
Matthew G. Whitbeck, M.D., F.A.C.C. Essentia Health
Matthew G. Whitbeck, MD
STEMI Case Reviews from the SE Region
FINANCIAL DISCLOSURE:
» No relevant financial relationship exists
» 20:28 – 57 y.o. male with hx CAD, prior stenting,
smoking, HTN, HLD, and DM called 9-1-1 two
hours after onset of substernal crushing chest
pain, diaphoresis and SOB
» 20:30 – Casselton Ambulance dispatched; FM
Ambulance dispatched for ALS intercept
» 20:41 – First medical contact by EMS
» 20:46 – 12-lead ECG done and transmitted via
Lifenet to Essentia Fargo ED
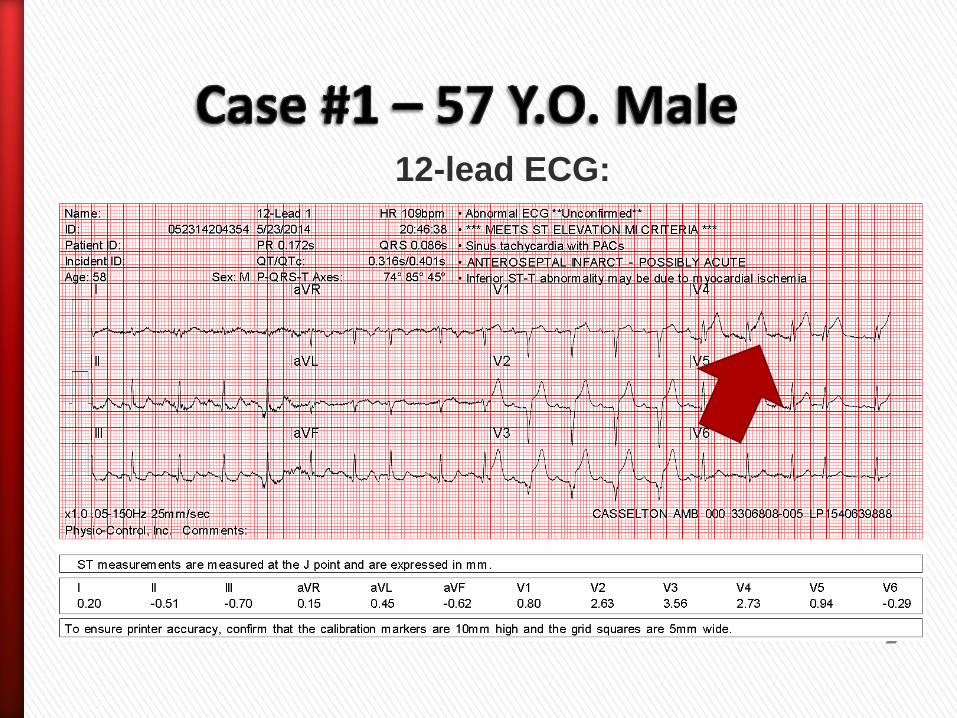
12-lead ECG:

» 20:50 – ALS intercept (F-M
Ambulance) arrived
» 20:51 – Departed scene with patient
» 20:53 – STEMI Alert activated
» 21:10 – Arrived at Essentia ED
» 21:30 – Arrived in cath lab

Pre PCI Post PCI
»21:34 – Case started –
100% mid LAD in-stent
stenosis identified
»21:49 – Reperfusion
obtained with mechanical
thrombectomy and balloon
angioplasty

» 118 minute delay from symptom onset to
call – much work remains in educating
patients to seek help sooner
» Prehospital ECG transmission helps save
time and prepare lab staff, especially during
on-call hours
» BLS services: It is important to develop and
formalize ALS intercept relationships!
Regional Systems of STEMI Care,
Reperfusion Therapy, and Time-to-
Treatment Goals
All communities should create and maintain a regional system of
STEMI care that includes assessment and continuous quality
improvement of EMS and hospital-based activities. Performance
can be facilitated by participating in programs such as Mission:
Lifeline and the D2B Alliance.
I IIa IIb III
Performance of a 12-lead ECG by EMS personnel at the site of
FMC is recommended in patients with symptoms consistent with
STEMI.
I IIa IIb III

