
Benoit Benoit ValletVallet
PôlePôle dd’’AnesthAnesthéésiesie RRééanimationanimationHôpitalHôpital HuriezHuriez
CHRU de Lille CHRU de Lille -- [email protected]@chru--lille.frlille.fr
Lille – 25 mars 2010
La “Goal-Directed
Therapy”
prévient-ellede l’insuffisance rénale postopératoire ?
Conflit d’Intérêt• Consultant pour Edwards Lifesciences

Définir l’insuffisance rénale ?
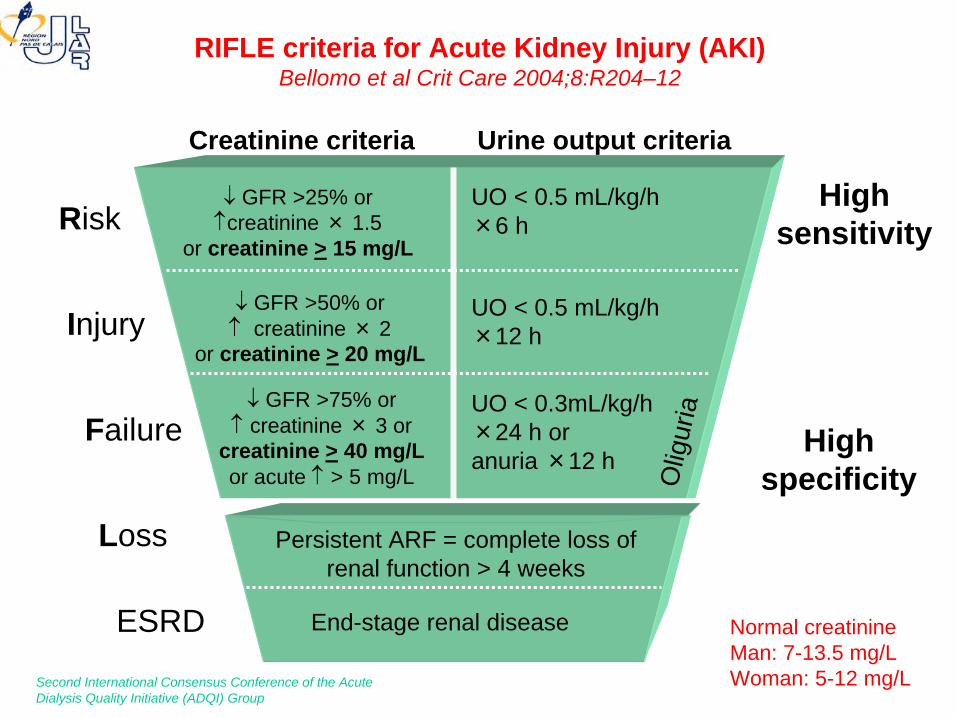
RIFLE criteria for Acute Kidney Injury (AKI) Bellomo et al Crit Care 2004;8:R204–12
ESRD End-stage renal disease
GFR >25% orcreatinine × 1.5
or creatinine
>
15 mg/L
UO < 0.5 mL/kg/h×6 h
UO < 0.5 mL/kg/h×12 h
GFR >50% or
creatinine × 2or creatinine
>
20 mg/L
Persistent ARF = complete loss of renal function > 4 weeks
UO < 0.3mL/kg/h×24 h or anuria ×12 h
GFR >75% or
creatinine × 3 orcreatinine
>
40 mg/Lor acute
> 5 mg/L Olig
uria
Risk
Injury
Failure
Loss
Highsensitivity
Highspecificity
Creatinine
criteria Urine output criteria
Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group
Normal creatinineMan: 7-13.5 mg/LWoman: 5-12 mg/L
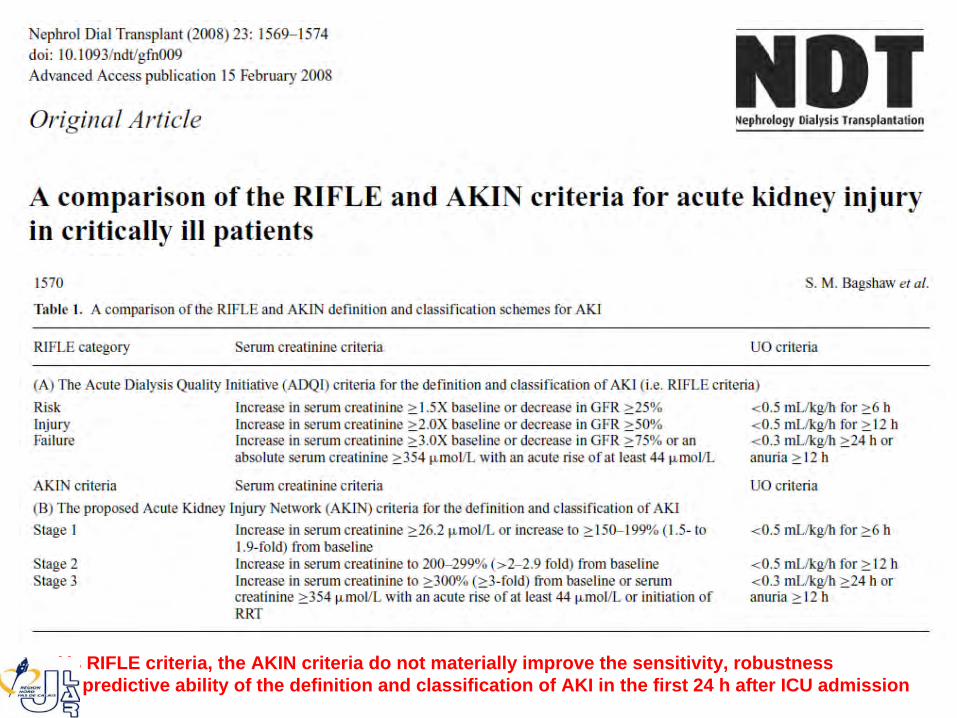
Vs RIFLE criteria, the AKIN criteria do not materially improve the sensitivity, robustnessor predictive ability of the definition and classification of AKI in the first 24 h after ICU admission
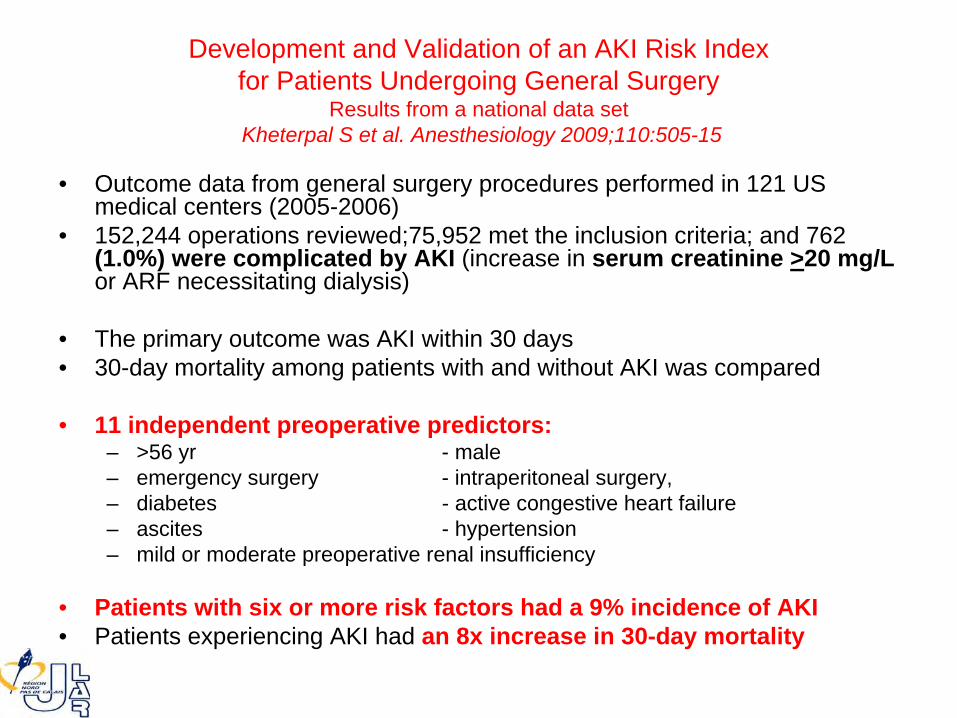
Development and Validation of an AKI Risk Index for Patients Undergoing General Surgery
Results from a national data set Kheterpal S et al. Anesthesiology 2009;110:505-15
• Outcome data from general surgery procedures performed in 121 US medical centers (2005-2006)
• 152,244 operations reviewed;75,952 met the inclusion criteria; and 762 (1.0%) were complicated by AKI
(increase in serum creatinine
>20 mg/L
or ARF necessitating dialysis)
• The primary outcome was AKI within 30 days• 30-day mortality among patients with and without AKI was compared
• 11 independent preoperative predictors:– >56 yr - male– emergency surgery - intraperitoneal surgery,– diabetes - active congestive heart failure– ascites - hypertension– mild or moderate preoperative renal insufficiency
• Patients with six or more risk factors had a 9% incidence of AKI• Patients experiencing AKI had an 8x increase in 30-day mortality
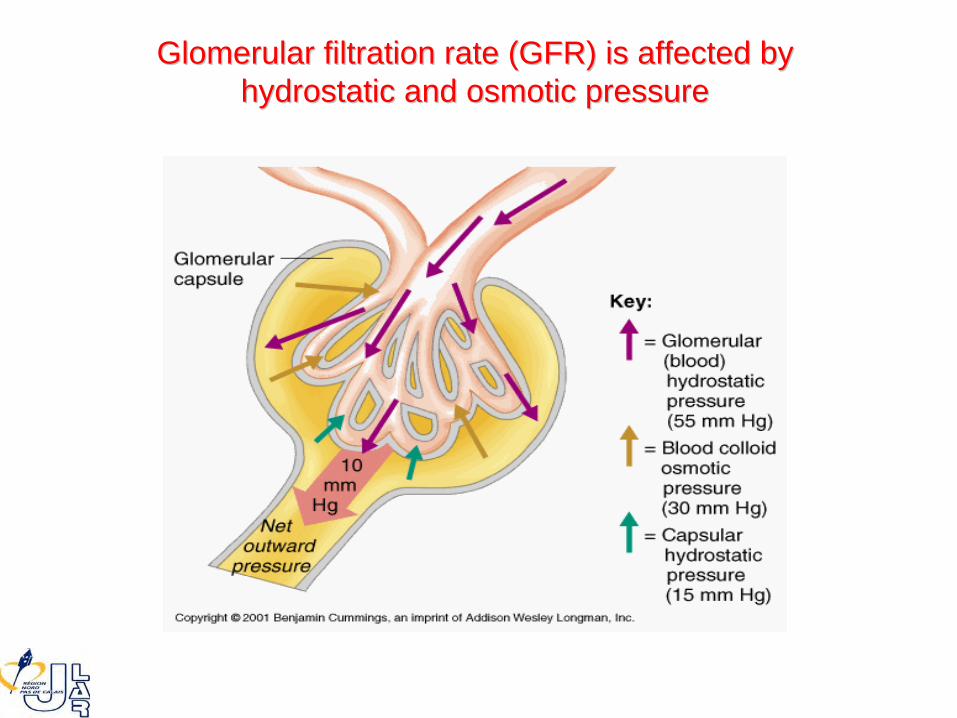
GlomerularGlomerular filtration rate (GFR) is affected byfiltration rate (GFR) is affected byhydrostatic and osmotic pressurehydrostatic and osmotic pressure

