1
INSTRUMENT-ASSISTED SOFT TISSUE MOBILIZATION TO THE
UPPER QUARTER
Robert McCabe, DPT, MTC, OCS, CSCS
Provider Disclaimer• Allied Health Education and the presenter of this
webinar do not have any financial or other
associations with the manufacturers of any products or
suppliers of commercial services that may be
discussed or displayed in this presentation.
• There was no commercial support for this
presentation.• The views expressed in this presentation are the views
and opinions of the presenter.• Participants must use discretion when using the
information contained in this presentation.
» Sheet or band of connective tissue that
attaches to and separates skeletal muscles or internal organs
» 3 dimensional collagen matrix that is attached
to all of the biological structures which assists the body systems to operate in an integrated
manner
Zugel, BJSM, 2018
2
» Mechanical Support - chains, slings or lines
• Local and Regional
• Impacts posture
» Movement
• Detects, Transmits, and modifies forces
• “ Cellular crosstalk” among sensory receptors
» Visceral function
Chaitow, 2012 , Lee & Lee 2013, Myers 2011
» Tensegrity-Transfer of tension through network of mechanoreceptors
• Deep fasciae• Superficial fasciae
• Aponeurosis• Epineurium• Visceral fasciae
• Endomysium• Tendons
• Epimysium
• Joint Capsule
• Meninges
• Ligaments
• Retinacula
• Tendon
• Intermuscular septa
• Dermis
• Perimysium
3
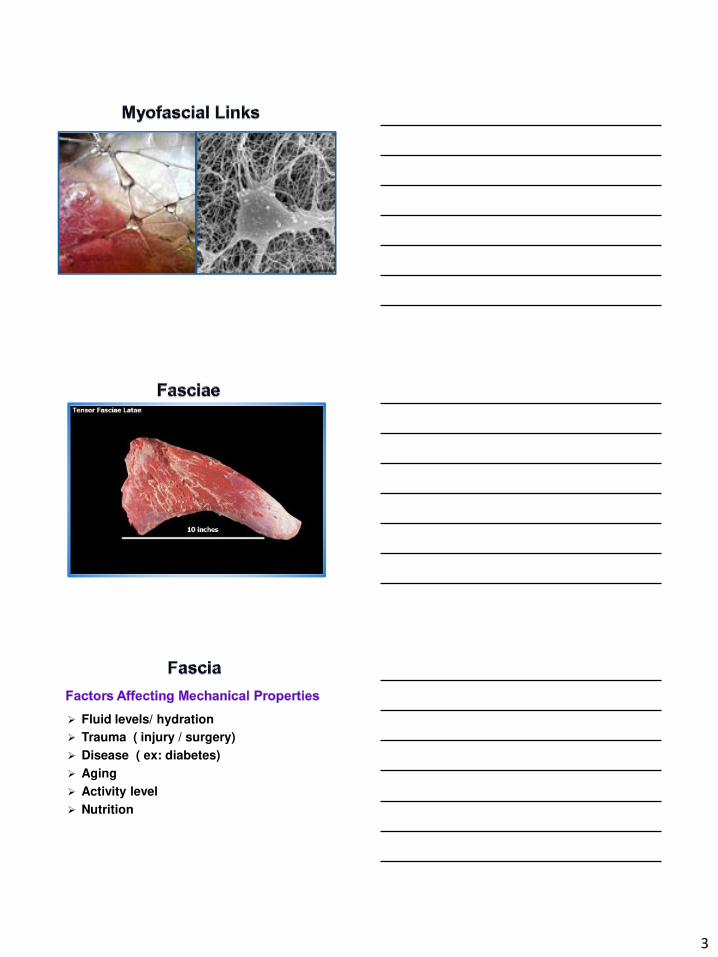
Fluid levels/ hydration
Trauma ( injury / surgery)
Disease ( ex: diabetes)
Aging
Activity level
Nutrition
4
Acute
Necessary response for tissue healing / regeneration
Applic : Long-term use of NSAIDS may inhibitmuscle growth
Chronic
Excessive response Fibrosis (collagen)Tethering/ compression
of soft tissues pain“Spillover” of
inflammatory cytokines into bloodstream
Central nociceptor stim.Fatty infiltration / mm
atrophy (ex : Disc injury Applic: Strength gains
in elderly
Tissue regeneration
Muscle growth
Neuromuscular
performance
• Ex- Power generation
Chronic MSK pain
5
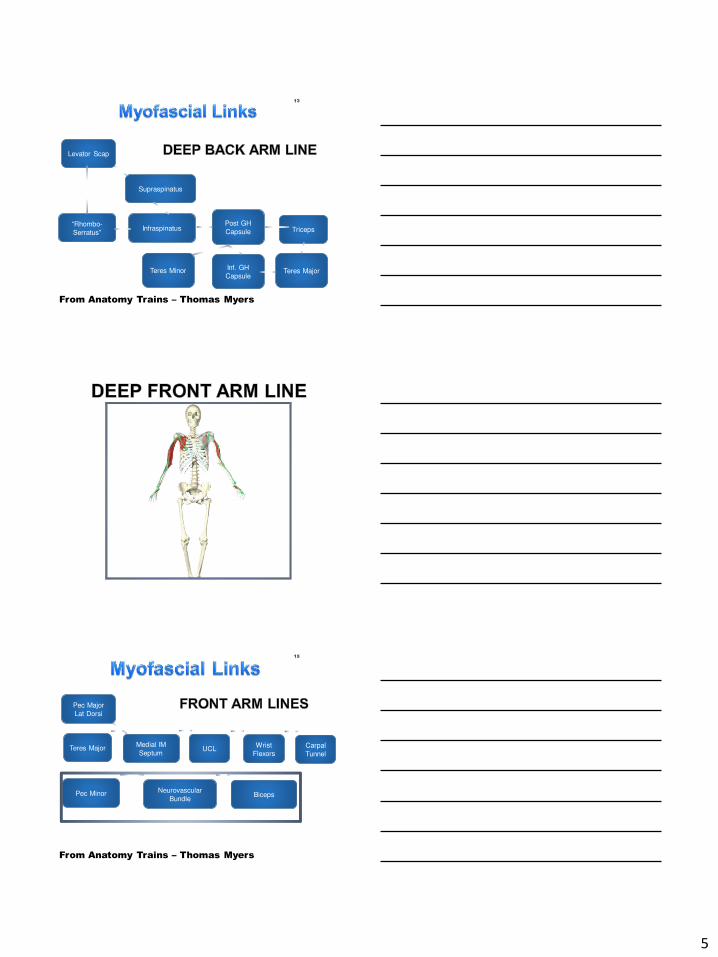
13
B
From Anatomy Trains – Thomas Myers
