
1
Mechanism of Abnormal Septal Motion in Left Bundle Branch
Block: Role of Left Ventricular Wall Interactions and Myocardial
Scar
Brief title: Modifiers of Septal Motion in Left Bundle Branch Block
John M. Aalen a, b, c, f, MD; Espen W. Remme a, b, d, MSc, Dr.ing.; Camilla K. Larsen a, b, c, f,
MD; Oyvind S. Andersen a, b, c, f, MD; Magnus Krogh a, d, MSc; Jürgen Duchenne g, h, MSc;
Einar Hopp e, MD, PhD; Stian Ross b, c, MD; Ahmed S. Beela g, h, MD; Erik Kongsgaard b, c,
MD, PhD; Jacob Bergsland a, d, MD, PhD; Hans H. Odland b, c, MD, PhD; Helge Skulstad a, b,
c, f, MD, PhD; Anders Opdahl c, MD, PhD; Jens-Uwe Voigt g, h, MD, PhD; Otto A. Smiseth a,
b, c, f, MD, PhD, FACC.
Total word count: 5331
a Institute for Surgical Research, b Center for Cardiological Innovation, c Department of
Cardiology, d The Intervention Center, e Division of Radiology and Nuclear Medicine, Oslo
University Hospital, f Institute of Clinical Medicine, University of Oslo, Oslo, Norway, g Department of Cardiovascular Sciences, University of Leuven, and h Department of
Cardiovascular Diseases, University Hospitals Leuven, Leuven, Belgium
Funding:
Dr Aalen was supported by a grant from the Norwegian Health Association. Drs Larsen and
Andersen were recipients of clinical research fellowships from the South-Eastern Norway
Regional Health Authority. Professor Voigt holds a personal research mandate of the Flemish
Research Council. Professor Voigt and Mr Duchenne were further supported by a grant of the
University of Leuven. Dr Beela received a research grant from the Egyptian Ministry of
Higher Education.
Disclosures:
Professor Smiseth is co-inventor, but has no longer ownership of the patent “Method for
myocardial segment work analysis”, which was used to calculate myocardial work in the
clinical study. The other authors report no conflicts.
Address for correspondence:
Otto A. Smiseth, MD, PhD
Department of Cardiology
Oslo University Hospital, Rikshospitalet
N-0027 Oslo, Norway
Phone: + 47 23 07 00 00
Fax: + 47 23 07 39 17
E-mail: [email protected]
Acknowledgments:
The authors thank Surgical Nurse Aurora Pamplona for her contribution to the animal
experiments.

2
Abstract:
Objectives: This study sought to investigate how regional left ventricular (LV) function
modifies septal motion in left bundle branch block (LBBB).
Background: In LBBB the interventricular septum often has marked pre-ejection shortening,
followed by immediate re-lengthening (rebound stretch). This motion, often referred to as
septal flash, is associated with positive response to cardiac resynchronization therapy (CRT).
Methods: In 10 anesthetized dogs we induced LBBB by radiofrequency ablation and
occluded the circumflex (CX) (n=10) and left anterior descending (LAD) (n=6) coronary
arteries, respectively. Myocardial dimensions were measured by sonomicrometry and
myocardial work by pressure-segment length analysis. In 40 heart failure patients with LBBB,
including 20 with post-infarct scar and 20 with non-ischemic cardiomyopathy, myocardial
strain was measured by speckle-tracking echocardiography and myocardial work by pressure-
strain analysis. Scar was assessed by cardiac magnetic resonance imaging with late
gadolinium enhancement.
Results: During LBBB each animal showed typical septal flash with pre-ejection shortening
and rebound stretch, and reduced septal systolic shortening (p<0.01). CX occlusion caused
LV lateral wall dysfunction and abolished septal flash due to loss of rebound stretch
(p<0.0001). Furthermore, CX occlusion restored septal systolic shortening to similar level as
before induction of LBBB and substantially improved septal work (p<0.001). LAD occlusion,
however, accentuated septal flash by increasing rebound stretch (p<0.05).
Consistent with the experimental findings, septal flash was absent in patients with LV lateral
wall scar due to lack of rebound stretch (p<0.001), and septal systolic shortening and septal
work far exceeded values in non-ischemic cardiomyopathy (p<0.0001). Septal flash was
present in most patients with anteroseptal scar.
Conclusions: LV lateral wall dysfunction and scar abolished septal flash and markedly
improved septal function in LBBB. Therefore, function and scar in the LV lateral wall should
be taken into account when using septal motion to evaluate dyssynchrony.
Condensed abstract:
Septal flash is a characteristic feature of left bundle branch block (LBBB) and predicts
response to cardiac resynchronization therapy (CRT), but is not consistently present. In the
present clinical and experimental study, we evaluated the effect of ischemia on septal motion
during LBBB. LV lateral wall ischemia abolished septal flash and septal work improved
markedly. Similar findings were present in patients with LV lateral wall scar. During septal
ischemia, however, septal flash was preserved. These findings suggest that LV lateral wall
function is important when evaluating dyssynchrony and future studies should investigate
how this is related to CRT response.
Keywords: Cardiac Resynchronization Therapy, Heart Failure, Left Bundle Branch Block,
Myocardial Work, Septal Flash, Strain

3
Abbreviations:
CMR = cardiac magnetic resonance
CRT = cardiac resynchronization therapy
CX = circumflex coronary artery
ECG = electrocardiogram
GLS = global longitudinal strain
LA = left atrial
LAD = left anterior descending coronary artery
LBBB = left bundle branch block
LGE = late gadolinium enhancement
LV = left ventricular

