
Radiosurgery as part of the neurosurgical armamentarium:Educational Symposium – November 24th 2011
Impact of Gamma KnifeRadiosurgery on the neurosurgicalmanagement of skull-base lesions:
The Combined ApproachProf. Roy Thomas Daniel
Médecin-Chef, Service de NeurochirurgieCHUV, Lausanne, Switzerland
First Anniversary Gamma Knife Center CHUV

Anterior Cranial Fossa
Posterior Cranial Fossa
Middle Cranial Fossa
Vestibular schwanommaPosterior Petrous meningioma
Meningioma Olfactory groove Planum sphenoidaleCarcinomaEsthesioneuroblastoma
Meningioma Diagphragmma sellae Clinoid /Optic foramen Cavernous sinusSchwanomma (5th N)Pituitary adenoma
Skull Base surgery
When to treat ?!And which modality?
• Large / symptomatic lesions -> microsurgery- Total / subtotal removal ?- Remnant: to treat or not to treat ? When ?
• Small to medium-size symptomatic lesions :-> microsurgery or radiosurgery ?
• Small to medium-size asymptomatic lesions :-> microsurgery or radiosurgery ? When ?- clinical and radiological follow-up?- treatment upfront?
good knowledge of the treatment outcomes(location, age, … ) and natural history (highly variable)

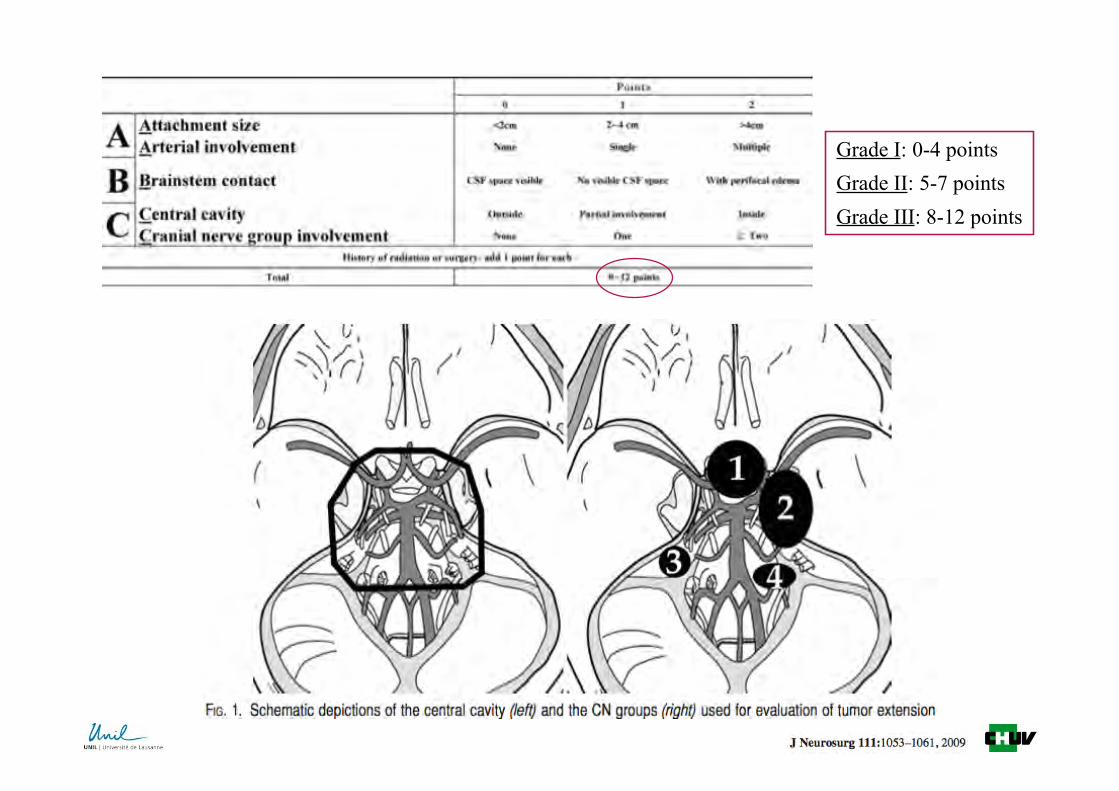
Grade I: 0-4 pointsGrade II: 5-7 pointsGrade III: 8-12 points
1. To define the optimal dose distribution to thetarget-volume = conformity :quality of the fit between the dose volume and the target
2. To define the optimal dose distribution to the normal tissue = selectivity :
to minimize irradiation of healthy tissue and critical areas
Limiting factor = volume of the target
↑ volume ⇒ ↑ dose outside of the target ⇒ ↑ complications( fonction of the location and of the treated indication )
SRS: TREATMENT PLANNING
= DOSIMETRY

