Mast Cell Disorders Andrew M. Smith, MD, MS
Division of Immunology, Allergy, and Rheumatology University of Cincinnati and Cincinnati VA Medical Centers
August 10 and 11, 2012
Disclosures
• None
• The contents do not represent the view of the Department of Veterans Affairs or U.S. Government

Objectives
• Identify the clinical features of mast cell disorders
• Explain the immunologic mechanisms of mast cell disorders
• Describe appropriate evaluation and treatment of mast cell disorders
Case Presentation
• 35 year old male, previously healthy • Symptoms began in the winter of 2011 • Woke up in the middle of the night
– Started with hands and feet itching – Abdominal pain, diarrhea, and vomiting – Lip swelling, quickly progresses to tongue swelling
• Presented to the Emergency Department – Received epinephrine and steroids
Case Presentation
• Fall 2011 - most severe episode • Awaked in the early morning • Hives head to toe, tongue and lip swelling
• Treated with loratidine, famotidine, and
prednisone daily
Case Presentation
• Further episodes: 11 times in 12 months and 4 episodes in the past 14 days – Facial/lip swelling with every episode – Faster progression to respiratory distress and
low blood pressure – Most recent episodes with chest pain – Most episodes have started in the middle of
the night

Case Presentation
• Allergy/Immunology consulted • “What is causing the recurrent episodes of
anaphylaxis?”
• Definitions of anaphylaxis, angioedema, and urticaria

Anaphylaxis - Definition
• Difficulty in defining anaphylaxis • Traditional Definition
– A systemic, immediate hypersensitivity reaction caused by immunoglobulin E (IgE)-mediated immunologic release of mediators from mast cells and basophils