Supraspinatus
Levator Scap
TricepsInfraspinatusPost GH
Capsule“Rhombo-
Serratus”
Inf. GH
CapsuleTeres MajorTeres Minor
15
From Anatomy Trains – Thomas Myers
Medial IM
Septum
Pec Major
Lat Dorsi
Teres Major
Neurovascular
BundlePec Minor
Carpal
TunnelUCL
Wrist
Flexors
Biceps
6
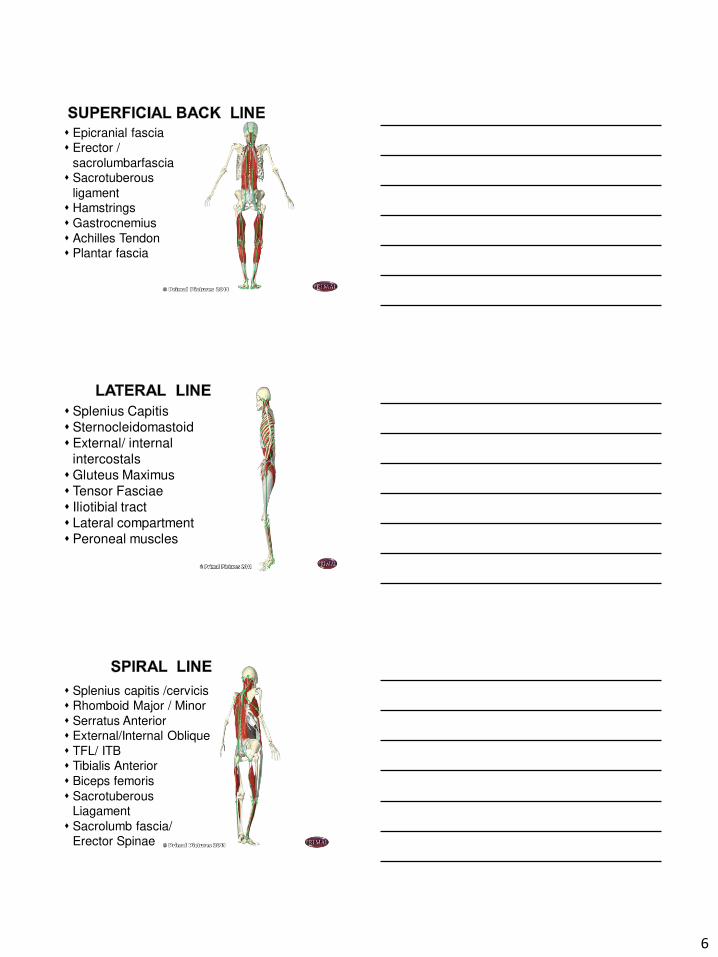
Epicranial fascia Erector /
sacrolumbarfascia Sacrotuberous
ligament Hamstrings
Gastrocnemius
Achilles Tendon Plantar fascia
Splenius Capitis
Sternocleidomastoid
External/ internal
intercostals
Gluteus Maximus
Tensor Fasciae
Iliotibial tract
Lateral compartment
Peroneal muscles
Splenius capitis /cervicis Rhomboid Major / Minor
Serratus Anterior External/Internal Oblique
TFL/ ITB Tibialis Anterior
Biceps femoris
SacrotuberousLiagament
Sacrolumb fascia/ Erector Spinae

7
SternocleidomastoidRectus Abdominis
Quadriceps TendonAnterior Compartment
Tibialis Anterior
Latissimus DorsiThoraco-lumbar Fascia
Sacral FasciaGluteus Maximus
Vastus Lateralis
Quadriceps Tendon
8
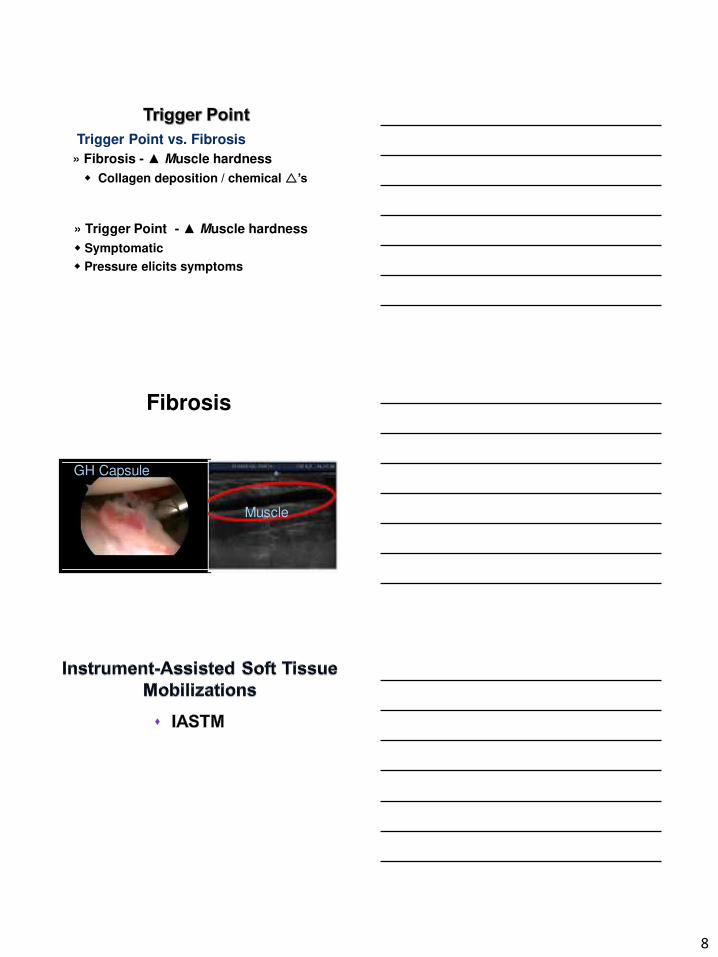