TARGET VOLUME
SRS: TREATMENT PLANNING

TARGET VOLUME
Microsurgery(combined approach)
DOSIMETRY
Under-treatment

Vestibular Schwanomma


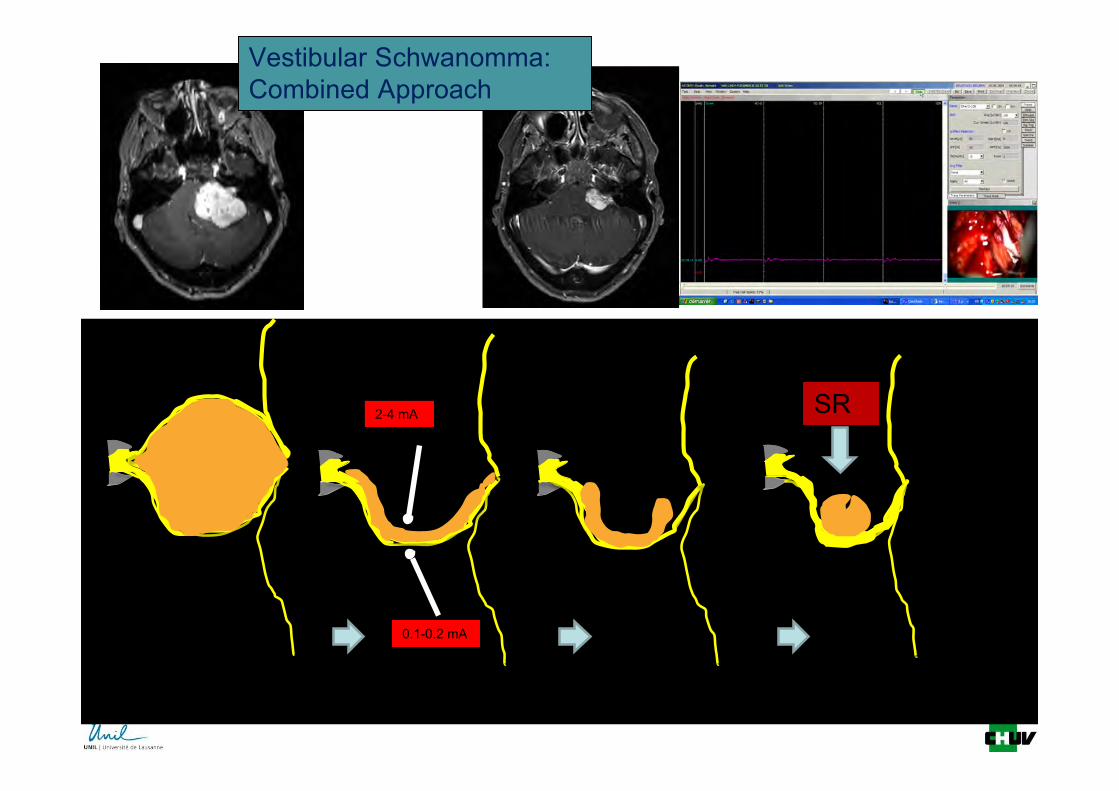
SRS
Vestibular Schwanomma:Combined Approach
2-4 mA
0.1-0.2 mA