» 20:34 – 49 y.o. female with hx of tobacco use presented to Zone 2 ED with c/o nausea, vomiting, and sudden-onset chest pain
» 20:40 – 12-lead ECG completed; STEMI criteria met
» 20:55 – Fibrinolytic given with resulting relief of symptoms and resolution of ST elevations
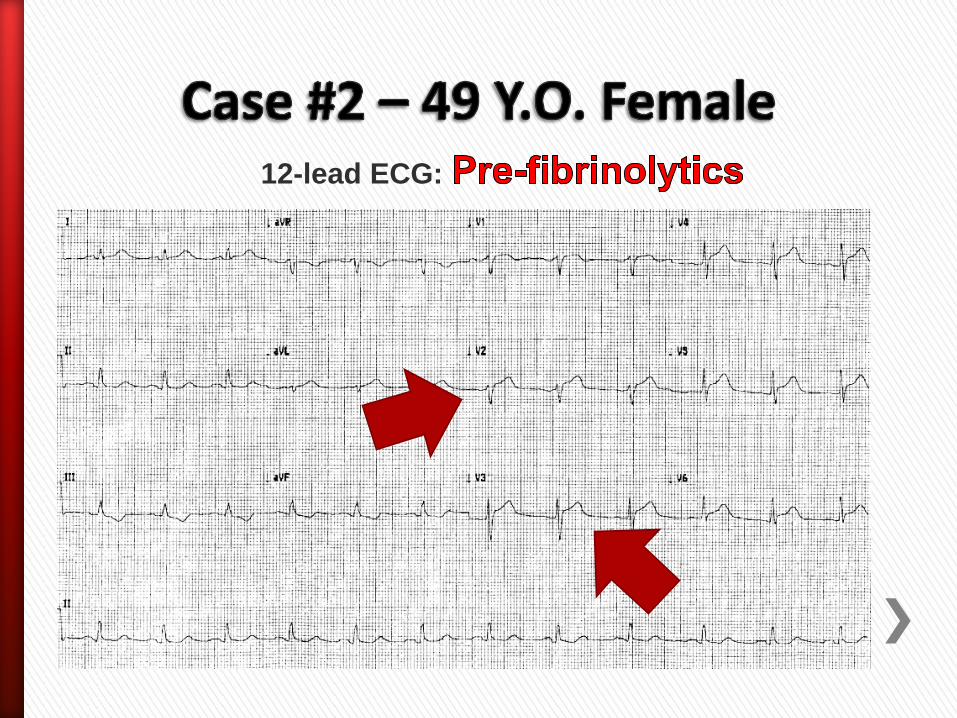
12-lead ECG:
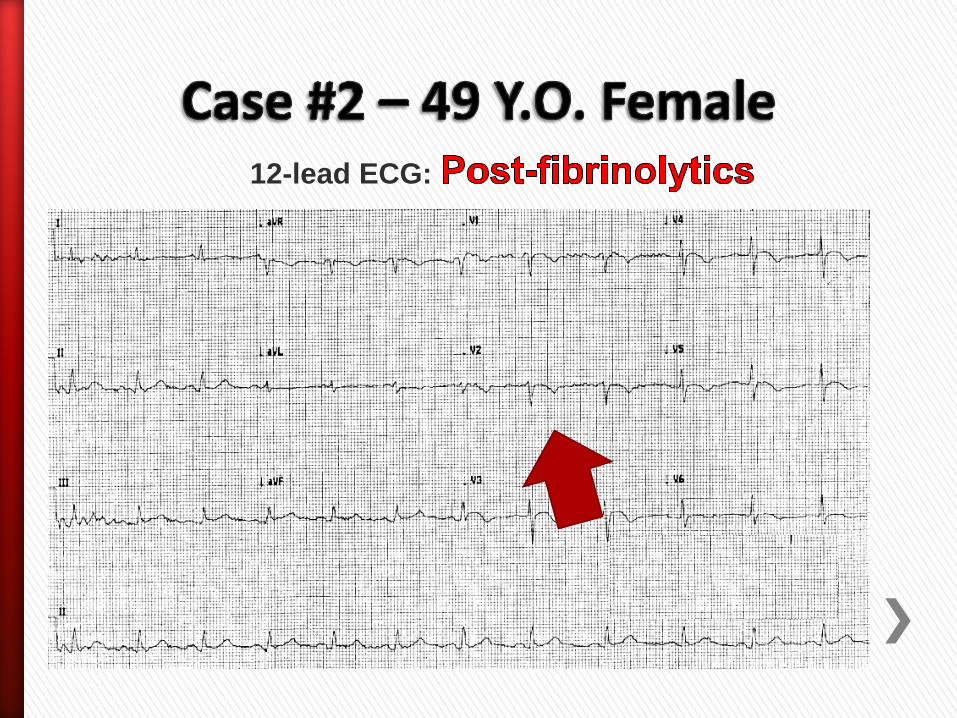
12-lead ECG:

