
Lifestyle Medicine and Primary Care: Implementing Effective Lifestyle Changes
Brad Biskup, PA-C, MHS, MALifestyle Medicine Clinic
Pat and Jim Calhoun Cardiology Center
University of Connecticut Health
Learning Objectives
• Describe the benefits of lifestyle as
medicine.
• Understand guidelines for diet and
exercise.
• Identify the cost-effectiveness of
implementing lifestyle medicine within
primary care.
• 43 year old male:
– Hypertension - dyslipidemia
– insulin resistant diabetes - morbid obesity
– obstructive sleep apnea (OSA) - family history of CAD
• Meds: metformin, glyburide, Lisinopril, furosemide,
Nexium, wellbutrin, Androgel, vitamin D3, lovastatin,
trazadone, Celexa, and temazepam.
• After 3 years: stopped glyburide and Lisinopril; ½
dose of lovastatin and furosemide
Results?
“Bill”
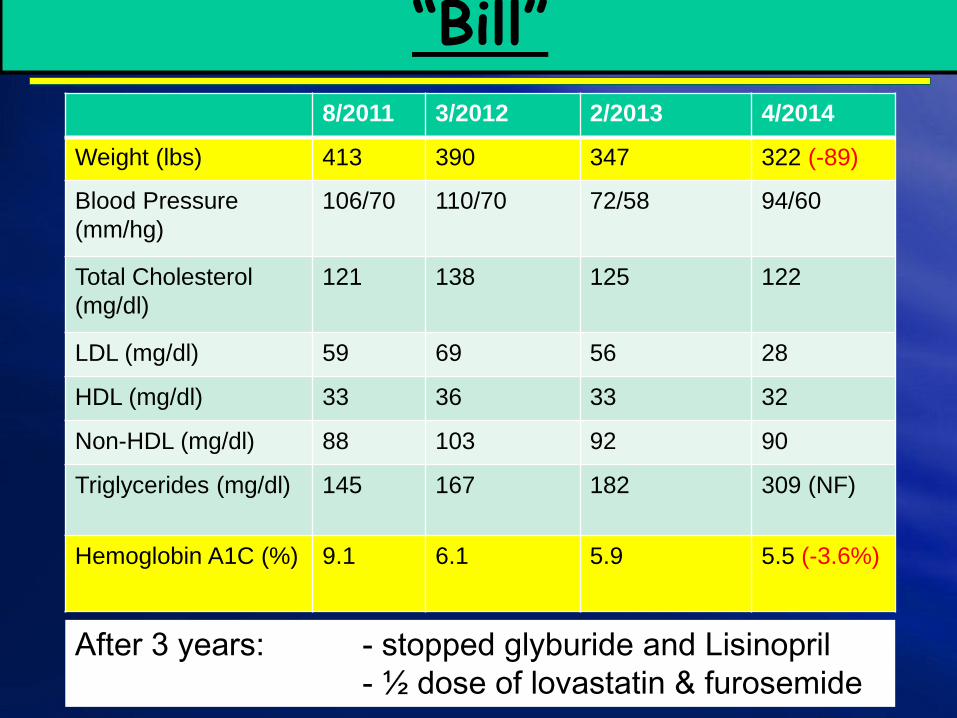
8/2011 3/2012 2/2013 4/2014
Weight (lbs) 413 390 347 322 (-89)
Blood Pressure
(mm/hg)
106/70 110/70 72/58 94/60
Total Cholesterol
(mg/dl)
121 138 125 122
LDL (mg/dl) 59 69 56 28
HDL (mg/dl) 33 36 33 32
Non-HDL (mg/dl) 88 103 92 90
Triglycerides (mg/dl) 145 167 182 309 (NF)
Hemoglobin A1C (%) 9.1 6.1 5.9 5.5 (-3.6%)
“Bill”
After 3 years: - stopped glyburide and Lisinopril
- ½ dose of lovastatin & furosemide

Cause of Disease:Is it due to genetics?
The World Health Organization has
estimated that if the major risk factors for
chronic disease were eliminated, at least:
– 80% of all heart disease, stroke, and
type 2 diabetes would be prevented,
and
– more than 40% of cancer cases would
be prevented.
World Health Organization. Preventing chronic diseases: a vital
investment. Geneva: World Health Organization; 2005.
What is Lifestyle Medicine?
• Lifestyle Medicine (LM) is the use of
lifestyle interventions in the treatment
and management of disease.
– Interventions:
• nutrition
• exercise
• stress management
• smoking cessation
• a variety of other non-drug modalities
American College of Lifestyle Medicine
http://www.lifestylemedicine.org/define
Why Lifestyle Medicine?
• Today:
– 7 in 10 deaths in the U.S. are related to preventable
diseases such as obesity, diabetes, high blood pressure,
heart disease and cancer.
– 75% of our health care dollars are spent treating such
diseases.
– However, only 3% of our health care dollars go toward
prevention.”
- American Public Health Association
Current “Health Care System” in the U.S. =
“Disease Management System”
• A growing body of scientific evidence has
demonstrated that lifestyle intervention is
an essential component in the treatment of
chronic disease that can be as effective
as medication, but without the risks and
unwanted side-effects.
American College of Lifestyle Medicine
http://www.lifestylemedicine.org/define
Lifestyle Medicine Research
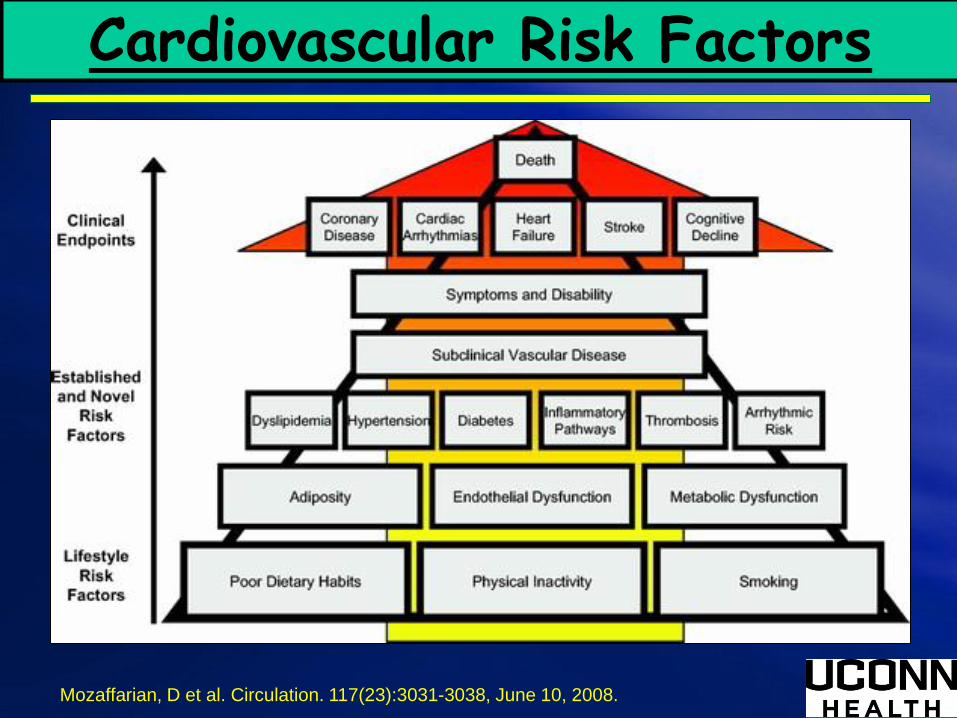
Cardiovascular Risk Factors
Mozaffarian, D et al. Circulation. 117(23):3031-3038, June 10, 2008.

• Treats individual risk factors
• Patient is often passive
recipient of care
• Patient is not required to
make big changes
• Treatment is often short
term
• Responsibility falls mostly
on the clinician
• Medication is often the
“end” treatment
Conventional Lifestyle
• Treats lifestyle causes
• Patient is active partner in
care
• Patient is required to make
big changes
• Treatment is always long
term
• Responsibility falls mostly on
the patient
• Medication, but as an adjunct
to lifestyle change
http://c.ymcdn.com/sites/www.acpm.org/resource/resmgr/lmi-files/lifestylemedicine-literature.pdf
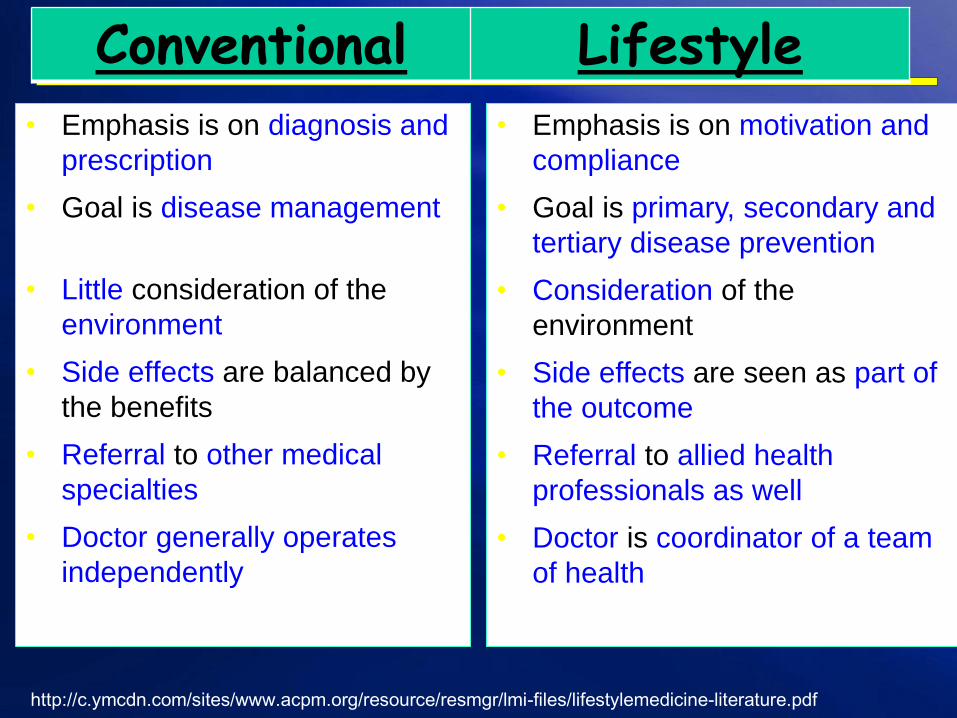
• Emphasis is on diagnosis and
prescription
• Goal is disease management
• Little consideration of the
environment
• Side effects are balanced by
the benefits
• Referral to other medical
specialties
• Doctor generally operates
independently on a one-to-one
basis
• Emphasis is on motivation and
compliance
• Goal is primary, secondary and
tertiary disease prevention
• Consideration of the
environment
• Side effects are seen as part of
the outcome
• Referral to allied health
professionals as well
• Doctor is coordinator of a team
of health
http://c.ymcdn.com/sites/www.acpm.org/resource/resmgr/lmi-files/lifestylemedicine-literature.pdf
Conventional Lifestyle
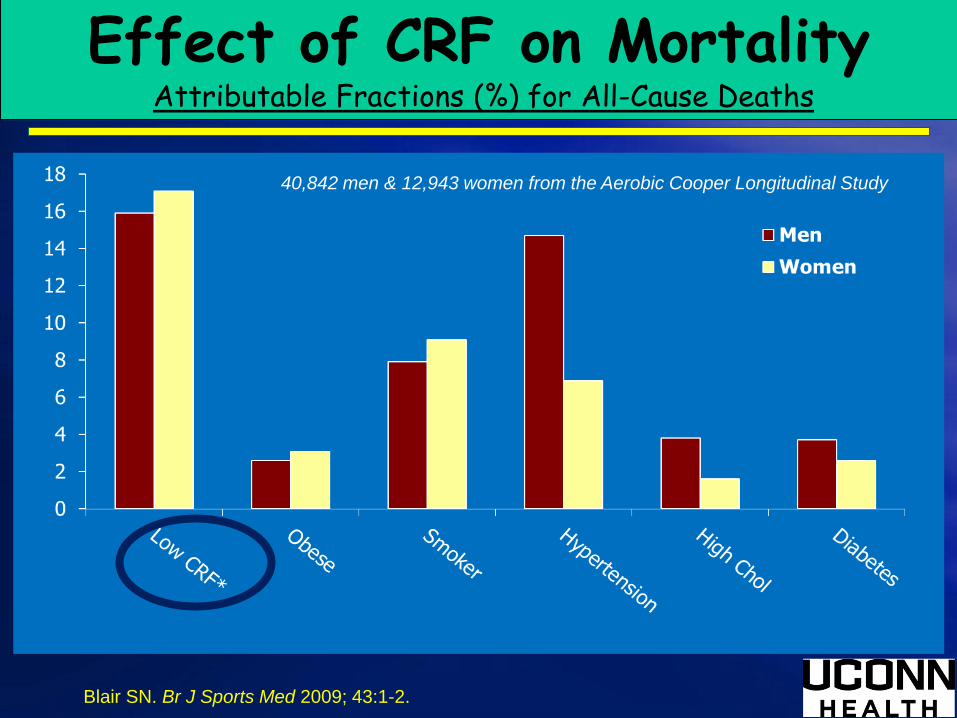
40,842 men & 12,943 women from the Aerobic Cooper Longitudinal Study
Effect of CRF on MortalityAttributable Fractions (%) for All-Cause Deaths
Blair SN. Br J Sports Med 2009; 43:1-2.

