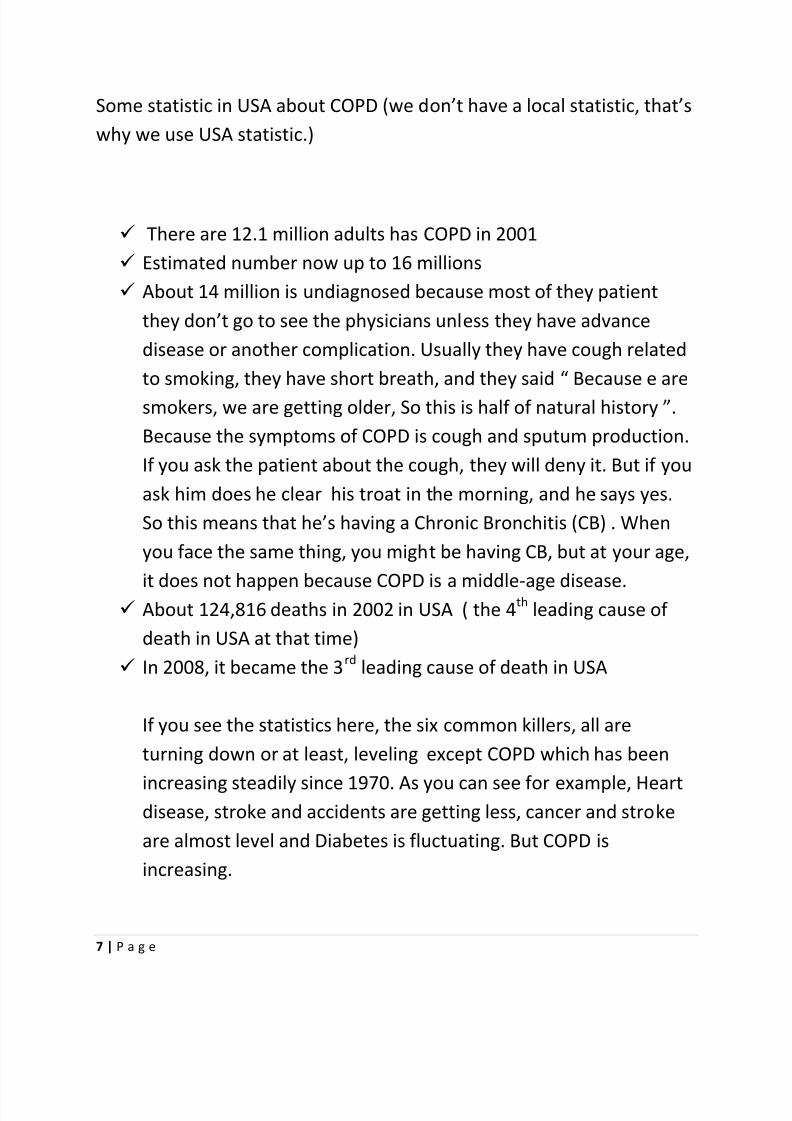
Some statistic in USA about COPD (we don’t have a local statistic, that’s
why we use USA statistic.)
There are 12.1 million adults has COPD in 2001 Estimated number now up to 16 millions About 14 million is undiagnosed because most of they patient
they don’t go to see the physicians unless they have advance
disease or another complication. Usually they have cough related
to smoking, they have short breath, and they said “ Because e are
smokers, we are getting older, So this is half of natural history ”.
Because the symptoms of COPD is cough and sputum production.
If you ask the patient about the cough, they will deny it. But if you
ask him does he clear his troat in the morning, and he says yes.