4
Introduction:
Cardiac resynchronisation therapy (CRT) causes reverse left ventricular (LV)
remodelling and improves survival in heart failure patients with left bundle branch block
(LBBB) (1). Using current ECG-based selection criteria, however, only about 50-70% of
patients show positive response. A number of different imaging-based criteria have been
tested to optimize selection of patients for CRT, but so far none are proven to add clinical
value (2).
Observational studies of patients with LBBB have shown an association between
abnormal septal motion and positive response to CRT (3-9). Therefore, it was proposed to use
abnormal septal motion by echocardiography as a means to identify patients who are likely to
benefit from CRT. The characteristic features of septal motion in LBBB are marked pre-
ejection contraction with leftward motion of the septum, followed by immediate re-
lengthening (rebound stretch) and subsequent paradoxical rightward motion (10,11). This
contraction pattern is often referred to as septal flash (4). As shown previously, pre-ejection
shortening is mainly due to active septal contraction (12), whereas rebound stretch is the
result of contractions in late activated remote myocardium (3,11,13). Furthermore, as
suggested by mathematical simulation studies (14), reduction of LV lateral wall contractility
may reduce septal rebound stretch and increase septal shortening in LBBB.
About one third of patients with wide QRS and LBBB do not demonstrate septal flash
(7,15), suggesting that non-electrical factors have major influence on septal motion in LBBB.
Since septal pre-ejection shortening and rebound stretch are dependent on active contraction
in the septum and LV lateral wall, respectively, we hypothesized that a shift in the balance of
forces between the two parts of the ventricle would modify septal flash and septal pump
function. To address the specific hypothesis that impairment of LV lateral wall function
would attenuate rebound stretch and therefore abolish septal flash, we occluded the

5
circumflex coronary artery (CX) in acutely instrumented, anesthetized dogs. We also induced
septal ischemia to determine if impairment of septal function would shift the balance of forces
in favour of the LV lateral wall and modify septal flash accordingly. To investigate the same
hypothesis in patients, we compared patients with LBBB and non-ischemic cardiomyopathy
to patients with LBBB and post infarct myocardial scar.
Methods:
Experimental study
Animal preparation:
Ten mongrel dogs of either sex and body weight of 40±4 kg were anesthetized by
propofol and opioids (single dose methadone 0.2 mg/kg, followed by propofol 3-4 mg/kg and
a bolus of fentanyl 2-3 μg/kg, thereafter continuous infusion of propofol 0.2-1 mg/kg/min and
fentanyl 5-40 μg/kg/hour). The animals were ventilated and surgically prepared as previously
described (16), including partial splitting of the pericardium from apex to base and loose
resuturing of the pericardial edges after completed instrumentation. Cardiac and aortic
pressure catheters and catheter for radiofrequency ablation were introduced via peripheral
vessel incisions and a left atrial (LA) pressure catheter was introduced via the LA appendage.
To obtain LV lateral wall ischemia we occluded the proximal part of the CX by an adjustable
extravascular occluder cuff (n=5) or intravascular balloon inflation (n=5). Similarly, septal
ischemia was obtained by proximal left anterior descending coronary artery (LAD) occlusion
(adjustable occluder (n=1) or balloon inflation (n=5)). In animals with both LAD and CX
occlusion (n=6), the protocol was varied so that LAD was occluded first in 4 animals and CX
first in 2 animals. In one animal the posterior descending coronary artery (PDA) was occluded
simultaneously as LAD to obtain adequate septal ischemia. The National Animal

6
Experimentation Board approved the study. The animals were supplied by the Center for
Comparative Medicine (Oslo University Hospital, Rikshospitalet, Oslo, Norway).
Pressures, dimensions and electromyograms
LV pressure was measured by a 5F micromanometer-tipped catheter (model MPC 500,
Millar Instruments Inc., Houston,TX, USA). The LV micromanometer was zero referenced to
LA pressure measured via a fluid-filled catheter during diastasis, using extrasystolic beats
with long diastoles.
LV dimensions were measured as circumferential segment lengths by sonomicrometry
using 2 mm wide crystals (Sonometrics Corporation, London, Ontario, Canada) implanted in
the inner third of the myocardium in the interventricular septum and in the posterior, anterior
and lateral LV walls. Apical and basal crystals were added to allow measurement of LV
volume (17). The ultrasonic crystals were combined with a bipolar electrode for recording of
intramyocardial electromyograms. This enabled simultaneous assessment of myocardial
electrical and mechanical activation. Data were sampled at 200 Hz.
Experimental protocol:
LBBB was induced by radiofrequency ablation as previously described (12).
Measurements were obtained during sinus rhythm or atrial pacing prior to and after 61±16
seconds of complete CX occlusion and after 42±16 seconds of complete LAD occlusion.
Data analysis:
Values are given as average of three consecutive heart beats. Systolic shortening was
measured as end-diastolic minus end-systolic dimension. End-diastole was defined as onset
septal shortening following myocardial electrical activation as determined by the septal
electromyogram. Septal pre-ejection shortening, rebound stretch and ejection shortening were

7
measured as indicated in Figure 1. LV lateral wall pre-ejection lengthening was defined as the
corresponding stretch seen simultaneously with septal pre-ejection shortening. Systolic stretch
index was calculated as the sum of systolic stretch in septum and LV lateral wall (18).
Segmental myocardial work was estimated as the pressure-segment length loop area. Work
performed during counter-clockwise rotation was defined as positive and work during
clockwise rotation, reflecting stretching of the segment, was considered negative. Work for a
given segment was defined as the sum of positive and negative work.
Clinical study
Study population:
Forty heart failure patients with LBBB were recruited from the Department of
Cardiology at Oslo University Hospital, Oslo, Norway and University Hospitals Leuven,
Leuven, Belgium. All patients were planned for CRT implantation. Patients were separated
based on non-ischemic (n=20) and ischemic (n=20) cause of cardiomyopathy and the latter
was further divided into a posterolateral (n=10) and anteroseptal scar group (n=10) based on
predominant scar location. Cardiac magnetic resonance (CMR) imaging with late gadolinium
enhancement (LGE) ruled out previous myocardial infarction in 17 out of 20 non-ischemic
patients. In the remaining 3 patients, a coronary angiogram without signs of significant
coronary artery disease was performed within the last 10 months. CMR with LGE was
performed in 8 out of 10 patients in the posterolateral scar group and all 10 patients in the
anteroseptal scar group. For posterolateral scar patients not undergoing CMR (n=2), scar was
assessed echocardiographically by an experienced reader. Medical history, clinical
examination, ECG and echocardiography were obtained in all participants. LBBB was defined
according to Strauss (19).