Anaphylaxis World Allergy Organization definition: • A severe, life threatening, generalized or systemic hypersensitivity reaction involving two or more organ systems
• Allergic anaphylaxis – reaction mediated by an immunologic mechanism
• Non-allergic anaphylaxis – non-immunologic reaction
WAO Journal 2011; 4:13–37
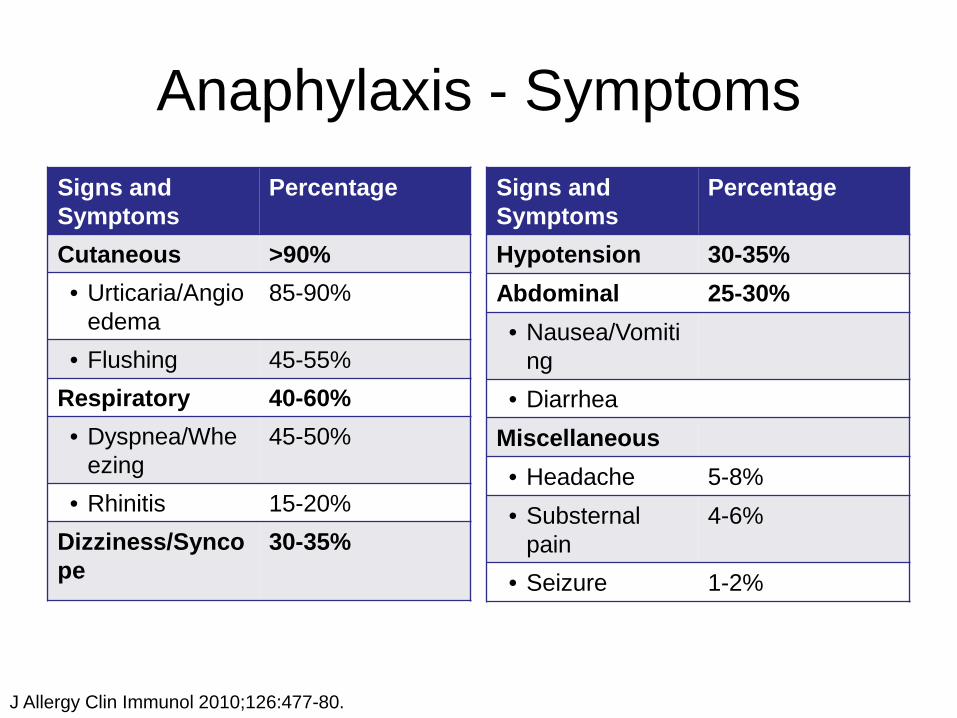
Anaphylaxis - Symptoms Signs and Symptoms
Percentage
Cutaneous >90% • Urticaria/Angio
edema 85-90%
• Flushing 45-55% Respiratory 40-60% • Dyspnea/Whe
ezing 45-50%
• Rhinitis 15-20% Dizziness/Syncope
30-35%
Signs and Symptoms
Percentage
Hypotension 30-35% Abdominal 25-30% • Nausea/Vomiti
ng • Diarrhea
Miscellaneous • Headache 5-8% • Substernal
pain 4-6%
• Seizure 1-2%
J Allergy Clin Immunol 2010;126:477-80.
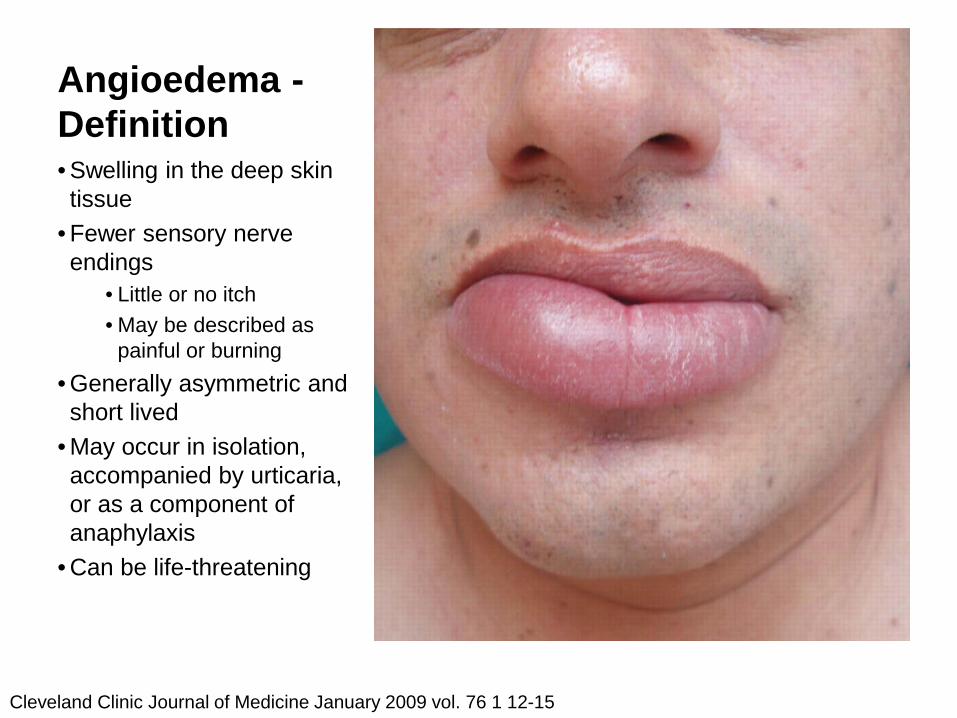
Angioedema - Definition • Swelling in the deep skin tissue
• Fewer sensory nerve endings
• Little or no itch • May be described as
painful or burning • Generally asymmetric and short lived
• May occur in isolation, accompanied by urticaria, or as a component of anaphylaxis
• Can be life-threatening
Cleveland Clinic Journal of Medicine January 2009 vol. 76 1 12-15