Lifestyle Medicine
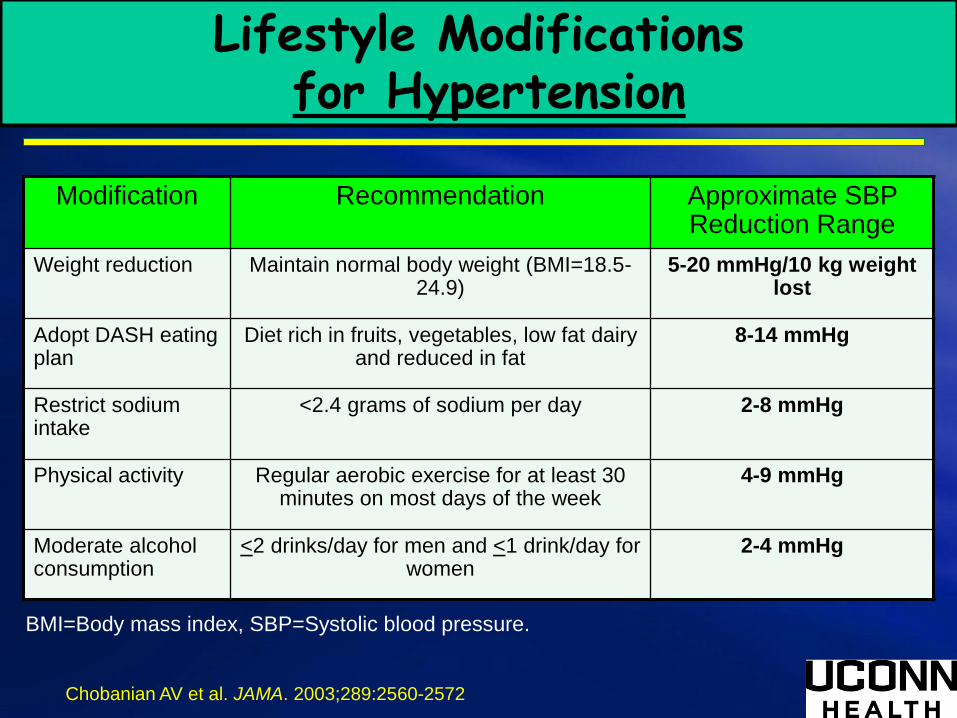
Modification Recommendation Approximate SBP Reduction Range
Weight reduction Maintain normal body weight (BMI=18.5-24.9)
5-20 mmHg/10 kg weight lost
Adopt DASH eating plan
Diet rich in fruits, vegetables, low fat dairy and reduced in fat
8-14 mmHg
Restrict sodium intake
<2.4 grams of sodium per day 2-8 mmHg
Physical activity Regular aerobic exercise for at least 30 minutes on most days of the week
4-9 mmHg
Moderate alcohol consumption
<2 drinks/day for men and <1 drink/day for women
2-4 mmHg
Lifestyle Modificationsfor Hypertension
Chobanian AV et al. JAMA. 2003;289:2560-2572
BMI=Body mass index, SBP=Systolic blood pressure.
Medication vs. Lifestyle Medicine:
Diabetes Risk
Diabetes Prevention Program
• 3,234 IGT (51 y, BMI 34, 68% female,
45% minority) randomized for 2.8 y
(study stopped early) to
– placebo, or
– metformin (850mg bid), or
– lifestyle-modification (7% weight loss
and 150 minutes physical activity per
week)
Diabetes Prevention Program Research Group, . N Engl J Med 2002;346:393-403
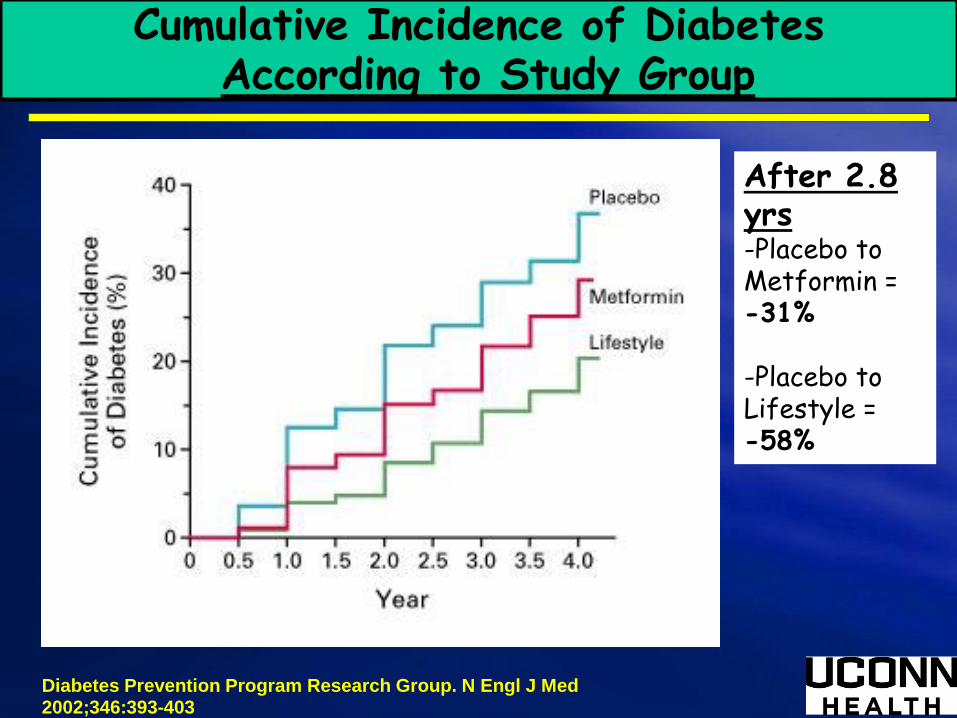
Cumulative Incidence of DiabetesAccording to Study Group
Diabetes Prevention Program Research Group. N Engl J Med 2002;346:393-403
After 2.8 yrs-Placebo to Metformin = -31%
-Placebo to Lifestyle = -58%
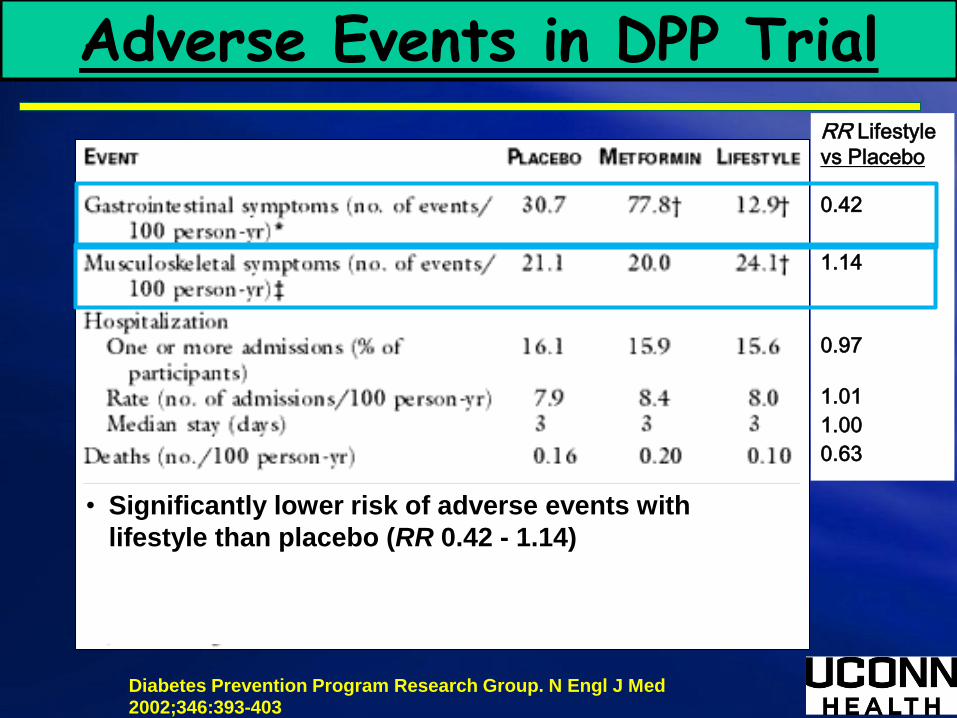
Adverse Events in DPP TrialRR Lifestyle
vs Placebo
0.42
1.14
0.97
1.01
1.00
0.63
• Significantly lower risk of adverse events with
lifestyle than placebo (RR 0.42 - 1.14)
Diabetes Prevention Program Research Group. N Engl J Med 2002;346:393-403
Exercise WithinLifestyle Medicine
Exercise and Disease
• Research shows that exercise
helps treat and prevent more
than 40 chronic diseases, such as
diabetes, heart disease, obesity
and hypertension.
Exercise and Cardiovascular Risk Reduction: Time to Update the Rationale for Exercise?
> 40% of the risk reduction associated with exercise cannot be
explained by changes in risk factors
Cardioprotection via a “Vascular Conditioning” Effect
Improvement in nitric oxide vasodilator function
Improved vascular function + altered vascular structure
Increased Parasympathetic, Decreased Sympathetic
Enhanced heart rate variability
?
Green DJ et al., J Appl Physiol 2008;105:766-768.
Exercise and Disease
➢Can reduce mortality and the risk of recurrent
breast cancer by approximately 50%.1
➢Can lower the risk of colon cancer by over 60%.2
➢Can reduce the risk of developing of Alzheimer’s
disease by approximately 40%.3
➢Reduces the incidence of high blood pressure
and heart disease by approximately 40%.4-5
1- Physical activity and survival after breast cancer diagnosis. Holmes MD et al. JAMA 2005; 293:2479
2- Physical activity and colon cancer: confounding or interaction? Medicine & Science in Sports & Exercise: June 2002 - Volume
34 - Issue 6 - pp 913-919
3- Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Larsen EB et al.
Annals of Internal Medicine 2006; 144:73-81.
4- Cardiorespiratory fitness is an independent predictor of hypertension incidence among initially normotensive healthy women.
Barlow CE et al. Am J Epidemiol 2006; 163:142-50
5- Exercise in the prevention of coronary heart disease: today's best buy in public health. Med Sci Sports Exerc. 1994
Jul;26(7):807-14.