» 20:55 – Transport called and transfer
arranged to Essentia Fargo for CCU monitoring and cardiology evaluation
» 22:08 – Discharged from regional ED via air helicopter
» 22:49 – Arrived at Essentia Fargo ED
» 22:57 – ECG performed; free of ST elevation
» 01:07 – ECG repeated when patient began c/o recurrence of severe chest pain

12-lead ECG:

»01:14 – STEMI Alert activated
»01:42 – Arrived in cath lab
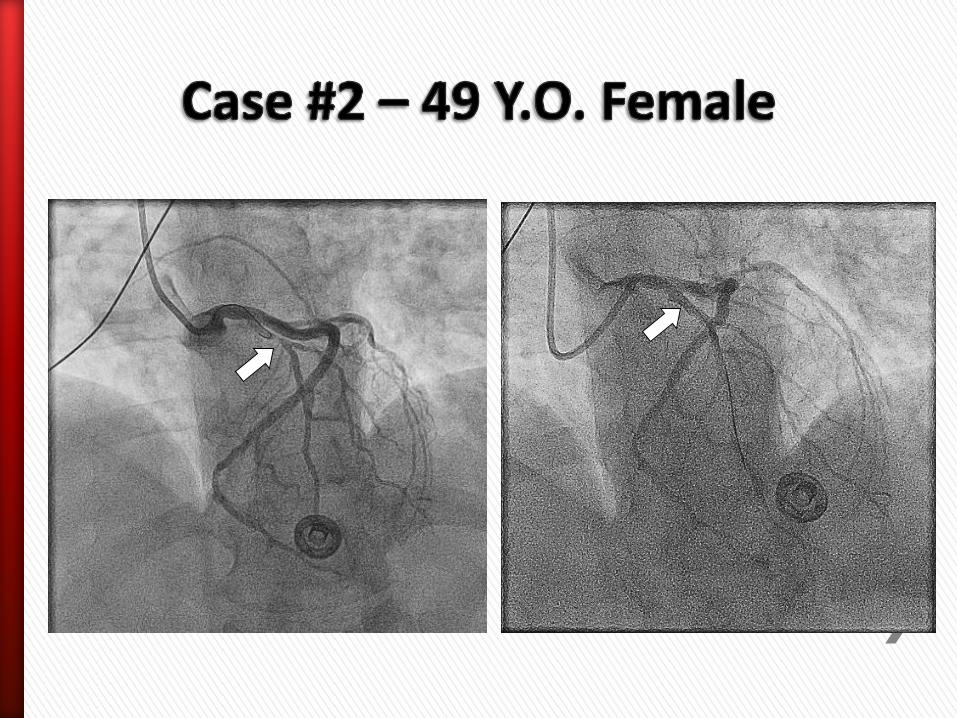

