Download - Introduction to Respiratory Physiology Robert Padera, M.D., Ph.D. HBTM 235 September 19, 2014

Introduction to Respiratory Physiology
Robert Padera, M.D., Ph.D.
HBTM 235
September 19, 2014

Goals
• To teach you everything something about respiratory physiology and pathology
• To set the stage for lecture on lung transplantation


Outline
• Respiratory physiology– Lung anatomy– Mechanics of respiration– Control of respiration– Gas exchange– Pulmonary function tests
• Respiratory pathology– Emphysema– Usual interstitial pneumonia

Respiratory System
• Central nervous system (medulla)• Peripheral nervous system (phrenic nerve)• Skeletal muscle (diaphragm, intercostals)• Chest wall (ribs)• Lung
Conducting region (airways)
Respiratory region (alveoli)
Pulmonary vasculature• Heart

Anatomy Overview

• Lead inspired air to gas exchanging regions of the lung
• Components–Trachea–Mainstem bronchi–Lobar bronchi–Terminal bronchi
(smallest airways without alveoli)
Conducting Zone

Respiratory Zone• Gas exchanging region• Surface area and
volume• Functional unit: acinus
or lobule• Components
–Respiratory bronchioles
–Alveolar ducts–Alveoli

Alveolar Walls
• Diffusion• Surface area• Thin
• Elastin – contributes to recoil for expiration

Lung Anatomy
Vasculature

Outline
• Respiratory physiology– Lung anatomy– Mechanics of respiration– Control of respiration– Gas exchange– Pulmonary function tests
• Respiratory pathology– Emphysema– Usual interstitial pneumonia

Mechanics of Breathing
• Changing the shape, volume of thorax

Inspiration
• Active process• Contraction of
diaphragm causes increase in intrathoracic volume and decrease in intrapleural, alveolar pressure
• Air rushes in, lung expands, energy stored in elastic fibers in alveoli and pleura, chest wall

Expiration
• Passive process during quiet breathing– Diaphragm relaxes– Elastic recoil of lung,
chest wall structures– Raises intrapleural,
alveolar pressure– Air expelled
• Can add active component during exertion– Abdominal muscles– Internal intercostals

Outline
• Respiratory physiology– Lung anatomy– Mechanics of respiration– Control of respiration– Gas exchange– Pulmonary function tests
• Respiratory pathology– Emphysema– Usual interstitial pneumonia

Control of Respiration

Outline
• Respiratory physiology– Lung anatomy– Mechanics of respiration– Control of respiration– Gas exchange– Pulmonary function tests
• Respiratory pathology– Emphysema– Usual interstitial pneumonia

Gas Exchange• Alveoli• Diffusion down concentration gradient
– O2 highest in alveolus (airspace)
– CO2 highest in blood

Outline
• Respiratory physiology– Lung anatomy– Mechanics of respiration– Control of respiration– Gas exchange– Pulmonary function tests
• Respiratory pathology– Emphysema– Usual interstitial pneumonia

Pulmonary Function Tests:Spirometry

Lung Volumes

Lung Volumes

Pulmonary Function Tests:Diffusion Capacity (DLCO)
• Total gas exchange measurement• Can be affected by many pathologies

Outline
• Respiratory physiology– Lung anatomy– Mechanics of respiration– Control of respiration– Gas exchange– Pulmonary function tests
• Respiratory pathology– Emphysema– Usual interstitial pneumonia

Pulmonary Pathologies
• Asthma (airways, inflammatory)• Diffuse alveolar damage (alveoli)• Pneumonia (infection, inflammatory)• Lung cancer (malignancy)• [Chronic obstructive pulmonary disease]• [Usual interstitial pneumonia]

Chronic Obstructive Pulmonary Disease (COPD)
• Diseases that cause airflow obstruction primarily during expiration
• Patients with COPD often show overlapping features of these specific disease entities:
Emphysema
Chronic bronchitis
Bronchiectasis
Asthma
Small airways disease
• Reduced FEV1

Forced Expiration - Spirometry
• In obstructive lung disease (e.g., emphysema), both FVC and FEV1 will be decreased, FEV1 more so than FVC
• Monitor patients over time and effect of therapy

Emphysema
• Abnormal permanent enlargement of the airspaces distal to the terminal bronchiole, accompanied by tissue loss via destruction of alveolar walls
• Often co-exists with chronic bronchitis• Most strongly associated with cigarette smoking; most
people develop symptoms after about 1-2 packs per day for 20 years
• Also associated with IV drug use, immune deficiency syndromes, vasculitis, connective tissue disorders