8
The study was approved by the Regional Ethics Committees and written, informed
consent was obtained from all study participants.
Echocardiography and strain analysis:
A Vivid E9 or E95 ultrasound scanner (GE Vingmed Ultrasound, Horten, Norway)
was used to acquire two dimensional (2D) grey-scale echocardiographic images from
parasternal and apical views. Average frame rate was 60±9 frames/s. Ventricular volumes and
LV ejection fraction were calculated by the biplane Simpson’s method.
Global and segmental longitudinal strain analyses were performed by speckle tracking
echocardiography (Echopac, GE Vingmed Ultrasound, Horten, Norway). Segmental strains
were obtained from the average septal and LV lateral wall strain curves in single wall analysis
in the apical 4-chamber view. Systolic shortening was measured at end-systole. Septal pre-
ejection shortening, rebound stretch, ejection shortening, and systolic stretch index were
measured similar to the experimental study (Figure 1).
Estimation of regional work:
An index of segmental myocardial work was calculated by LV pressure-strain analysis
using a semi-automated analysis tool (Echopac, version 202, GE Vingmed Ultrasound,
Horten, Norway). The method, which includes a non-invasive estimate of LV pressure, was
validated previously and is described in detail in the validation paper (20). Similar to the
experimental study, work for a segment was calculated as the sum of positive and negative
work.

9
CMR and scar analysis:
Patients were scanned with a 1.5 or 3.0 Tesla unit (in Oslo: Aera or Skyra, Siemens,
Erlangen, Germany; in Leuven: Ingenia, Philips Healthcare, Best, the Netherlands), using a
phased array coil. LGE images in long- and short axis projections were obtained during steady
state after intravenous injection of 0.15 mmol/kg gadoterate meglumine (Doteram™, Guerbet,
Villepinte, France). An experienced radiologist visually interpreted the LGE images to
determine if myocardial infarct was present. Infarct size was thereafter quantified
semiautomatically in Segment software v2.0 R5270 (21) using a stack of short axis slices, and
polar maps were constructed using a 17 segment model (22). Myocardial infarct size was
reported as percentage of the total amount of tissue per segment. Anteroseptal wall infarct was
defined as the average infarct size of the LV anterior and septal segments, whereas
posterolateral wall infarct was defined as the average infarct size of the LV posterior and
lateral wall segments.
Statistical analysis:
Values are presented as mean ± standard deviation (SD). If not otherwise stated,
comparisons within the same group were performed by paired samples t-tests, whereas
comparisons between two groups were performed by independent samples t-tests. A value of
p<0.05 was considered significant for the experimental study. Since comparison of each of
the two ischemic groups to the non-ischemic group in the clinical study was not orthogonal,
we used Bonferroni correction so that only a value of p<0.025 was considered significant.
IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp was used for the
analyses.

10
Results:
Experimental study
In each animal induction of LBBB caused abnormal septal motion with pre-ejection
shortening followed by rebound stretch and marked reduction in septal systolic shortening
(Table 1). A representative septal strain trace is displayed in Figure 1.
Occlusion of CX caused marked hypokinesia in the LV lateral wall (p<0.0001), and
abolished septal flash due to loss of rebound stretch (p<0.0001) (Figures 2 and 3, Table 1).
Furthermore, CX occlusion restored septal systolic shortening to values similar to control
recordings prior to induction of LBBB (4.2±1.3 vs. 4.0±2.6 mm, respectively, NS) (Figure 3).
Figure 4 shows how progressive reduction in LV lateral wall systolic shortening during
increasing ischemia was associated with progressive decrease in septal rebound stretch,
illustrating the tight coupling between contractile function in early-activated septum and late-
activated LV lateral wall.
Occlusion of the LAD, on the other hand, increased septal rebound stretch (p<0.05)
and caused marked reduction in septal systolic shortening (p<0.02) (Figure 2, Table 1). Septal
pre-ejection shortening was maintained during LAD occlusion. There was no significant
change in LV lateral wall shortening.
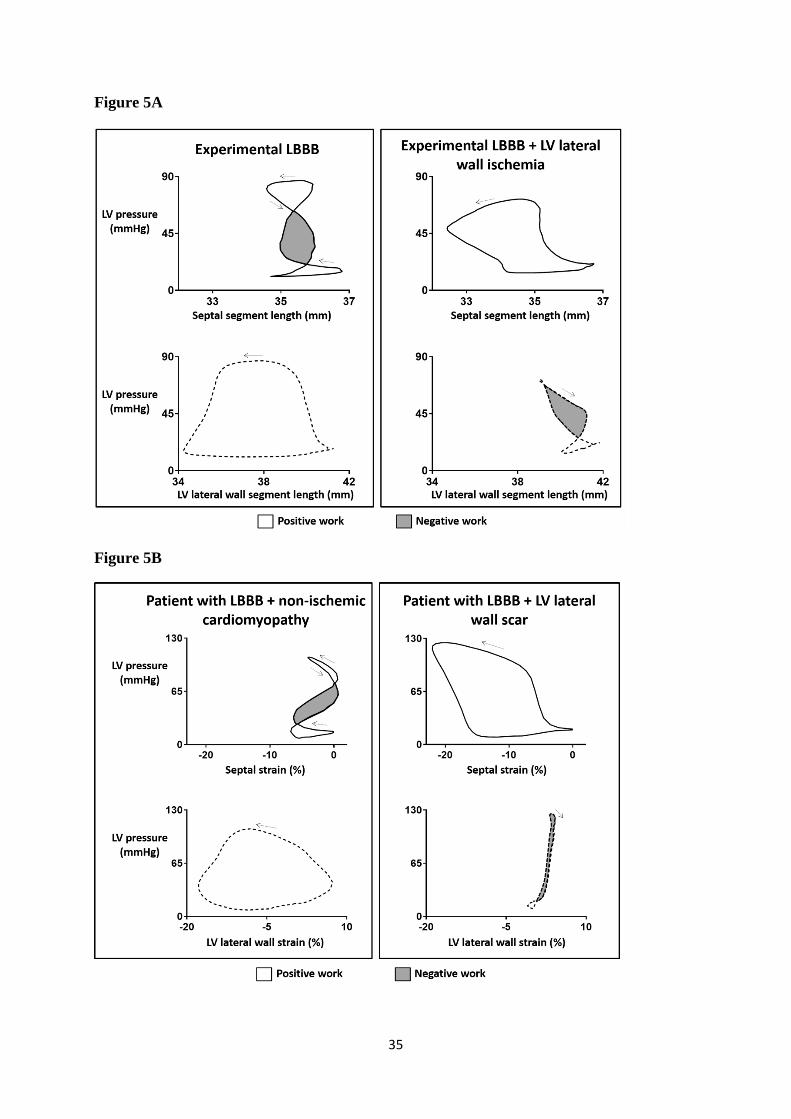
Figure 5A shows a grossly abnormal pressure-segment length loop for the septum with
lengthening during part of systole, which is typical for LBBB. The systolic lengthening
implies that work was performed by other parts of the ventricle to stretch the septum, which
by definition is negative septal work, and is indicated by the gray-shaded part of the loop.
During CX occlusion, septal function improved markedly as the septum performed positive
work throughout the entire heart cycle (Figure 5A, Table 1). During LAD occlusion, however,
septal dysfunction was aggravated as indicated by marked increase in rebound stretch and