Post op(early)
Post op 6 m
6 m Post GK
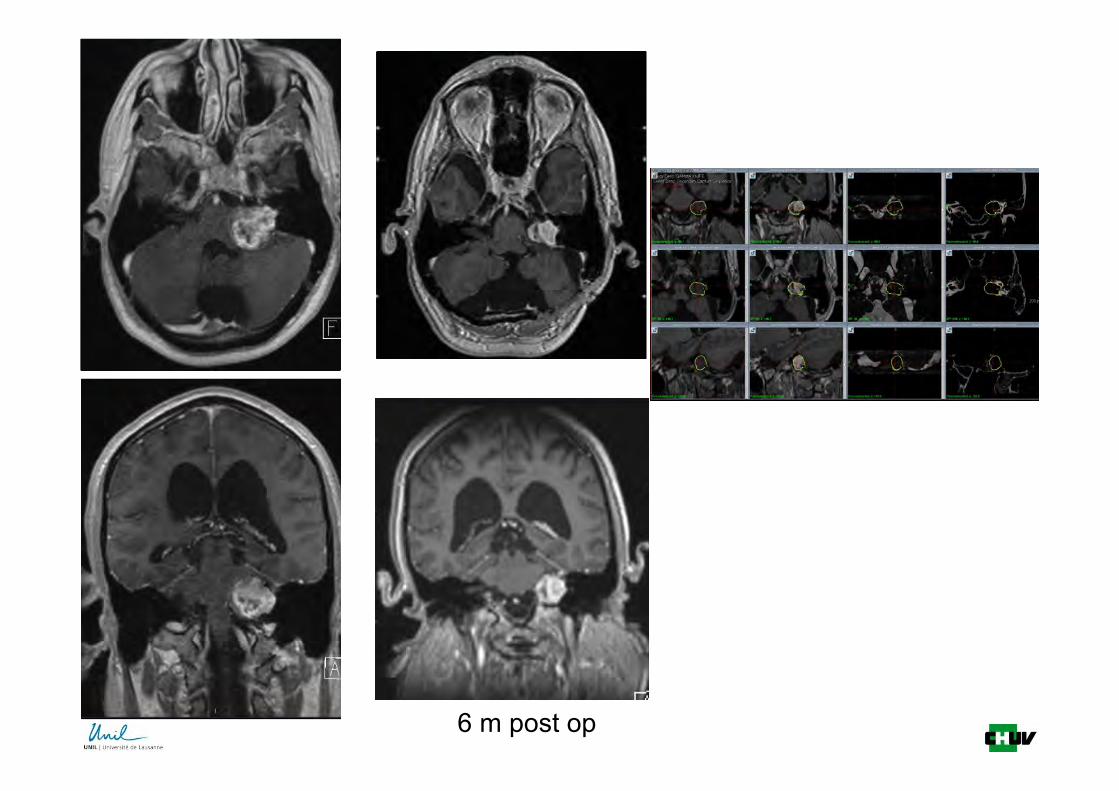
6 m post op

Rendinachristina 6 m post op


Petroclival meningioma
Petrous bone
IAM

Specific issues withpetro-clival meningiomas
• More variable clinical presentation
• More variability in surgical approaches
– Retrolabrynthic pre sigmoid
– Trans labrynthic or trans cochlear
– Middle fossa trans petrous
– Retrosigmoid
• More “compression-related” symptoms, needing surgery (more limitedresponse to radiosurgery)If radical resection is too risky -> combined approach
• Brain stem = 12 Gy (like the prescription dose) less limitation than with cavernous sinus lesions(not always …. ; cf. post-radiation therapy)
• New functional challenges:e.g. cochlea (4 Gy)