»01:50 – Case started; 99%
occluded proximal LAD identified
»02:15 – Reperfusion obtained with balloon angioplasty and placement of drug-eluting stents
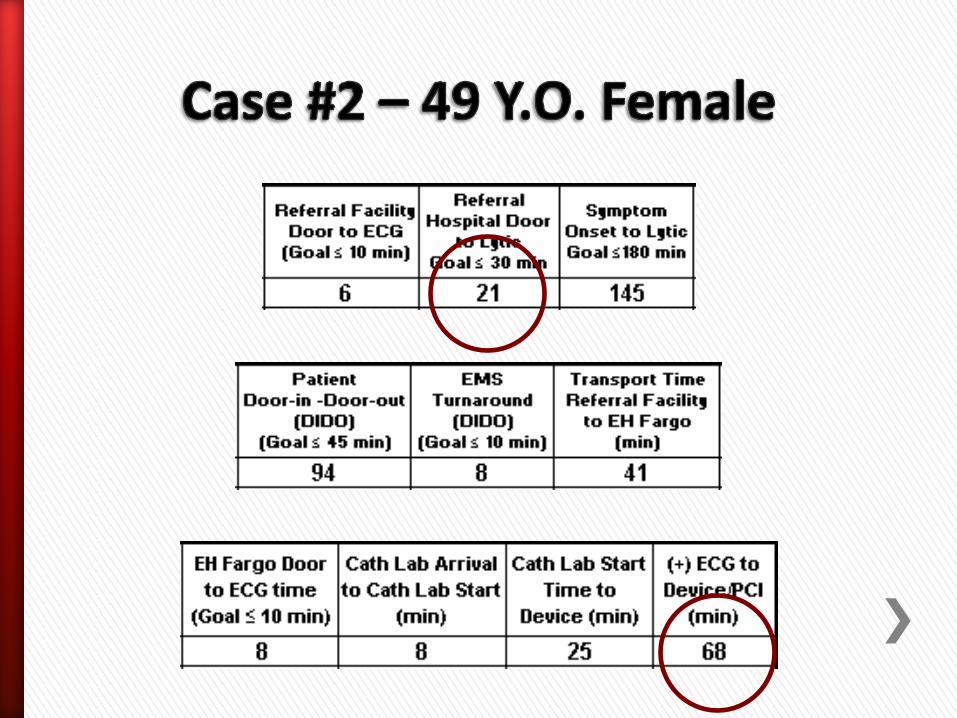
» Air transport service called at same time lytics were given—21 minutes from patient’s arrival
» Non-PCI center door to PCI-center door was 135 minutes – significant delay if patient was transferred for primary PCI and lytics not given
Zone 2 facilities: timely fibrinolytic usage is preferable to
delayed PCI!


» Patient had evidence of re-occlusion; needed cath lab intervention emergently even after initial success of lytics!
Always transfer patients directly to PCI center
post-lytic administration!

“Even when interhospital transport times are short, there may be advantages to the immediate delivery of fibrinolytic therapy versus any delay to primary PCI for patients with STEMI and low bleeding risk who present within the first 1 to 2 hours of symptom onset.”
-2013 ACC/AHA STEMI GuidelinesO’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow
DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:18.
» 11:00 – 54 yo male with hx HTN, ETOH abuse crashed vehicle into a snowbank on a busy road
» 11:02 – Event witnessed; 9-1-1 called by bystanders
» 11:05 – First responders pulled patient from vehicle and began CPR after finding him to be in cardiac arrest