Normal Emphysema

Normal Emphysema

Normal EmphysemaSame magnification

Normal EmphysemaSame magnification

Airflow Obstruction - 1• Due to collapse of small airways during expiration
• Damage to alveolar parenchyma leads to loss of elastic recoil of the lung, so it doesn’t provide as much “push” to expel the air
• The chest wall, diaphragm and abdominal muscles therefore need to squeeze harder to expel air; in addition, they are now pushing on a softer, floppier lung

Airflow Obstruction - 2• Due to collapse of small airways during expiration
• Normal alveolar parenchyma is radially attached to small airways and tethers them open during expiration
• Loss of alveolar parenchyma in emphysematous lungs fails to adequately tether these small airways open, resulting in premature collapse during expiration

“Experiment of Nature”Alpha-1 Antitrypsin (AAT) Deficiency
• AAT inhibits many proteases, including neutrophil elastase• Production of AAT is increased during acute inflammation• Patients with deficiency of AAT develop severe, early onset (40s-
50s) emphysema, even in the absence of smoking• Patients with deficiency of AAT who smoke develop emphysema
and destruction in their 20s-30s• In animal models, emphysema is caused by:
- Intratracheal administration of elastase- Recurrent pulmonary neutrophilia (source of elastase)- Genetic defects of native elastin (easier to degrade)
• Smoking increases acute inflammation in the lung, and leads to increased production of neutrophil elastases

Emphysema: Pathogenesis

Emphysema Pathogenesis
Destruction of lung parenchyma
Natural protective mechanisms
Balance between destructive and protective mechanisms

COPD – Inflammation
Barnes et al, Clin Chest Med 2014; 35:71-86

COPD – Oxidative Stress
Barnes et al, Clin Chest Med 2014; 35:71-86

COPD – Systemic Effects
Barnes et al, Clin Chest Med 2014; 35:71-86

Ross and Hansel, Clin Chest Med 2014; 35:219-39
COPD – Potential Therapies

Outline
• Respiratory physiology– Lung anatomy– Mechanics of respiration– Control of respiration– Gas exchange– Pulmonary function tests
• Respiratory pathology– Emphysema– Usual interstitial pneumonia
Usual Interstitial Pneumonia• Also known as idiopathic pulmonary fibrosis• UIP adds cells and fibrous tissue (scar) to the lung,
thickening and stiffening it and restricting the elastic stretching, making inspiration harder
• Manifestations include:
Decreased compliance – stiff lung
Decreased lung volumes – spirometry measurements
Impaired diffusion - DLCO measurement
Abnormal small airway function
Pulmonary hypertension
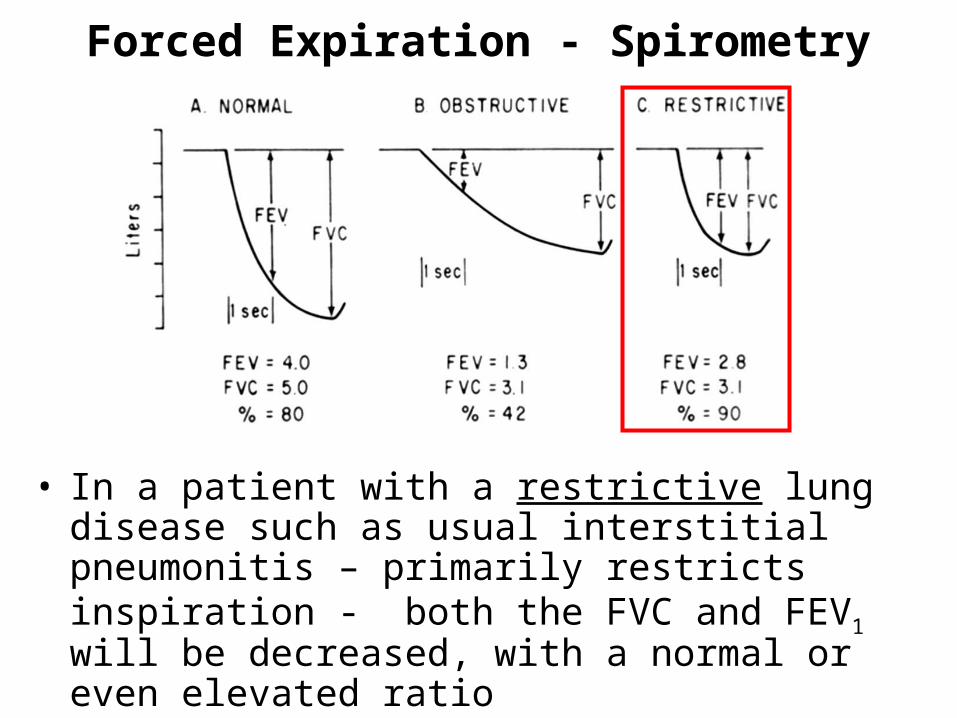
Forced Expiration - Spirometry
• In a patient with a restrictive lung disease such as usual interstitial pneumonitis – primarily restricts inspiration - both the FVC and FEV1 will be decreased, with a normal or even elevated ratio
• Monitor patients over time and effect of therapy