Exercise and Disease
➢Lowers the risk of stroke by 27%.1
➢Reduces the incidence of diabetes by
approximately 50%.2-3
➢Can decrease depression as effectively as Prozac
or behavioral therapy. 4
➢Muscle strength decreases mortality risk. 5
1- Physical activity and risk of stroke in women. JAMA. 2000 Jun 14;283(22):2961-
2- The association between cardiorespiratory fitness and impaired fasting glucose and type 2 diabetes mellitus in men.
Wei M et al. Annals of Internal Medicine. 1999
3- Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin.
DPP Research Group. New England Journal of Medicine 2002; 346:393-403
The Diabetes Prevention Program Research Group: Within-trial cost-effectiveness of lifestyle intervention or
metformin for the primary prevention of type 2 diabetes. DPP Res Group. Diab Care 2003; 26:2518.
4- Exercise treatment for depression: efficacy and dose response. Dunn A et al. American Journal of Preventive Medicine 2005
Jan;28(1):1-8.
5- Association between muscular strength and mortality in men. Ruiz JR, Sui X, Lobelo F, Morrow JR, Jackson AW, Blair SN.
BMJ 2008; 337:a439.
Key Guidelines for Adults
➢ All adults should avoid inactivity. Some
physical activity is better than none, and
adults who participate in any amount of
physical activity gain some health benefits.
➢ For substantial health benefits, adults should
do at least 150 minutes (2 hours and 30
minutes) a week of moderate intensity, or 75 minutes (1
hour and 15 minutes) a week of vigorous-intensity aerobic
physical activity, or an equivalent combination of moderate-
and vigorous-intensity aerobic activity. Aerobic activity
should be performed in episodes of at least 10 minutes, and
preferably, it should be spread throughout the week.http://www.health.gov/paguidelines/
Key Guidelines for Adults (more)
➢ For additional and more extensive health benefits, adults
should increase their aerobic physical activity to 300 minutes
(5 hours) a week of moderate-intensity, or 150 minutes a
week of vigorous-intensity aerobic physical activity, or an
equivalent combination of moderate- and vigorous-intensity
activity. Additional health benefits are gained by engaging in
physical activity beyond this amount.
➢ Adults should also do muscle-strengthening activities that are
moderate or high intensity and involve all major muscle
groups on 2 or more days a week, as these activities provide
additional health benefits.
http://www.health.gov/paguidelines/
Key Guidelines for Older Adults
The Key Guidelines for Adults also apply to older adults. In addition, the
following Guidelines are just for older adults:
➢ When older adults cannot do 150 minutes of moderate-intensity aerobic
activity a week because of chronic conditions, they should be physically
activity as their abilities and conditions allow.
➢ Older adults should do exercises that maintain or improve balance if
they are at risk of falling.
➢ Older adults should determine their level of effort for physical activity
related to their level of fitness.
➢ Older adults with chronic conditions should under-
stand whether and how their conditions affect
their ability to do regular physical activity safely.
http://www.health.gov/paguidelines/
The Beneficial Effects of Increasing Physical Activity: It's About Overload, Progression, and Specificity
• Overload is the physical stress placed on the body when
physical activity is greater in amount or intensity than usual.
• Aerobic
• Muscle Strength
• Balance
• Progression is closely tied to overload. Once a person reaches
a certain fitness level, he or she progresses to higher levels of
physical activity by continued overload and adaptation.
– Small, progressive changes in overload help the body adapt
to the additional stresses while minimizing the risk of injury.–
• Specificity means that the benefits of physical activity are
specific to the body systems that are doing the work.
http://www.health.gov/paguidelines/
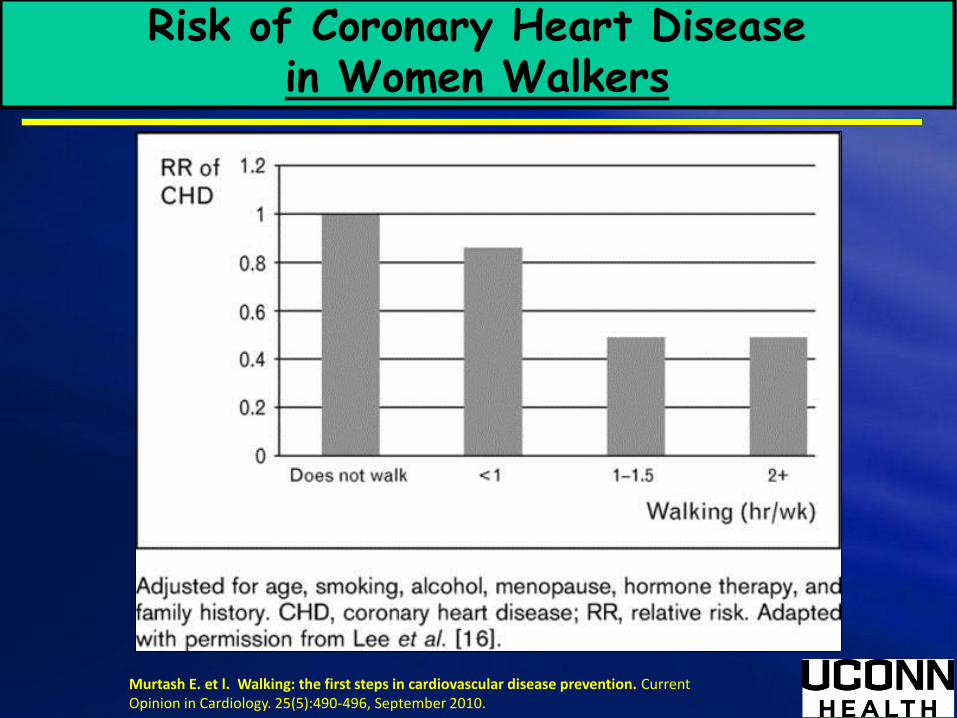
2Murtash E. et l. Walking: the first steps in cardiovascular disease prevention. Current Opinion in Cardiology. 25(5):490-496, September 2010.
Risk of Coronary Heart Disease in Women Walkers
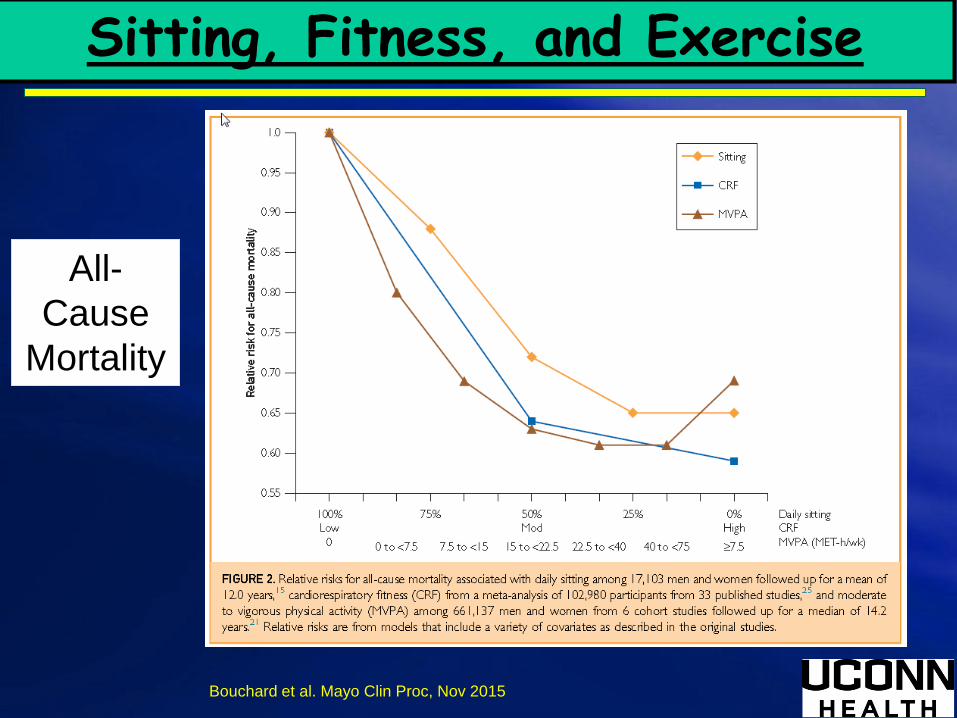
Sitting, Fitness, and Exercise
Bouchard et al. Mayo Clin Proc, Nov 2015
All-
Cause
Mortality

Williams, M et al. Circulation. 116(5):572-584, July 31, 2007.
Aerobic vs. Resistance Exercise
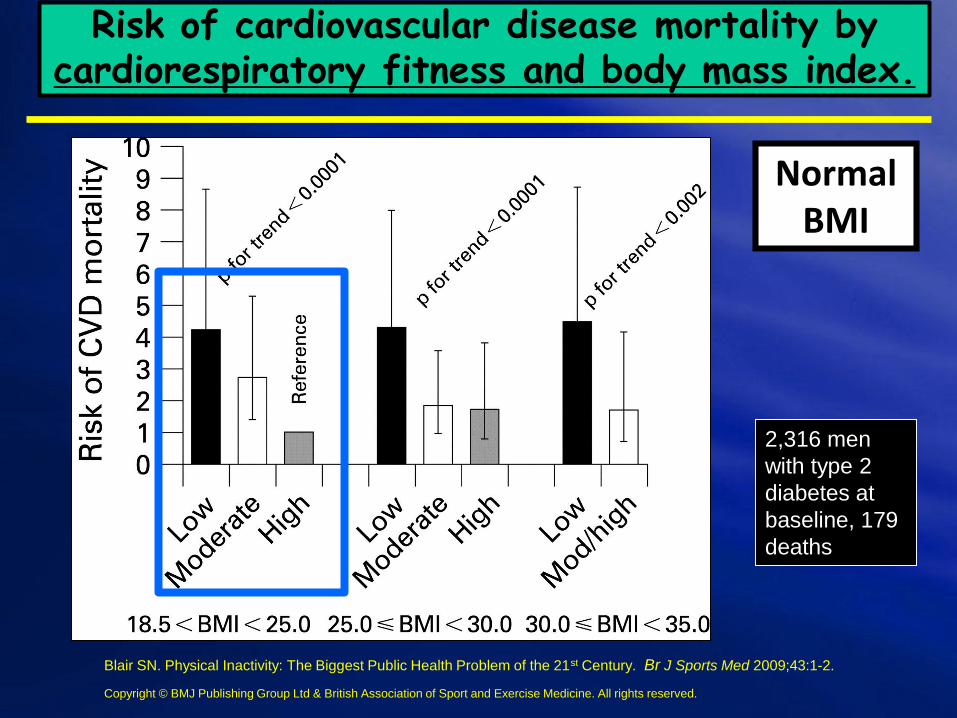
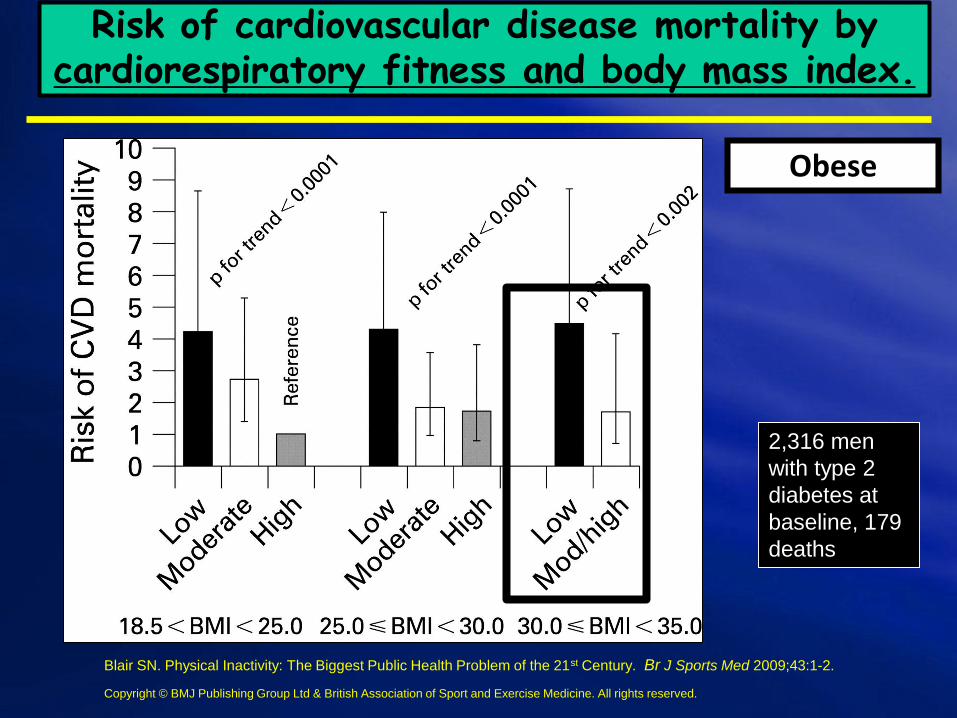
Risk of cardiovascular disease mortality by cardiorespiratory fitness and body mass index.