11
septum behaved as a net passive structure during most of systole (Table 1). The supplemental
video illustrates beat-to-beat changes in the septal and LV lateral wall pressure-segment
length loops with CX occlusion during LBBB.
Clinical study
All patients were in sinus rhythm with ECG features of LBBB and there were similar
QRS-duration and LV ejection fraction among the groups (Table 2). Patients with
posterolateral scar had largest LV volumes, whereas patients with anteroseptal scar had lowest
absolute values for global longitudinal strain (GLS) (Table 2).
For the group of patients with posterolateral scar undergoing CMR, gadolinium
enhanced tissue represented 61±26% of LV posterolateral wall and 13±9% of the anteroseptal
wall. For the anteroseptal scar group, gadolinium enhanced tissue represented 32±18% of the
anteroseptal wall and 6±7% of the posterolateral wall.
As expected, LV lateral wall shortening was substantially reduced in the posterolateral
scar group (p<0.001 vs. non-ischemic group) (Figure 2, Table 2). Similar to the observations
in the experimental study with CX occlusion, rebound stretch was completely absent in
patients with posterolateral scar (p<0.001 vs. non-ischemic group), and septal systolic
shortening was substantially larger (p<0.0001 vs. non-ischemic group) (Figure 2 and Figure 6,
Table 2). In patients with anteroseptal scar, however, septal rebound stretch was present
(Table 2).
Segmental pressure-strain loop analysis showed marked differences between patients
with posterolateral scar and non-ischemic patients. As illustrated in Figure 5B, non-ischemic
LBBB patients had deformed septal pressure-strain loops, indicating reduced positive work

12
and a substantial portion of negative work. This was accompanied by a large pressure-strain
loop area in the LV lateral wall, reflecting increased lateral wall work. In patients with
posterolateral scar there was markedly lower LV lateral wall work (p<0.002) (Table 2). This
was, similar to the experimental findings, associated with a large septal pressure-strain loop
area, reflecting that the septum performed more positive work (p<0.001) (Figure 5B).
Discussion:
The present study demonstrates that abnormal septal contraction pattern in LBBB can
be enhanced or aggravated by purely mechanical factors. In experimental LBBB, induction of
LV lateral wall ischemia gradually abolished septal rebound stretch and improved septal
systolic shortening to similar values as recordings during normal conduction, whereas
induction of septal ischemia increased rebound stretch and caused reduction of septal systolic
shortening. This interaction between septal and LV lateral wall function in LBBB was
confirmed in the clinical study by the observation that patients with LBBB and LV lateral
wall scar had apparently normal septal contraction pattern. In patients with LBBB and
anteroseptal scar there was abnormal septal motion, essentially similar to patients with LBBB
and non-ischemic cardiomyopathy.
Taken together, these observations indicate that abnormal septal motion in LBBB is
determined not only by electrical conduction delay, but also by the balance of contractile
forces between septum and LV free wall. Our findings help to explain why a substantial
number of LBBB patients do not have septal flash (7), and suggest that function and structure
of the LV lateral wall should be taken into account when using septal contraction pattern to
evaluate LV dyssynchrony.
13
Terminology and mechanisms of abnormal septal motion in LBBB
Abnormal early-systolic septal motion in LBBB was defined as septal beaking by
Dillon et al (1974) who used M-mode echocardiography (23). Somewhat later the same
phenomenon was imaged by tissue Doppler echocardiography and the color change of early-
systolic septal thickening/thinning was referred to as septal flash (4). Mechanisms behind
abnormal septal motion in LBBB have been debated. Rapid leftward motion of the septum at
onset systole has been attributed to right ventricular (RV) contraction preceding LV
contraction, causing RV pressure to transiently exceed LV pressure and septum moves
leftwards analogous to a passive membrane (24,25). Subsequently, when LV pressure exceeds
RV pressure, the septum is pushed towards the RV and accounts for paradoxical rightward
motion of the septum in LBBB. The proposed mechanism for leftward motion of the septum
was challenged by studies from our group, which concluded that the pre-ejection septal
shortening was mainly due to active septal contraction (12,26). This was based upon the
observation that the septum was contracting against rising LV pressure and rising trans-septal
pressure, which is not compatible with passive motion. Furthermore, the LV pressure-segment
length relation was shifted upwards during pre-ejection, indicating stiffening of the
myocardium. This was confirmed in the present study as illustrated in Figure 5A (upper left
panel). Walmsley et al (27) in a simulation study, argued in favor of a passive mechanism.
When taking the different studies into account, it seems likely that a passive mechanism is
superimposed on the active pre-ejection septal contraction and may contribute to the abnormal
leftward shift of the septum in LBBB.
As shown previously, septal rebound stretch is due to contraction in the LV lateral
wall (3,11,13). This mechanism was supported by the observation in the present study that
rebound stretch and paradoxical rightward septal motion were lost during LV lateral wall
ischemia (Figure 3). Unfortunately, the term septal flash is used inconsistently in the