Angioedema - Locations • Larynx
– Can develop rapidly – Early symptoms: hoarse voice, throat tightness, and
difficulty swallowing • Skin and mucous membranes
– Mild pain and warmth may be present, burning sensation – Resolves without leaving residual markings on the skin
• Bowel wall – Colicky abdominal pain, sometimes nausea, vomiting
and/or diarrhea – Bowel wall edema often visualized by abdominal CT or
ultrasound
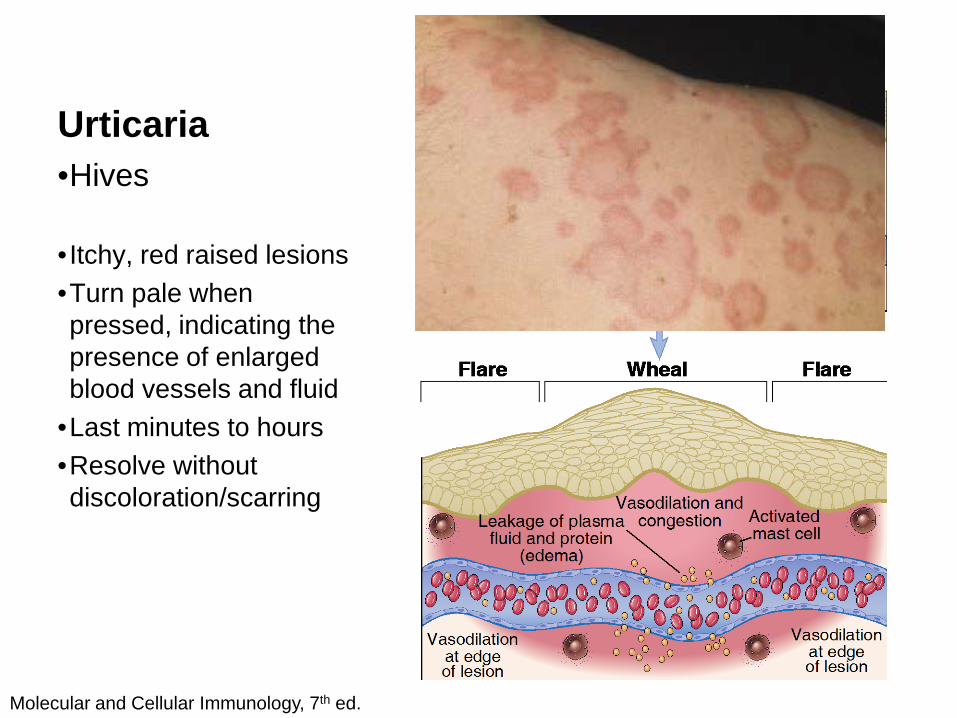
Urticaria •Hives • Itchy, red raised lesions •Turn pale when pressed, indicating the presence of enlarged blood vessels and fluid
•Last minutes to hours •Resolve without discoloration/scarring
Molecular and Cellular Immunology, 7th ed.

Anaphylaxis, Angioedema, Urticaria Causes Approximately 1% of the population is dispensed outpatient epinephrine
WAO Journal 2011; 4:13–37
Mast Cells and the Immune System
Immune System
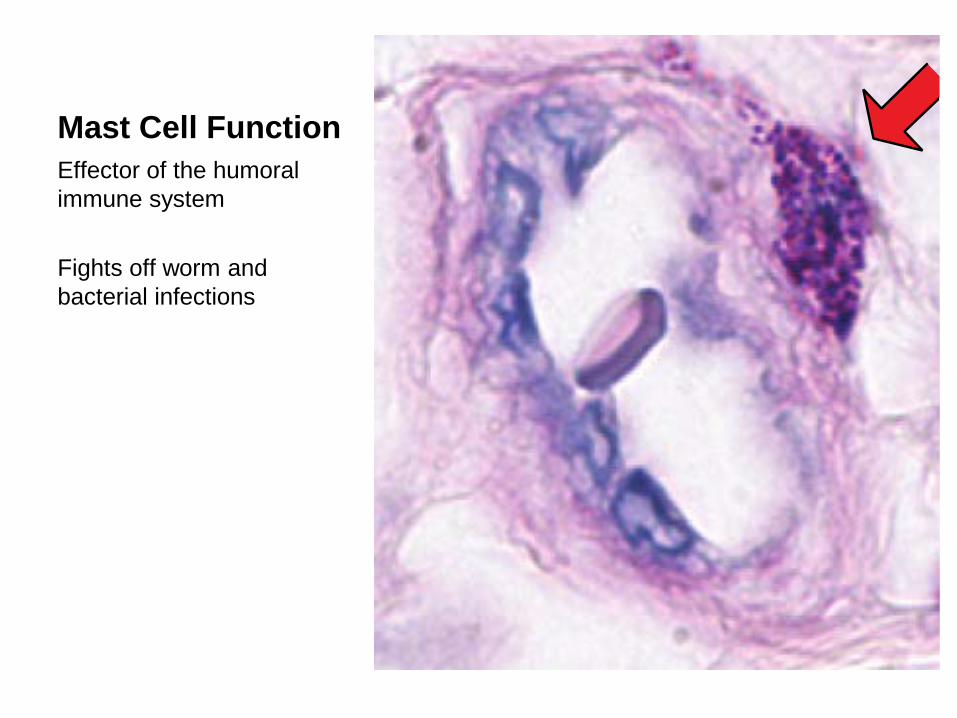
Mast Cell Function Effector of the humoral immune system Fights off worm and bacterial infections