» 11:07 – First medical contact by EMS; ACLS initiated (v-fib identified on monitor; received multiple defibrillations)
» 11:18 – Code Blue alert called to Essentia
» 11:26 – ROSC
» 11:30 – ED arrival
» 11:32 – ECG performed
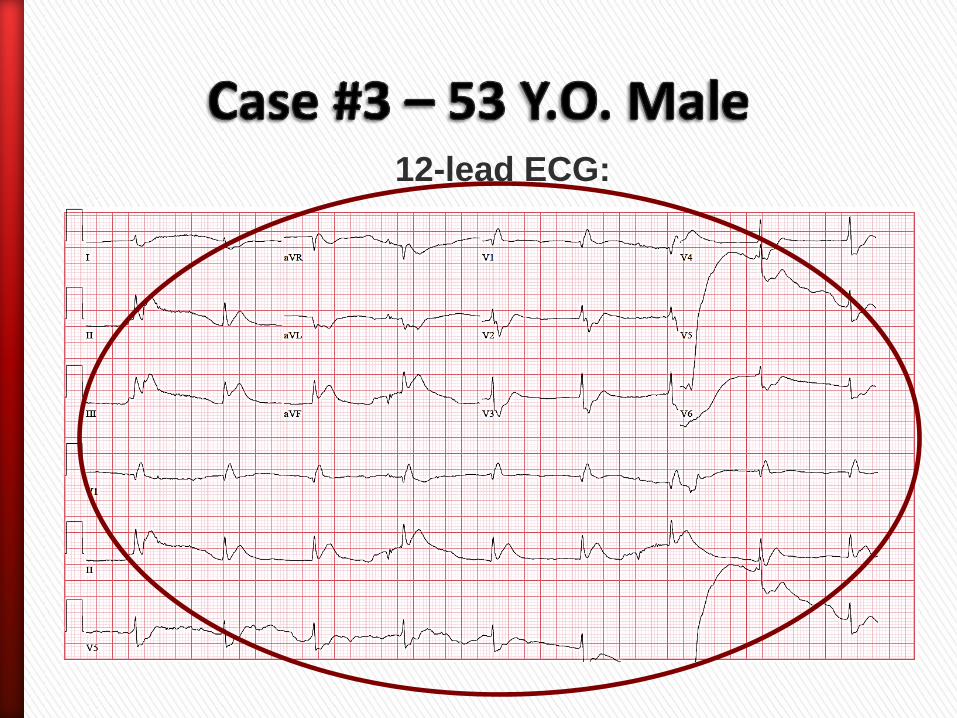
12-lead ECG:

»11:33 – STEMI Alert activated
»11:40 – Patient arrived in cath lab
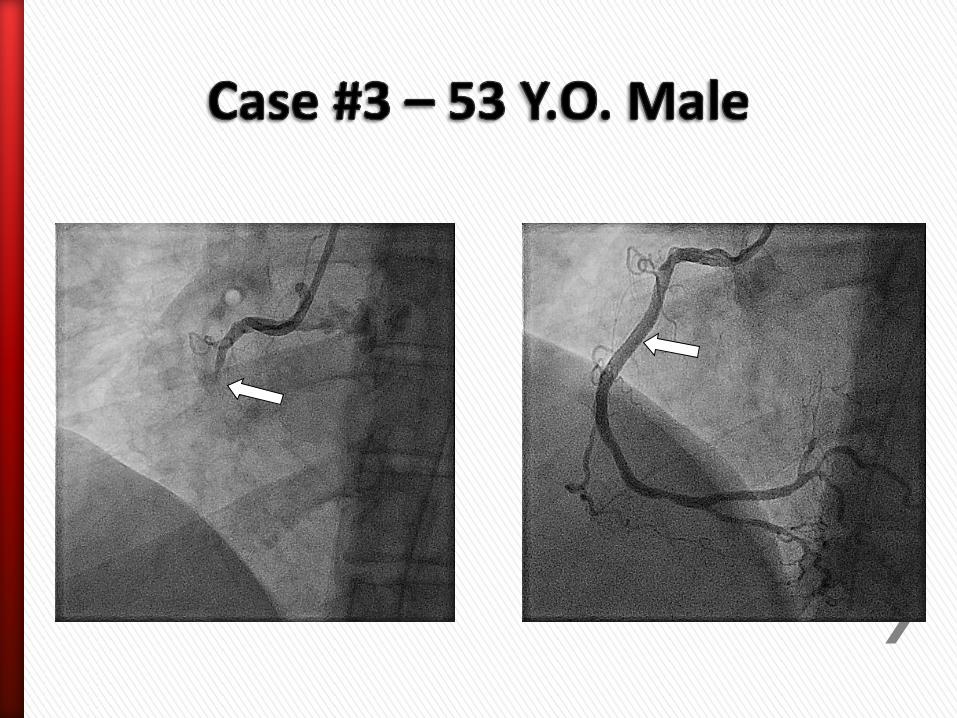
» 11:45 – Case started – 100% mid-RCA occlusion identified
» 12:00 – Reperfusion obtained with manual thrombectomy and stents to mid RCA and right posterolateral artery