So this means that he’s having a Chronic Bronchitis (CB) . When
you face the same thing, you might be having CB, but at your age,
it does not happen because COPD is a middle-age disease. About 124,816 deaths in 2002 in USA ( the 4
thleading cause of
death in USA at that time) In 2008, it became the 3
rdleading cause of death in USA
If you see the statistics here, the six common killers, all are
turning down or at least, leveling except COPD which has been
increasing steadily since 1970. As you can see for example, Heartdisease, stroke and accidents are getting less, cancer and stroke
are almost level and Diabetes is fluctuating. But COPD is
increasing.
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 8/25
8 | P a g e
Not only that, By gender, in female, the number of death due to COPD
you are catching up males by years statistically. The reason that even in
the west, during 60s and 70s female were not accepted to smoke. Only
males who usually smoke during the era but not for females. However,nowadays thing are different, females are also participating in smoking
like males causing the rates between both are similar. The prevelance
of smoking in males are getting down while females are getting up, and
now they are equal. That’s why, mortality of male and female in year
2000 are similar.
The risk factor for COPD especially in Jordan like I said, is caused by
1. smoking MOSTLY (90%) 2. Some host factors (Less than 1%)
- Rarely they have alpha-1 antitrypsin/alpha-1 antiprotease
deficiency (It is inherited). Usually they have emphysema but
quite different from smoker related emphysema by havingsymptoms at early 40s. But if they smoke, and have alpha-
1antitrypsin deficiency, they would have symptoms at their early
30s. If they are non-smoker, there is replacement for alpha-1
antitrypsin. - It might also cause by airway hyperresponsiveness which is a main
feature of asthma. The airway is constricted due to response
against non-specific stimuli like histamine or methacoline. Forsmoker, the chance of COPD is higher.
- Lung growth. Those who has a lung infection during neonatal
period or childhood period, the lung wouldn’t grow properly, and
smoking at the same time, are tend to have COPD.

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 9/25
9 | P a g e
3. Exposures - The most important thing is, tobacco smoke is the major factor of
COPD. And this is in our hand, If we stop smoking, we’ll stop COPD
and other diseases. Even if you escape COPD (not all smokershave COPD about 20% ), you might have lung cancer, coronary
disease, and other problems - Occupational- Working outdoors like Farming and mining may
expose you to COPD.
- Indoor and outdoor air pollution, - Infections - Socieconomic status- Poor people tends to have COPD more than
rich people as rich people usually buy and eat fresh fruits and
vegetables which act as antioxidants. But it doesn’t mean that
you smoke and take antioxidants you can escape COPD. Some
poor people tend to spend their money more in cigarette rather
than feeding. In the west, they are usually poor, they smoke
and take alcohol and also poor nutrition, which mainly cause
COPD.
Prevalance in Jordan
Statistic In Jordan, this was during 2007, for adults above age 18
years old, there were 49.6% Males smokers and 10.5% Females
smokers (this is quite not true because female smoker tend to
hide their habit of smoking). Even in University Street, you can see
many people smoking and also Shisha-ing (aragella) along the
street.
For school children (13-15 years), In 1999, a study was done,

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 10/25
10 | P a g e
saying that 25% of males are smoker as well as 10.5% of females.
But they’re an experiment smoker (which means they’d tried
smoke once or more-not like regular smoker). This is the problem
usually once when they try to smoke cigarette for the first time ,they will start get addicted.
In 2007, the prevalence increased, as males smoker became 37%
while female smokers 26%. In the west, prevalence of smoker is
decreasing by year nowadays, but not in third year country like
Jordan which is increasing. Last year, it was the first time in United
States, for the prevalence of smoking becoming less than 20 %which is about 19%. But In Jordan, you can see about 80% of
physicians are smoker, especially anesthetist and surgeons. And
our hospital for example, I’m sure more that 80% of anesthetist
and surgeons are smoker. And in medical department, we have 50
members, only one is smoking .
