Download - Massive Hemoptysis

Massive Hemoptysis
Massive Hemoptysis
Defined as expectoration of blood exceeding 100 to 600 mL over a 24-hour period.
Only 5% of hemoptysis is massive but mortality is 80%.
Massive Hemoptysis
Must r/o non-pulmonary causes– upper airway or gastrointestinal tract
Alkaline pH, foaminess, or the presence of pus may sometimes suggest the lungs as the primary source of bleeding

Initial approach to the patient is dictated by the clinical presentation. How sick is the patient? Patients with rapid bleeding or decompensation need
ACLS first and control of their bleeding. Secondary goals are determining the site and
cause of the bleeding and whether or not the patient is a surgical candidate.
History
Prior lung, cardiac, or renal disease? History of cigarette smoking? Prior hemoptysis, other pulmonary
symptoms, or infectious symptoms? Family history of hemoptysis or brain
aneurysms (suggesting hereditary hemorrhagic telangiectasia)?

History
Exposure to asbestos, trimellitic anhydride or other organic chemicals?
Patient's travel history? History of bleeding disorders or use of ASA,
NSAIDS, or anticoagulants? History of upper airway or upper
gastrointestinal complaints or diseases?
Physical Exam
Telangiectasias -- hereditary hemorrhagic telangiectasia.
Skin rash -- vasculitis, systemic lupus erythematosus, fat embolism, or infective endocarditis.
Splinter hemorrhages -- endocarditis or vasculitis. Clubbing is nonspecific, since it can occur in
many chronic lung diseases.

Physical Exam
Audible chest bruit or murmur that increases with inspiration -- large pulmonary AV malformations .
Cardiac murmurs -- congenital heart disease, endocarditis with septic emboli, or mitral stenosis.
Legs should be examined carefully for possible deep venous thrombi.



Causes of hemoptysis
90 % of cases are due to: TB Bronchiectasis Lung abscesses
Tuberculosis
Active cavitary or noncavitary lung disease can cause small or large amounts of bleeding.
Most of these patients have sputum smears that stain positively for acid-fast bacilli.

Tuberculosis
Sudden rupture of a Rasmussen's aneurysm
Inactive TB can cause bleeding due to residual bronchiectasis, erosion of a broncholith through a vessel and into an airway, or by a cavity that subsequently acquires a mycetoma.
The source of bleeding in each of these causes is usually the bronchial arterial circulation (except Rasmussen’s).

Bronchiectasis
Chronic airway inflammation that causes hypertrophy and tortuosity of the bronchial arteries
Accompanies the regional bronchial trees with expansion of the submucosal and peribronchial plexus of vessels.
This circulation is under systemic blood pressure, so that rupture of either the tortuous vessels or the capillary plexus causes rapid bleeding.

Bronchiectasis
Results from prior infection (bacterial or viral), cystic fibrosis, TB, or impairment of the mucociliary clearance apparatus (PCD, Kartagener’s)

Infections
Bleeding may occur acutely from necrosis of lung tissue or from rupture of hypertrophied bronchial arteries in the setting of chronic inflammation.
Hemoptysis occurs in 50 to 90 percent of patients with aspergilloma
Parasitic infections are a very common cause of hemoptysis Paragonimiasis in Southeast Asia. Severe leptospirosis may be complicated by massive
alveolar bleeding and hemoptysis

Lung Cancer
Bronchogenic carcinoma usually causes nonmassive hemoptysis.
Hemoptysis occurs at presentation in 7 to 10% of patients.
Hemoptysis occurs during the disease course in approximately 20%.

Immunologic Lung Disease
Goodpasture's syndrome Wegener's granulomatosis Systemic lupus erythematosus (SLE) Idiopathic pulmonary hemosiderosis. Pathologically, many of these diseases have
components of pulmonary capillaritis

Management and its Difficulties
Multitude of potential etiologies. Course of bleeding is unpredictable. It is frightening to see patients dying from
asphyxiation, even in spite of intubation. There is no consensus regarding the optimal
management of these patients.
Management
Adequate airway protection, ventilation, and cardiovascular function
Intubate if pt. has poor gas exchange, rapid ongoing hemoptysis, hemodynamic instability, or severe shortness of breath
Reverse coagulation disorders CT Surgery Consult +/- VIR
Management
A major priority in the acute management in protection of the nonbleeding lung.
Spillage of blood into the non-bleeding lung can either block the airway with clot or fill the alveoli and prevent gas exchange.
Need to know site of bleeding!!!
Protection of nonbleeding lung
Place bleeding lung in the dependant position Selectiely intubate the nonbleeding lung- easiest if
you want to intubate right mainstem brochus during a left lung bleed.
Risk = blocking RUL bronchus
Balloon tamponade via bronchoscopy Placement of a double lumen ETT specially designed
for selective intubation of the right or left mainstem bronchi
Used as a last option in an asphyxiating pt.

Management with Bronchoscopy
There are no controlled trials in bronchoscopic techniques used to slow or stop bleeding
Lavage with iced saline and application of topical epinephrine (1:20,000), vasopressin, thrombin, or a fibrinogen-thrombin combination.

Management with Arterial Embolization
Used as a semi-definitive treatment option or a bridge to elective surgery.
85% of the time the bleeding stops after embolization
10-20% of patietns rebleed in the following 6-12 months.

Management with Surgery
Patients with lateralized, uncontrollable bleeding should be assessed early.
Usual assessment includes pulmonary function tests, but often these patients are too ill for physiologic testing
Relative contraindications to surgery are: severe underlying pulmonary disease, active TB, cystic fibrosis, multiple AVMs, multifocal bronchiectasis, and diffuse alveolar hemorrhage.