14
literature, and therefore it may be preferable to specify the abnormal motion rather than using
a term such as septal flash.
Modifiers of abnormal septal motion in LBBB
Mathematical simulation studies have suggested that septal contraction patterns typical
for LBBB can be modified by changing regional LV contractility (14). The present study
shows that this mechanism is operative in the in vivo heart as indicated by the tight coupling
between septal rebound stretch and contractile function in the LV lateral wall in the
experimental study, and the observation that septal contraction pattern was apparently normal
in patients with scar in the LV lateral wall.
Enhanced septal deformation pattern during LV lateral wall ischemia and scar was
reflected in marked improvement in septal work estimated by septal pressure-dimension
analysis. Therefore, not only septal deformation pattern, but also septal pump function was
markedly improved when the LV lateral wall was dysfunctional. In a recent study of patients
with LBBB we also demonstrated a strong afterload dependency of septal motion (28). In that
study we showed aggravation of septal dysfunction with enhanced septal rebound stretch
during acute elevation of aortic pressure (28). Therefore, septal contraction pattern in LBBB
is modified by non-electrical factors, which need to be taken into account when using septal
contraction pattern as marker of electrical dyssynchrony.
In the present clinical study, there was no difference in rebound stretch between non-
ischemic patients and patients with anteroseptal scars, which is in apparent contradiction to
the experimental data where septal ischemia increased septal rebound stretch. This difference
between the acute dog experiments where ischemic myocardium is relatively elastic (29) and
post infarct patients may be due to increased stiffness of the scar as stiff tissue is less prone to
stretch. Furthermore, most of the patients with anteroseptal scar had apical aneurysms that

15
could potentially absorb displaced blood due to shortening in the LV lateral wall and thereby
lead to less stretch in the mid and basal portions of the septum.
Despite proximal LAD occlusion in the experimental study and anteroseptal scar in the
clinical study, there were no differences in pre-ejection septal shortening as compared to no
ischemia, which is somewhat unexpected assuming this is an active contraction. This could in
part be explained by the fact that septal pre-ejection shortening occurs against low LV
pressure representing only a small amount of work and, hence, can still be performed by a
weakened segment. In accordance with this, it was shown by Lyseggen et al that short-lasting
pre-ejection shortening was preserved in ischemic segments (30) and furthermore, computer
modeling studies of LBBB have shown that septal pre-ejection shortening was present despite
reduced septal contractility (14). However, collaterals preventing complete septal ischemia in
the dog model and substantial amounts of viable myocardium, especially in the basal and
inferior parts of the septum in anteroseptal scar patients, have likely affected our results. This
does not necessary limit clinical relevance as scar in the entire septum is rare, also after LAD-
infarcts (31).
Posterolateral scar and CRT response
In patients evaluated for CRT, septal rebound stretch has been suggested as a
functional substrate for CRT (3), and in support for this concept it was shown that
normalization of septal motion after CRT implantation is a predictor of long term survival (7).
The finding that reduced contractility in the LV lateral wall markedly improved septal
contraction pattern raises the question whether such patients experience favorable effect from
CRT. In fact, there is convincing evidence that patients with posterolateral scar do not
respond to CRT (32-34). This has been attributed to lack of efficient pacing as the LV lead is
placed over fibrotic tissue and was supported by the observation that lead location outside

16
scar tissue improved acute response to CRT in animals with LBBB and CX infarction (35).
However, a mathematical simulation study showed that the benefit of CRT was small in
patients with LV lateral wall scar, even when pacing in an optimal location (36). Thus,
absence of septal dysfunction as target for CRT, which implies less potential for improvement
of LV function by resynchronization, may also contribute to lack of response in patients with
posterolateral scars (14).
Clinical implications:
Currently, ECG is the only dyssynchrony parameter used routinely in the evaluation of
CRT candidates. The finding in the present study of apparently normal septal contraction
pattern in patients with LV lateral wall scar in spite of wide QRS and typical LBBB
morphology, implies that abnormal septal motion pattern has limited sensitivity for
identifying patients with electrical dyssynchrony. This, however, does not necessarily
represent a limitation of septal motion analysis to improve selection of patients for CRT. As
suggested by the insights provided by the present study, when heart failure patients with
LBBB do not have abnormal septal contraction pattern, one should search for scar in the LV
lateral wall. In addition, apparently normal septal contraction pattern implies that the potential
for improvement of LV function with CRT is less than in patients with abnormal septal
motion. Possibly, patients with LBBB and absence of septal flash should not receive CRT.
Whether this will be useful diagnostic approaches when evaluating patients for CRT, should
be further explored in future prospective studies.
Limitations:
The experimental part of the study was performed in an acute animal model during
general anesthesia and extensive instrumentation. Furthermore, the clinical part of the study

17
was cross-sectional with relatively small size of patient groups and acute ischemia in the
experimental study is different from post-infarct scar in the clinical study. In total, however,
the present investigation with a combined experimental and clinical design was well suited to
determine the role of LV lateral wall scar and function in generation of abnormal septal
contraction patterns in LBBB.
Conclusions:
The present study demonstrates that septal contraction pattern in LBBB is determined
by contractile function in the LV lateral wall. When patients with LBBB and wide QRS do
not have abnormal septal contraction pattern, one should search for scar in the LV lateral wall.
Therefore, evaluation of septal function may be important not only to use typical abnormal
contraction pattern to favor CRT, but also to use apparently normal septal contractions to raise
suspicion of LV lateral wall scar with less likelihood of good response to CRT. Future studies
should explore if these proposed strategies will provide added clinical value when selecting
patients for CRT.

