
LOWER GI HEMORRHAGEINFLAMMATORY BOWEL
DISEASE
Dr.B.SELVARAJ MS;Mch;FICS:
PROFESSOR OF SURGERY
MELAKA MANIPAL MEDICAL COLLEGE
MELAKA 75150 MALAYSIA
INFLAMMATORY BOWEL DISEASE
Causes of Lower GI Hemorrhage
Epidemiology
Etiology
Pathology
Clinical Features
Investigations
Complications
Medical Treatment
Surgical Treatment
Comparision of Crohn’s & Ulcerative Colitis
Diagnostic Algorithm
Management Algorithm

Causes for Lower GI Hemorrhage
Diverticular disease
Angiodysplasia- AV Malformation
Colorectal carcinoma
Hemorrhoids
Fissure-in-ano
Ischemic colitis
Inflammatory bowel disease
Meckel’s diverticulum
Upper GI hemorrhage

IBD-CROHN’S- ETIOLOGY
Crohn’s disease is a trans mural IBD that can affect any part of the GI tract from the mouth to the anus.
The incidence is about 3 new cases/ 100,000 people, with a prevalence of about 30 cases/100,000 people.
Both genetic and environmental factors are implicated
Genetic: The IBD1 locus on chromosome 16 is strongly associated with Crohn disease.
Environment: Infective agents implicated measles virus and Mycobacterium para tuberculosis
Cigarette smoking and intake of refined sugars
IBD-CROHN’S-PATHOLOGY
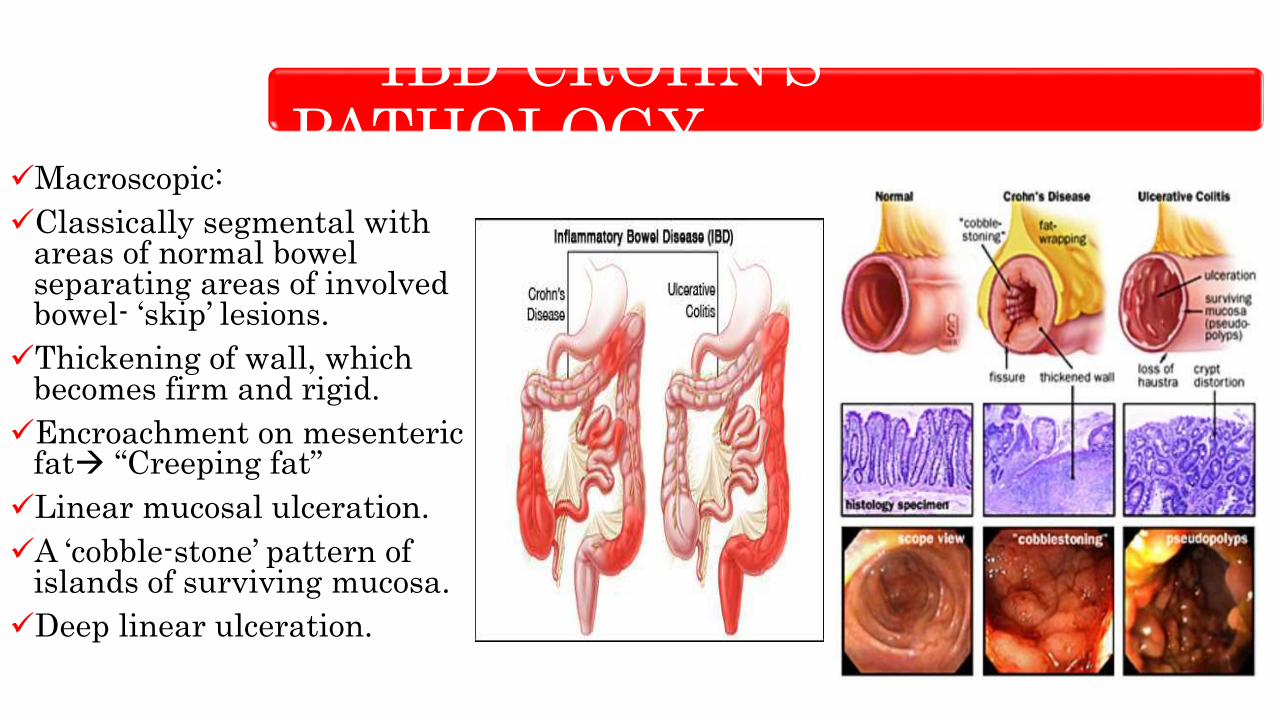
Macroscopic:
Classically segmental with areas of normal bowel separating areas of involved bowel- ‘skip’ lesions.
Thickening of wall, which becomes firm and rigid.
Encroachment on mesenteric fat “Creeping fat”
Linear mucosal ulceration.
A ‘cobble-stone’ pattern of islands of surviving mucosa.
Deep linear ulceration.