Trigger Point vs. Fibrosis
» Fibrosis - ▲ Muscle hardness
Collagen deposition / chemical ’s
» Trigger Point - ▲ Muscle hardness
Symptomatic
Pressure elicits symptoms
Muscle
GH Capsule
Fibrosis
9
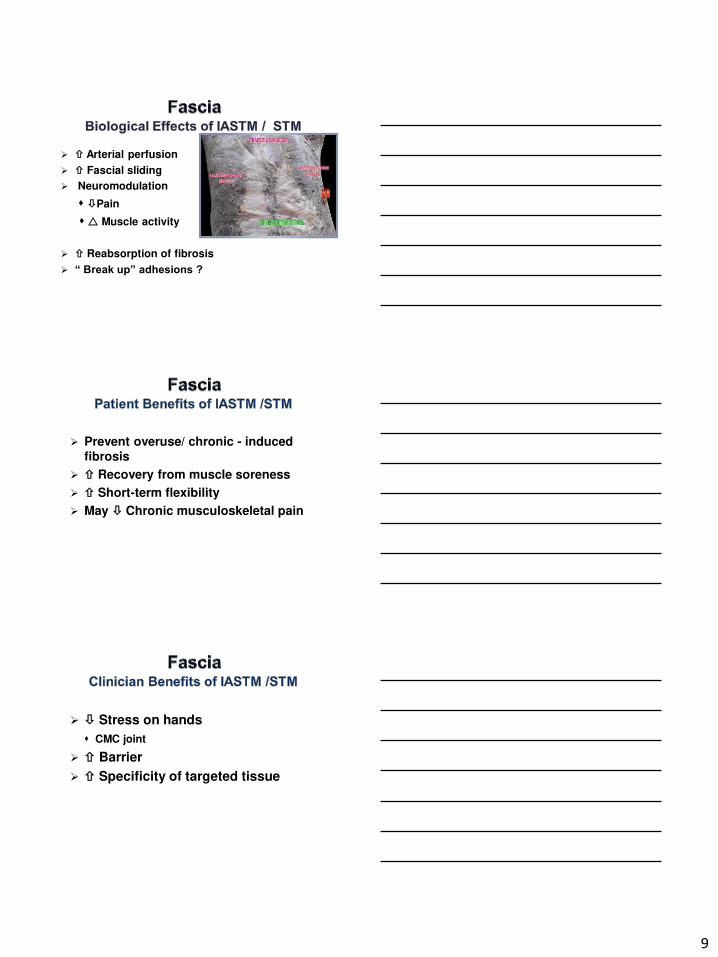
Arterial perfusion
Fascial sliding
Neuromodulation
Pain
Muscle activity
Reabsorption of fibrosis
“ Break up” adhesions ?
Prevent overuse/ chronic - induced fibrosis
Recovery from muscle soreness
Short-term flexibility
May Chronic musculoskeletal pain
Stress on hands
CMC joint
Barrier
Specificity of targeted tissue
10
» Trigger points/ MFP
» Chronic tendinopathies
» Adhesions / fibrosis /excessive scar
» Neuromuscular imbalances
» Scapula Dyskinesis
» Postural Dysfunction
» Ligament sprains (i.e. UCL)
» Nerve entrapments (CTS, TOS)
Movement
Disorder
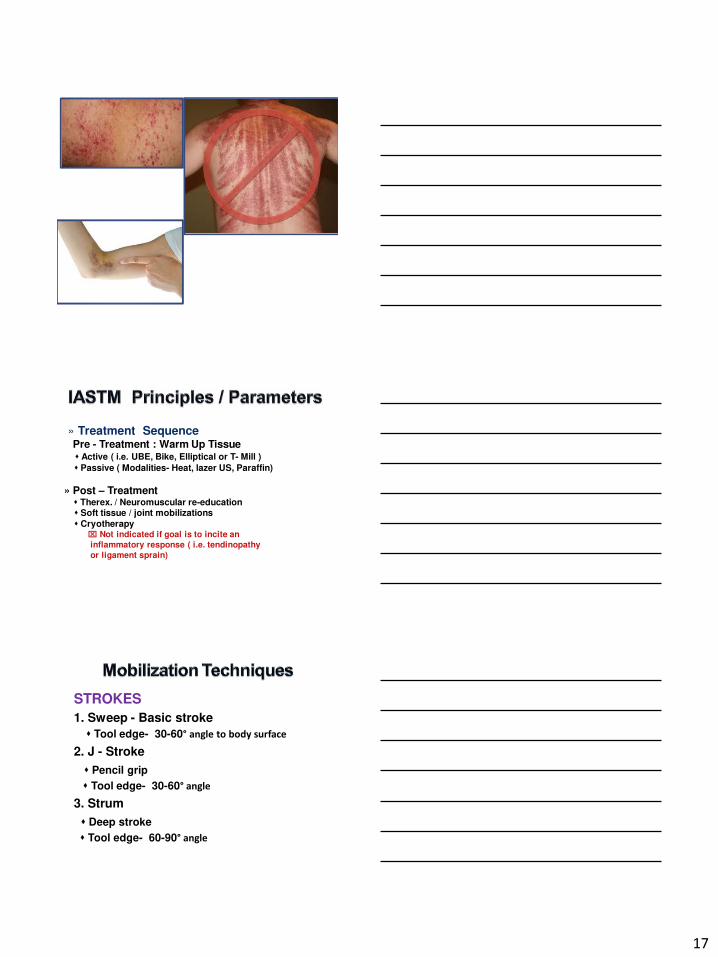
» Inflammatory or infectious skin conditions
- Psoriasis, dermatitis, eczema, cellulitis,
shingles, Athlete’s foot, foot- mouth disease
» Impaired skin integrity
Open Wound / non- closed wound margins
» Directly over surgical incision