Mast Cell Dysfunction
• Anaphylaxis • Systemic mastocytosis • Mast cell activation syndrome (MCAS) • MCAS and postural tachycardia syndrome
(POTS)
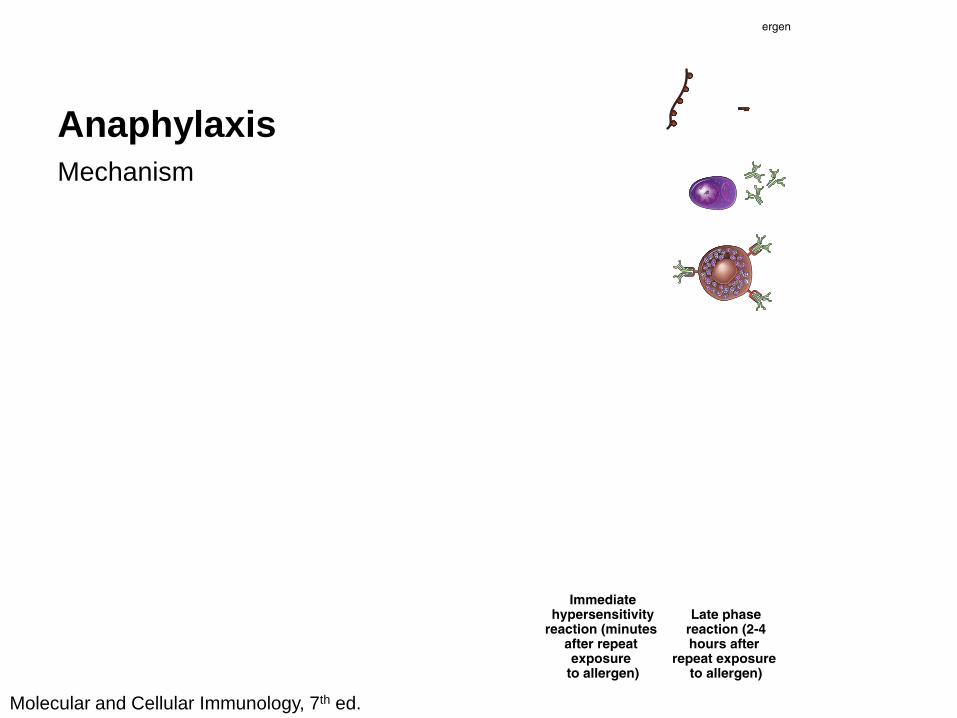
Anaphylaxis Mechanism
Molecular and Cellular Immunology, 7th ed.
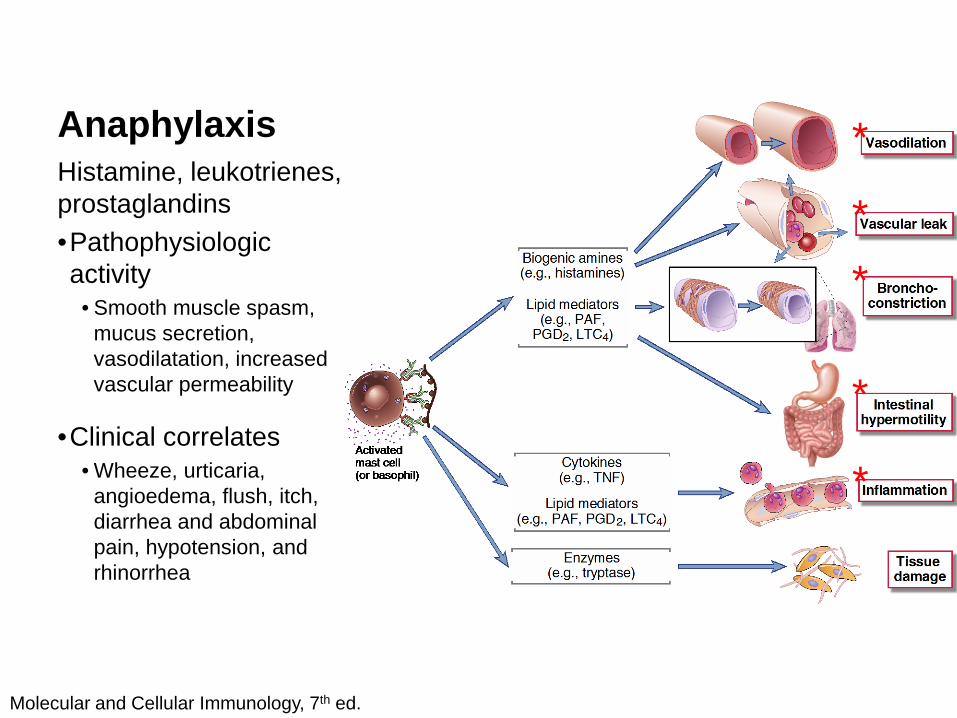
Anaphylaxis Histamine, leukotrienes, prostaglandins •Pathophysiologic activity
• Smooth muscle spasm, mucus secretion, vasodilatation, increased vascular permeability
•Clinical correlates • Wheeze, urticaria,
angioedema, flush, itch, diarrhea and abdominal pain, hypotension, and rhinorrhea
Molecular and Cellular Immunology, 7th ed.
*
*
*
*
*