IBD-CROHN’S-PATHOLOGY
Microscopic:
Transmural inflammation from mucosa to serosa.
Marked edema of submucosa.
Lymphoid aggregates
Patchy mucosal ulceration and fissuring.
Presence of non-caseatinggranulomas (found in only 60% of cases).

CROHN’S-CLINICAL FEATURES
Three distinct types of disease are seen: inflammatory, stricturing and perforating
Patients are young and present with abdominal pain, weight loss, and diarrhea.
Abdominal pain is colicky. Some patients present with frequent bloody stools with mucus . These patients are indistinguishable from those with ulcerative colitis.
Extraintestinal manifestations include erythema nodosum, pyoderma gangrenosum, uveitis and sacroiliitis, large joint involvement, and clubbing.
Perianal Crohn diseaseRectal examination reveals evidence of ulceration, edematous skin tags, perianal abscess and/or fistulation, and stricture.

CROHN’S-INVESTIGATIONS
Colonic disease is best diagnosed by colonoscopy.
The distribution of colitis is discontinuous with rectal sparing.
Terminal ileum can be visualized and biopsied to confirm small bowel disease.
Upper GI series with small bowel follow-through or CT enterographymay be useful in identifying small bowel involvement.
Definitive imaging of perineal disease may require examination under anesthesia with proctoscopy or sigmoidoscopy.
Transrectal ultrasonography and magnetic resonance imaging of the anal canal can also reveal perineal disease
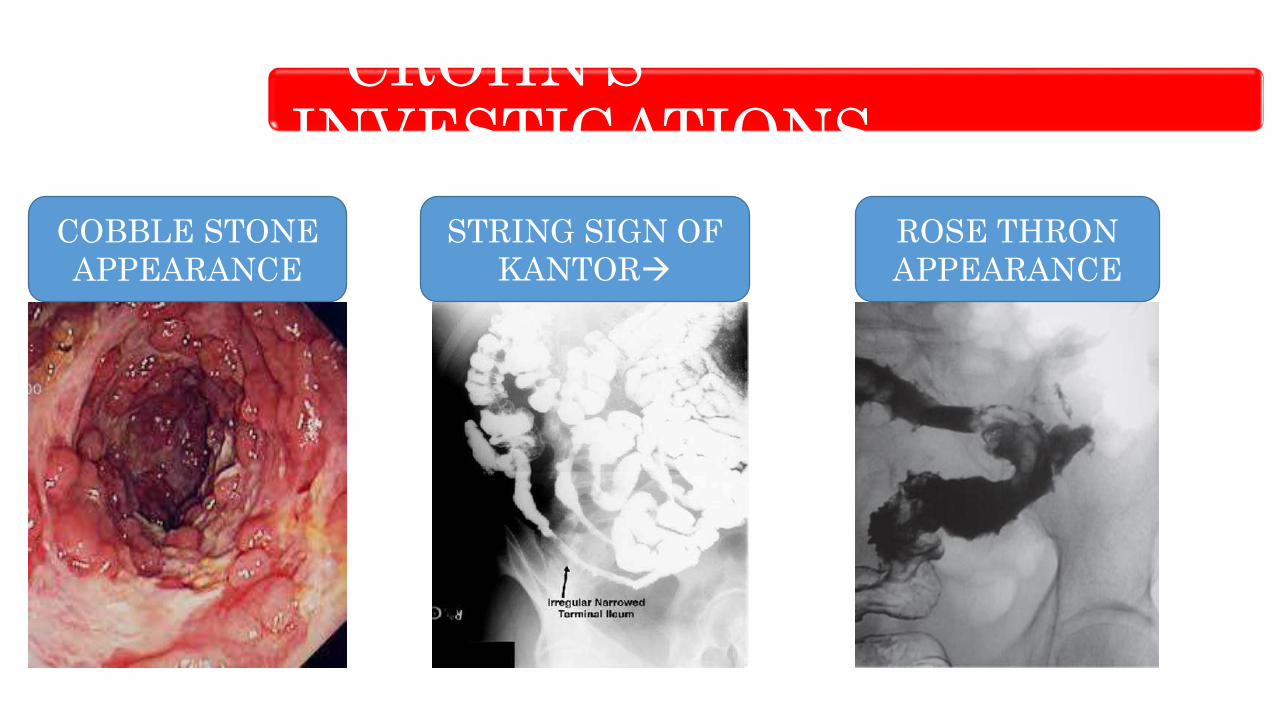
CROHN’S-INVESTIGATIONS
STRING SIGN OF
KANTOR
ROSE THRON
APPEARANCE
COBBLE STONE
APPEARANCE
CROHN’S-COMPLICATIONS
Intestinal obstruction.
Fistula formation.
Abscess formation.
Malabsorption syndrome.
Toxic dilatation.
Haemorrhage.
Perianal complications.
Gallstones (reduction of entero hepatic circulation of bile in terminal ileum).
CROHN’S- Medical Treatment