Fibroblastic stage 0-12 weeks
» Directly over ecchymosis/effusion
» Directly over acutely traumatized tissue
» Directly over unstable fractures
» Hematoma/ myositis ossificans
» Osteomyelitis
» Varicose veins
» Cancer
» Body art
» CRPS
» Polyneuropathies
» Unhealed, closed non- complicated fractures
» Autoimmune disorders
» Diabetes
11
» Rheumatoid arthritis
» Ankylosing spondylitis
» Adjacent to pacemakers, insulin pumps
» Post- injection ( i.e. PRP )
» Lymphedema
» Central sensitization / hypersensitivity
• Massage cream
• Moisturizing lotion
Ex : Albolene TM
• Ultrasound gel
Medical Grade Disinfectant / Cleaner
After every use !
MRSA
Ex : ProtexTM
12
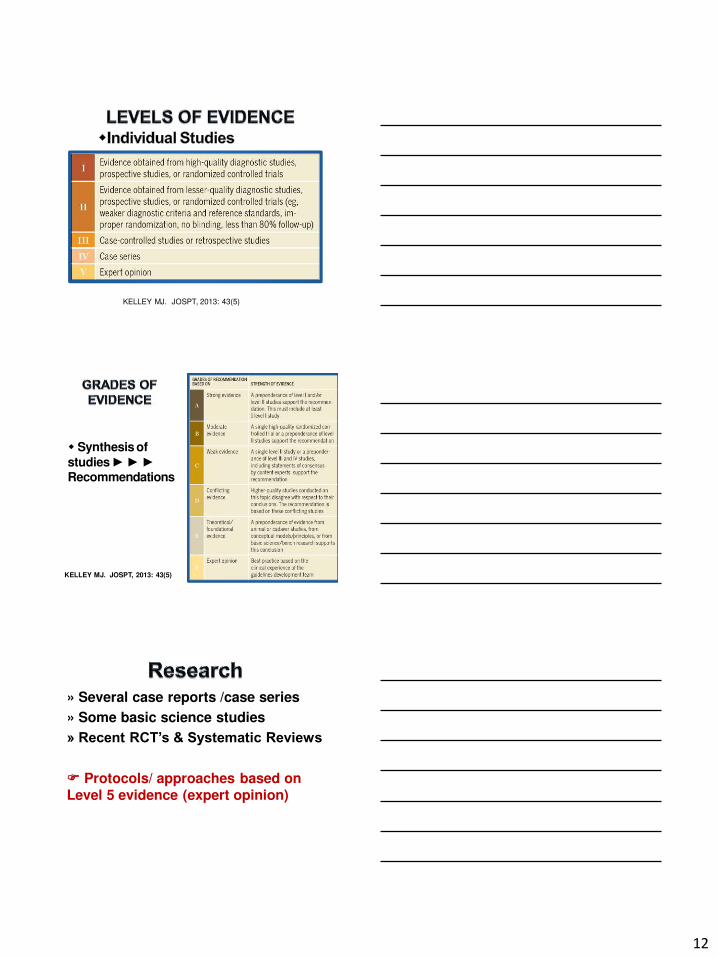
KELLEY MJ. JOSPT, 2013: 43(5)
Synthesis of
studies ► ► ►Recommendations
KELLEY MJ. JOSPT, 2013: 43(5)
» Several case reports /case series
» Some basic science studies
» Recent RCT’s & Systematic Reviews
Protocols/ approaches based on Level 5 evidence (expert opinion)
13
• Nielsen 07’ - ↑ in surface circulation ↓ pain locally and distal.