Soluté de remplissage et risque rénal ?

Type de Soluté de Remplissage et Risque Rénal Schortgen F, Girou E, Deye N, Brochard L; CRYCO Study Group
Intensive Care Med 2008;34:2157-68
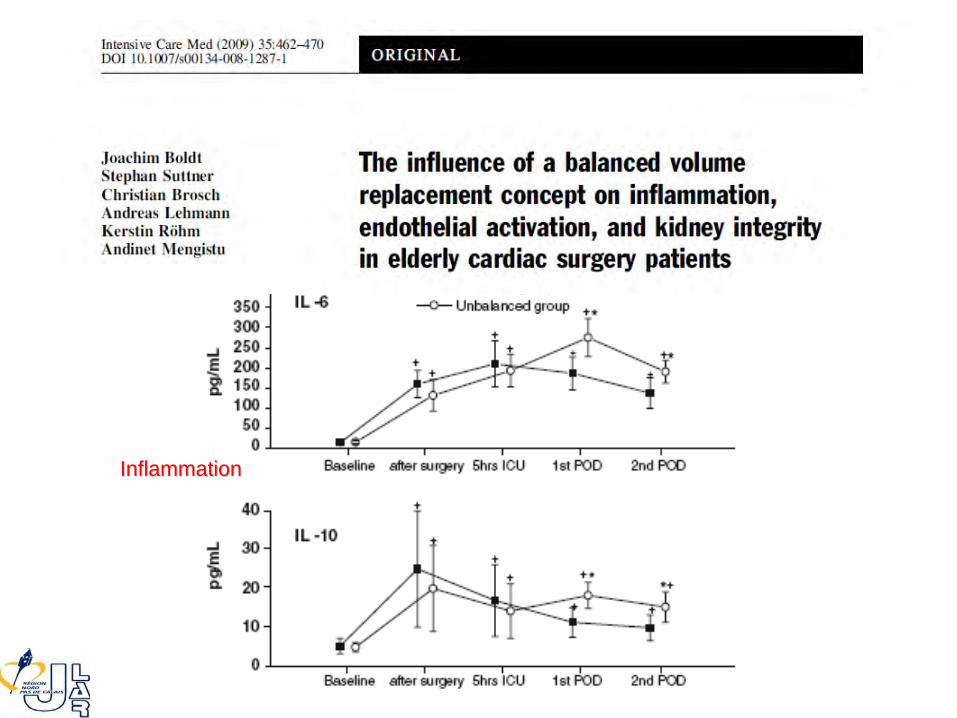
InflammationInflammation