» 10:05 47 y.o female with hx of HTN presented to local clinic after a 3-day history of left arm, throat, and upper chest discomfort
» 10:50 – 12-lead ECG completed
» 11:05 – EMS called to transport patient; STEMI Alert called
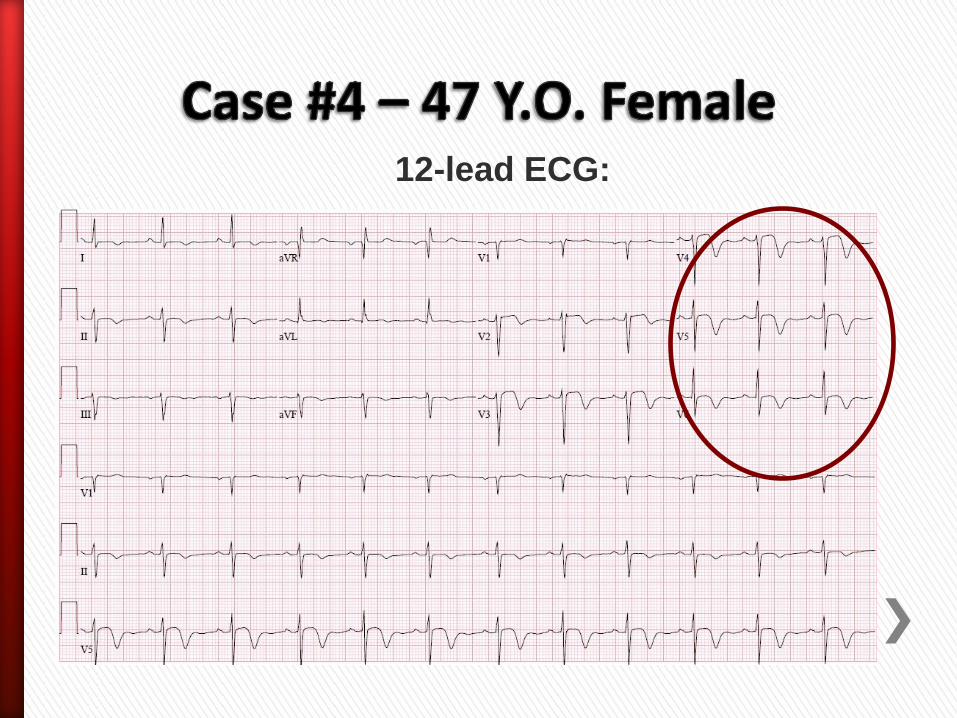
12-lead ECG:
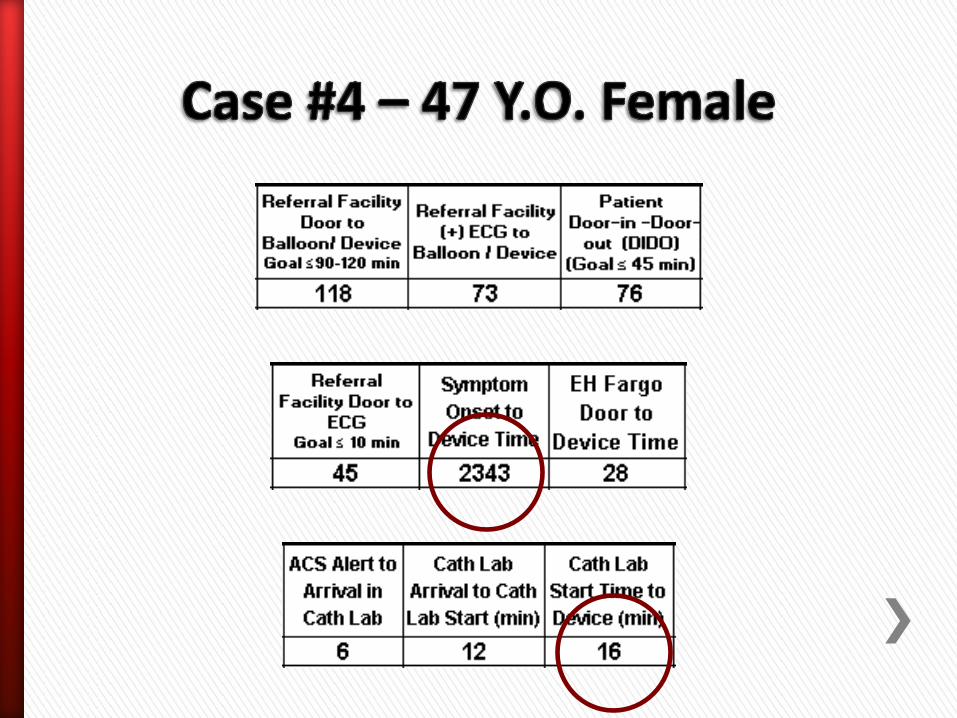
»11:35 – Patient arrived in cath lab