• 76% radiologicaltumor growth
• 63% functionaldeterioration withtumor growth
In our opinion, clival meningiomas are inoperable.(Castellano and Ruggiero, 1953)
Clivus meningiomas in particular have until recent years been uniformly lethal. Theoutlook of such patients must be bettered by achieving earlier diagnosis, by improvingsurgical technique and better understanding on the pathological anatomy.(Yasargil, 1980)
In nearly all cases, the patient came out in worse clinical and neurological conditions aftersurgery than before and therefore need constant, meticulous assistance.(Bricolo, 1992)
By a combined application of advanced microsurgical techniques, thoughtful,intraoperative decision making with limited surgical aggressivity, and in selected patients,with small remnants simple observation or alternative or adjunct radiosurgery, excellentresults as measured by tumor control and preservation of quality of life can be achieved.(Seifert, 2010)
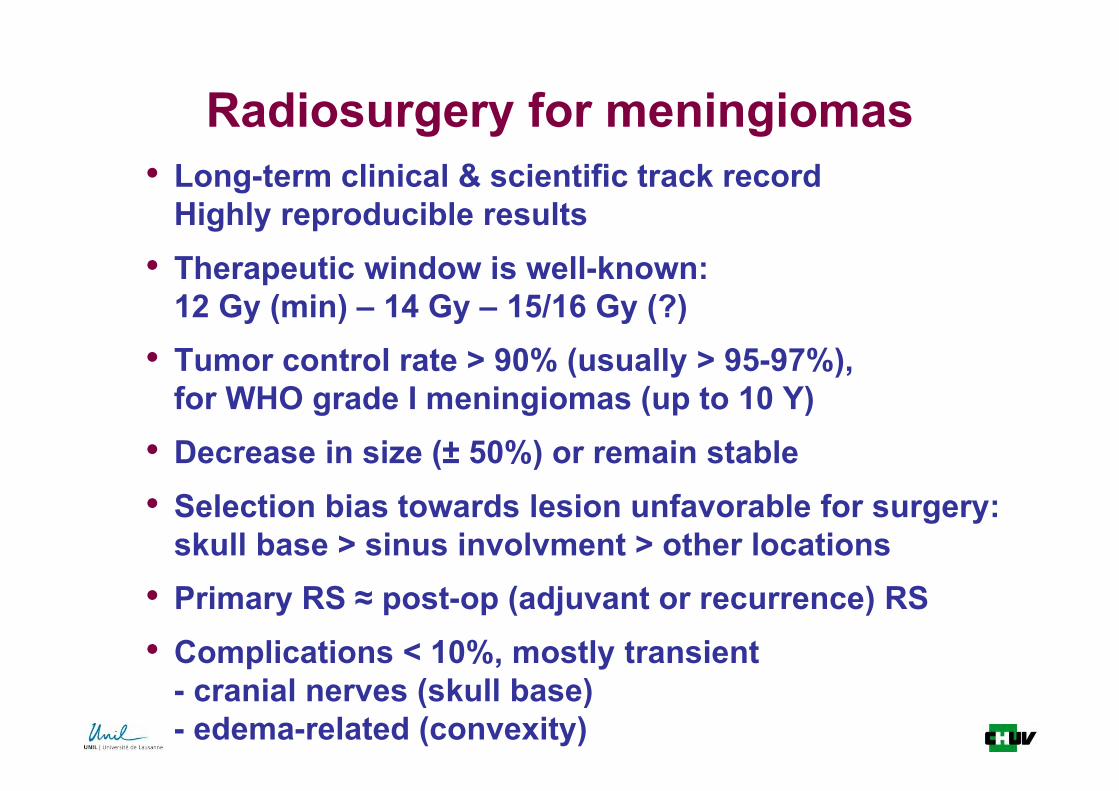
Radiosurgery for meningiomas• Long-term clinical & scientific track record
Highly reproducible results• Therapeutic window is well-known:
12 Gy (min) – 14 Gy – 15/16 Gy (?)• Tumor control rate > 90% (usually > 95-97%),
for WHO grade I meningiomas (up to 10 Y)• Decrease in size (± 50%) or remain stable• Selection bias towards lesion unfavorable for surgery:
skull base > sinus involvment > other locations• Primary RS ≈ post-op (adjuvant or recurrence) RS• Complications < 10%, mostly transient
- cranial nerves (skull base)- edema-related (convexity)

7thN
7thN
5thN
Petroclival meningioma

Middle Cranial Fossa Tumours
Clinoidal meningioma
Trigeminal schwanomma
Pituitary adenoma
Specific issues with Middle fossameningioma radiosurgery
• Total excision of tumours in or around the cavernous sinus
– 50% cranial nerve morbidity
• Small intracavernous lesions: Radiosurgery
• Larger tumours need combined approach
– The optic nerve is mostly sensitive to radiationFor radiosurgery: 8 Gy (up to 10 Gy?) no contact between the tumor and optic tract- combined approach (with opening of optic canal when needed)- “undertreatment” (lower dose at interface)
– The content of the cavernous sinus is considered resistant tohigh-dose radiosurgery(risk of carotid obliteration?)