• Lambert, M. Phys. Ther. Reviews. 2017
- Systematic review
- Significant short-term ( < 3 mos.) in pain and/or
ROM vs. control and/ or other tx. groups
• Moon, JH. J. Phys Ther Sci.
- RCT
- IASTM superior to static hamstring stretches
on immediate hamstring flexibility on pts. w
non-specific LBP
• Gulick, D. J. Bodyworks & Movement Ther. 2017 -
- RCT – 3 groups of pts w UT trigger points
- IASTM – 3 techniques applied 6x over 3 weeks
- UT PPT in all 3 groups
• Miller, S - JOSPT 2018
- RCT – 3 groups of pts w UT trigger points
- IASTM vs. static stretching vs. self STM (Theracane)
- Significantly greater improvements in cervical
ROM and PPT in IASTM group
Increase career longevity
• 68 % of PT experience thumb pain.
• Of these, 25% will retire or change professions
• Based on 1102 Australian Physiotherapists
McMahon- Australian J of PT 06’
14
● Buffalo Horn
● Jade Stone
● Stainless Steel
Scanning vs. mobilizing tissue
Clinician technique
Tissue depth of application
Frequency
Duration
Treatment objective
Tissue Reactivity
Treatment Sequence
15
» Scanning = Assessing the tissue
Parallel to muscle/ Both directions
Superficial Deep
Assess for resistance
- “Bump” - Trigger point
- Grainy or gritty feel- Fascial
» Treatment Multiple angles
Superficial Deep
» Clinician Technique
Two hand technique
- Tissue is on slack Deep effect
One hand technique
- Take up soft tissue slack with non-
instrument hand Superficial effect
Application angle : 30° to 60°
» Tissue Depth = Pressure
Variables affecting tissue depth
A. Degree of tissue tension / slack
B. Degree of force
C. Angle of application
Angle Deeper effect
B. Tool surface
Concave vs. convex
Large vs. small surface
Sharp vs. dull surface area
More Superficial effect
16
Superficial ( Fasciae)
Larger surface area
Sharp/ thinner edges
Concave edges
Deep Structures ( Muscle)
Smaller surface area
Dull/ thicker edges
Convex edges
» Frequency
2-3 x’s / week ( 2- 3 days in between)
» Duration
Per session: 8-10 min
Per structure / muscle : 3-10 minutes
- Knee MCL - 2 min
- ITB - 8-10 min
- PIGH shoulder capsule - 4 to 5 min
» Treatment objective
Pain /edema (Acute)
- Non- aggressive
ROM / Disrupt fibrotic tissue
- More aggressive
- Ecchymosis is normal
- STOP if petechiae is produced
- Bruising is not necessary
» Tissue Reactivity
- Must adjust parameters !