Blair SN. Physical Inactivity: The Biggest Public Health Problem of the 21st Century. Br J Sports Med 2009;43:1-2.
2,316 men
with type 2
diabetes at
baseline, 179
deaths
Copyright © BMJ Publishing Group Ltd & British Association of Sport and Exercise Medicine. All rights reserved.
Normal BMI
2,316 men
with type 2
diabetes at
baseline, 179
deaths
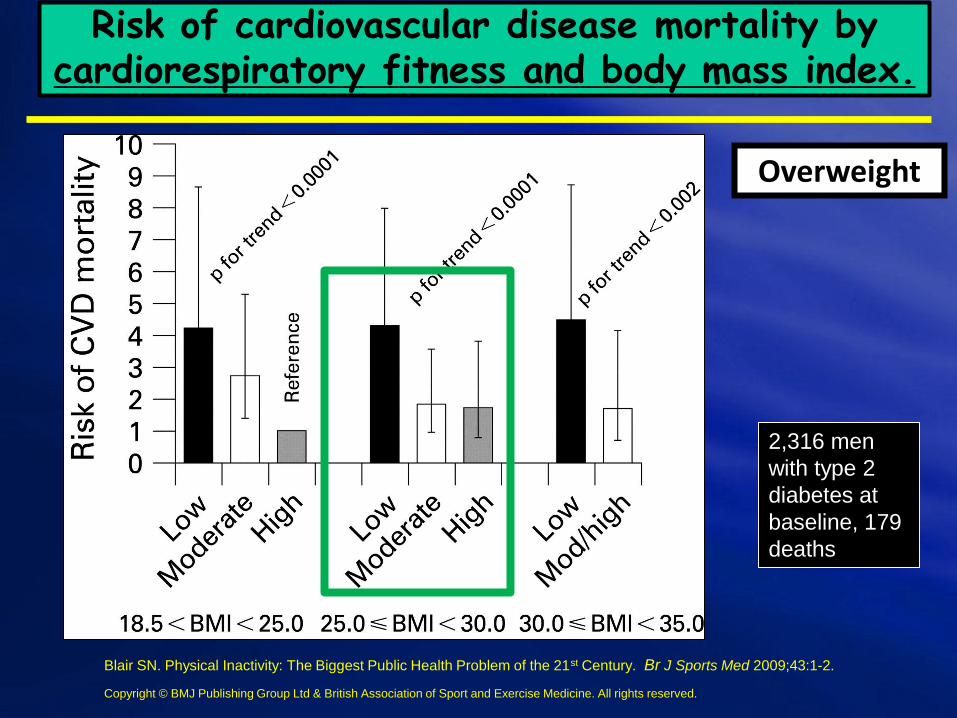
Overweight
Risk of cardiovascular disease mortality by cardiorespiratory fitness and body mass index.
Blair SN. Physical Inactivity: The Biggest Public Health Problem of the 21st Century. Br J Sports Med 2009;43:1-2.
Copyright © BMJ Publishing Group Ltd & British Association of Sport and Exercise Medicine. All rights reserved.
2,316 men
with type 2
diabetes at
baseline, 179
deaths
Obese
Risk of cardiovascular disease mortality by cardiorespiratory fitness and body mass index.
Blair SN. Physical Inactivity: The Biggest Public Health Problem of the 21st Century. Br J Sports Med 2009;43:1-2.
Copyright © BMJ Publishing Group Ltd & British Association of Sport and Exercise Medicine. All rights reserved.
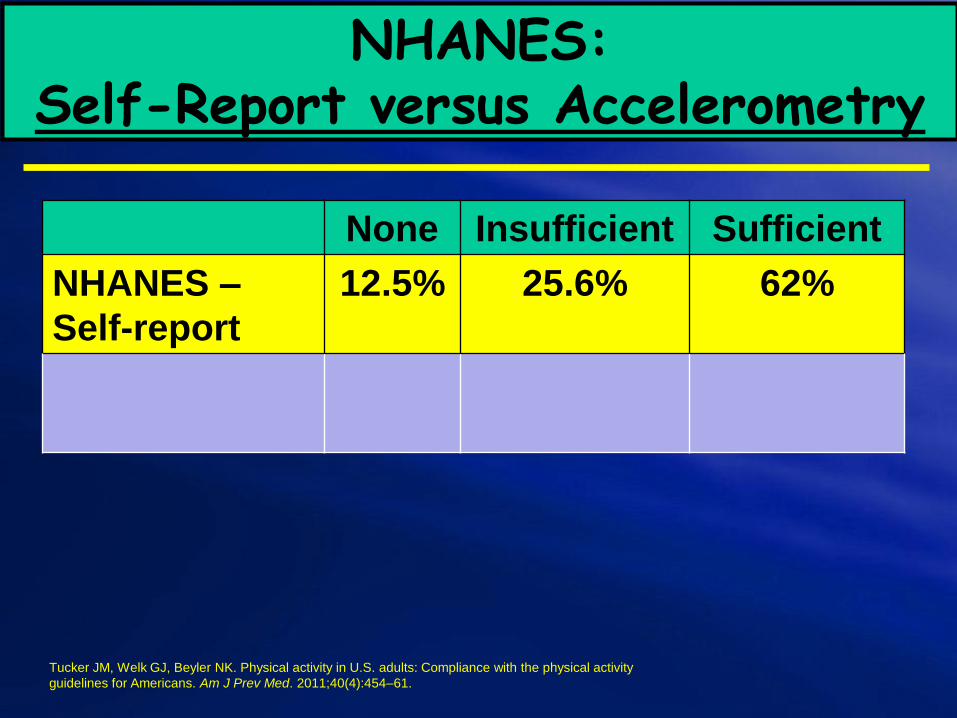
NHANES: Self-Report versus Accelerometry
None Insufficient Sufficient
NHANES –
Self-report
12.5% 25.6% 62%
Tucker JM, Welk GJ, Beyler NK. Physical activity in U.S. adults: Compliance with the physical activity
guidelines for Americans. Am J Prev Med. 2011;40(4):454–61.

NHANES: Self-Report versus Accelerometry
None Insufficient Sufficient
NHANES –
Self-report
12.5% 25.6% 62%
NHANES -
Accelerometry
53.0% 37.3% 9.6%
Tucker JM, Welk GJ, Beyler NK. Physical activity in U.S. adults: Compliance with the physical activity
guidelines for Americans. Am J Prev Med. 2011;40(4):454–61.
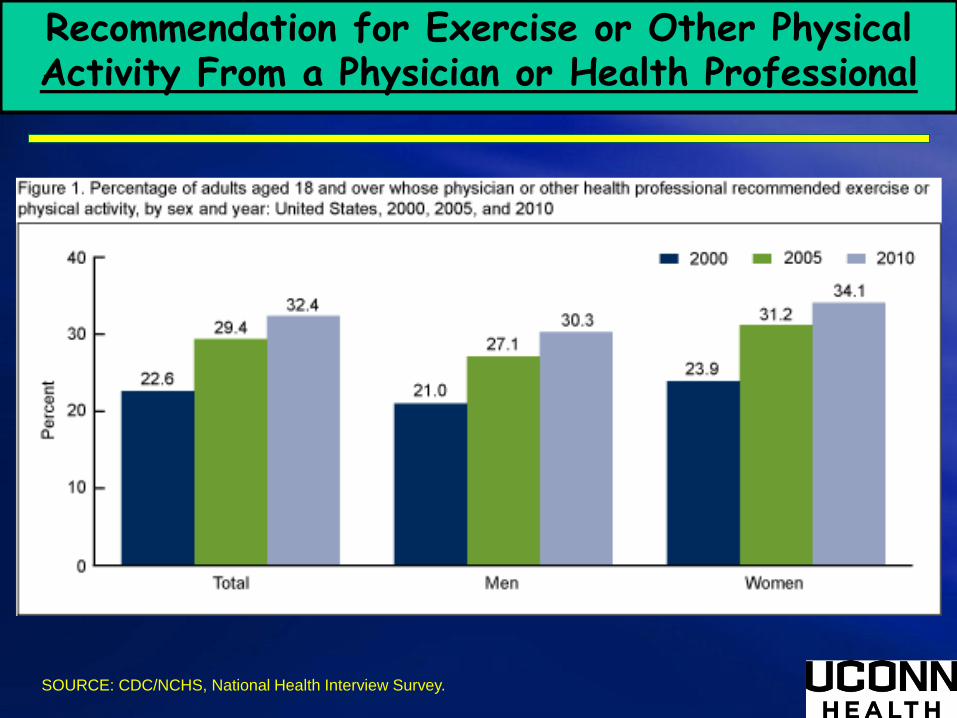
Recommendation for Exercise or Other Physical Activity From a Physician or Health Professional
SOURCE: CDC/NCHS, National Health Interview Survey.
If Exercise Is Medicine, Where Is Exercise in Medicine?
Review of U.S. Medical Education Curricula for Physical Activity-Related Content
Cardinal BJ, et al. If Exercise Is Medicine, Where Is Exercise in Medicine? Review of U.S. Medical Education Curricula for
Physical Activity-Related Content. J Physical Activity and Health. 2015; 12(9):1336-43.
This study provides an update on the amount and type of physical activity education occurring in medical education in the United States in 2013. It is the first study to do so since 2002.
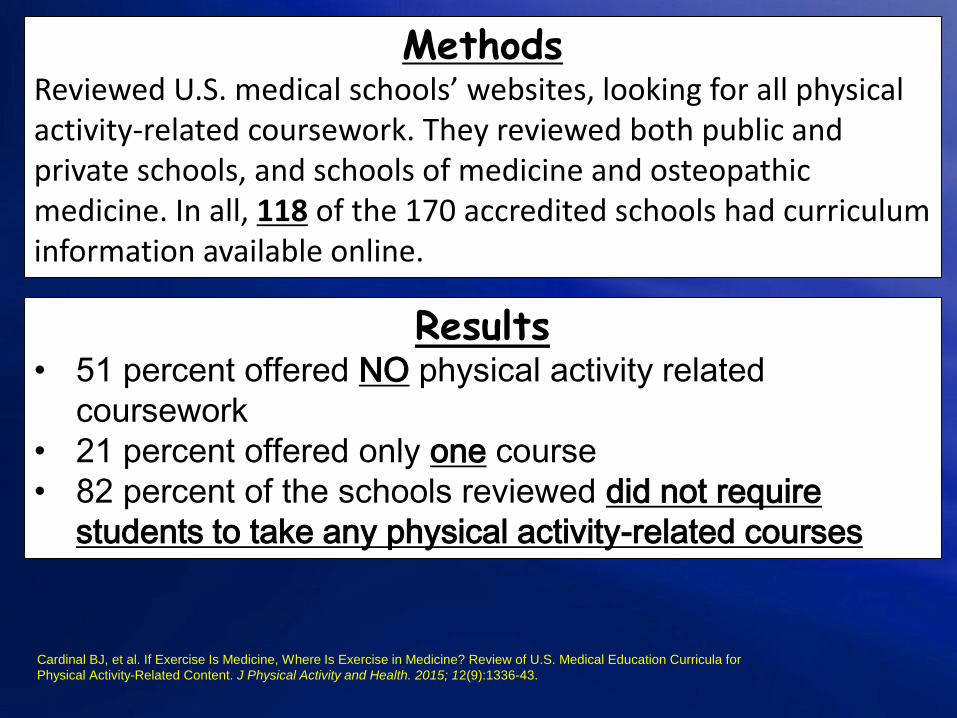
MethodsReviewed U.S. medical schools’ websites, looking for all physical activity-related coursework. They reviewed both public and private schools, and schools of medicine and osteopathic medicine. In all, 118 of the 170 accredited schools had curriculum information available online.