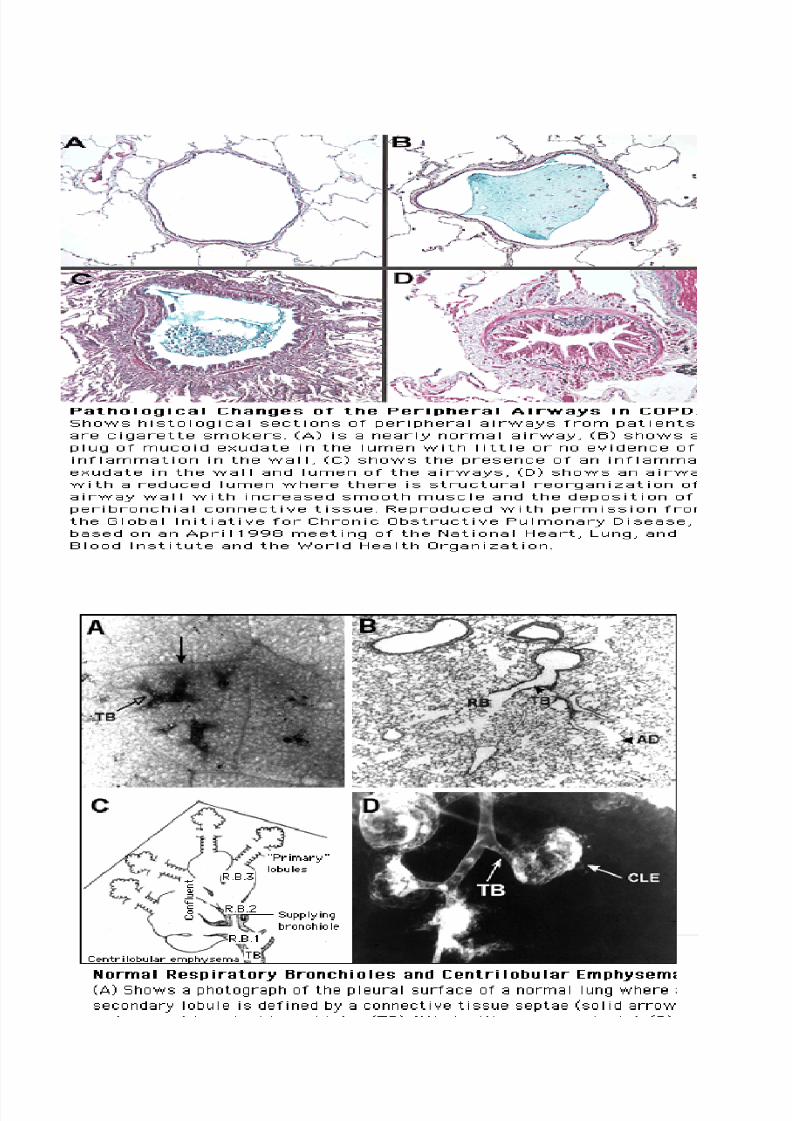
Pathology and Pathogenesis
As you said, the COPD, the main things is the airway obstruction,
the cough and sputum production. Why do we cough? Because
toxin in tobacco smoke leads to hypertrophy of the mucus
secreting lung if you remember histology of airways there are
lined by pseudostratified ciliated columnar epithelium and you
have mucous gland. As you go down, you’ll get Goblet Cell in the
smaller airways, there is hypertrophy in goblet cell and secreting
mucous gland. And the toxin leads to inhibition of ciliary function,
which have an important function as I said bronchiole tree is lined
by pseudostratified ciliated columnar epithelium and these cilia,

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 11/25
11 | P a g e
they beat in an ordinal manner from down to up, about 30
beats/second, as to propel the mucous and irritants that go down.
So the toxin from smoking will inhibit the ciliary function which
cause the production of sputum and cough. The airflow limitation & Hyperinflation (Because the destruction
of alveolar septa , that leads to shortness of breath) If the patient has emphysema that will affect gas exchange unit,
because the conducting airways has nothing to do with gas
exchange of Oxygen and Carbon Dioxide. But in emphysema,
you’ll have pulmonary hypertension that leads to hypoxia, that
might cause cor-pulmonale (right ventricular hypertrophy) with or
without failure of secondary disease. And they might end with
respiratory failure.