17
» Treatment SequencePre - Treatment : Warm Up Tissue Active ( i.e. UBE, Bike, Elliptical or T- Mill )
Passive ( Modalities- Heat, lazer US, Paraffin)
» Post – Treatment Therex. / Neuromuscular re-education Soft tissue / joint mobilizations
Cryotherapy Not indicated if goal is to incite an
inflammatory response ( i.e. tendinopathy
or ligament sprain)
STROKES
1. Sweep - Basic stroke
Tool edge- 30-60° angle to body surface
2. J - Stroke
Pencil grip
Tool edge- 30-60° angle
3. Strum
Deep stroke
Tool edge- 60-90° angle
18
STROKES
4. Scoop Tool edge - 90° angle
Deep tissue
5. Brushing/ Framing
Light/ De- sensitizing strokes
Bony prominences ( ex: scapula, patella)
6. Fanning
Hold one end of tool stationary
Move other end- fan like pattern
BASIC TECHNIQUES
» Structures
Splenius capitis
Oblique capitis superior
Lateral, spiral and superficial back fascial
lines
» Common indications Occipital and retro-orbital (“behind eye”)
headaches
Forward head posture

19
Suboccipital- Lateral •
» Structures
Semispinalis capitis
Rectus capitis posterior minor/major
Spiral fascial line/ superficial back line
» Common indications Occipital and retro-orbital (“behind eye”)
headaches
Forward head posture
Suboccipital- Medial•

20
» Common indications
Cervical ROM
Scapula dyskinesis
Forward head posture
LS trigger point
Cervical radiculopathy
Levator Scapulae
» Common indications
Cervical ROM
Scapula dyskinesis
Cervical pain
UT trigger point
LS trigger point
21
Upper Trapezius 1
Upper Trapezius 2
Upper Trapezius 3
22
» Common indications
Shoulder ROM
Functional reach behind back
Scapula dyskinesis
Sp trigger point
Supraspinatus
» Common indications
Shoulder ROM
IR
Horizontal adduction
Scapula dyskinesis
Posterior/ internal impingement
SLAP tears
Ip trigger point
PIGH – Posterior- Inferior Glenohumeral
23
Infraspinatus- PIGH Capsule
Infraspinatus Tendon
» Common indications
Cervical ROM
Scapula dyskinesis
Thoracic mobility
Periscapular trigger point
24
Scapula Framing 1
Scapula Framing 2
Rhomboids 1

25
» Common indications
Shoulder ROM
Abduction
Scapula dyskinesis
Posterior/ internal impingement
SLAP tears
TM trigger point
PIGH – Posterior - Inferior Glenohumeral
Teres Major
» Common indications
Promote LT muscle activation
Scapula dyskinesis
LT trigger point
Subacromial/ coracoid impingement
Forward shoulder posture

26
Lower Trapezius 1
» Common indications
Forward shoulder posture
SA trigger point
Scapula dyskinesis
Serratus Anterior

27
Posterior- Lateral Deltoid
» Common indications
Forward shoulder posture
Costal chondritis
PM trigger point
Shoulder ROM
ER (90°) abduction
Pectoralis Major

28
» Common indications Forward shoulder posture Median nerve dysfunction
- CTS
- Cervical radiculopathy- Thoracic outlet syndrome