ON(Ex)
SOF ON(In)
ON
ICA
ON(In)
ON(Ex)
Chiasmopexy & Hypophysopexy

EDON
ID ON
Optic foramen Meningioma

• Anterior Lobe:– FSH– LH– ACTH– TSH– Prolactin– GH
• Posterior Lobe:– ADH– Oxytocin
Pituitary Adenoma

Microadenomas (< 10 mm)
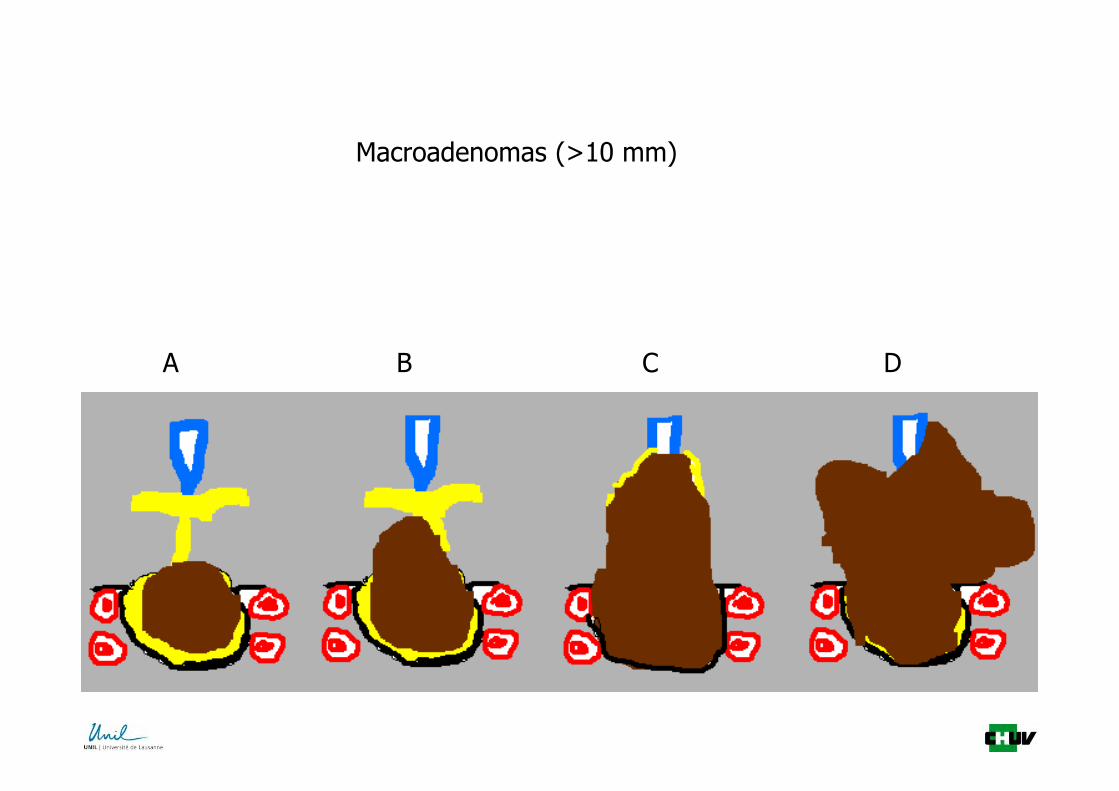
Hardy’s classification
A B C D
Macroadenomas (>10 mm)


The Trans-sphenoidalapproach
Transsphenoidal Line ofVision on MRIfor Pituitary Tumor Surgery
Neurol India, 2002; 50 : 136-140


Stage 1 Stage 2
Stage 3
Non-functionalPituitary Adenoma

6m post op: IGF1 still high
SRS
Combined Treatment(Microsurgery +Radiosurgery)
for skull base tumours• Avoids the need (in most cases) for complicated and
invasive skull base approaches
• Potential for cranial neuropathy greatly decreased
• Low risk of permanent complications
• Long-term tumor control needs to be studied in thissubgroup
– Growth pattern is unpredictable careful imaging follow-up is mandatory
• Will become standard of care as long term resultsemerge from this approach







