
Mathematical modeling of human eye

The eye: a window on the body
Diseases of the Body:
Diabetes
Hypertension
Neurodegenerative
Disorders (NDD)
Diseases of the Eye:
Glaucoma
Retinopathies
Age-related Macular
Degeneration (AMD)
Need of quantitative methods to
detect and grade vascular abnormalities in the
eyes and identify underlying pathogenic
mechanisms
?

Modeling of Ocular Blood Flow
Glick Eye Institute
IU Medicine
Alon Harris
Brent Siesky
Math IUPUIGiovanna Guidoboni
Lucia Carichino
Simone Cassani
Math PoliMi
Riccardo Sacco
Francesca Malgaroli
Math WSUSergey Lapin
Tyler Campbell

Motivation
• Alterations in retinal hemodynamics are associated
with
– Ocular diseases (e.g. glaucoma, age-related macula
degeneration - AMD)
– And more (e.g. hypertension, diabetes, multiple sclerosis,
Alzheimer, Parkinson)
• The Retinal circulation can be assessed non-invasively
– Visualization (e.g. fundus camera)
– Hemodynamic measurements in macro- and micro-
circulation
Fundus Camera
http://www.medicine.uiowa.edu/eye/Ocular-Fundus-Photograhy/
http://en.wikipedia.org/wiki/Macular_degeneration
Normal AMDDiabetic
Retinopathy

The Human Eye: Physiology of the Retina
• Central Retinal Artery (CRA)
Delivers blood to the retina
in the form of capillaries
which are one cell thick
blood vessels.
• Central Retinal Vein (CRV)
Retrieves used blood and
waste back to the heart for
more oxygen.
• Retinal Arterioles
Small branches of the artery
that distribute blood
throughout the retina.
• Retinal Venules
Small branches of the vein
that collect blood
throughout the retina.

Ocular Blood Flow
Ophthalmic Arteryfrom
Internal
Carot idArtery
to anter iorpart of eye,
face and nose
Temporal
Poster iorCiliaryArtery
NasalPoster ior
CiliaryArtery
Ophthalmic
Vein
Ophthalmic
Vein
Cavernous
Sinus
to InternalJugular Vein
Int raocularPressure
ret ina
choroid
laminacr ibrosa
Cent ralRet inalA rtery
Cent ralRet inalVein
1
Arterial Blood
Pressure
Venous Blood
Pressure
Intraocular
Pressure
Cerebrospinal
Fluid Pressure Intracranial
Pressure
Is driven by:Difference in Arterial and
Venous Blood pressure
Is impeded by:Intraocular pressure (IOP)
Cerebrospinal Fluid pressure (CSFp)
Intracranial pressure (ICP)
Is modulated by:Vascular regulation
Vascular
Regulation

• Intraocular pressure (IOP) is
the overall pressure within the
eye.
• During each cardiac cycle, the
velocity of the blood-flow
within the retina is changed
dramatically.
• Because of this change, the eye
has built in autoregulation
mechanisms that attempt to
maintain constant blood
pressure within the retina.
• These mechanisms can fail and
without proper autoregulation,
some eye diseases can
develop.
Ophthalmic Arteryfrom
Internal
Carot idArtery
to anter iorpart of eye,
face and nose
Temporal
Poster iorCiliaryArtery
NasalPoster ior
CiliaryArtery
Ophthalmic
Vein
Ophthalmic
Vein
Cavernous
Sinus
to InternalJugular Vein
Int raocularPressure
ret ina
choroid
laminacr ibrosa
Cent ralRet inalA rtery
Cent ralRet inalVein
1
Intraocular
Pressure
Intraocular Pressure and Auto Regulation

• Glaucoma is a term used to describe a group of diseases that affect the
optic nerve.
• This occurs in patients with excess IOP caused by poor drainage of the
Aqueous Humor fluid.
• Performing a Trabeculectomy can alleviate some of this pressure but the
damage to the optic nerve is not reversible.
• Macular Degeneration occurs when the central portion of the retina
deteriorates and causes vision loss in more than 10 million Americans.
• Both Glaucoma and Macular Degeneration are incurable diseases and
there no reliable methods to predict their development.
Diseases related to increased IOP