Endothelium InjuryEndothelium Injury Kidney FunctionKidney Function
Qu’est-ce que la “Goal-Directed Therapy” (GDT) ?
En simplifiant à
l’extréme
: la GDT applique le principe de Frank et Starling
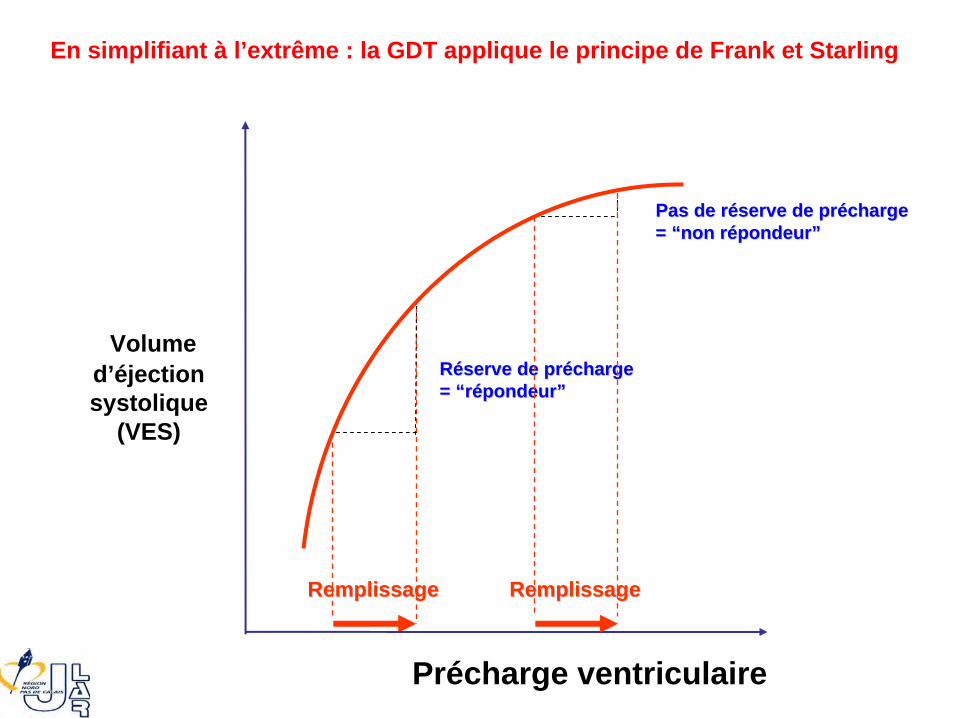
RemplissageRemplissage
Volumed’éjectionsystolique
(VES)
Précharge
ventriculaire
En simplifiant à
l’extrême : la GDT applique le principe de Frank et Starling
RRééserveserve
de de prprééchargecharge= = ““rréépondeurpondeur””
Pas de Pas de rrééserveserve
de de prprééchargecharge= = ““non non rréépondeurpondeur””
RemplissageRemplissage
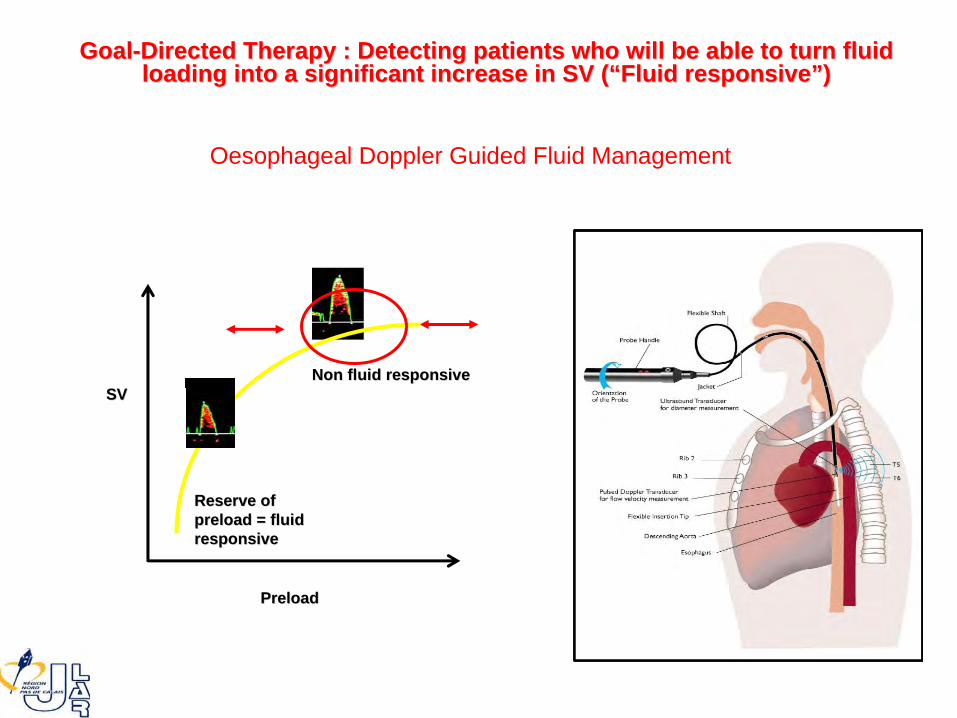
PreloadPreload
SVSV
Reserve of Reserve of preload = fluid preload = fluid responsiveresponsive
Non fluid responsiveNon fluid responsive
GoalGoal--Directed Therapy : Detecting patients who will be able to turn fDirected Therapy : Detecting patients who will be able to turn fluid luid loading into a significant increase in SV (loading into a significant increase in SV (““Fluid responsiveFluid responsive””) )
Oesophageal Doppler Guided Fluid Management