P. Minor trigger point Shoulder ROM
ER (90°) abduction
Pectoralis Major/ Front Arm Line
Biceps 1

29
» Common indications
Lateral epicondylalgia
Radial nerve entrapment
Elbow ROM
Wrist flexion
Lateral Elbow 1
Lateral Elbow 2 - Wrist Extensors
30
» Common indications
Medial epicondylalgia
CTS
Pronator teres nerve entrapment
Elbow ROM
Wrist extension
Medial Elbow- Wrist Flexors
Wrist –Extensor Retinaculum
31
Palm - 1
Palm - 2
Hand - Digits – Flexor Surface
32
Hand - Digits – Extensor Surface
ADVANCED TECHNIQUES
Upper Trapezius 1
33
Upper Trapezius 2
Scalenes1
Scalenes 2

34
Supraspinatus 2
PIGH Capsule- Teres Major 1
PIGH Capsule- Teres Major 2
35
IGH Capsule- Teres Major
Triceps - Teres Major 1
Lower Trapezius
36
Front Arm Line – Median Nerve
Biceps
Lateral Elbow – Wrist extensor tendon
37
Medial Elbow – Wrist flexor tendon
• Mike is a 40 year old cross fit athlete
• Former Division III
baseball player
• Beach volleyball in off-season
Current ComplaintsReason for seeking treatment
Chief c/o right shoulder pain (P1)
• Pain location - Supero - posterior shoulder
Secondary c/o “dull ache”/ tingling in right UE (P2)
• Symptom location – Antebrachium, hand and 2nd-5th digits
• Tertiary c/o “tightness” in right cervical / UT (P3)
38
Observation/ Inspection –Key Findings » Slouched posture
» Thoracic kyphosis
» Scapulae
Anterior tilted abducted and internal rotation
Right > Left
» Bilateral upper trapezius muscle guarding
» Lower right shoulder
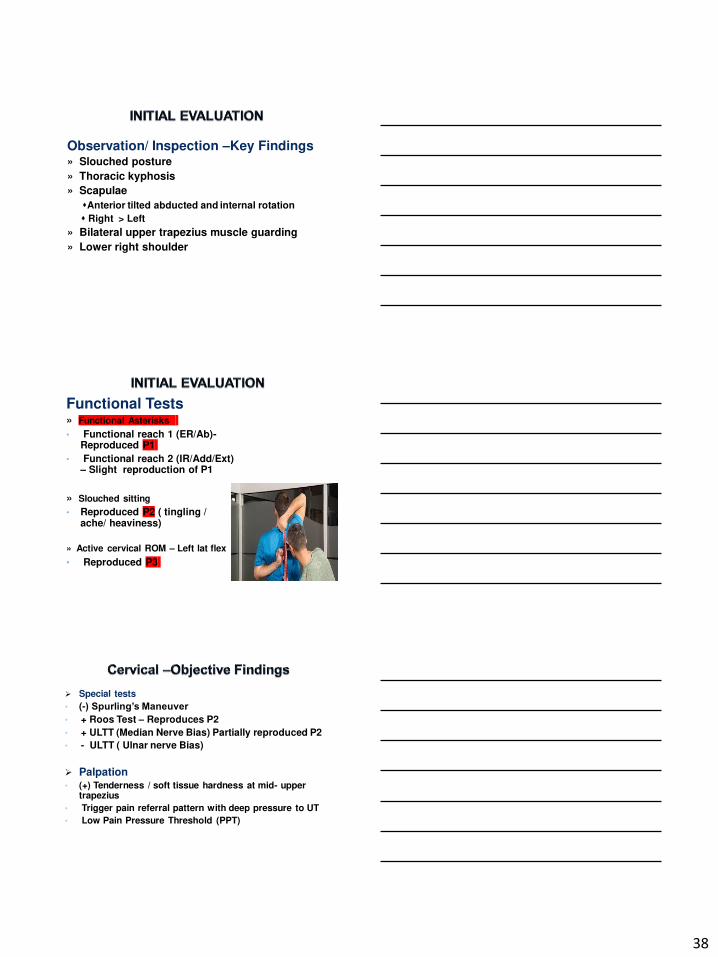
Functional Tests » Functional Asterisks
• Functional reach 1 (ER/Ab)-Reproduced P1
• Functional reach 2 (IR/Add/Ext) – Slight reproduction of P1
» Slouched sitting
• Reproduced P2 ( tingling / ache/ heaviness)
» Active cervical ROM – Left lat flex
• Reproduced P3
Special tests
• (-) Spurling’s Maneuver • + Roos Test – Reproduces P2
• + ULTT (Median Nerve Bias) Partially reproduced P2
• - ULTT ( Ulnar nerve Bias)
Palpation• (+) Tenderness / soft tissue hardness at mid- upper
trapezius
• Trigger pain referral pattern with deep pressure to UT
• Low Pain Pressure Threshold (PPT)
39
AROM/ PROM • IR
Joint Mobility • posterior and Inferior (GH) glide
Special Tests• Inconclusive SLAP
• + SA test cluster
• (+) Posterior impingement sign
» Diagnosis
• Thoracic Outlet Syndrome ( median nerve sub-type)
• Posterior impingement / possible SLAP tear
• Cervical radiculopathy
» Key Impairments• Cervical AROM
• Shoulder AROM (IR)
• Poor posture
» PIGH• Re-assess functional asterisk (P1)
» Front arm line • Re-assess functional asterisk / (P2)
» UT/ LS / cervical spine
• Re-assess functional asterisk / (P2)
40
Course Completion
You have completed the course
•
THANK YOU.
Instrument – Assisted Soft Tissue
Mobilizations to the Upper Quarter