Why modeling?
• Interpretation of clinical data is
challenging! Understand physiology
in health and disease
IOP
CSF
• Pressurized ambient (intraocular pressure - IOP)
• Fluid-structure interactions
• Complex vascular system
• Sub-systems
• Flow regulation
• Traditionally:
• Animal studies
• Clinical or
population-based studies
• Our Approach
• Mathematical models
• Clinical data

• In a disease state, some of the vascular
regulation mechanisms might be impaired,
compromising the oxygenation in the retina.
• There is inconsistency in the scientific
literature regarding the vascular response to
changes in oxygen demand.
• Inconsistent clinical observations are due to
the numerous factors, including arterial blood
pressure and vascular regulation, that
influence the relationship between IOP and
ocular hemodynamics.
• Mathematical modeling can be used to
investigate the complex relationship among
these factors and to interpret the outcomes of
clinical studies.
Why modeling?

• The retinal circulation is described using the
analogy between the flow of a fluid in a
hydraulic network and the flow of current in
an electric circuit
• The vasculature supplying the retina is divided
into five main compartments the CRA,
arterioles, capillaries, venules, and the CRV.
• Using the analogy between hydraulic and
electrical circuits, blood flow is modeled as
current flowing through a network of resistors
(R), representing the resistance to flow offered
by blood vessels, and capacitors (C),
representing the ability of blood vessels to
deform and store blood volume.
Mathematical Model

IOP
Mathematical Model

• Intraocular segments are exposed to the IOP.
• Retrobulbar segments are exposed to the retro laminar tissue
pressure.
• Translaminar segments are exposed to an external pressure based on
stress within the lamina cribosa.
• Diameters of the venules vary passively with IOP whereas the arterioles
are assumed to be affected by the blood pressure.
Mathematical Model

Mathematical Model
Flow Q through a resistor is directly proportional to the
pressure drop P across the resistor.
Flow Q through a capacitor is directly proportional to the
time derivative of the product between the pressure
drop across the capacitor and the capacitance.
volume change = flow in - flow outKirchoff’s law applied to the retinal vascular network

Mathematical Model
Obtain system of ordinary differential equations for the nodal pressures
𝑃1, 𝑃2, 𝑃4, 𝑃5:
The inlet and outlet pressures 𝑃𝑖𝑛and 𝑃𝑜𝑢𝑡 vary with time along a cardiac cycle and,
consequently, the calculated pressures are time dependent.
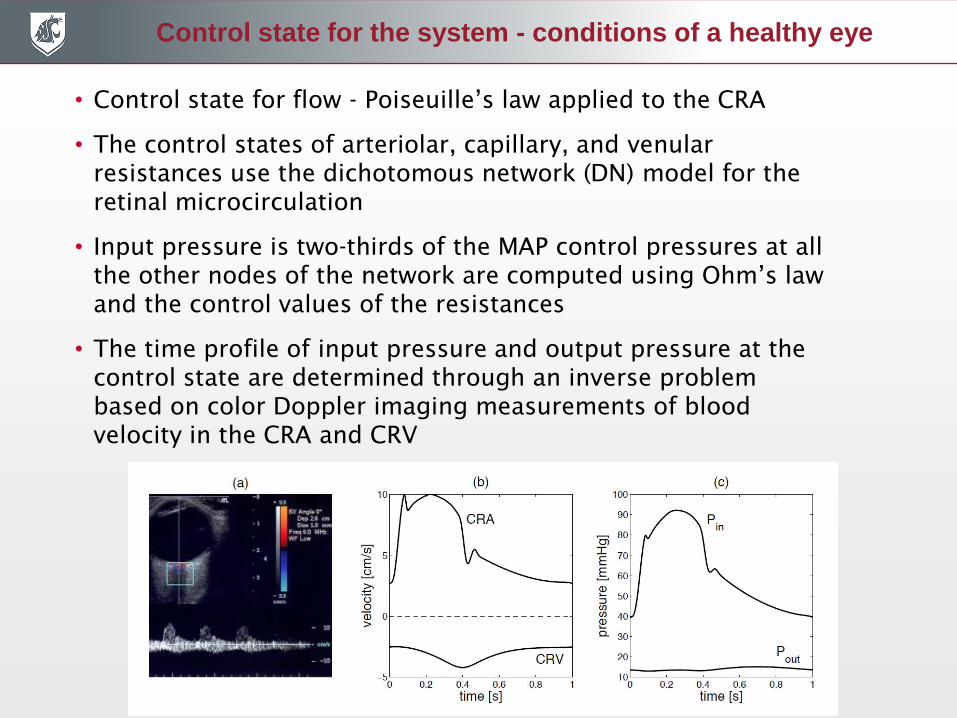
Control state for the system - conditions of a healthy eye
• Control state for flow - Poiseuille’s law applied to the CRA
• The control states of arteriolar, capillary, and venular
resistances use the dichotomous network (DN) model for the
retinal microcirculation
• Input pressure is two-thirds of the MAP control pressures at all
the other nodes of the network are computed using Ohm’s law
and the control values of the resistances
• The time profile of input pressure and output pressure at the
control state are determined through an inverse problem
based on color Doppler imaging measurements of blood
velocity in the CRA and CRV