» 11:47 – Case started – 99% distal LAD occlusion identified
» 12:03 – Reperfusion obtained with aspiration thrombectomy, balloon angioplasty, and stent placement

Patient Perspective: Lynnette Anderson
» 07:24 – 53 y.o. male with hx of smoking and family hx of CAD called 911 with c/o sharp chest pain x40 minutes
» 07:24 – FM Ambulance dispatched
» 07:37 – First medical contact by EMS
» 07:40 – 12-lead ECG completed
» 07:44 – ECG transmitted to Essentia ED via Lifenet system

» 07:50 – STEMI Alert activated
» 08:08 – Patient arrived in cath lab
(bypassed ED)
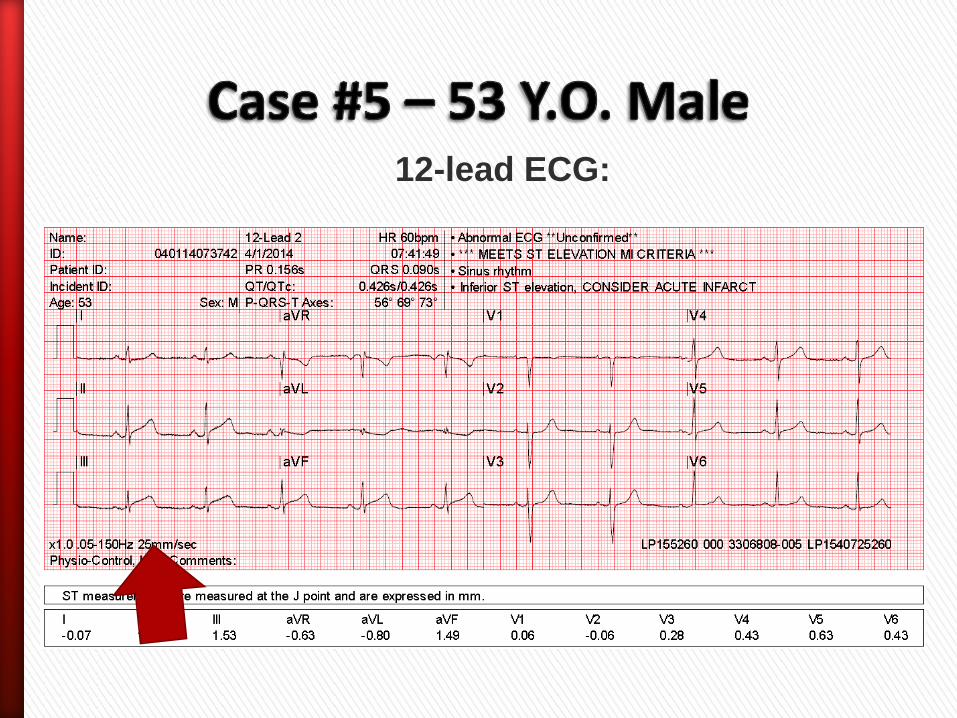
12-lead ECG:
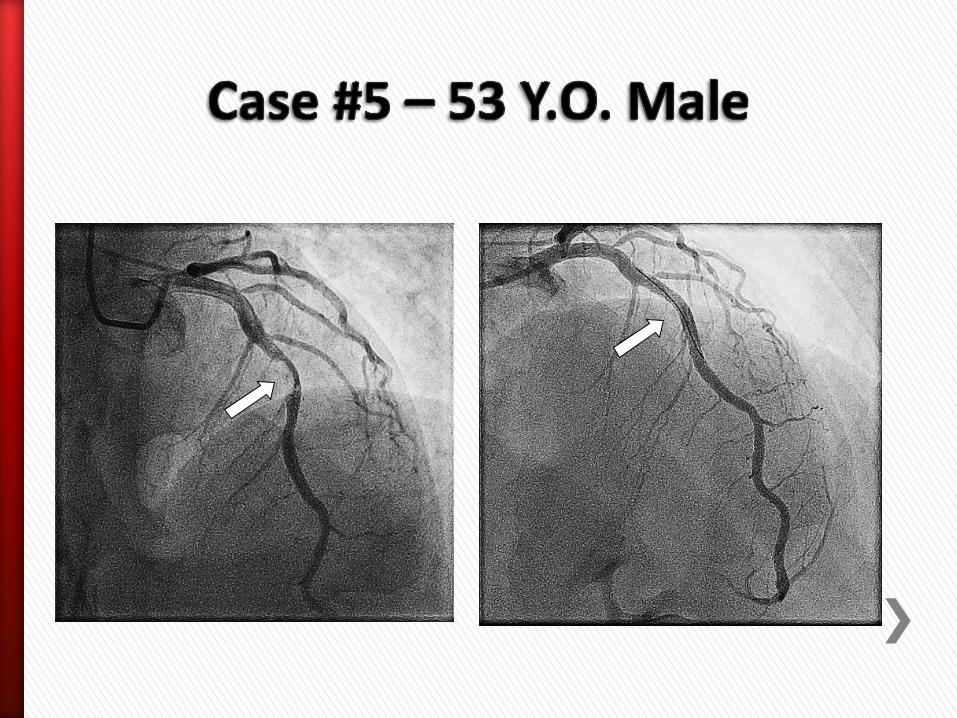
» 08:12 – Case started; 80% occluded mid LAD thrombotic acute plaque rupture identified
» 08:26 – Reperfusion obtained with balloon angioplasty and placement of a drug-eluting stent


ECG Transmission Systems Save Time!!
Prehospital Perspective: FM Ambulance Jessie Pestel, Kathy Lonski
Thank you for your time and
commitment to providing
excellent STEMI care!