Cardinal BJ, et al. If Exercise Is Medicine, Where Is Exercise in Medicine? Review of U.S. Medical Education Curricula for
Physical Activity-Related Content. J Physical Activity and Health. 2015; 12(9):1336-43.
Results• 51 percent offered NO physical activity related
coursework
• 21 percent offered only one course
• 82 percent of the schools reviewed did not require
students to take any physical activity-related courses
More than one-half of the physicians trained in the United States in 2013 received no formal education in physical activity and may, therefore, be ill-prepared to assist their patients in a manner consistent with Healthy People 2020, the National Physical Activity Plan, or the Exercise is Medicine initiative.
Cardinal BJ, et al. If Exercise Is Medicine, Where Is Exercise in Medicine? Review of U.S. Medical Education Curricula for
Physical Activity-Related Content. J Physical Activity and Health. 2015; 12(9):1336-43.
Conclusion

An In-Depth Look at the 2015-2020
Dietary Guidelines
Information adapted from the 2015-2020 Dietary Guidelines for Americans. Available at
DietaryGuidelines.gov.
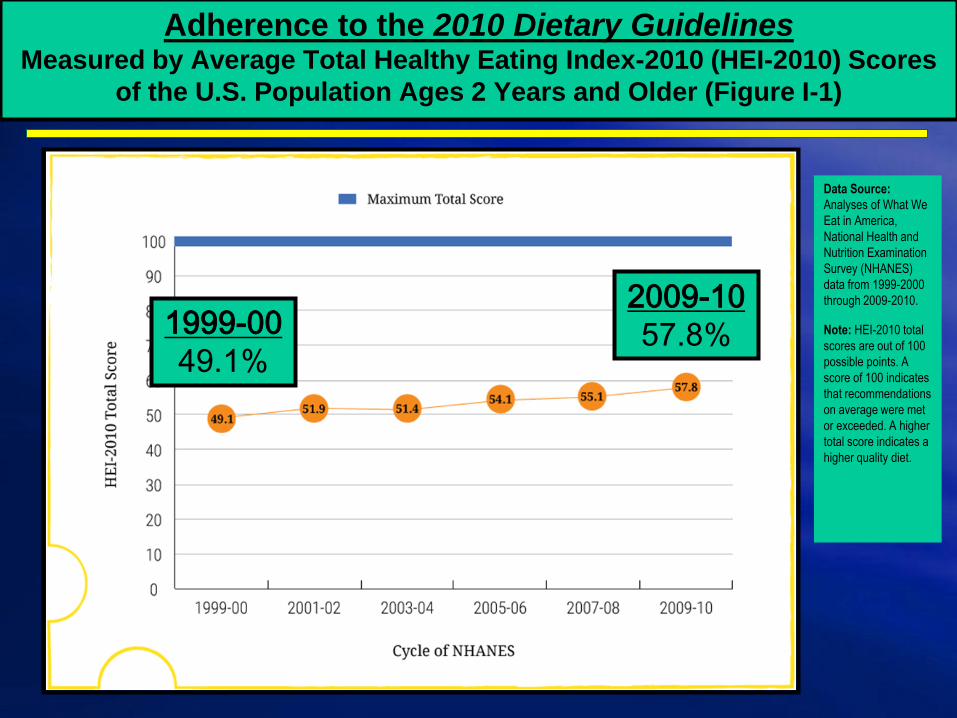
Adherence to the 2010 Dietary GuidelinesMeasured by Average Total Healthy Eating Index-2010 (HEI-2010) Scores
of the U.S. Population Ages 2 Years and Older (Figure I-1)
Data Source:
Analyses of What We
Eat in America,
National Health and
Nutrition Examination
Survey (NHANES)
data from 1999-2000
through 2009-2010.
Note: HEI-2010 total
scores are out of 100
possible points. A
score of 100 indicates
that recommendations
on average were met
or exceeded. A higher
total score indicates a
higher quality diet.
1999-00
49.1%
2009-10
57.8%
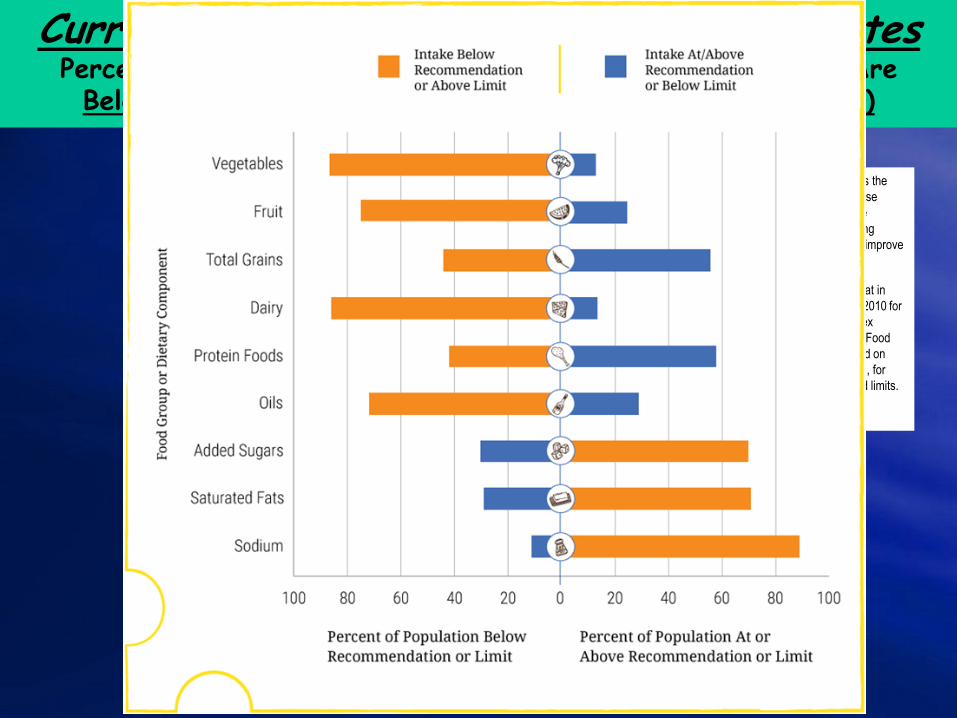
Current Eating Patterns in the United StatesPercent of the U.S. Population Ages 1 Year and Older Who Are Below, At, or Above Each Dietary Goal or Limit (Figure 2-1)
Note: The center (0) line is the
goal or limit. For most, those
represented by the orange
sections of the bars, shifting
toward the center line will improve
their eating pattern.
Data Source: What We Eat in
America, NHANES 2007-2010 for
average intakes by age-sex
group. Healthy U.S.-Style Food
Patterns, which vary based on
age, sex, and activity level, for
recommended intakes and limits.
2015-2020 Dietary Guidelines for Americans:The Guidelines
1. Follow a healthy eating pattern across the lifespan. All food and
beverage choices matter. Choose a healthy eating pattern at an
appropriate calorie level to help achieve and maintain a healthy body
weight, support nutrient adequacy, and reduce the risk of chronic
disease.
2. Focus on variety, nutrient density, and amount. To meet nutrient
needs within calorie limits, choose a variety of nutrient-dense foods
across and within all food groups in recommended amounts.
3. Limit calories from added sugars and saturated fats and reduce
sodium intake. Consume an eating pattern low in added sugars,
saturated fats, and sodium. Cut back on foods and beverages higher in
these components to amounts that fit within healthy eating patterns.
Information adapted from the 2015-2020 Dietary Guidelines for Americans. Available at DietaryGuidelines.gov.
2015-2020 Dietary Guidelines for Americans:The Guidelines (cont.)
4. Shift to healthier food and beverage choices. Choose nutrient-dense foods and beverages across and within all food groups in place of less healthy choices. Consider cultural and personal preferences to make these shifts easier to accomplish and maintain.
5. Support healthy eating patterns for all. Everyone has a role in helping to create and support healthy eating patterns in multiple settings nationwide, from home to school to work to communities.
Key Elements of Healthy Eating Patterns:Key Recommendations
Consume a healthy eating pattern that accounts for all foods and
beverages within an appropriate calorie level.
A healthy eating pattern includes:
• A variety of vegetables from all of the subgroups—dark green, red and orange,
legumes (beans and peas), starchy, and other
• Fruits, especially whole fruits
• Grains, at least half of which are whole grains
• Fat-free or low-fat dairy, including milk, yogurt, cheese, and/or fortified soy
beverages
• A variety of protein foods, including seafood, lean meats and poultry, eggs, legumes
(beans and peas), and nuts, seeds, and soy products
• Oils
A healthy eating pattern limits:
• Saturated fats and trans fats, added sugars, and sodium
Key Elements of Healthy Eating Patterns:Key Recommendations (cont.)