Passive variable resistances
Start with Navier–Stokes equations in a straight cylinder.

Passive variable resistances
Assume:
• Body forces and mass sources are absent
• 𝑝 is constant on each Σ• 𝑢𝑧 = 𝑢 𝑧 𝑓 Σ , where 𝑢 𝑧 is average axial velocity and 𝑓 Σ is appropriate
shape function
• Axial motion is predominant
Obtain reduced equations:
Where 𝐾𝑟 depends on 𝑓(Σ), 𝑄 𝑧 is volumetric flow and 𝐴 𝑧 is cross-sectional area

Variable passive resistances
• Arterial walls are thicker than
venous walls:
– Arteries described as compressible
tubes
– Veins described as collapsible tubes
– Sterling resistor
The cross-section
changes as transmural
pressure difference
decreases. 𝑘𝐿 = 12𝑟𝑟𝑒𝑓
ℎ
2

Active variable resistances
The resistances for arterioles are modeled through phenomenological description
of blood flow autoregulation:
• Without autoregulation the resistances kept constant equal to their control value.
• With autoregulation the resistance are computed using:
𝑅2𝑎 = R2b =𝑐𝐿 + 𝑐𝑈exp(𝐾 𝑄𝑛𝑜𝐴𝑅 − 𝑄 − 𝑐)
1 + exp(𝐾 𝑄𝑛𝑜𝐴𝑅 − 𝑄 − 𝑐)

Mathematical Model
CRA
CRV
venules
arterioles 𝑅2𝑎 = R2b =𝑐𝐿 + 𝑐𝑈exp(𝐾 𝑄𝑛𝑜𝐴𝑅 − 𝑄 − 𝑐)
1 + exp(𝐾 𝑄𝑛𝑜𝐴𝑅 − 𝑄 − 𝑐)

Results
Comparison of model predicted values with measured data.

Results
Model predicted values of total retinal blood flow; peak systolic velocity in
the CRA; end diastolic velocity in the CRA; and resistivity index ((PSV-
EDV)/PSV) in the CRA as IOP varies between 15 and 45 mmHg for
theoretical patients with low, normal or high blood pressure (LBP-, NBP-,
HBP-) and functional or absent blood flow autoregulation.

Computer-aided identification of novel
ophthalmic artery waveform
parameters in healthy subjects and
glaucoma patients.
L. Carichino, G. Guidoboni, A.C. Verticchio Vercellin, G.
Milano, C.A. Cutolo, C. Tinelli, A. De Silvestri, S. Lapin, J.C.
Gross, B.A. Siesky, A. Harris.

CDI and waveform parameters
• Significant blood velocity derangements in the OA, CRA, and
PCAs are associated with diabetic retinopathy and glaucoma
• CDI is a consolidated noninvasive technique to measure blood
velocity profile in some of the major ocular vessels
• Typical waveform parameters utilized in ophthalmology are
peak systolic velocity (PSV), end diastolic velocity (EDV) and
resistive index (RI).
• CDI is commonly used in the fields of radiology, cardiology,
and obstetrics, and various waveform parameters have been
proposed in the scientific literature.
• Recently, waveform parameters commonly used in renal and
hepatic arteries have been used to characterize OA velocity
waveform in glaucoma patients.
We propose a computer-aided manipulation process
of OA-CDI images that enables the extraction of a
novel set of waveform parameters that might help
better characterize the disease status in glaucoma.