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 12/25
12 | P a g e
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 13/25
13 | P a g e
Diagnosis
Clinical features
As clinical problem we go for clinical symptoms and signs in thepatient. Anyone who is middle age and he has chronic cough,
sputum production or shortness of breath(Dyspnea) and if he has
risk factors we have to consider COPD. Example of risk factors are
smoker or occupation( job that deal with highly exposure to irritants
or chemicals)
And as I said the cough, we ask the patient in early morning did they
cough and clear their throat . This cough of COPD and this usually
above 40 years old of age if he is younger than that, probably you
think of other like bronchial asthma although he is a smoker.
Q: does the cough occur only in early morning?
Not necessarily but usually started in the morning but they can
cough at anytime. Bcoz probably during sleep the mucus secretion
increase it retain there and they are not conscious so the mucus
start to accumulate and they start coughing to clear their airways.
We have two types of COPD
Chronic Broncitis(Blue Bloaters)- usually this patient have cough
and sputum production especially obese patient. Typical history
that this obese is a smoker and he will tell you that he start to
have cough and sputum production. If they have cold in winter
they have more shortness of breath , cough and sputum
production usually stay for 3 or 4 days and these symptoms can
goes ten days or two weeks later on they start having shortness

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 14/25
14 | P a g e
of breath and coughing all day around. And they are called Blue
Bloaters bcos they have the tendency to have cyanosis.
Emphysema(Pink Puffers)-usually they have very thin airways but
they don’t have cyanosis instead have worst shortness of breathalthough they are maintaining their oxygenation and their lungs
are hyper inflate
These are the extremes but majority of patients they have emphysema
and chronic bronchitis at the same time if both are smoker related
If you suspect a patient to have COPD, we have to comfirm bcoz as we
said he might have emphysema without COPD, or he might have
chronic bronchitis without COPD. Bcoz COPD means chronic
obstructive airways disease so we have to demonstrate that there isairways obstruction, and the only way to determine it is by doing
Pulmonary Function Test . We measure it by calculating Force
Expiratory Volume of the first second(FEV1) / Force Vital Capacity (FVC)
ratio. Normal people if you take a deep breath and you exhale

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 15/25
15 | P a g e
forcefully most people they can exhale about 80% or more of their
vital capacity in the first second, these people(patients) bcoz they have
airways obstruction, they cannot expel that amount so the FEV1/ FVC
is less than 70%.
So all COPD they have this ratio reduce, the FEV1 have absolute value
is variable according to the severity of the disease. If we measure the
airways resistance it is increase bcoz by logic if we have narrow airways
the resistance in that airways will be higher. The total lung capacity is
increase. The residual volume, which is the amount of air remains afterforce expiration normally there’s 20% of total lung capacity remained .
But this patient might have 30% or 40% or more.
The Diffusion capacity which is a measurement across the gas
exchange unit that will differentiate a patient to have COPD of
Emphysema or Chronic bronchitis. The ratios is reduce, the FEV1 isreduce, there is increase airway resistance, total lung capacity is
increase especially in emphysema but even chronis bronchitis have but
more to emphysema, the residual volume is increase but more in
emphysema, while in diffusion lung capacity in chronic bronchitis is
normal, while in emphysema it is reduce bcoz the diffusion capacity it
measure the gas exchange across the gas exchange unit and chronic
bronchitis we said is a disease of conducting airways has nothing to do
with gas exchange. While emphysema is a disease of gas exchange unit
which is started after the terminal bronchioles, the respiratory
bronchioles, the alveolar ducts and the alveolar sacs.

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 16/25
16 | P a g e
So you have an airways obstruction with the reduce diffusion capacity.