De nombreuses études ont démontré que la « maximalisation »du VES améliorait le pronostic des patients…
Mythen et al. Arch Surg 1995Sinclair et al. BMJ 1997Venn et al. Br J Anaesth 2002Gan et al. Anesthesiology 2002Conway et al. Anaesthesia 2002Wakeling HG et al. Br J Anaesth 2005Noblett SE et al. Br J Surg 2006
DURING “HIGH-RISK SURGERY”…
De nombreuses études ont démontré que la « maximalisation »du VES améliorait le pronostic des patients…
Mythen et al. Arch Surg 1995Sinclair et al. BMJ 1997Venn et al. Br J Anaesth 2002Gan et al. Anesthesiology 2002Conway et al. Anaesthesia 2002Wakeling HG et al. Br J Anaesth 2005Noblett SE et al. Br J Surg 2006
DURING “HIGH-RISK SURGERY”…
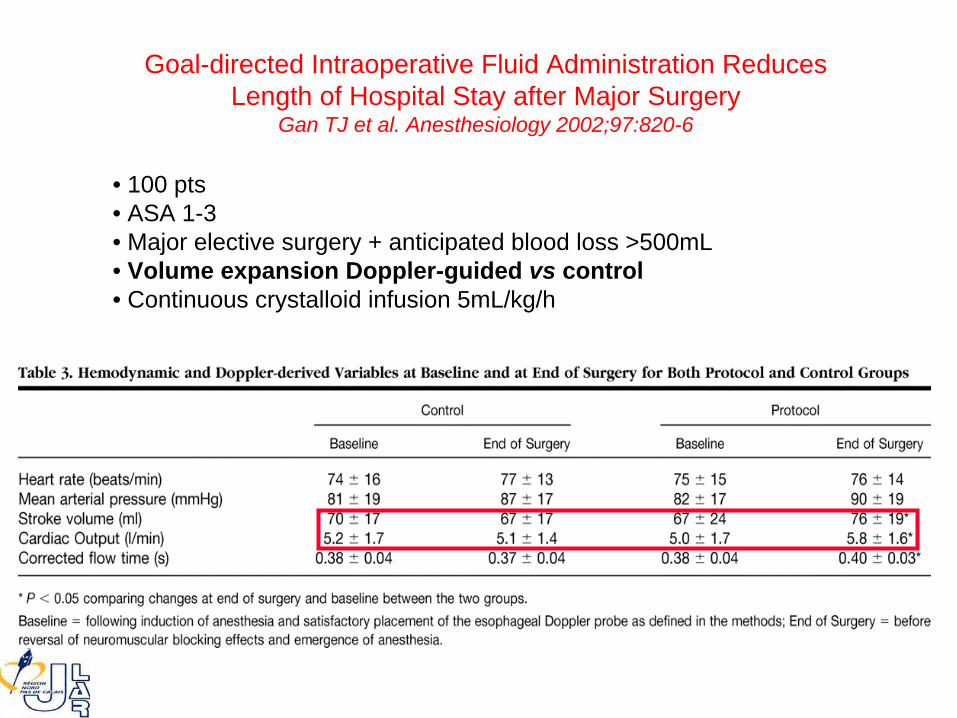
• 100 pts• ASA 1-3• Major elective surgery + anticipated blood loss >500mL• Volume expansion Doppler-guided vs control• Continuous crystalloid infusion 5mL/kg/h
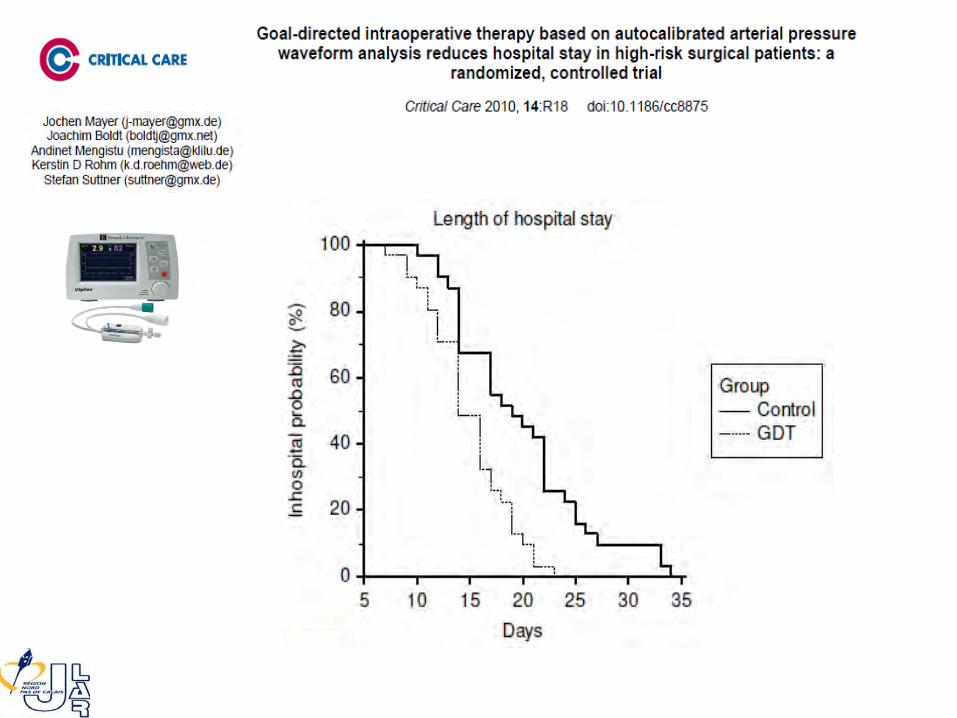
Goal-directed Intraoperative Fluid Administration Reduces Length of Hospital Stay after Major Surgery
Gan TJ et al. Anesthesiology 2002;97:820-6
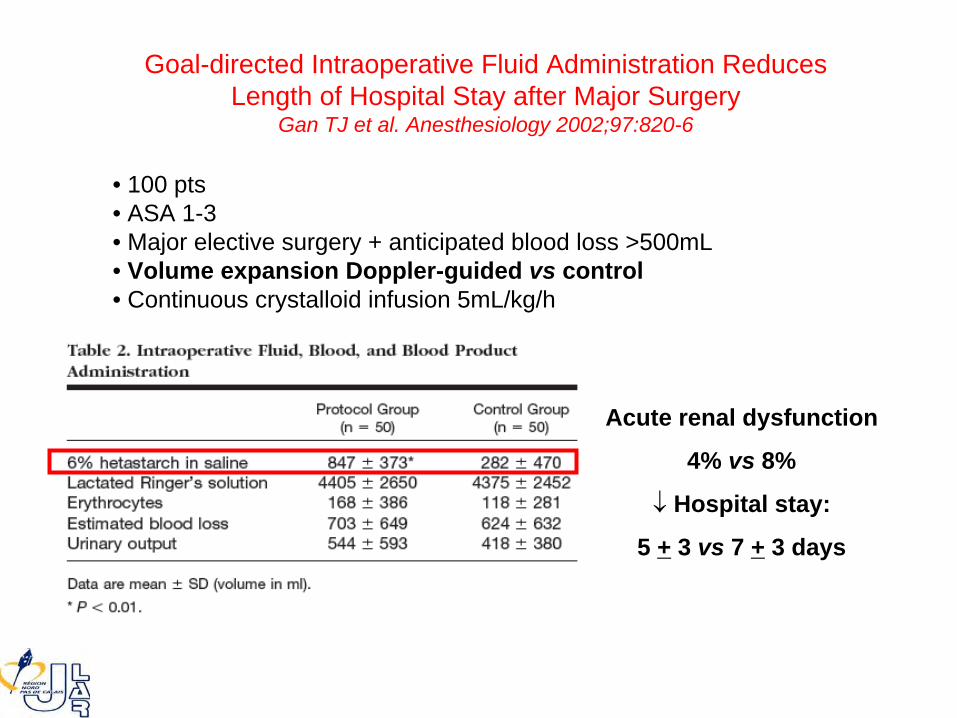
Acute renal dysfunction
4% vs 8%
Hospital stay:
5 +
3 vs 7 +
3 days
Goal-directed Intraoperative Fluid Administration Reduces Length of Hospital Stay after Major Surgery
Gan TJ et al. Anesthesiology 2002;97:820-6
• 100 pts• ASA 1-3• Major elective surgery + anticipated blood loss >500mL• Volume expansion Doppler-guided vs control• Continuous crystalloid infusion 5mL/kg/h