Key Recommendations that are quantitative are provided for several components of the diet that should be limited. These components are of particular public health concern in the United States, and the specified limits can help individuals achieve healthy eating patterns within calorie limits:
Consume less than 10 percent of calories per day from added sugars
Consume less than 10 percent of calories per day from saturated fats
Consume less than 2,300 milligrams (mg) per day of sodium
If alcohol is consumed, it should be consumed in moderation—up to
one drink per day for women and up to two drinks per day for men—
and only by adults of legal drinking age
Meet the Physical Activity Guidelines for Americans
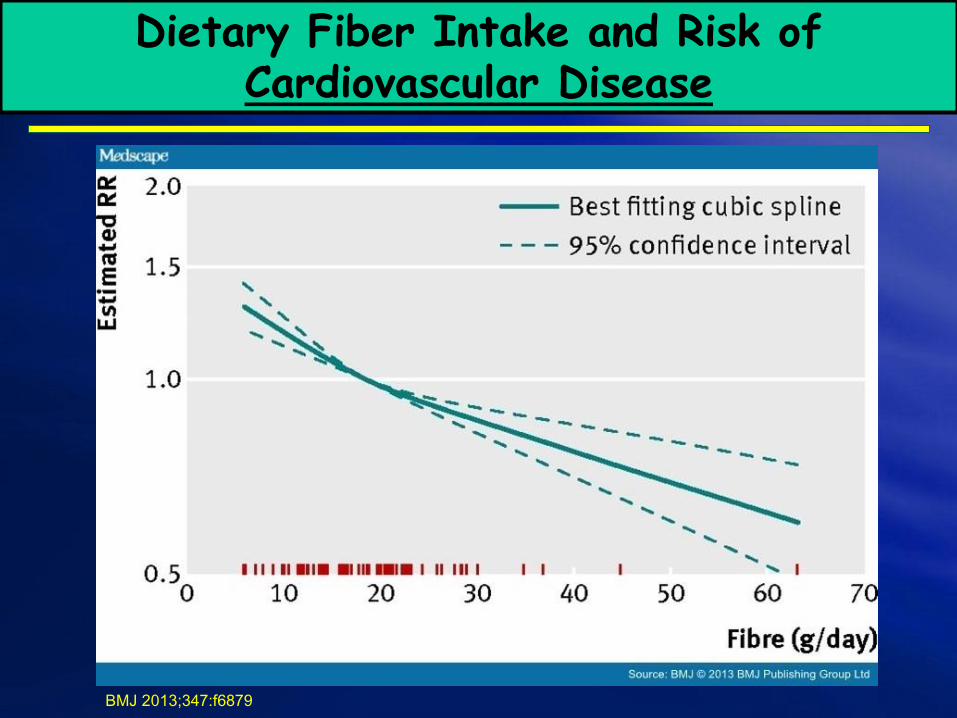
Dietary Fiber Intake and Risk of Cardiovascular Disease
BMJ 2013;347:f6879
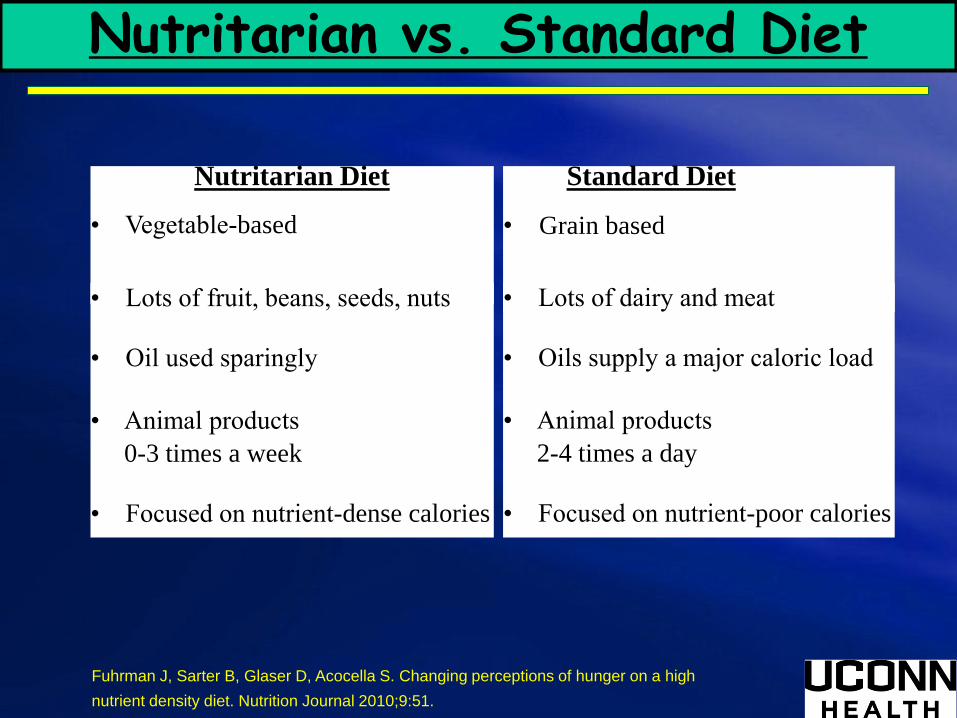
Nutritarian vs. Standard Diet
Nutritarian Diet
• Vegetable-based
• Lots of fruit, beans, seeds, nuts
• Oil used sparingly
• Animal products
0-3 times a week
• Focused on nutrient-dense calories
Standard Diet
• Grain based
• Lots of dairy and meat
• Oils supply a major caloric load
• Animal products
2-4 times a day
• Focused on nutrient-poor calories
Fuhrman J, Sarter B, Glaser D, Acocella S. Changing perceptions of hunger on a high
nutrient density diet. Nutrition Journal 2010;9:51.
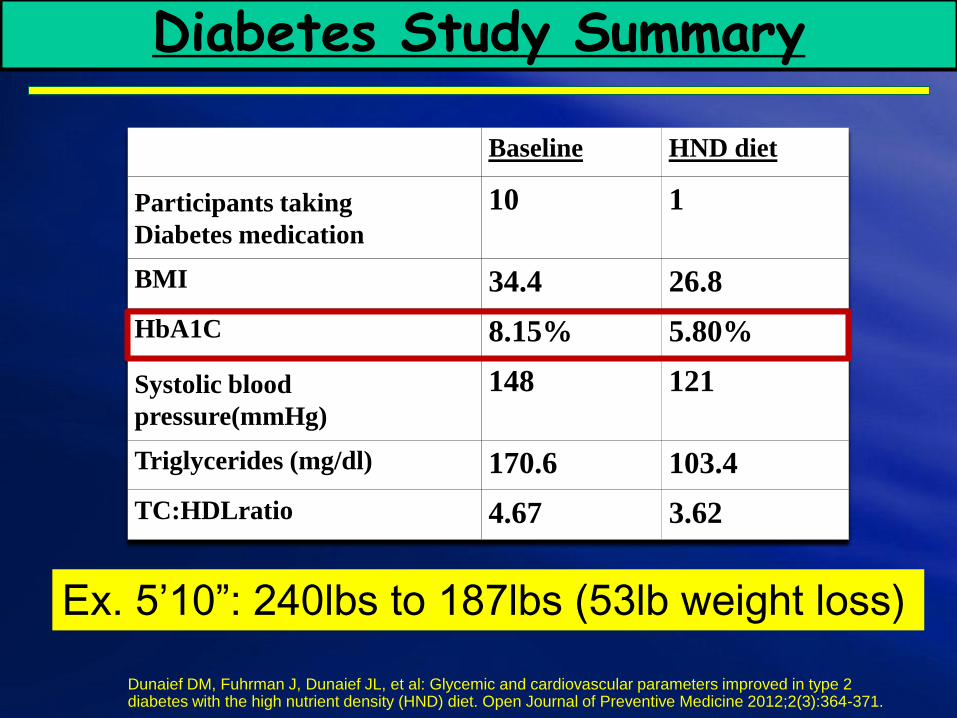
Diabetes Study Summary
Baseline HND diet
Participants taking
Diabetes medication
10 1
BMI 34.4 26.8
HbA1C 8.15% 5.80%
Systolic blood
pressure(mmHg)
148 121
Triglycerides (mg/dl) 170.6 103.4
TC:HDLratio 4.67 3.62
Dunaief DM, Fuhrman J, Dunaief JL, et al: Glycemic and cardiovascular parameters improved in type 2 diabetes with the high nutrient density (HND) diet. Open Journal of Preventive Medicine 2012;2(3):364-371.
Ex. 5’10”: 240lbs to 187lbs (53lb weight loss)
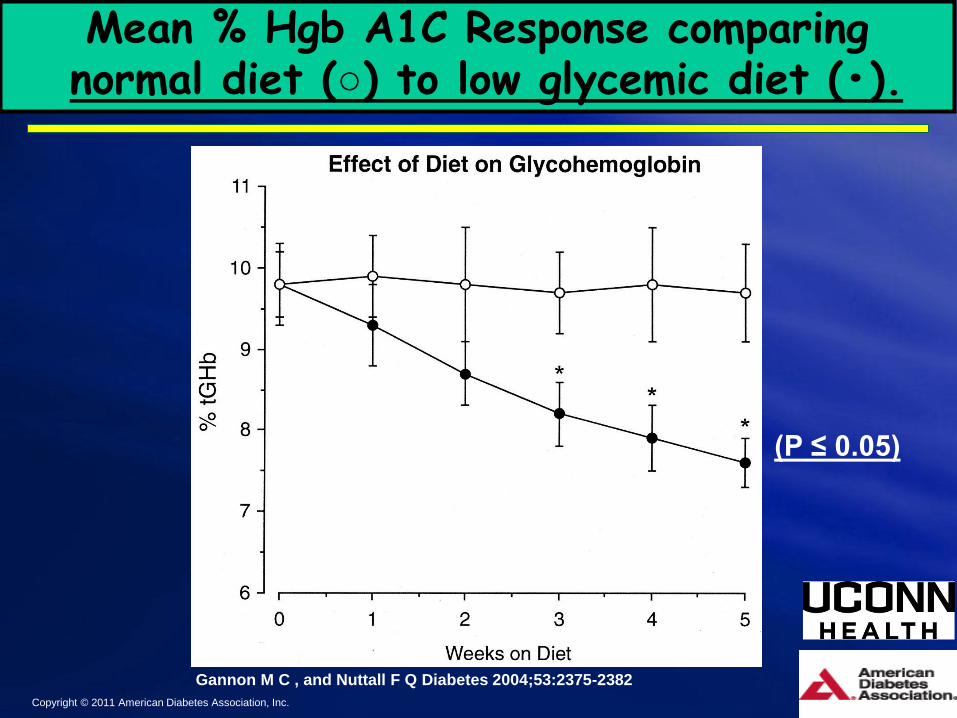
Mean % Hgb A1C Response comparingnormal diet (○) to low glycemic diet (•).
Gannon M C , and Nuttall F Q Diabetes 2004;53:2375-2382
Copyright © 2011 American Diabetes Association, Inc.