Anaphylaxis Neutral proteases: tryptase
•Pathophysiologic activity
• Further activation of mast cells
•Clinical correlates • Can magnify response due
to further mast cell activation
• Tissue damage
Molecular and Cellular Immunology, 7th ed.
*
Systemic Mastocytosis
• Excess growth of mast cells and accumulation in 1 or more organs
• 93% of cases due to a mutation of c-kit gene (KIT D816V)
• Symptoms are due to mast cell mediator release
• Rare: 1 in 20,000-40,000 – More common in Caucasians

Systemic Mastocytosis Symptoms
• GI – abdominal pain,
diarrhea, nausea/vomiting • Skin – itching/flushing, fixed
skin lesions • Cardiovascular (CV) – fast
heart rate, loss of consciousness, anaphylaxis
• Nervous system (CNS) – headache, confusion
• Musculoskeletal (MS) – bone pain
• Constitutional – weakness, fatigue, malaise
• Respiratory – shortness of breath, nasal symptoms
GI: 5-80%
Skin: 8-95%
CV: 5-30%
CNS: 10-90%
MS: 9-75%
Const: 12-56%
Resp: 4-57%
Annals of allergy, asthma & immunology. 2010 Jan;104(1):1-10.

Systemic Mastocytosis
• Presence of at least 1 major and 1 minor or 3 minor criteria in bone marrow or other organ
• Major – Excessive mast cells on bone marrow biopsy***
• Minor – Excessive atypical mast cells – c-KIT D816V mutation – Mast cells with surface markers (CD2, CD25, CD117) – Serum tryptase >20 ng/mL

Systemic Mastocytosis
• Neuroendocrine evaluation – Rule out pheochomocytoma, VIPoma,
carcinoid syndrome
• Multispecialty approach likely necessary

Systemic Mastocytosis
• Avoid triggers – Alcohol – Spicy foods – NSAIDs – Narcotics – Intense exercise – Stinging insects – Stress