Acute renal dysfunction
4% vs 8%
Hospital stay:
5 +
3 vs 7 +
3 days
Goal-directed Intraoperative Fluid Administration Reduces Length of Hospital Stay after Major Surgery
Gan TJ et al. Anesthesiology 2002;97:820-6
• 100 pts• ASA 1-3• Major elective surgery + anticipated blood loss >500mL• Volume expansion Doppler-guided vs control• Continuous crystalloid infusion 5mL/kg/h

Intraoperative
Oesophageal
Doppler Guided Fluid ManagementShortens Postoperative Hospital Stay after
Major Bowel SurgeryWakeling et al. Brit J Anaest 2005;95:634-42
GDT-Doppler patients:- Larger volume of iv colloids than controls (median 2000 vs 1500 mL, P<0.01)- Higher CO- Higher SV- Higher DO2
-
GI morbidity- 45.3 vs 14.1% (p<0.001)
- Renal- 3.1 vs 4.7% (p=0.661)
-
Total number of
patients withComplications- 59.3 vs 37.5% (p=0.013)
64 ctrls vs 64 GDT

En simplifiant à
l’extrême : la GDT applique le principe de Frank et Starling

En simplifiant à
l’extrême : la GDT applique le principe de Frank et Starling
Est-ce suffisant ?
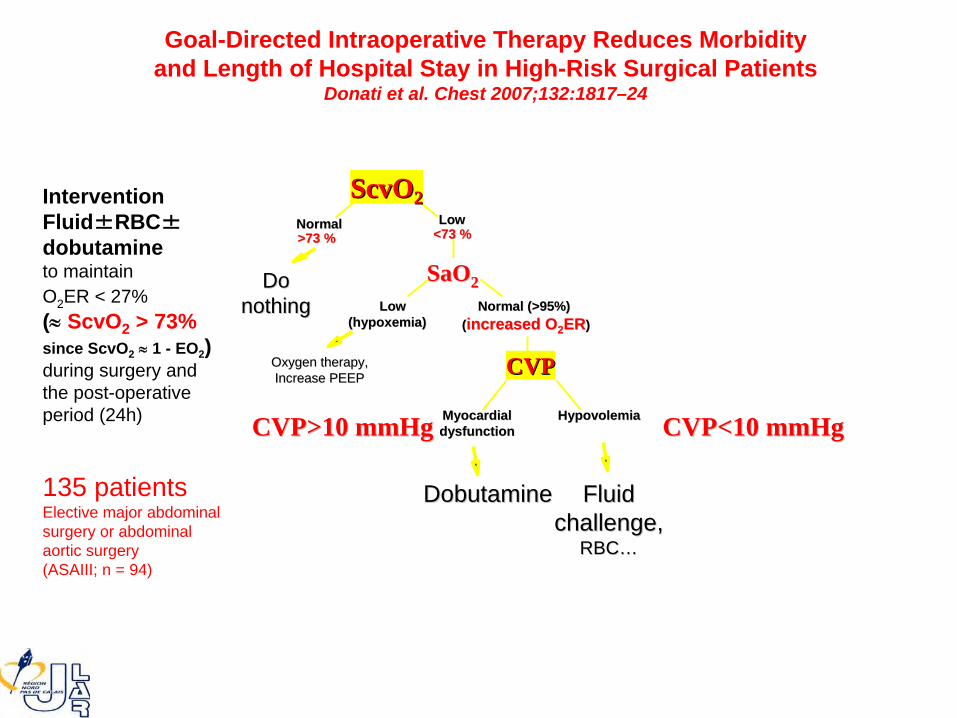
InterventionFluid±RBC±
dobutamineto maintainO2 ER < 27%(
ScvO2
> 73% since ScvO2
1 -
EO2
) during surgery and the post-operative period (24h)
135 patientsElective major abdominalsurgery or abdominalaortic surgery(ASAIII; n = 94)
NormalNormal>73 %>73 %
LowLow<73 %<73 %
Oxygen therapy,Oxygen therapy,Increase PEEPIncrease PEEP
DoDonothingnothing
ScvOScvO22
Normal (>95%)Normal (>95%)((increased Oincreased O22
ERER))
SaOSaO22LowLow
(hypoxemia)(hypoxemia)
FluidFluidchallenge,challenge,
RBCRBC……
CVPCVP
HypovolemiaHypovolemiaMyocardialMyocardialdysfunctiondysfunction
DobutamineDobutamine
CVP<10 mmHgCVP<10 mmHgCVP>10 mmHgCVP>10 mmHg
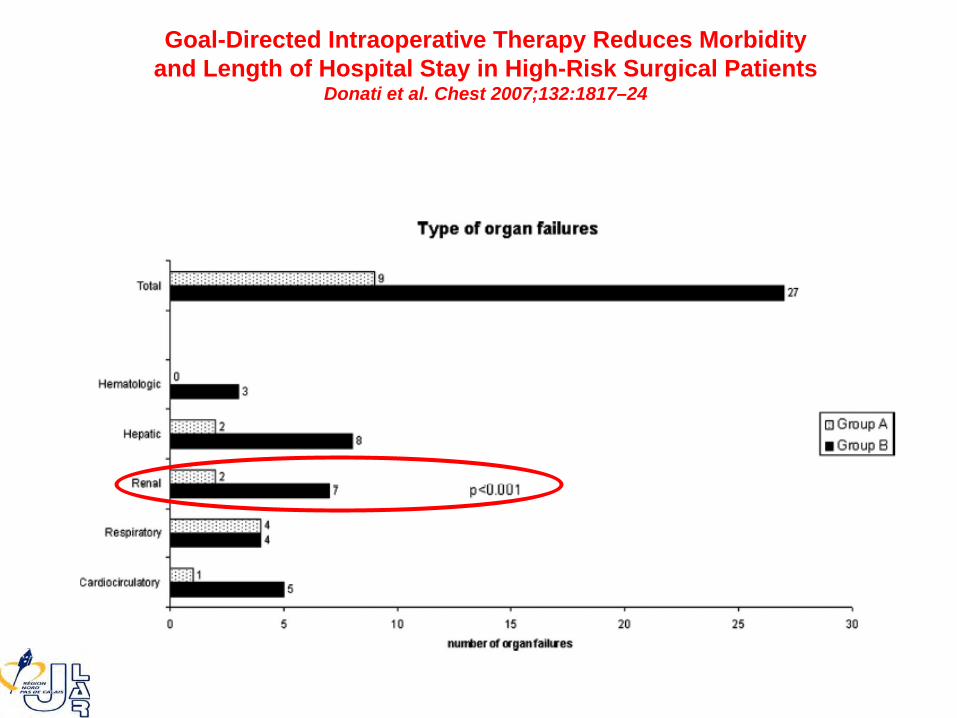
Goal-Directed Intraoperative
Therapy Reduces Morbidityand Length of Hospital Stay in High-Risk Surgical Patients
Donati et al. Chest 2007;132:1817–24