18
Clinical perspectives:
Competency in Medical Knowledge: LV lateral wall function is an important
determinant of abnormal septal motion and reduced septal function in LBBB.
Competency in Patient Care and Procedural Skills: Patients with LBBB and apparent normal
septal motion should be examined for scar in the LV lateral wall.
Translational Outlook 1: There is need for prospective trials to evaluate whether LBBB
patients without septal flash should receive CRT.
Translational Outlook 2: Future studies should explore whether imaging has added value on
top of ECG for dyssynchrony assessment in CRT candidates.

19
References:
1. Cleland JG, Daubert JC, Erdmann E et al. The effect of cardiac resynchronization on
morbidity and mortality in heart failure. N Engl J Med 2005;352:1539-1549.
2. Ponikowski P, Voors AA, Anker SD et al. 2016 ESC Guidelines for the diagnosis and
treatment of acute and chronic heart failure: The Task Force for the diagnosis and
treatment of acute and chronic heart failure of the European Society of Cardiology
(ESC). Developed with the special contribution of the Heart Failure Association
(HFA) of the ESC. Eur J Heart Fail 2016;18:891-975.
3. De Boeck BW, Teske AJ, Meine M et al. Septal rebound stretch reflects the functional
substrate to cardiac resynchronization therapy and predicts volumetric and
neurohormonal response. Eur J Heart Fail 2009;11:863-871.
4. Parsai C, Bijnens B, Sutherland GR et al. Toward understanding response to cardiac
resynchronization therapy: left ventricular dyssynchrony is only one of multiple
mechanisms. Eur Heart J 2009;30:940-949.
5. Doltra A, Bijnens B, Tolosana JM et al. Mechanical abnormalities detected with
conventional echocardiography are associated with response and midterm survival in
CRT. JACC Cardiovasc Imaging 2014;7:969-979.
6. Risum N, Tayal B, Hansen TF et al. Identification of Typical Left Bundle Branch
Block Contraction by Strain Echocardiography Is Additive to Electrocardiography in
Prediction of Long-Term Outcome After Cardiac Resynchronization Therapy. J Am
Coll Cardiol 2015;66:631-641.
7. Stankovic I, Prinz C, Ciarka A et al. Relationship of visually assessed apical rocking
and septal flash to response and long-term survival following cardiac
resynchronization therapy (PREDICT-CRT). Eur Heart J Cardiovasc Imaging
2016;17:262-269.

20
8. Menet A, Bernard A, Tribouilloy C et al. Clinical significance of septal deformation
patterns in heart failure patients receiving cardiac resynchronization therapy. Eur
Heart J Cardiovasc Imaging 2016;0:1-10.
9. Sohal M, Amraoui S, Chen Z et al. Combined identification of septal flash and
absence of myocardial scar by cardiac magnetic resonance imaging improves
prediction of response to cardiac resynchronization therapy. J Interv Card
Electrophysiol 2014;40:179-190.
10. McDonald IG. Echocardiographic demonstration of abnormal motion of the
interventricular septum in left bundle branch block. Circulation 1973;48:272-280.
11. Prinzen FW, Hunter WC, Wyman BT, McVeigh ER. Mapping of regional myocardial
strain and work during ventricular pacing: Experimental study using magnetic
resonance imaging tagging. J Am Coll Cardiol 1999;33:1735-1742.
12. Gjesdal O, Remme EW, Opdahl A et al. Mechanisms of abnormal systolic motion of
the interventricular septum during left bundle-branch block. Circ Cardiovasc Imaging
2011;4:264-273.
13. De Boeck BW, Kirn B, Teske AJ et al. Three-dimensional mapping of mechanical
activation patterns, contractile dyssynchrony and dyscoordination by two-dimensional
strain echocardiography: rationale and design of a novel software toolbox. Cardiovasc
Ultrasound 2008;6:22.
14. Leenders GE, Lumens J, Cramer MJ et al. Septal Deformation Patterns Delineate
Mechanical Dyssynchrony and Regional Differences in Contractility Analysis of
Patient Data Using a Computer Model. Circ-Heart Fail 2012;5:87-96.
15. Corteville B, De Pooter J, De Backer T, El Haddad M, Stroobandt R, Timmermans F.
The electrocardiographic characteristics of septal flash in patients with left bundle
branch block. Europace 2017;19:103-109.

21
16. Urheim S, Edvardsen T, Torp H, Angelsen B, Smiseth OA. Myocardial strain by
Doppler echocardiography. Validation of a new method to quantify regional
myocardial function. Circulation 2000;102:1158-1164.
17. Opdahl A, Remme EW, Helle-Valle T et al. Determinants of left ventricular early-
diastolic lengthening velocity: independent contributions from left ventricular
relaxation, restoring forces, and lengthening load. Circulation 2009;119:2578-2586.
18. Lumens J, Tayal B, Walmsley J et al. Differentiating Electromechanical From Non-
Electrical Substrates of Mechanical Discoordination to Identify Responders to Cardiac
Resynchronization Therapy. Circ Cardiovasc Imaging 2015;8:e003744.
19. Strauss DG, Selvester RH, Wagner GS. Defining left bundle branch block in the era of
cardiac resynchronization therapy. Am J Cardiol 2011;107:927-934.
20. Russell K, Eriksen M, Aaberge L et al. A novel clinical method for quantification of
regional left ventricular pressure-strain loop area: a non-invasive index of myocardial
work. Eur Heart J 2012;33:724-733.
21. Engblom H, Tufvesson J, Jablonowski R et al. A new automatic algorithm for
quantification of myocardial infarction imaged by late gadolinium enhancement
cardiovascular magnetic resonance: experimental validation and comparison to expert
delineations in multi-center, multi-vendor patient data. J Cardiovasc Magn Reson
2016;18:27.
22. Cerqueira MD, Weissman NJ, Dilsizian V et al. Standardized myocardial
segmentation and nomenclature for tomographic imaging of the heart: A statement for
healthcare professionals from the Cardiac Imaging Committee of the Council on
Clinical Cardiology of the American Heart Association. J Am Soc Echocardiog
2002;15:463-467.