Aim is symptom relief and maintenance of well-being
Patients should have a well-balanced diet and maintain weight.
An acute flare-up of obstructive symptoms can be managed with a short, high-dose regimen of oral steroids.
Azathioprine may allow maintenance at a lower steroid dosage.
Budesonide is an enteric-coated steroid that is released into the terminal ileum averts the side effects of oral steroids
In a patient with remission, sulfasalazine derivatives may also be used (e.g.mesalazine or Pentasa) .
Immune suppressants such as azathioprine and cyclosporine have been shown to be effective
The anti-TNF antibody infliximab has been shown to promote healing in complex cases of P C D .

CROHN’S- Surgical Treatment
Surgery is used when drug therapy cannot achieve optimal relief.
Ileocecal disease resection to grossly normal bowel with primary anastomosis Recurrence tends to occur
Extensive colitis with rectal sparing urgent colectomy with ileorectal anastomosis
Segmental Crohn colitis also lends itself to segmental resection and reanastomosis
Rectal Crohn disease Crohn colitis require panproctocolectomy and the ileal pouch is not generally accepted because of the tendency of Crohn disease to affect the pouch, leading to its failure.
Ulcerative Colitis- Etiology
This diffuse inflammatory disease affects the mucosa of the colon and rectum.
Incidence: 1to15 new cases per 100,000 population. Bimodal distribution, with most cases occurring in the teen years followed by a second peak in the 40s.
Etiology is uncertain.
Abnormal immune response to gut microorganisms
Autoimmunity against colonic epithelial cells
Genetic factors: -familial clustering occurs; - association with HLA-DR2; - higher concordance rate in monozygotic twins
Geographic factors: much commoner in western countries than in developing world