44.1%2.6+4.0g/kg/min
4.5%0.4+2.2g/kg/min
Goal-Directed Intraoperative
Therapy Reduces Morbidityand Length of Hospital Stay in High-Risk Surgical Patients
Donati et al. Chest 2007;132:1817–24
Goal-Directed Intraoperative
Therapy Reduces Morbidityand Length of Hospital Stay in High-Risk Surgical Patients
Donati et al. Chest 2007;132:1817–24
En simplifiant à
l’extrême : la GDT applique le principe de Frank et Starling
En simplifiant à
l’extrême : la GDT applique le principe de Frank et Starling
La GDT pourrait être avantageusement complémentéepar un paramètre «
global
»
d’utilisation de l’O2
chez les patients les plus à
risque…
En simplifiant à
l’extrême : la GDT applique le principe de Frank et Starling
La GDT pourrait être avantageusement complémentéepar un paramètre «
global
»
d’utilisation de l’O2
chez les patients les plus à
risque…
Quelles sont les preuves ?
• “Perioperative hemodynamic optimization” or “goal-directed therapy” refers to the perioperative monitoring and manipulation of physiologic hemodynamic parameters by means of fluids, red blood cells, and inotropic drugs
• With the aim to reach values of cardiac output and oxygen delivery to face the increase in oxygen demand and to prevent organ failure

20 studies4,220 patients
13 as “high quality studies”
9 enrolled “high-risk” patients
Sensitivity analysis combining:- Grade “R” of RIFLE classification- Stage “1” of AKIN classification- SCr>20 mg/L, increase>50%or by 5 mg/L or need of RRT,disregarding urine output

5.4% 8.3%

6.1% 9.2%


7.3% 11.2%

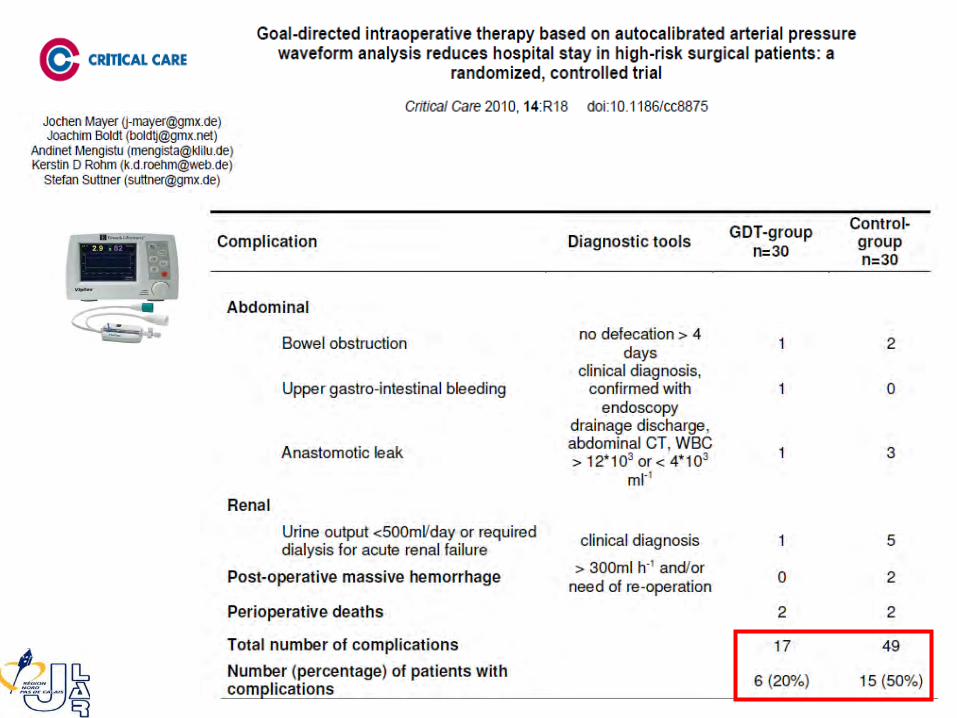
Un effet de la GDT sur d’autres organes ?
• 16 randomized controlled trials (3410 participants)
• GI complications
were ranked as major
(required radiological or surgical intervention or life-threatening condition) or minor
(no or
only pharmacological treatment required)
• Major GI complications were significantly reduced by GDT when compared with a control group (OR, 0.42; 95% CI, 0.27-0.65)
• Minor GI complications were also significantly decreased in the GDT group (OR, 0.29; 95% CI, 0.17-0.50)
• Treatment did not reduce hepatic injury rate (OR, 0.54; 95% CI, 0.19-1.55)
Goal-Directed Haemodynamic Therapy and Gastrointestinal Complications in Major Surgery: A Meta-Analysis of Randomized Controlled Trials
Giglio MT, Marucci M, Testini M, Brienza N Br J Anaesth. 2009 Nov;103(5):637-46