Pic A
Usually we measure the diffusion capacity of carbon monoxide this
means that predominantly an emphematous patient.
Pic B
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 17/25
17 | P a g e
Pic C
The above Pic A is example of normal graph of spirometry . We look for
the first three parameter, the sex of the patient, the height and the age.
The computer will tell you what are the predictive value or PRED(third
line from the table) for that person. Usually we do spirometry
before(PRE-RX) and after using bronchodilator(POST-RX). So we do
spirometry as a baseline then we give a bronchodilator usually we give
Salbutamol to differentiate whether it is asthma or non-asthma. Bcoz
asthma is reversible while COPD is not reversible.
So this is (Pic A) a pretreatment between before and after giving thebronchodilator any value between 80% an 100% of within predictive is
within normal limit and the ratio FEV1/FVC is 79 and it is above 70 so
this is normal spirometry.
This is typical spirometry(Pic B) of asthmatic patient. The ratio was low
which is 69 and within normal range and improve after givin
bronchodilator which is 80.So there is significant improvement.
While in COPD (Pic C) the ratio is reduce. The ratio before giving
bronchodilator was 63 and there is no improvement after giving
bronchodilator which is 59. So this is irreversible airways obstruction
which confirmed COPD.

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 18/25
18 | P a g e
This is a normal chest x-ray you can see the diaphragm is dome shape
and presence of bronco vascular marking.
This is a chest x-ray of of an emphysematous person, there is
hyperinflation the lungs are larger and the background is blacker and
you don’t see the bronco vascular margin bcoz of enlargement air
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 19/25
19 | P a g e
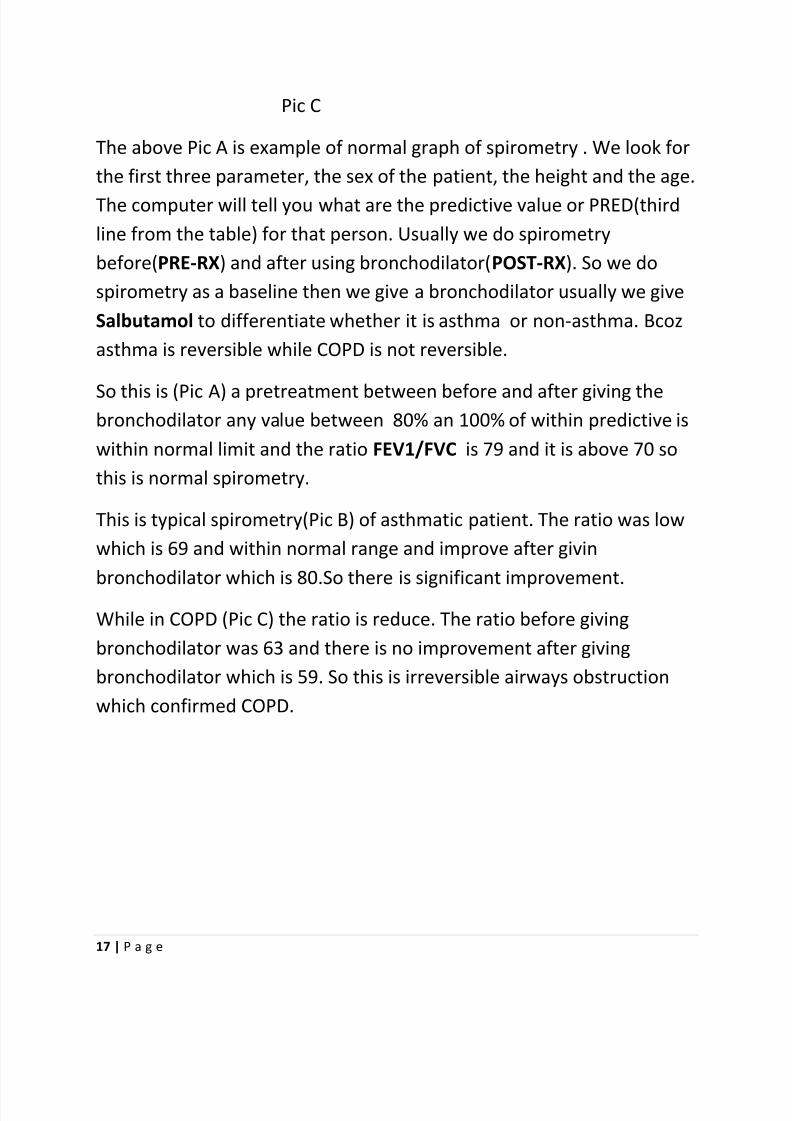
spaces. But the chest x-ray is not sensitive. The most sensitive is the
high resolution CT scan.