Ulcerative Colitis- Pathology
Macroscopic:
Proctitis: inflammation of mucosa limited to rectum.
Colitis extending for a variable distance proximally from the rectum.
Total colitis with or without backwash ileitis.
The mucosal surface is ulcerated with areas of heaped regenerating mucosa called pseudopolyps
Fistulae do not occur
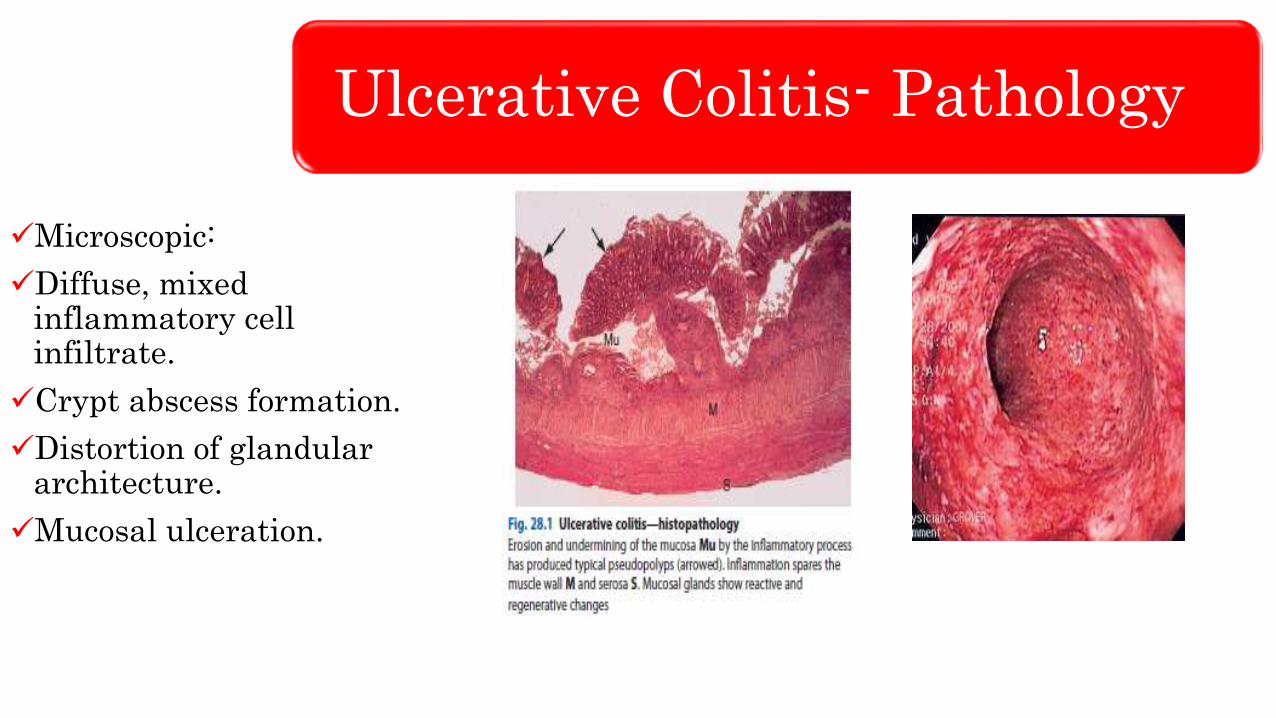
Ulcerative Colitis- Pathology
Microscopic:
Diffuse, mixed inflammatory cell infiltrate.
Crypt abscess formation.
Distortion of glandular architecture.
Mucosal ulceration.

Ulcerative Colitis- Types
Ulcerative Colitis
Clinical FeaturesClinical severity is extremely variable
Frequent passage of blood-stained stools or diarrhea that contains mucus
Mild lower abdominal pain, fever, and tenesmus
Rectal examination reveals blood and, on sigmoidoscopy, there is evidence of proctitis
A severe attack, usually with pancolitis results bloody diarrhea ( 10 to 24 times a day) , colicky lower abdominal pain, and weight loss.
Extraintestinal features: Pyoderma gangrenosum, Erythema nodosum, Scleritis/episcleritis, Uveitis, Iritis, Ankylosing spondylitis and Sclerosing cholangitis.