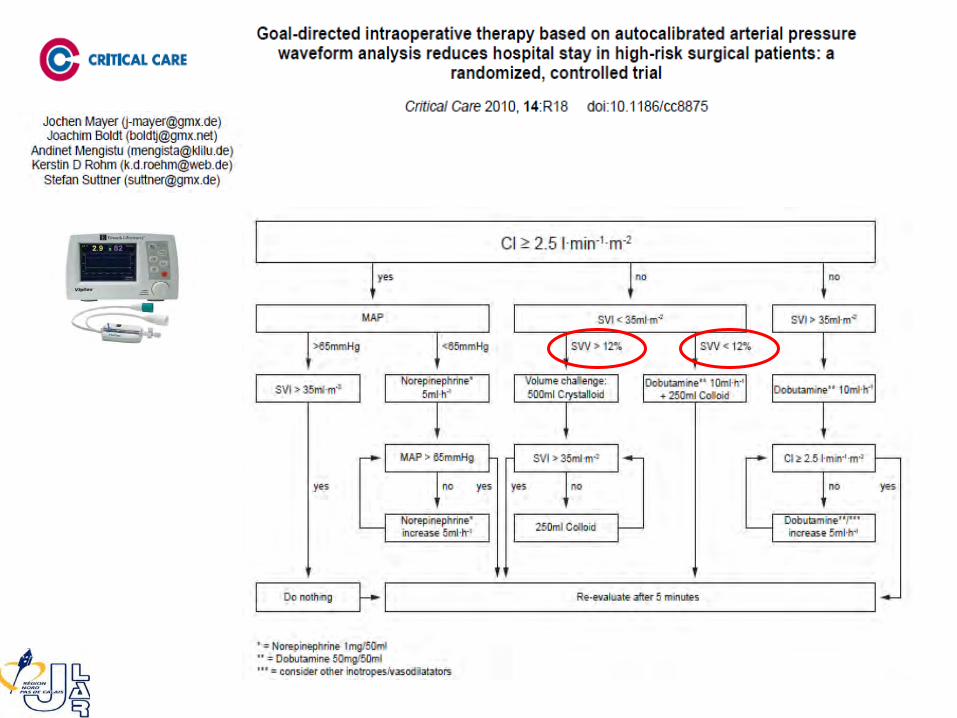
Quels outils au quotidien ?

Intellivue, Philips
Flotrac/Vigileo, Edwards
PiCCO plus, Pulsion
S/5, GE
Monitorage Automatisé
et Invasif (KT artériel) de la Réponse au Remplissage

« Plateau »
∆PFaible PPV
Portio
n acs
enda
nte
Précharge
(P)
VES
∆P =
modifications cycliques de préchargeinduites par la ventilation mécanique
Large PPV20.5%
4.5%
REMPLISSAGEREMPLISSAGE
PPPPmaxmax
--
PPPPminmin
((PPPPmaxmax
++
PPPPminmin
) /2) /2PPV =PPV =
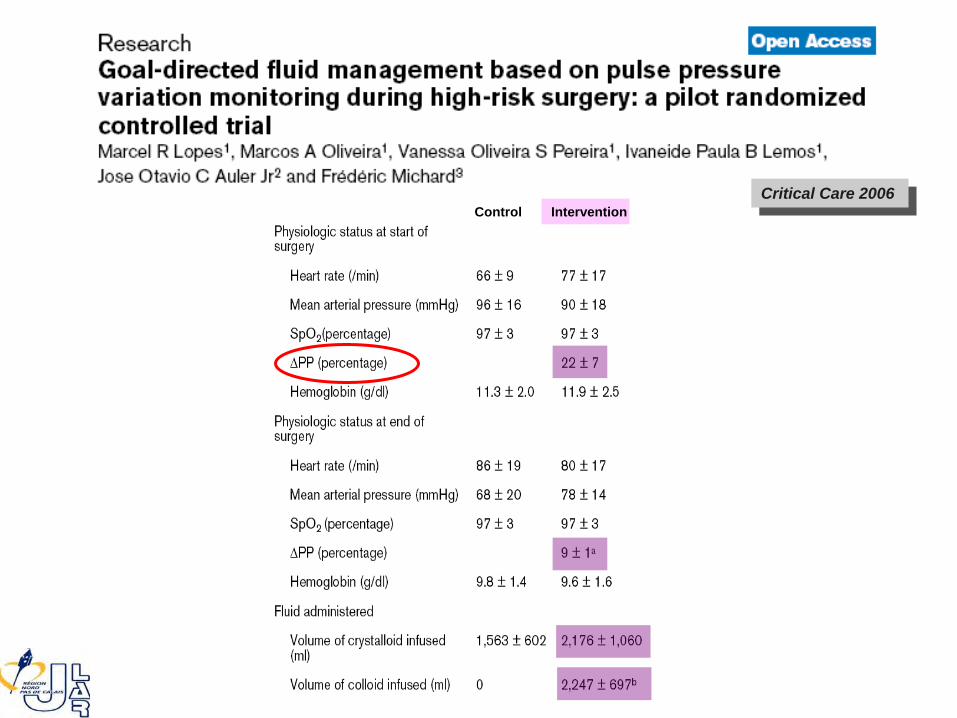
Critical Care 2006Critical Care 2006Control Intervention