This is typical of hight resolution CT scan. You can see lots of holes here,these are the centrilobular emphysema and usually effect on the upper
lobe rather than the lower lobe
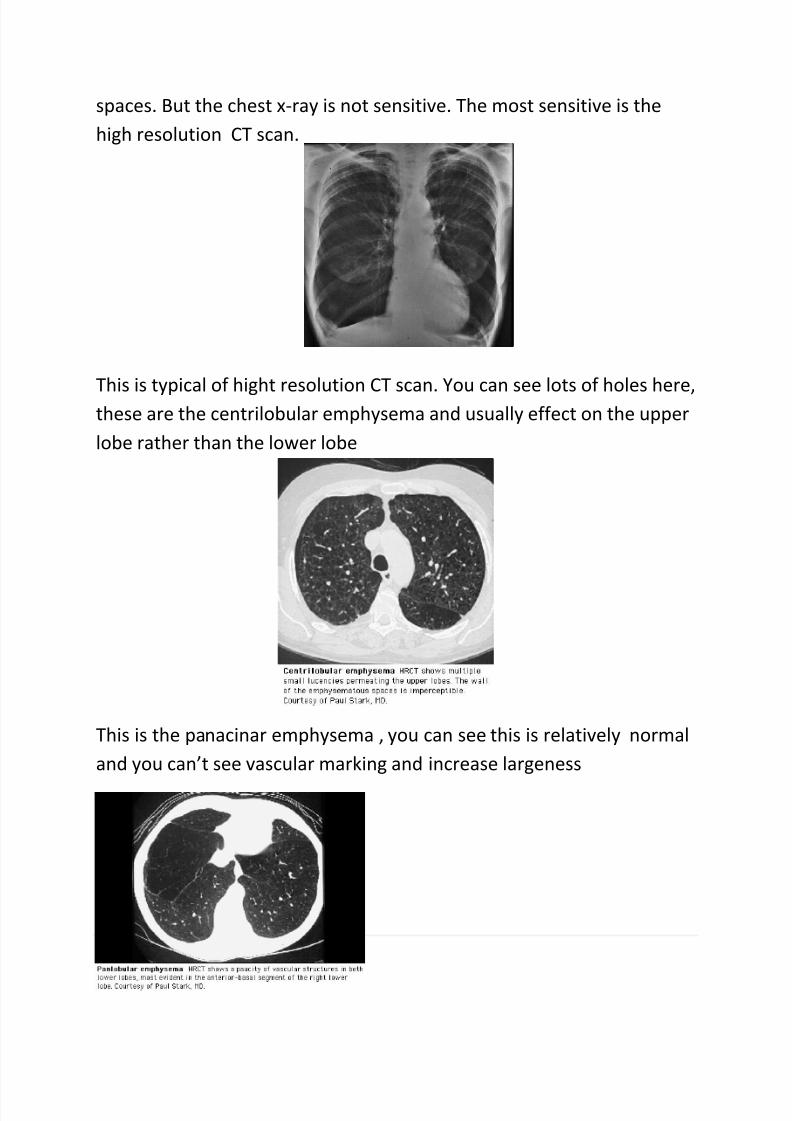
This is the panacinar emphysema , you can see this is relatively normal
and you can’t see vascular marking and increase largeness

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 20/25
20 | P a g e
Sometimes it can go into what we call bullous emphysema very large
airspaces compare to the normal lungs tissue.