• Block mast cell related symptoms – H1 Antihistamines – H2 Antihistamines – Epinephrine – Cromolyn – LTRA – Steroids
• Chemotherapy only if severe

MCAS
• Newly recognized disorder • No excessive growth of mast cells • Symptoms are due to mast cell mediator
release • Demographics
– Females: 89% of cases in one series – Can happen in any age group – On average, 4.6 years before referral
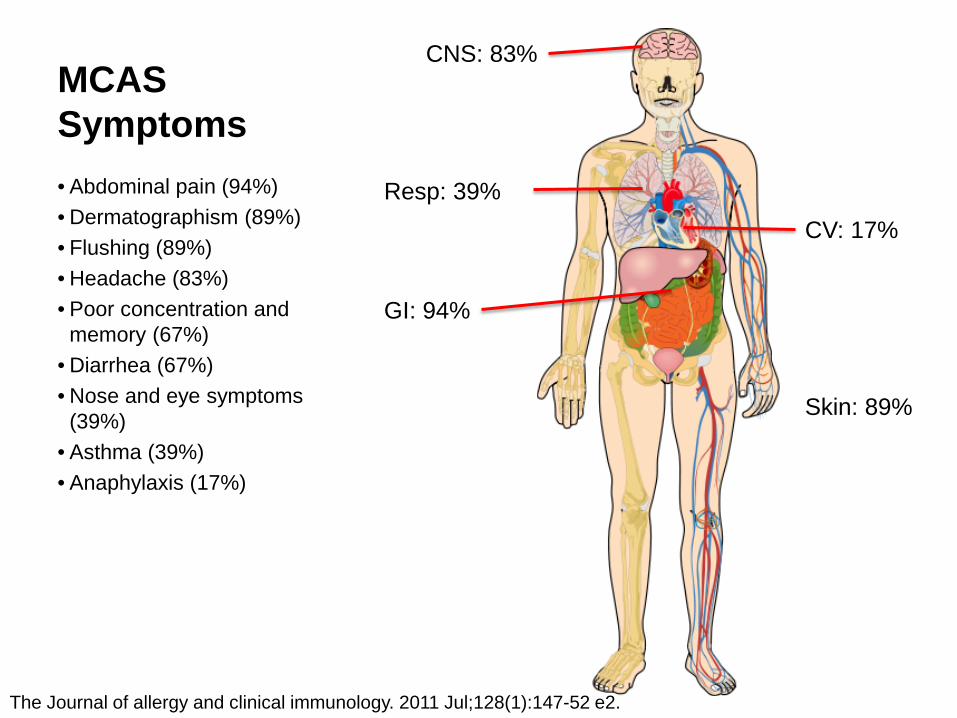
MCAS Symptoms
• Abdominal pain (94%) • Dermatographism (89%) • Flushing (89%) • Headache (83%) • Poor concentration and
memory (67%) • Diarrhea (67%) • Nose and eye symptoms
(39%) • Asthma (39%) • Anaphylaxis (17%)
GI: 94%
Skin: 89%
CV: 17%
CNS: 83%
Resp: 39%
The Journal of allergy and clinical immunology. 2011 Jul;128(1):147-52 e2.
MCAS
• Clinical history • Laboratory evaluation
– Serum total tryptase, 24-hour urine for histamine, N-methylhistamine, prostaglandin D2
• Rule out other causes, including systemic mastocytosis (bone marrow biopsy) – Neuroendocrine evaluation

MCAS
• Avoid triggers – Alcohol – Spicy foods – NSAIDs – Narcotics – Intense exercise – Stinging insects – Stress
• Block mast cell related symptoms – H1 Antihistamines – H2 Antihistamines – Epinephrine – Cromolyn – LTRA – Steroids

MCAS and POTS
• Postural tachycardia syndrome (POTS) – Rare, disabling condition – High heart rate with standing – More common in young females – Unclear cause
• Poor nerve signaling (neuropathic) • Excessive adrenal activation (hyperadrenergic)
– Some patients with flushing, suggesting mast cells might be involved