PVI/SpO2 , Masimo
Finometer, Finapres
CNAP, CNS
Monitorage Automatisé
et Non Invasif de la Réponse au Remplissage ?
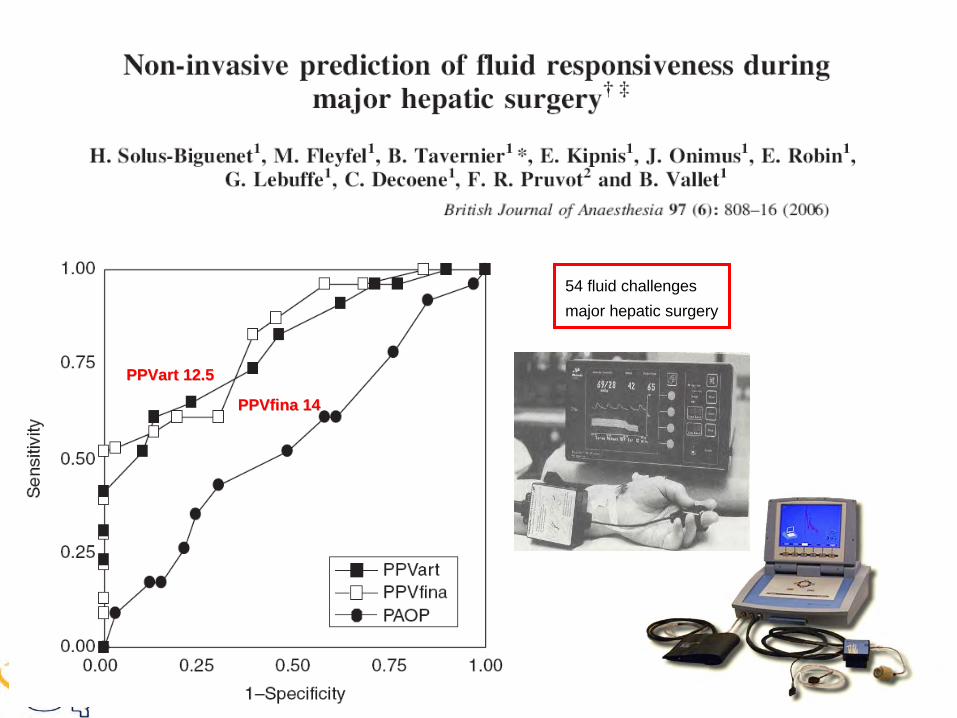
54 fluid challengesmajor hepatic surgery
PPVartPPVart
12.512.5
PPVfinaPPVfina
1414

Adapted
from
Cannesson
M. et al. Br
J Anesth
2008;101:200-6
A PVI >14% before
volume expansion discriminatedbetween
responders
and non-responderswith
81% sensitivity
and 100% specificity
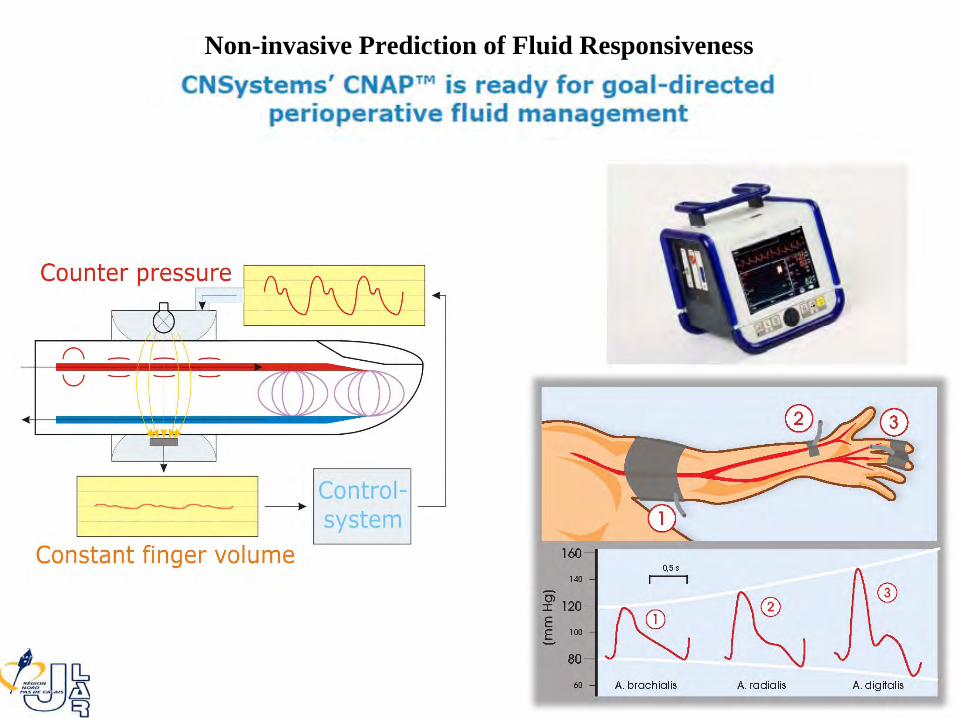
Non-invasive Prediction of Fluid Responsiveness

PAni
PAi
Pairway
Monnet X, Dres M, Ferré A, Bleibtreu A, Richard C, Teboul JLESICM 2009 poster # 0293
Respiratory variation and invasive estimation of arterial pressure

Pulse pressure variation and stroke volume variation: from
flying
blind
to flying
right?Cannesson M, Vallet B, Michard F. Br J Anaesth 2009;103:896-7
La “Goal-Directed Therapy” (GDT) prévient-elle de l’insuffisance rénale postopératoire ?
• Oui (vraisemblablement) quand la GDT:– Est débutée en pré ou per-opératoire– Est réalisée chez les patients à risque:
• Sujet âgé et/ou avec comorbidités (diabète, HTA, cardiopathie)• Chirurgie d’urgence ou intrapéritonéale• Présentant une instabilité hémodynamique préopératoire
– Est réalisée par le remplissage et l’utilisation d’inotropes• Le choix du type de soluté de remplissage doit faire l’objet
d’études complémentaires• Dans la métaanalyse de Brienza et al. (CCM 2009), la mortalité
est réduite par la GDT (OR 0.50; CI 0.31–0.80; p = 0.004), quoique l’hétérogénéité statistique soit importante
• Il apparaît raisonable d’identifier en per-opératoire les patients (selon la chirurgie envisagée) qui doivent bénéficier de la GDT pour choisir le monitorage le plus adapté à la conduite du traitement