Treatment
The first thing in treatment of COPD is to prevent the disease
progression the only thing that can prevent or stop disease progression
is stopping smoking. If you stop smoking the disease will not progress
and will not go back to normal but at least the disease will not progress
further and we have to make every effort to convince the patient to
stop smoking. Smoking is an addiction and qualifies the criteria of
addiction there is physical and mental dependence on nicotine. So if
you stop there are withdrawal symptoms. So if the patient tried and he
fail, we can assist him by giving nicotine replacement or we can use
antidepressant or varinicline( which is nicotine receptor agonist). But all
these, the success rate are probably 20% or 30%. We have to give
them the vaccines to prevent infections, they have to take the influenza
vaccines every one cup and they have to take the pneumococcal
vaccines once in their life. We can improve the pulmonary function by

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 21/25
21 | P a g e
giving medical treatment, and the main treatment we gave
bronchodilators either the β2 agonist with short acting or long acting
depend on the stage of the disease or anticholinergic drugs wither
short acting like Ipratropium or the long acting like Tiotropium. Inhaledcortical streroid can be given especially those who have frequent
exacerbation and they have moderately severe disease there is
evidence that that giving inhale cortical steroid might improve their
symptoms. While in asthma the main steroid treatment is the inhaled
cortical steroid. Sometimes we have some surgical treatment for
certain disease.
Normally about the age of 25 we reach the maximum pulmonary
function after that we start losing FEV1. Normal people they lose about
20ml to 30ml of their FEV1 every year. For example for someone whose
25years and he’s 170cm his FEV1 probably around 3.5 liter, if he lived
to the ages of 75 after 50 years he will lose about 20ml to 30ml every
year so he lose about 1 liter of FEV1, so at age 75 his FEV1 is 2.5 liter. If
your FEV1 is below 2 liter can’t even tolerate pneumonectomy(removal of one lung). While a smoker who is susceptible to have COPD and
probably some genetic predisposition (bcoz why some people develop
COPD in smoker and others are not) as I said 20% to 30% person only
may develop COPD they lose between 50ml-70ml every year. So if we
take average of 60ml after 50 years he lose 60ml every year so probably
60ml times 50 about 3 liters. So at the age of 75 his FEV1 left is 0.5 liter
and if you have FEV1 less than 1 liter you are probably dead.
So this is the susceptible smoker of how the FEV1 drop, this is not
susceptible even if he smoke

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 22/25
22 | P a g e
At any stage if you stop smoking at least after years you stop smoking
and lose back only 20ml only not like the 50ml or 70ml that you lose if
you continue to smoking. So it is not late to quit smoking even if you
have advance diseases. You will not go back to normal but at least you
have some improvement and maintain you function. So this is
FEV1(above line) those who have sustain quitters stop smoking and
continue stop smoking their FEV1 remain relatively stationary, while
those who continue to smoke their FEV1 dropping every year.