UIP - Gross• Honeycombing, most severe/earliest in lower zones, subpleural areas

Pleural surface Heterogeneity
UIP - Gross

• Temporal and spatial heterogeneity - patchy– End-stage (“honeycomb”) lung– Fibroblastic foci– Normal lung– Minimal active inflammation (usually)
• Architectural distortion - fibrosis
UIP - Microscopic

End-stage lung Normal lung
Fibroblastic foci
UIP - Microscopic

End Stage (“Honeycomb”) Lung

Fibroblastic Foci

Normal Lung

Clinics in Chest Disease – Table of Contents
Pathogenesis of UIP
Pathogenesis of UIP• Some form of injury to alveolar epithelium, either inhaled or
blood-borne agents• Acute and then chronic inflammation (as response to injury) of
the alveolar interstitium, and alveolar exudate• Persistence of injury (or repetitive injuries) leads to maintenance
of chronic inflammation and eventual fibrosis
• Specific interstitial lung diseases will have different inciting injuries (many of which are still unknown) and different degrees/patterns of inflammation and fibrosis
• Both environmental and genetic factors likely play roles in determining if/when/how severe/what type of lung disease a patient will develop

Pathogenesis of UIP

UIP - Morphologic Progression Normal lung
Fibroblastic foci
End-stage lung
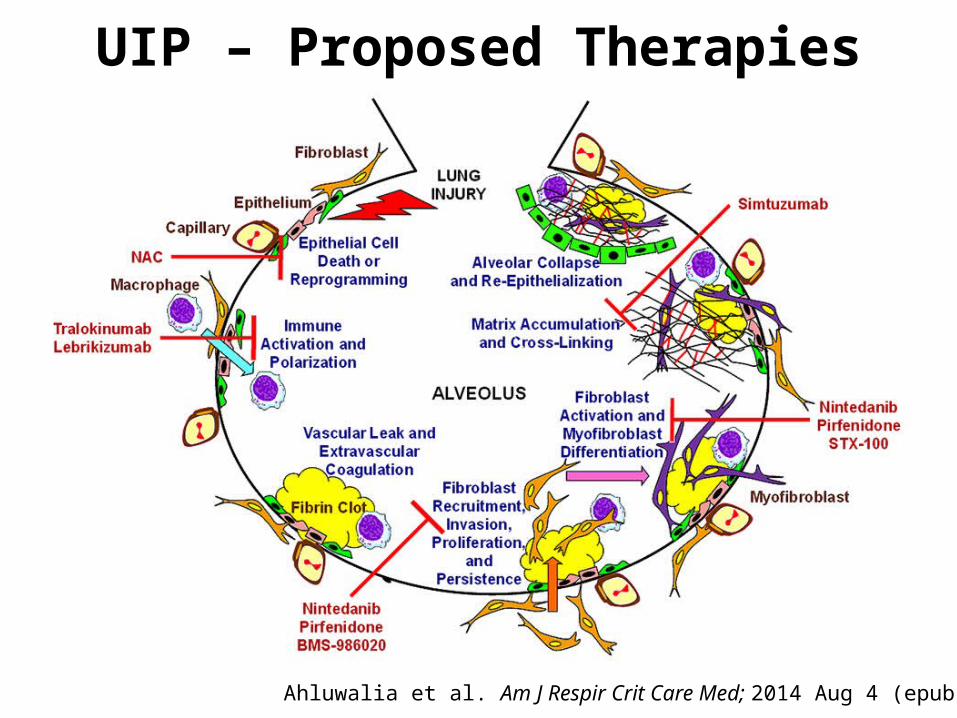
Ahluwalia et al. Am J Respir Crit Care Med; 2014 Aug 4 (epub)
UIP – Proposed Therapies

Summary and Foreshadowing
• Respiration requires coordinated effort of central and peripheral nervous system, the skeleton and skeletal muscle, lungs and heart
• COPD and UIP are pulmonary diseases that can progress to respiratory failure requiring lung transplantation (Mon. 9/22)
• What might be challenges to the use of stem cells for repair or regeneration of the lung, given the gross and microscopic pathologies of COPD and UIP?