22
23. Dillon JC, Chang S, Feigenbaum H. Echocardiographic manifestations of left bundle
branch block. Circulation 1974;49:876-880.
24. Little WC, Reeves RC, Arciniegas J, Katholi RE, Rogers EW. Mechanism of
abnormal interventricular septal motion during delayed left ventricular activation.
Circulation 1982;65:1486-1491.
25. Kingma I, Tyberg JV, Smith ER. Effects of diastolic transseptal pressure gradient on
ventricular septal position and motion. Circulation 1983;68:1304-1314.
26. Remme EW, Niederer S, Gjesdal O et al. Factors determining the magnitude of the
pre-ejection leftward septal motion in left bundle branch block. Europace
2015;18:1905-1913.
27. Walmsley J, Huntjens PR, Prinzen FW, Delhaas T, Lumens J. Septal flash and septal
rebound stretch have different underlying mechanisms. Am J Physiol-Heart C
2016;310:H394-H403.
28. Aalen J, Storsten P, Remme EW et al. Afterload Hypersensitivity in Patients With Left
Bundle Branch Block. JACC Cardiovasc Imaging 2018.
29. Lyseggen E, Skulstad H, Helle-Valle T et al. Myocardial strain analysis in acute
coronary occlusion: a tool to assess myocardial viability and reperfusion. Circulation
2005;112:3901-3910.
30. Lyseggen E, Rabben SI, Skulstad H, Urheim S, Risoe C, Smiseth OA. Myocardial
acceleration during isovolumic contraction: relationship to contractility. Circulation
2005;111:1362-1369.
31. Hopp E, Lunde K, Solheim S et al. Regional myocardial function after intracoronary
bone marrow cell injection in reperfused anterior wall infarction - a cardiovascular
magnetic resonance tagging study. J Cardiovasc Magn Reson 2011;13:22.

23
32. Bleeker GB, Kaandorp TA, Lamb HJ et al. Effect of posterolateral scar tissue on
clinical and echocardiographic improvement after cardiac resynchronization therapy.
Circulation 2006;113:969-976.
33. Steelant B, Stankovic I, Roijakkers I et al. The Impact of Infarct Location and Extent
on LV Motion Patterns: Implications for Dyssynchrony Assessment. JACC
Cardiovasc Imaging 2016;9:655-664.
34. Chalil S, Stegemann B, Muhyaldeen SA et al. Effect of posterolateral left ventricular
scar on mortality and morbidity following cardiac resynchronization therapy. Pacing
Clin Electrophysiol 2007;30:1201-1209.
35. Rademakers LM, van Kerckhoven R, van Deursen CJ et al. Myocardial infarction does
not preclude electrical and hemodynamic benefits of cardiac resynchronization therapy
in dyssynchronous canine hearts. Circ Arrhythm Electrophysiol 2010;3:361-368.
36. Huntjens PR, Walmsley J, Ploux S et al. Influence of left ventricular lead position
relative to scar location on response to cardiac resynchronization therapy: a model
study. Europace 2014;16:iv62-iv68.

24
Figure legends:
Figure 1. Septal deformation during left bundle branch block
Experimental study: Pressure and septal strain traces after induction of LBBB in a
representative animal. AVC=aortic valve closure; AVO=aortic valve opening;
ECG=electrocardiogram; LBBB=left bundle branch block; LV=left ventricular; LA=left
atrial; MVC=mitral valve closure; MVO=mitral valve opening.
Figure 2. Determinants of abnormal septal motion in left bundle branch block
Upper panels: Strain traces from representative animal during LBBB (left), LBBB with CX
occlusion (middle) and LBBB with LAD occlusion (right). Please note how septal rebound
stretch is lost and septal systolic shortening markedly improved with LV lateral wall
ischemia.
Lower panels: Strain traces and LGE-CMR images from representative LBBB patients (left:
non-ischemic cardiomyopathy; middle: LV lateral wall scar; and right: anteroseptal scar).
Similar to the experimental study, there is no rebound stretch and instead markedly improved
septal deformation in the patient with LV lateral wall scar, whereas septal rebound stretch is
present in the patient with anteroseptal scar.
AVC=aortic valve closure; CX=circumflex coronary artery; LAD=left anterior descending
coronary artery; LBBB=left bundle branch block; LGE-CMR=late gadolinium-enhanced
cardiac magnetic resonance; LV=left ventricular.
Figure 3. Effect of left ventricular lateral wall ischemia on septal flash
Upper panels: Parasternal M-mode images from representative animal during normal
conduction (left), LBBB (middle) and LBBB with CX occlusion (right). Please note how

25
septal flash is abolished with LV lateral wall ischemia due to loss of paradoxical rightward
septal motion.
Lower panels: Strain traces from representative animal during normal conduction (left),
LBBB (middle) and LBBB with CX occlusion (right). Similar to the paradoxical rightward
septal motion, septal rebound stretch (arrow) is lost with LV lateral wall ischemia and septal
systolic shortening restored to similar levels as normal conduction.
AVC=aortic valve closure; CX=circumflex coronary artery; LBBB=left bundle branch block;
LV=left ventricular.
Figure 4. Stepwise reduction in left ventricular lateral wall contractility during left
bundle branch block
Strain traces from representative animal before (left panel) and during increasing LV lateral
wall ischemia (right panels). The gradual loss of contractility in the LV lateral wall is closely
followed by decrease in septal rebound stretch and increase in septal systolic shortening.
AVC=aortic valve closure; LBBB=left bundle branch block; LV=left ventricular.
Figure 5. Septal pump function during left bundle branch block and left ventricular
lateral wall ischemia
A) Experimental study: Representative pressure-segment length loops from a dog after
induction of LBBB. The area of the loops reflects myocardial work where positive work is
performed during counter-clockwise rotation (segmental shortening) and negative work
during clockwise rotation (segmental lengthening). Please note how septal systolic function
improves markedly during LV lateral wall ischemia as the loop rotates counterclockwise
during systole and performs a large positive work.