MCAS and POTS Symptoms
• GI – nausea/vomiting, diarrhea
• Skin – flushing • Cardiovascular (CV) – fast
heart rate, lightheadedness, loss of consciousness
• Nervous system (CNS) – headache, confusion
• Constitutional – weakness, fatigue, dizziness, malaise, anxiety
• Respiratory – shortness of breath, nasal symptoms
GI: 38%
Skin: 100%
CV: 100%
CNS: 63% Const: 88%
Resp: 38%
Hypertension. 2005 Mar;45(3):385-90.
MCAS and POTS
• Tilt table testing • Evaluation and treatment as with MCAS • Trigger avoidance
– Exercise – Prolonged standing – After meals – Premenstrual – Heat intolerance – Emotional stress

Case Presentation Mast Cell Evaluation •Tryptase with episode – 26.7 (elevated)
•Urine histamine with episode – elevated
•Baseline tryptase – NL
•Bone marrow – NL
Neuroendocrine Evaluation •Urine/serum metanephrines – NL •Urine/serum catecholamines – NL
•GI scope for carcinoid – NL •Urine 5’-HIAA – NL •VIP – NL •Cortisol – NL •Neurokinin A – NL •CT scan of chest and abdomen – NL
Case Presentation
• Best diagnosis: MCAS
• The patient was transitioned to more appropriate treatment

Epinephrine Autoinjector
Treatment
• H1-Antihistamines – Decrease itch, flush, urticaria, sneezing, and
rhinorrhea – Do not prevent or relieve obstruction to airflow
or hypotension/shock – Cetirizine, doxepin, cyproheptadine
• H2-Antihistamines – Ranitidine
Ann Emerg Med 2000;36:462-8.
Treatment
• Glucocorticoids • Pharmacologic effects
– Switch off transcription of activated genes that encode pro-inflammatory proteins
• Clinical relevance – Onset of action takes several hours – Used to prevent and relieve mast cell related
symptoms
Ann Allergy Asthma Immunol 2005;95:217-26.
Treatment
• Leukotriene modifying agents (LTMA) – Montelukast, zafirlukast, zileuton
• Cromones (mast cell stabilizer)
– Cromolyn – GI symptoms only
• Dosing very important

Case Presentation
• Changed to: – Cetirizine 20mg twice a day (H1) – Ranitidine 300mg twice a day (H2)
• Start slow prednisone wean • Reviewed epinephrine autoinjector use
and indications
Case Presentation
• He has had only one mild episode including facial flushing, nausea and stomach pain – No Emergency Department visit
• Added zafirlukast 20mg twice a day (LTMA)
• No episodes since then

Resources • Bains SN, Hsieh FH. Current approaches to the diagnosis and
treatment of systemic mastocytosis. Annals of allergy, asthma & immunology. 2010 Jan;104(1):1-10.
• Hamilton MJ, Hornick JL, Akin C, et al. Mast cell activation syndrome: a newly recognized disorder with systemic clinical manifestations. The Journal of allergy and clinical immunology. 2011 Jul;128(1):147-52 e2.
• Shibao C, Arzubiaga C, Roberts LJ, 2nd, et al. Hyperadrenergic postural tachycardia syndrome in mast cell activation disorders. Hypertension. 2005 Mar;45(3):385-90.
• Pardanani A. Systemic mastocytosis in adults: 2012 Update on diagnosis, risk stratification, and management. American journal of hematology. 2012 Apr;87(4):401-11.
Resources
• American Academy of Allergy, Asthma, and Immunology – http://www.aaaai.org
• The Mastocytosis Society – http://www.tmsforacure.org
• The Elephant Project – Dr. Peter Vadas and Sarah Leach

Conclusions
• Mast cell disorders are relatively rare but severe
• Patient history is extremely important • Extensive evaluation and a multispecialty
approach may be necessary to rule out all probable causes
• Good outcomes with appropriate treatment

Questions