(P ≤ 0.05)
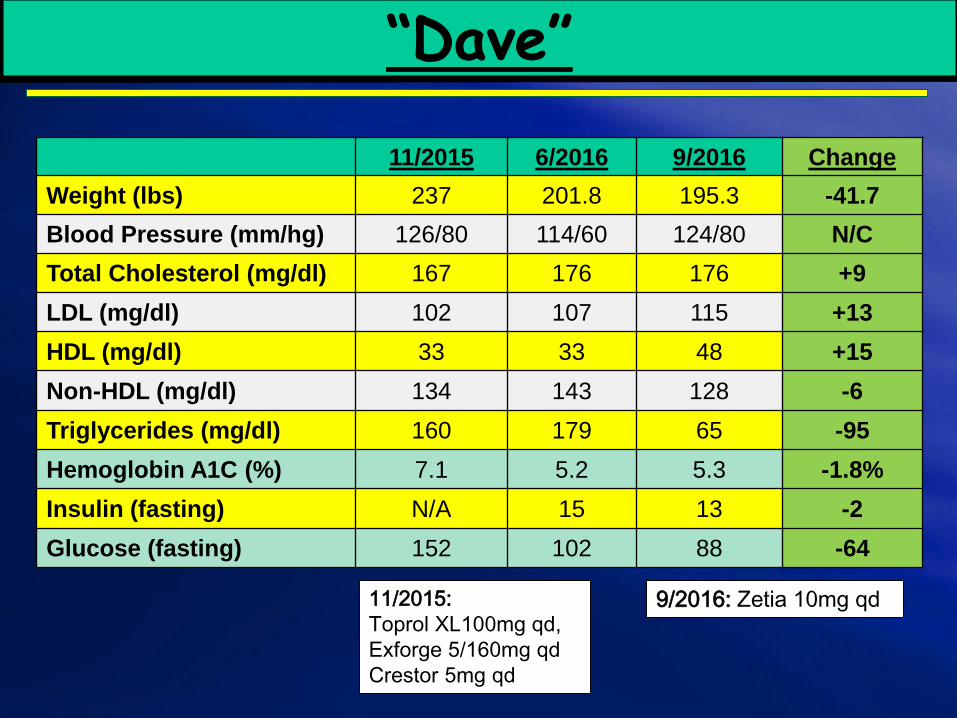
“Dave”
11/2015 6/2016 9/2016 Change
Weight (lbs) 237 201.8 195.3 -41.7
Blood Pressure (mm/hg) 126/80 114/60 124/80 N/C
Total Cholesterol (mg/dl) 167 176 176 +9
LDL (mg/dl) 102 107 115 +13
HDL (mg/dl) 33 33 48 +15
Non-HDL (mg/dl) 134 143 128 -6
Triglycerides (mg/dl) 160 179 65 -95
Hemoglobin A1C (%) 7.1 5.2 5.3 -1.8%
Insulin (fasting) N/A 15 13 -2
Glucose (fasting) 152 102 88 -64
11/2015:
Toprol XL100mg qd,
Exforge 5/160mg qd
Crestor 5mg qd
9/2016: Zetia 10mg qd

Aune, D., et al: Nut Consumption and Risk of Cardiovascular Disease, Total Cancer, All-Cause and Cause-Specific
Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. BMC Medicine 2016;14:207
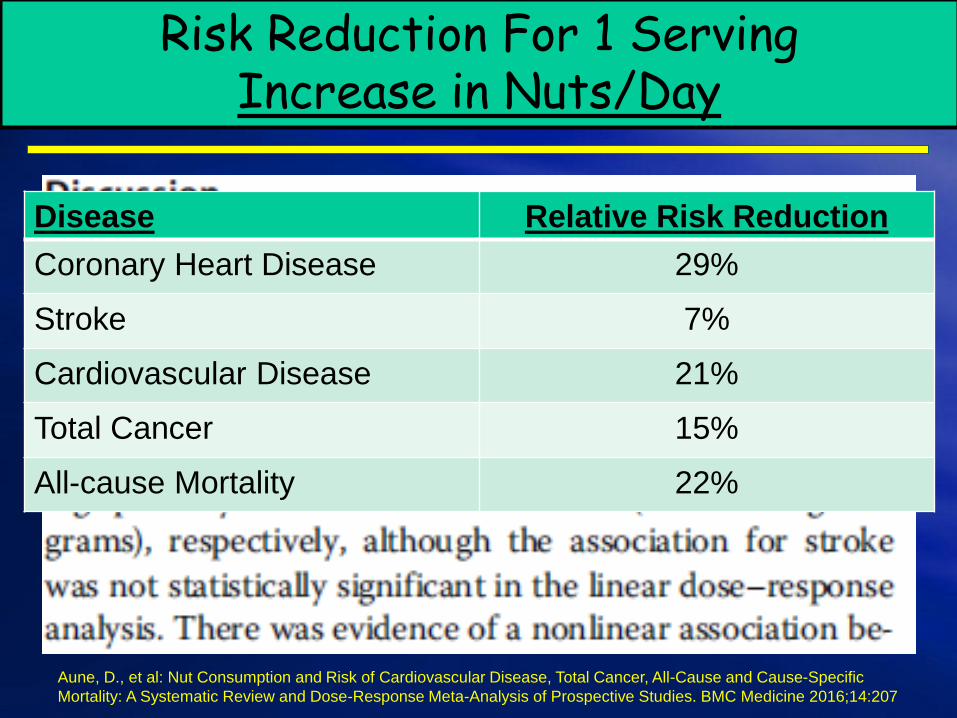
Risk Reduction For 1 Serving Increase in Nuts/Day
Disease Relative Risk Reduction
Coronary Heart Disease 29%
Stroke 7%
Cardiovascular Disease 21%
Total Cancer 15%
All-cause Mortality 22%
Aune, D., et al: Nut Consumption and Risk of Cardiovascular Disease, Total Cancer, All-Cause and Cause-Specific
Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. BMC Medicine 2016;14:207
Stress
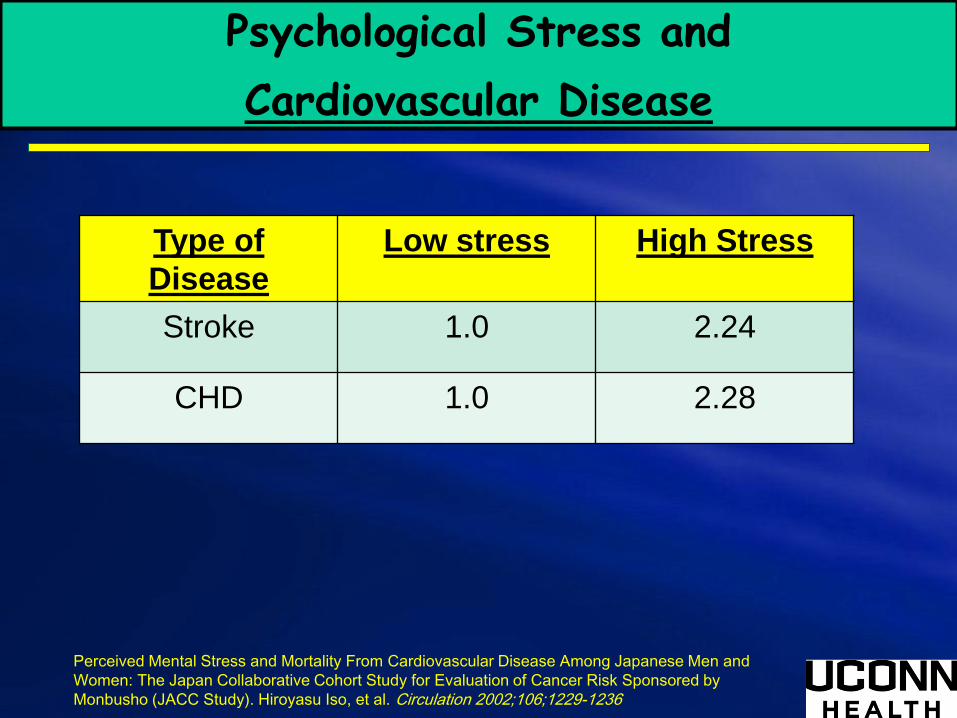
Psychological Stress and
Cardiovascular Disease
Type of
Disease
Low stress High Stress
Stroke 1.0 2.24
CHD 1.0 2.28
Perceived Mental Stress and Mortality From Cardiovascular Disease Among Japanese Men and
Women: The Japan Collaborative Cohort Study for Evaluation of Cancer Risk Sponsored by
Monbusho (JACC Study). Hiroyasu Iso, et al. Circulation 2002;106;1229-1236
Risks of Stress
• Work-related stress can double one's risk of dying from heart disease1.
• Stress is linked to the six leading causes of death -heart disease, cancer, lung ailments, accidents, cirrhosis of the liver, and suicide2.
• People with high levels of anxiety can have between two to seven times the risk of heart disease3.
1(British Medical Journal, 2002); 2("The Stress Solution: An Active Plan to Manage the Stress in Your Life," Lyle H. Miller, Ph.D. and Alma Dell Smith, Ph.D.); 3("Emotional Longevity: What Really Determines How Long You Live," Norman B. Anderson and Elizabeth P. Anderson, 2003)
The Keys to Successful Lifestyle Medicine
History, History, History – Questionnaire
– Cardiovascular history and risk factors
• CAD, PAD, or stroke (when and previous
imaging studies)
• Hypertension
– Blood pressure monitor at home
– Routine monitoring and how they check it
• Diabetes
– Insulin dependent versus oral medication
– Nutrition consultation or how they have
monitored their diet
– History of gestational diabetes
Cardiovascular history and risk factors (cont.)
• Hyperlipidemia
– Prescription medication
– OTC supplements (ie., omega-3, fiber, or phytosterols)
• Family history
– CVD history and risk factors
– Premature CAD
• Sleep apnea
– Snoring and quality of sleep
– Previous sleep study
– Using CPAP and it is helping
History, History, History – Questionnaire
– Cardiovascular history and risk factors (cont.)
• Smoking history
– Current or previous
– Smoking cessation methods used
– Triggers for smoking
• Social history
– alcohol, illegal drugs, and living situation
• Diet
– 7 day food log
History, History, History – Questionnaire
– Cardiovascular history and risk factors (cont.)
• Exercise/activity history
– Limitations (physical, financial, geographic, and time)
– What have they done before and what they like to do
• Overweight
– lowest and heaviest adult weight
– Weight loss program previously used
• Stress
– Current and previous stressors
– Stress relief modalities (ie., therapy, journaling,
medication, and exercise)
History, History, History – Questionnaire
Goals
• Blood pressure = less than 130/85
• Diabetes
– insulin dependent (Hgb A1C < 7.0)
– Oral medication (Hgb A1C < 6.5)
– No medication (Hgb A1C < 6.0)
• Cholesterol
– Set goal for HDL, LDL, triglycerides, and non-HDL

Diabetes
• Benefits of diet and exercise
– Increased insulin sensitivity with exercise
– Stabilizing blood sugar with diet (ie., low glycemic)
– Effects of stress on blood sugars
Hypertension
• Benefits of diet, exercise, and stress
management
– DASH/Mediterranean diet
– Effect of aerobic exercise on blood pressure
– Stress management
Cholesterol Levels
• Medications and/or over the counter
– Benefits of:
• Fiber
• Phytosterols/stanols
• Omega-3 supplements (high DHA/EPA)
• Exercise
• Low animal fat diet
• Medications
Smoking Cessation
• Start by not focusing on it
• Remember: 7 failures before success
• Start with exercises increases success 3
times
• Have them identify causes of smoking
• Give them resources to be successful
– Medications and 1-800-QUIT NOW
– Smoking programs available
– Diahann Wilcox, APRN program
– Dr. White’s smoking and hypertension study
Diet
• Review recent foods and look at label of the foods
• Substitutions within their diet
• Encourage high fiber/protein (ie., low glycemic
foods
– Explain how this helps decrease fat/sugar absorption
• 7 day food log
• Predominantly non-processed plant based foods!
• Treat = 100 calories/day
• Mayo Clinic Diet Book/Journal
• Dietary consult
Exercise/Activity
• Exercise prescription: What do you want it to do?
– Set them up for success!
– Dismiss the “No pain, no gain” theory
– Intensity: “Talk test”
• Don’t focus on heart rate
– Duration
• Gradually increase to goal of 30-45 minutes
– Days per week: 3-5 days or less
– Pedometer if not enough time
• Add 500 steps/day from baseline every 2 weeks until
~3,000 steps/day above baseline
Weight Loss
• Find what motivates them to lose weight
• It comes down to I’s and O’s (intake/output)
• Triggers to eating
• Change mind set to:
“Eating to live, instead of, living to eat” and
“Getting food to work for them”.
• Don’t focus on it
– Focus on the process of being healthy
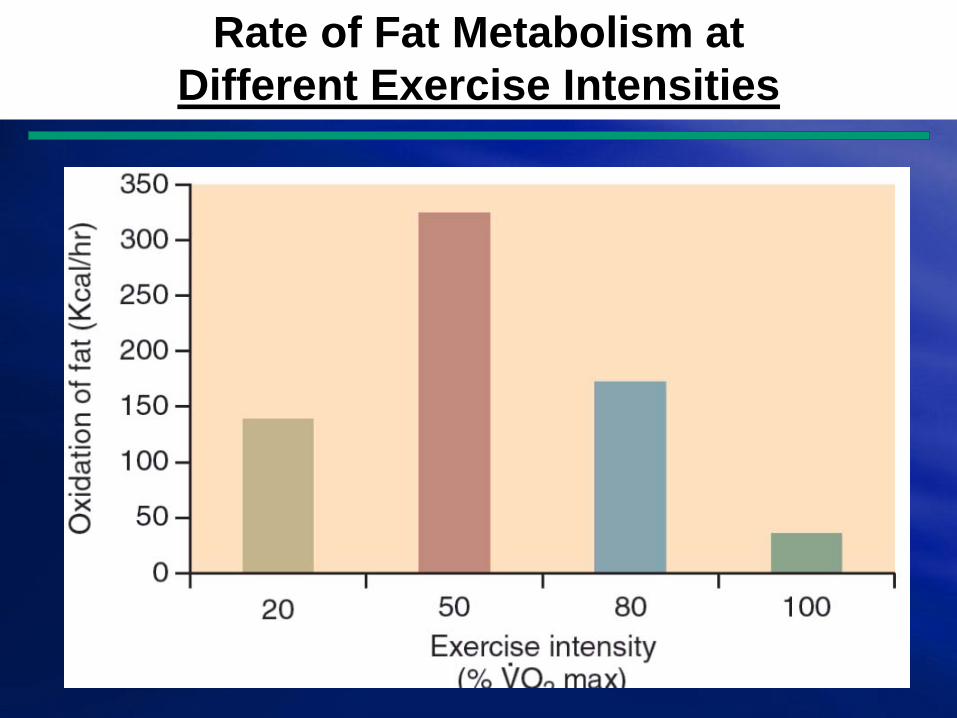
Rate of Fat Metabolism at
Different Exercise Intensities
Stress
• Remember that you are always in control!
• Mental relaxation at least twice daily.
• Eat healthy and exercise.
• Positive self-talk.
• Find pleasure.
• Serenity Prayer.
The Serenity Prayer
“God grant me the serenity to accept the things I cannot change, the courage to change the things that I can, and the wisdom to know the difference.”