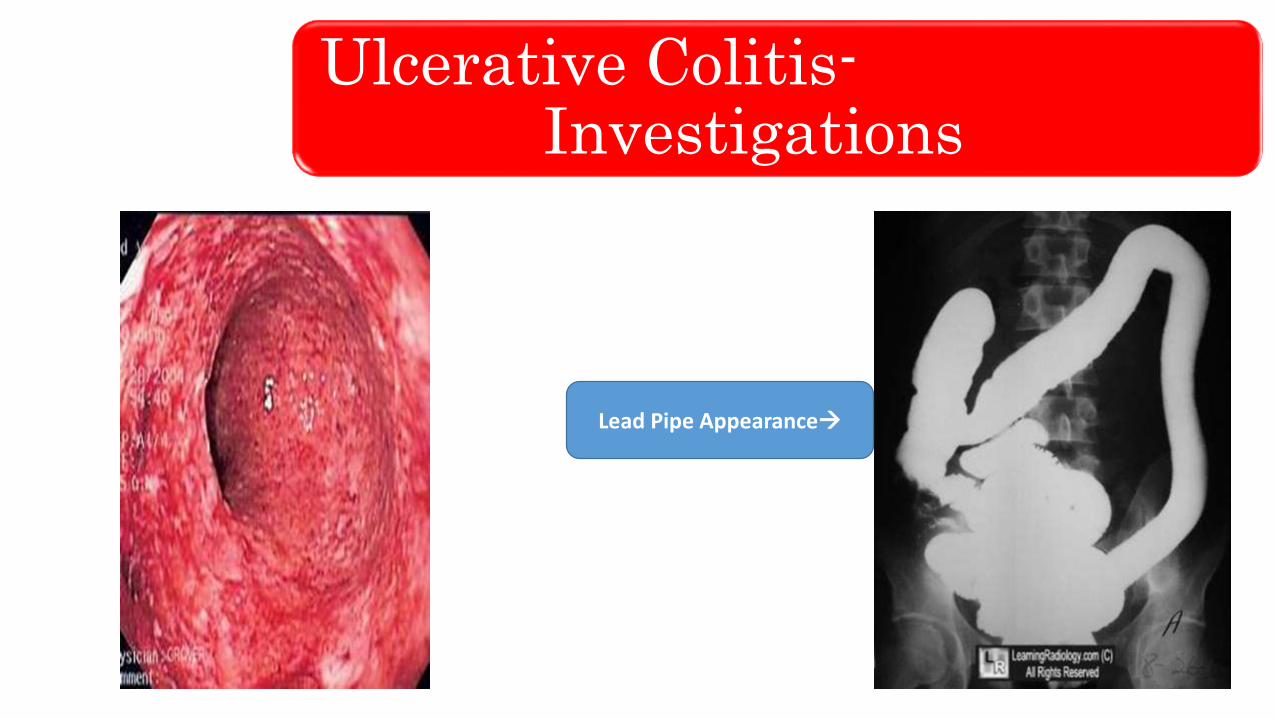
Ulcerative Colitis-Investigations
Colonoscopy is a definitive imaging technique. A full examination to the cecum is performed.
Visualization of the terminal ileum during colonoscopy to rule out Crohn disease.
A barium enema is used less frequently in the imaging of ulcerative colitis Lead pipe appearance, Thumb print sign and Rose thorn appearance are classical radiological signs
Upto 10% of patients, the differentiation between ulcerative colitis and Crohn’s disease may not be complete, and the colitis is thus labelled indeterminate.
Ulcerative Colitis-Investigations
Lead Pipe Appearance

Ulcerative Colitis-Investigations
Ulcerative Colitis-Complications
Toxic dilatation.
Perforation.
Increased risk of colorectal cancer.
Electrolyte disturbances with severe diarrhoea.