So the management of COPD according to these rate all COPD have to
avoid the risk factors and should have vaccination. We add the
bronchodilator like I said Salbutamol or the long acting bronchodilators
Salmeterol and Formoterol and the anticholinergic drugs. If they have
severe disease we start adding inhale cortical steroid. If they ended up
with respiratory failured we will use oxygen long therapy at home. Thetreatment option surgical which is rarely, is done by lung volume
reduction surgery. We have what we called the bullectomy if he has
large bulla(a large air-filled space) and lung transplant. Nobody is doing
lung transplant for COPD if related to smoking but those who have α1
Anthonisen et al. JAMA 1994;272:1497 –1505
S c r e e n
2 1 y
r 2 y
r 3 y
r 4 y
r 5 y
r2.4
2.5
2.6
2.7
2.8
2.9
P o s t b r o n c h o d i l a t o r F E V 1
Sustained Quitters
Continuing Smokers
Smoking Cessation and FEV1 Decline

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 23/25
23 | P a g e
antitrypsin defiency if they are not smoker and develop respiratoy
failure they can be candidates for lung transplant. The lung volume
reduction surgery for those who have emphysema not chronic
bronchitis bcoz smoke related to emphysema they are affecting theupper lobes of the lungs. So the upper lobes are hyperinflated and they
are compressing the relatively normal lung tissue in the middle and
lower zone. So the ideas is to remove this upper lobe to give more
space for the relatively lung tissue and that will improve the dynamic of
the diaphragm. Making the diaphragm to become normal dome shape
and thus help in breathing. This surgery is only done for emphysema
patient bcoz this disease affecting the upper lobe of the lung.
Acute Exacerbations
For the COPD patients, the most dreadful and fearful thing is acute
exacerbation which will have increase shortness of breath, cough,
sputum production , any three of those, for 48 hours, this is an
exacerbation. Usually they’re related to infections that might be viral
(however about 50 % are not related to infection) and the other might
be related to inviral cause. This disease may be mild or chronic that
require ICU admission or assisted ventilation.
1) And the main therapy is we have to get an oxygen therapy becausethey’re hypoxic. We also have to give the bronchodilator through
nebulization in acute exacerbation .

8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 24/25
24 | P a g e
2) And we have tp get the antibiotics as well which will recover the
bacteria like Haemophilus Influenza or Moroxilla Cataralist (not
suree!) or Strep Kimon(not sure!).
3) Corticosteroids are given systemically either orally or parentallyaccording to severity.
4) if they do not response they might need assisted ventilation of
non-invasive or mechanical ventilation. Those with advance disease
with time, they develop chronic respiratory failure, not only during
acute exacerbation, but during their usual days
Respiratory Failure
Anyone who has Pa O2 < 55mmHg(7.3kPa) ( providing he’s
not an exacerbation)
PaO2 ( Arterial Oxygen Partial Pressure ) of between 55 mmHg
and 60mmHg(7.3-8kPa) plus Corpulmonale (by clinically, or
ECG) or if he has erythrocytosis (secondary Polycythemia)
because they’re hypoxic as the body try to produce more
haemoglobin, more erythopoetin to compensate the hypoxia.
So if it’s between 55 and 60 plus, he’s a candidate for Long
Term Oxygen Therapy (LTOT) , you have to use the oxygen all
the day and night at home. And the oxygen is provided by
either in Cylinder (which is changed every 48 hours) or
nowadays we have ‘Oxygen Concentrater’ (A machine that is
pluged into electricity, it will take the atmospheric air, take
nitrogen out of it, and will leave the oxygen. This is expensive
relatively but more practical for the patient. And there are
8/2/2019 I M lec #3
http://slidepdf.com/reader/full/i-m-lec-3 25/25
25 | P
many studies has shown the long term oxygen therapy (LTOT)
for those who have respiratory failure do improve in their
survival . First study was done by medical research council, has
shown that those with RF, if they’re given LTOT, they survivelonger than who did not received LTOT.
-The End-
*Alhamdulillah!
Sorry for any mistake or confusion in our notes.
-Wan Muhammad Najib
-Amar Adam




![LEC 1 P N 1 LEFS16A-400 - content2.smcetech.com · LEC 1 P N 1 Controller Compatible motor Number of step data (Points) Parallel I/O type I/O cable length [m] Actuator part number](https://cdn.vdocuments.net/doc/165x107/5fd277119494594bde0fe5dd/lec-1-p-n-1-lefs16a-400-lec-1-p-n-1-controller-compatible-motor-number-of-step.jpg)