Take Home Message
• You’re a consultant for your patient.
• Give them goals (“To Do List”) each visit and start
low and go slow.
• Reassess/Replan on a regular basis (ie., what
worked and what didn’t work).
• Keep it positive.
• The more focus you put on lifestyle change and
giving them the tools, the more successful they
will be.

Identify the cost-effectiveness of implementing lifestyle medicine
within primary care.
1. Individual visits
2. Group visits
Individual Visits
CPT Code Complexity Total Time Counseling
Time
99211
99212
99213
99214
99215
Physician vs. Advanced Practice Practitioner




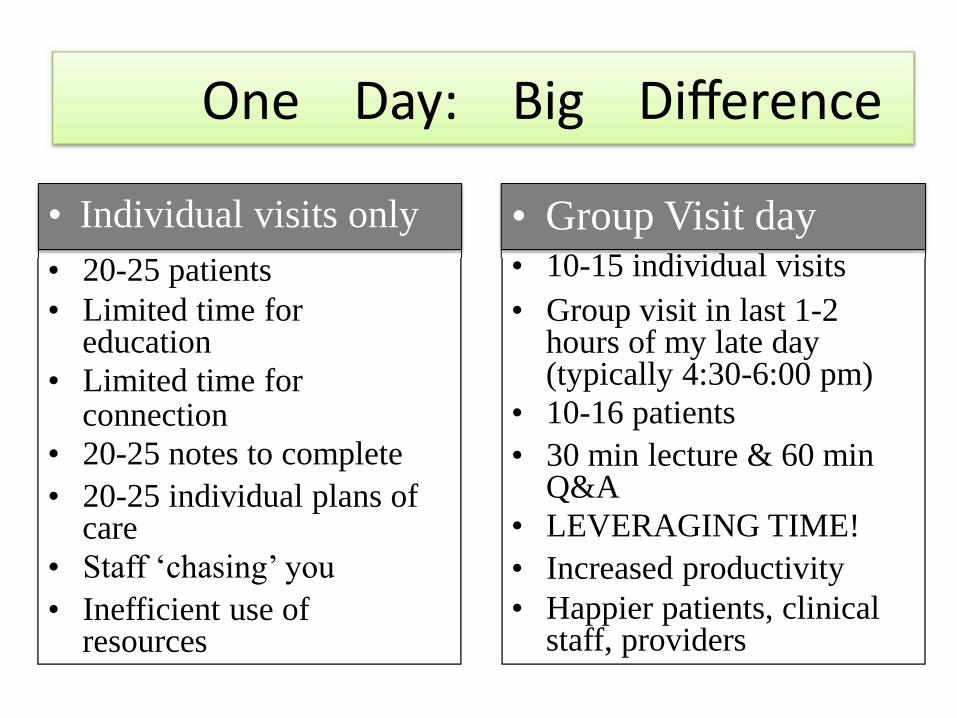
One Day: Big Difference
• Individual visits only
• 20-25 patients
• Limited time foreducation
• Limited time forconnection
• 20-25 notes to complete
• 20-25 individual plans ofcare
• Staff ‘chasing’ you
• Inefficient use ofresources
• Group Visit day• 10-15 individual visits
• Group visit in last 1-2hours of my late day(typically 4:30-6:00 pm)
• 10-16 patients
• 30 min lecture & 60 minQ&A
• LEVERAGING TIME!
• Increased productivity
• Happier patients, clinicalstaff, providers

LEVERAGING TIME
• see 16 pa9ents
• in 90 minutes
• billed 99213 each
_______________________
Health
Efficiency
Produc9vity
The Math is EASY!
• A win-‐win opportunity – Patients pay less
• INSURANCE: 1 visit charge for 3 visits’ value
• CASH: Patient pays less (e.g. $75 for 90 minutes)
– Provider earns more • (e.g. $75 x 16 pts= $1200, or works out to ~$800/
hour)
• been shown to increase productivity 200-‐600%
• Must create supporting systems to leverage time
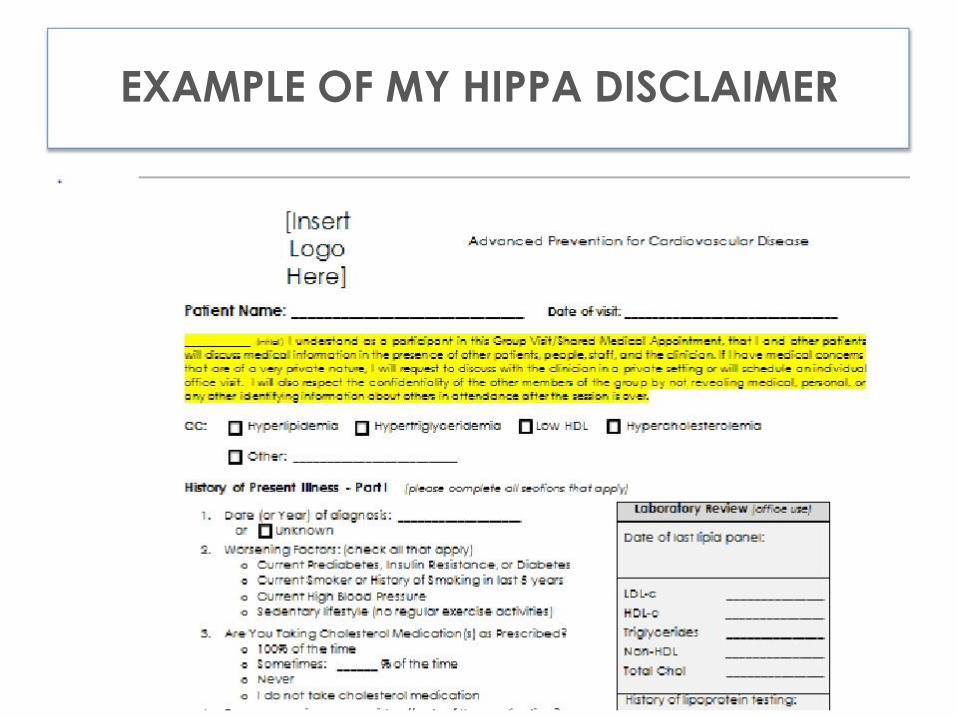
EXAMPLE OF MY HIPPA DISCLAIMER
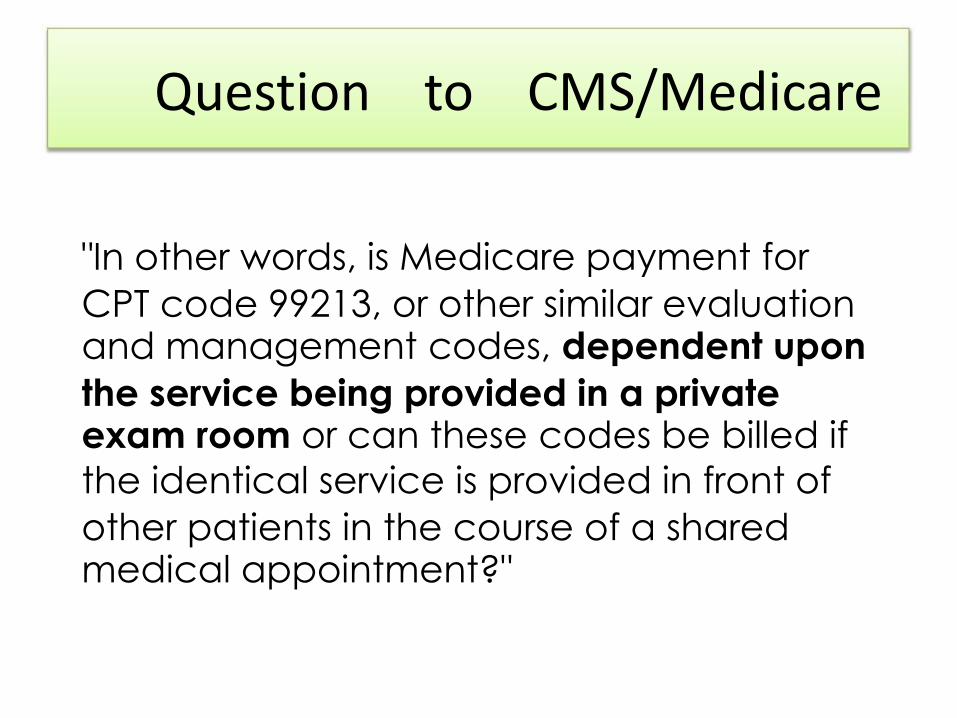
Question to CMS/Medicare
"In other words, is Medicare payment for
CPT code 99213, or other similar evaluationand management codes, dependent upon
the service being provided in a privateexam room or can these codes be billed if
the identical service is provided in front of
other patients in the course of a sharedmedical appointment?"
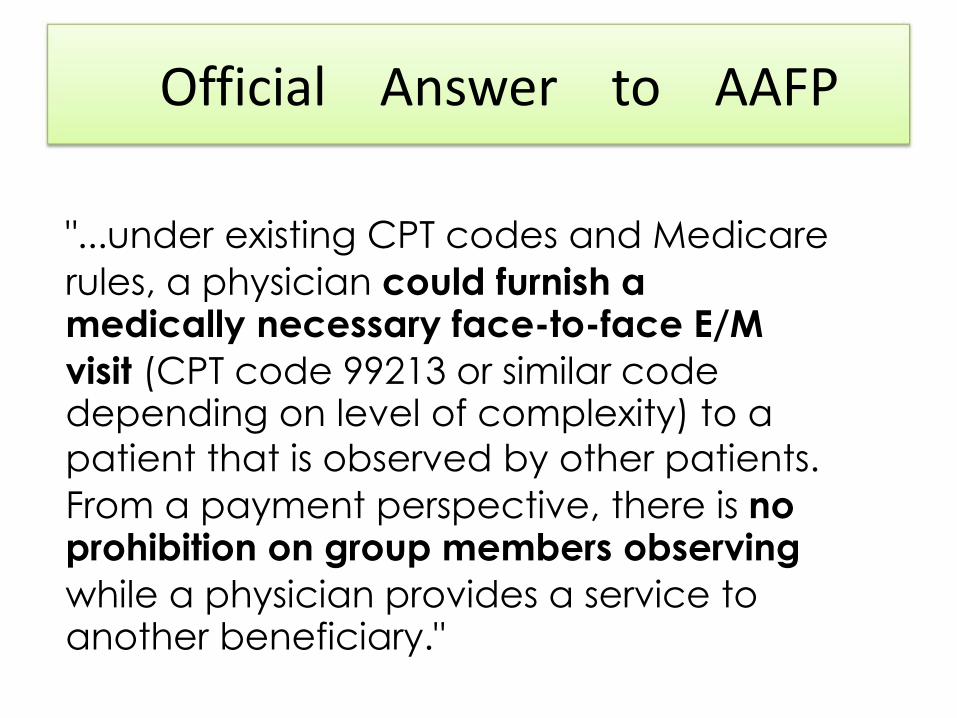
Official Answer to AAFP
"...under existing CPT codes and Medicare
rules, a physician could furnish amedically necessary face-to-face E/M
visit (CPT code 99213 or similar codedepending on level of complexity) to a
patient that is observed by other patients.
From a payment perspective, there is noprohibition on group members observing
while a physician provides a service toanother beneficiary."
Getting Paid: Insurance
• Just like individual billing – Based on face-‐to-‐face time
– Group time is NOT billable
– Level of documentation complexity
– Regardless if done semi-‐privately, privately, or publicly
Billing & Coding Takeaways
• Medical necessity is first• Proper documentation (as usual)
• Bill typical E/M codes based oncomplexity of your visit note (as usual)
• Avoid ‘unique’ group or specialty codes

Group Visits
CPT Code Complexity Total Time Counseling
Time
99211
99212
99213
99214
99215
Physician vs. Advanced Practice Practitioner

Opportunities

Lifestyle can
be Medicine.