Morbidity
Comparison of medical and surgical treatment for massive hemoptysis favors surgery as having a much lower mortality.
Highest risk patients were not considered to be surgical candidates and were managed medically.
Reports from the 1980s suggest that the mortality rates are approximately comparable in patients who qualified as surgical candidates.
However, medically treated patients probably have a higher risk of rebleeding within the first six months.
Stabilization:
Ensure adequate ventilation and perfusion Avoid asphyxiation Lateral decubitus position Administer oxygen Patients with poor gas exchange, rapid ongoing
hemoptysis, hemodynamic instability, or severe shortness of breath should be orally intubated with a large bore endotracheal tube
Monitor BP, pulse rate, respiratory rate and urine output
MASSIVE HEMOPTYSIS
pgmedicalworld.com
Large IV access + Fluid resuscitation Blood transfusions Cough-suppressing drugs can be added, but
they may favor the hazard of blood retention in to lungs.
Coagulation disorders should be rapidly reversed
pgmedicalworld.com

Protection of non-bleeding lung: Place bleeding lung in dependant position- lateral
decubitus ( if origin of bleed is known and limited to 1 lung) Prevent contamination of good lung
Selectively intubate the nonbleeding lung with bronchoscopic guidance ( isolate rt. and lt. mainstem bronchi)
Placement of a double lumen ETT specially designed for selective intubation of the right or left mainstem bronchi
Emergency bronchoscopy – cold saline lavagepgmedicalworld.com

Endobronchial tamponade: Balloon catheter is introduced via
bronchoscopy and inflated to occlude the bronchus(prevents aspiration of blood into unaffected areas and also stops the bleeding)
The balloon is left inflated for 24 to 48 hours, and the patient is then observed for rebleeding with the balloon deflated for several hours
pgmedicalworld.com
Bronchial arterial embolization:
Angiography should be performed initially Vessel proximal to bleeding site is cannulated and
material like gelfoam – injected to occlude the vessel Used as a semi-definitive treatment option or a
bridge to elective surgery. 85% of the time the bleeding stops after
embolization 10-20% of patients rebleed in the following 6-12
months Complication: embolization of the spinal artery
pgmedicalworld.com

Other methods to control bleeding:
Phototherapy Electrocautery Argon plasma coagulation Nd-YAG laser
pgmedicalworld.com

SURGICAL MANAGEMENT
Done in pts. with uncontrolled life-threatening hemoptysis or localized disease subject to recurrent bleeding
Resection of bleeding lobe or lung maybe done
Relative contraindications to surgery are: severe underlying pulmonary disease, active TB, cystic fibrosis, multiple AVMs, multifocal bronchiectasis, and diffuse alveolar hemorrhage.
pgmedicalworld.com
pgmedicalworld.com
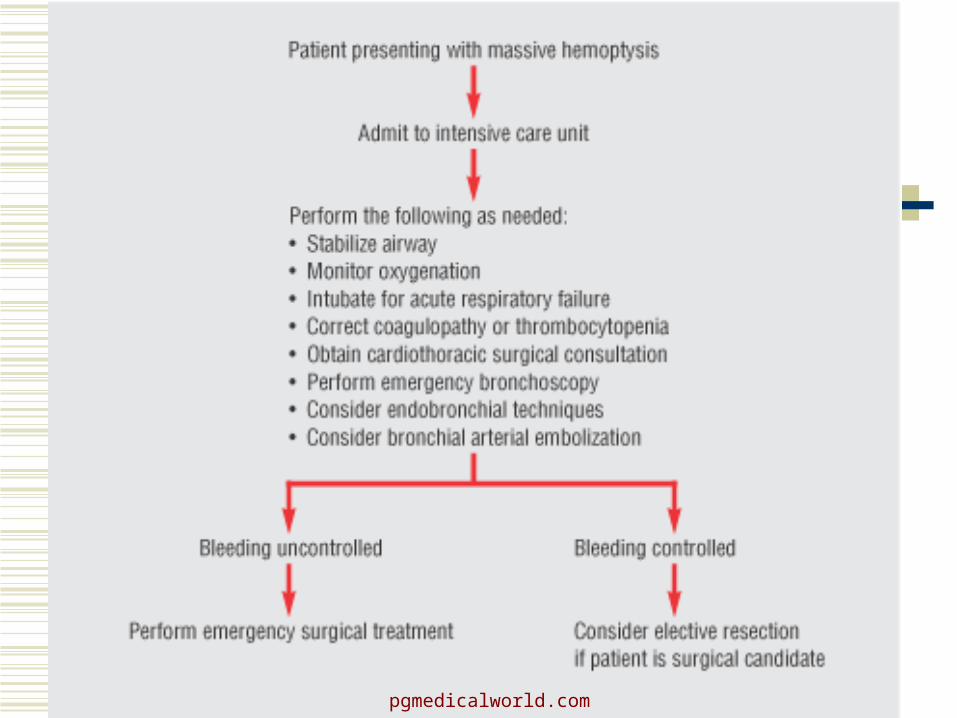
RECOMMENDATIONS
First, stabilize the patient and then perform early bronchoscopy along with other appropriate diagnostic studies
If the patient continues to bleed aggressively, arteriography is most reasonable for localization and therapy
If bleeding persists despite embolization or if the patient is too ill to go to angiography, then blockade therapy or a double lumen tube should be considered
While surgery remains the only truly definitive therapy, it should not be used in the acute emergent setting unless it cannot be avoided

pgmedicalworld.com