Baseline characteristics of the study group
CDI images:
• Pavia: 50 images acquired by 4 different operators on 9 healthy individuals (Siemens Antares Stellar
Plus™, probe VFX 9-4 MHz vascular linear array)
• Indianapolis: 38 glaucoma patients
(Philips HDI 5000 SonoCT Ultrasound System, 7.5 MHz linear probe)
The PSV, EDV and RI raw data are obtained directly from the ultrasound machine as an average over at
least three cardiac cycles.

Computer-aided image manipulation process
Waveform parameters:
• peak systolic velocity (PSV)
• dicrotic notch velocity (DNV)
• end diastolic velocity (EDV)
• resistive index RI = (PSV-EDV)/PSV
• period of a cardiac cycle (T)
• first systolic ascending time (PSVtime)
• difference between PSV time and DNV
time (Dt)
• subendocardial viability ratio between the
diastolic time interval (DTI) and the
systolic time interval (STI)
• area under the wave (A)
• area ratio f = Aw/Abox = Aw/(PSV Dt)
• normalized distance between ascending
and descending limb of the wave at two
thirds of the difference between PSV and
EDV (DAD/T)

Computer-aided image manipulation process
Waveform parameters:
• peak systolic velocity (PSV)
• dicrotic notch velocity (DNV)
• end diastolic velocity (EDV)
• resistive index RI = (PSV-EDV)/PSV
• period of a cardiac cycle (T)
• first systolic ascending time (PSVtime)
• difference between PSV time and DNV
time (Dt)
• subendocardial viability ratio between the
diastolic time interval (DTI) and the
systolic time interval (STI)
• area under the wave (A)
• area ratio f = Aw/Abox = Aw/(PSV Dt)
• normalized distance between
ascending and descending limb of the
wave at two thirds of the difference
between PSV and EDV (DAD/T)
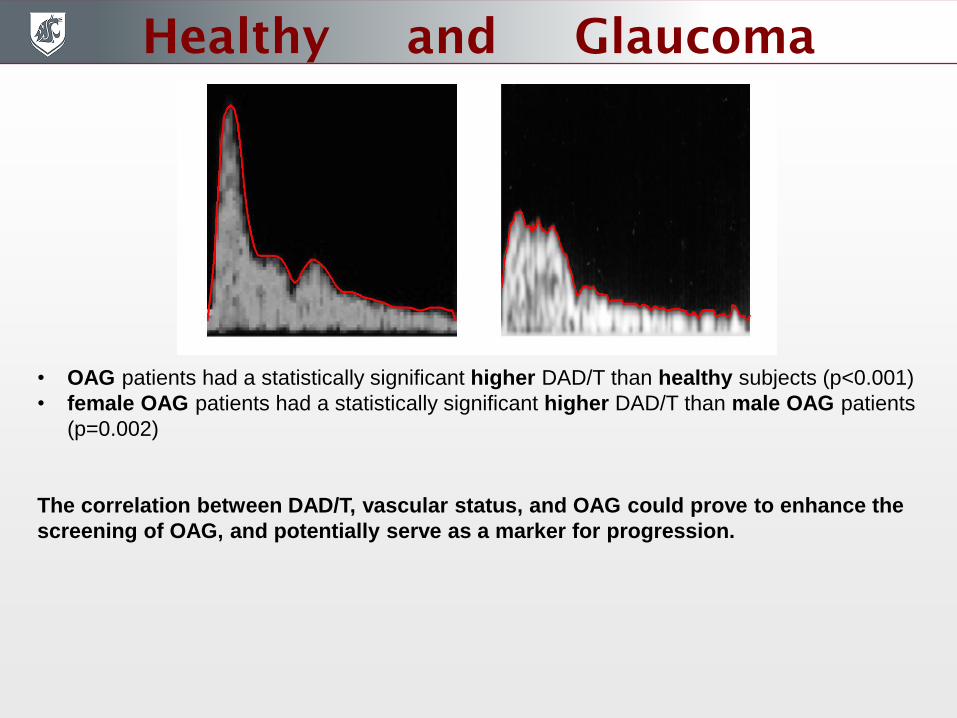
Healthy and Glaucoma
• OAG patients had a statistically significant higher DAD/T than healthy subjects (p<0.001)
• female OAG patients had a statistically significant higher DAD/T than male OAG patients
(p=0.002)
The correlation between DAD/T, vascular status, and OAG could prove to enhance the
screening of OAG, and potentially serve as a marker for progression.