Ulcerative Colitis-Medical Treatment
Medical management of the stable patient consists of drug therapy
Such a patient may be maintained for months or years on minimal medication, with occasional periods of high-dose steroid therapy for exacerbations.
5-Aminosalicylic acid (5-ASA) induces remission and prevents recurrence, and it is the mainstay of medical treatment.
Antidiarrheal drugs may be used to reduce bowel frequency
Bowel rest and total parenteral nutrition (TPN) are indicated in severe colitis.
Cyclosporine or tacrolimus , are used for refractory colitis.
Azathioprine and 6-mercaptopurine are used to facilitate remission induced by cyclosporine
Anti- TNF antibody infliximab and monoclonal antibodies, such as anti-interleukin-2 receptor antibody
Ulcerative Colitis-Surgical Treatment
Most common indication is intractability of disease and failure of medical management to control symptoms.
Other indications include bleeding, perforation, toxic colonic dilatation, and infection.
Total proctocolectomy involves excising all colon, rectum, and anus with closure of perineal wound. A permanent right lower quadrant spouted (Brooke) ileostomy is created.
The ileal pouch (0,W,or S pouch) or neorectum to replace diseased rectum offers the chance of surgical cure without the need for a permanent ileostomy.
Long-term sequelae include pouchitis , anastomotic stricture, pouch failure , and sexual dysfunction.
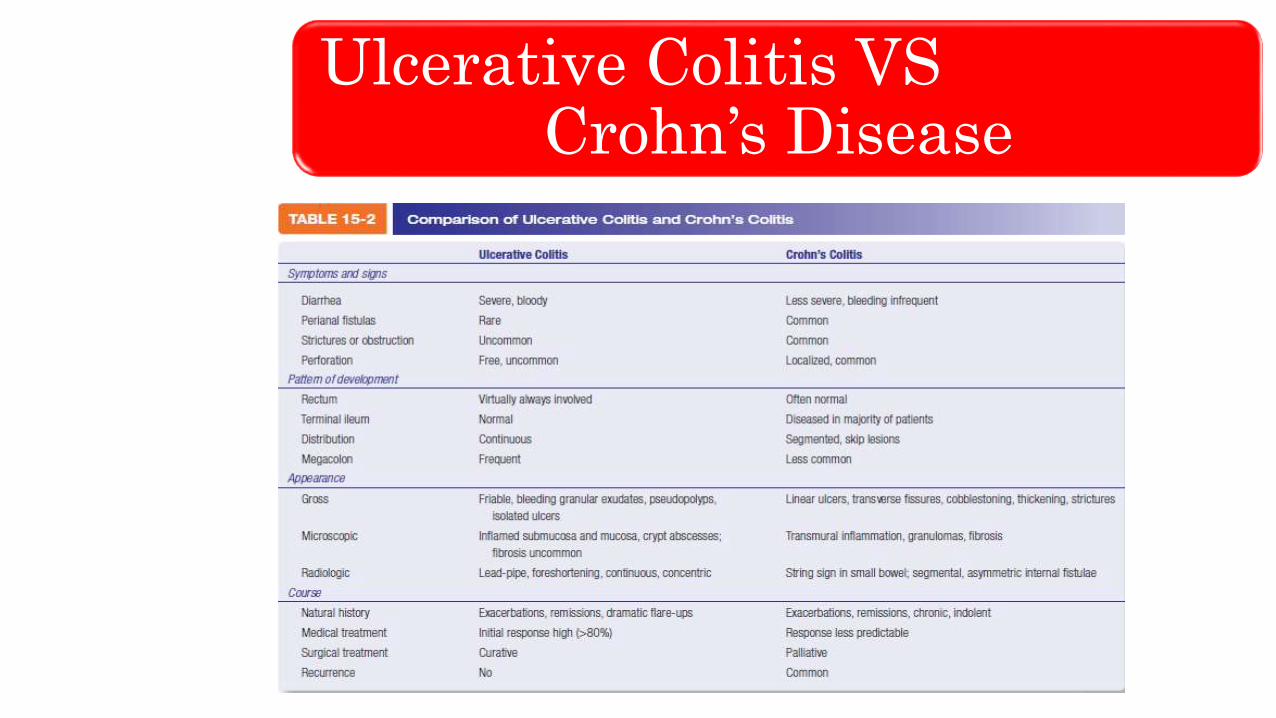
Ulcerative Colitis VS Crohn’s Disease
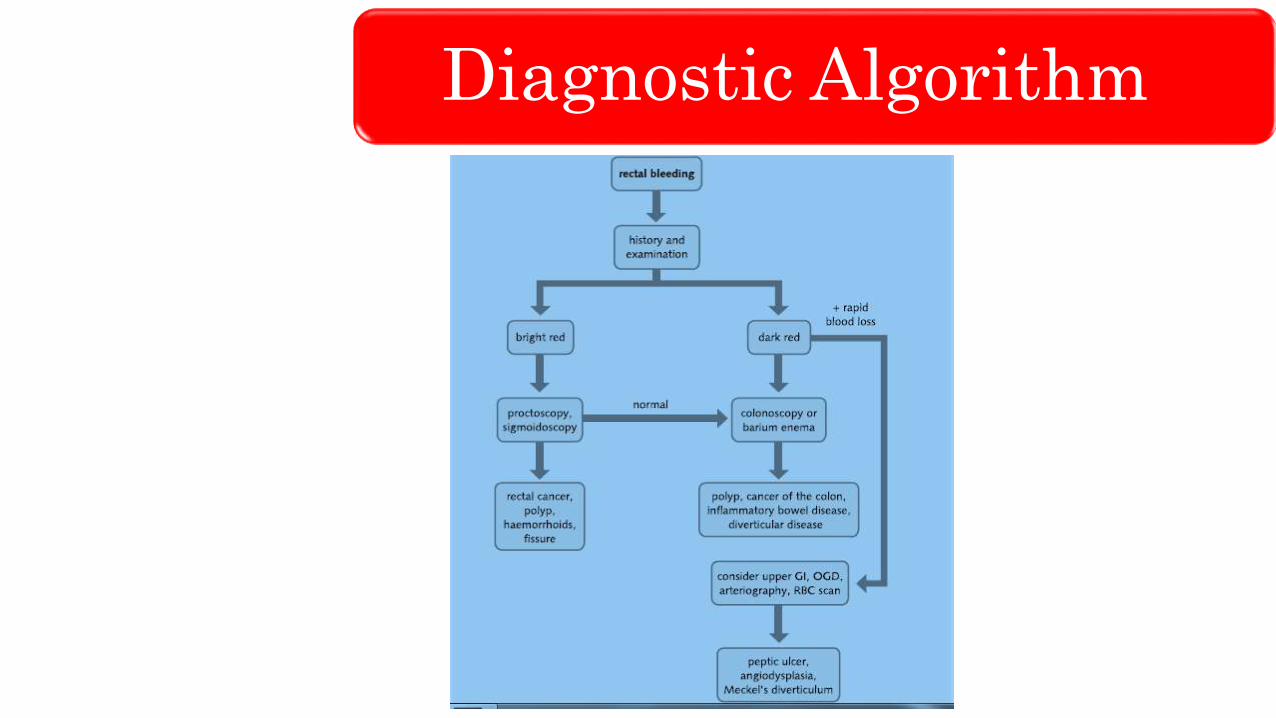
Diagnostic Algorithm

Treatment Algorithm

THANK YOU
LIKE
SHARE
SUBSCRIBE