26
B) Clinical study: Representative pressure-strain loops from two LBBB patients (to the left
patient with non-ischemic cardiomyopathy and to the right patient with LV lateral wall scar).
The loops resemble the experimental observations in A).
LBBB=left bundle branch block; LV=left ventricular.
Figure 6. Septal versus left ventricular lateral wall shortening in left bundle branch
block
Upper panel: Experimental study. During LBBB there is reduced septal and maintained LV
lateral wall systolic shortening. With LV lateral wall ischemia, however, the negative impact
from the LV lateral wall on the septum is removed and septal shortening improves markedly.
Lower panel: Clinical study. The findings in patients with non-ischemic cardiomyopathy as
compared to patients with LV lateral wall scar, resemble those from the experimental study.
LBBB=left bundle branch block; LV=left ventricular.
Supplemental video. Negative crosstalk between septum and left ventricular lateral wall
in left bundle branch block
The video displays beat-to-beat changes in septal and LV lateral wall pressure-segment length
loops in a representative animal immediately after onset of CX occlusion. The negative
impact of the LV lateral wall on the septum is removed as the LV lateral wall becomes
increasingly ischemic and allows the septal loop to perform predominantly positive work.
CX=circumflex coronary artery; LBBB=left bundle branch block; LV=left ventricular.
27
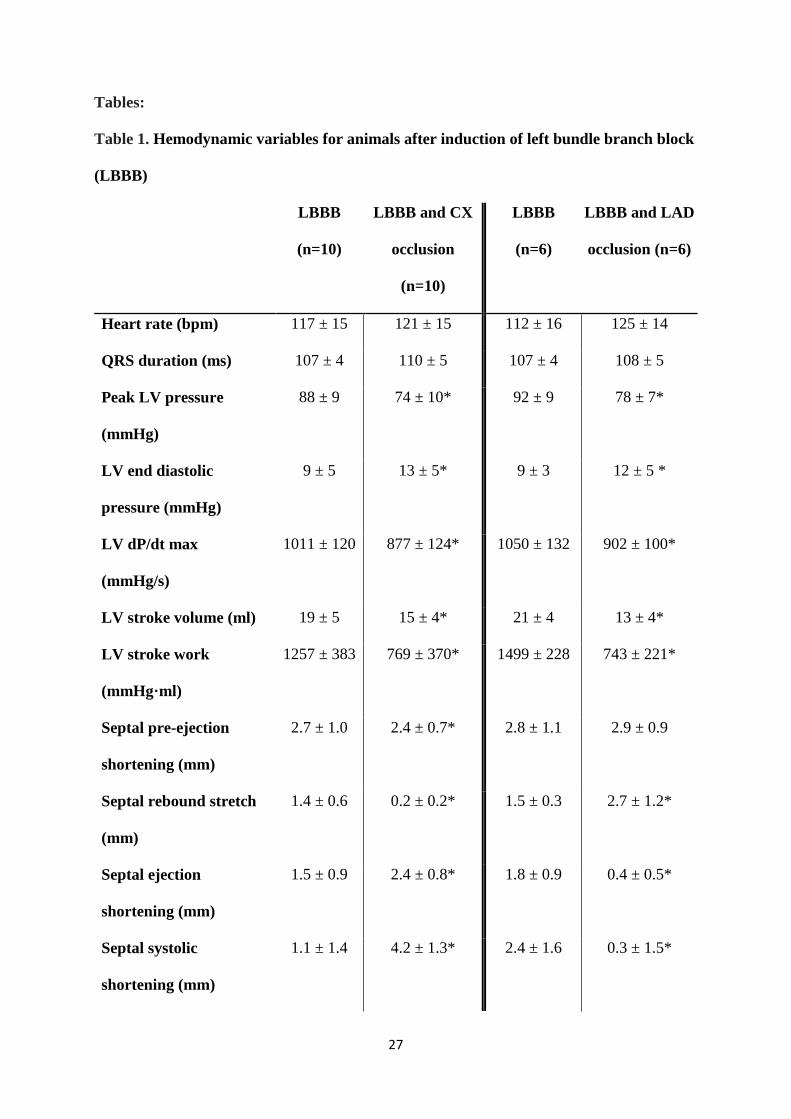
Tables:
Table 1. Hemodynamic variables for animals after induction of left bundle branch block
(LBBB)
LBBB
(n=10)
LBBB and CX
occlusion
(n=10)
LBBB
(n=6)
LBBB and LAD
occlusion (n=6)
Heart rate (bpm) 117 ± 15 121 ± 15 112 ± 16 125 ± 14
QRS duration (ms) 107 ± 4 110 ± 5 107 ± 4 108 ± 5
Peak LV pressure
(mmHg)
88 ± 9 74 ± 10* 92 ± 9 78 ± 7*
LV end diastolic
pressure (mmHg)
9 ± 5 13 ± 5* 9 ± 3 12 ± 5 *
LV dP/dt max
(mmHg/s)
1011 ± 120 877 ± 124* 1050 ± 132 902 ± 100*
LV stroke volume (ml) 19 ± 5 15 ± 4* 21 ± 4 13 ± 4*
LV stroke work
(mmHg·ml)
1257 ± 383 769 ± 370* 1499 ± 228 743 ± 221*
Septal pre-ejection
shortening (mm)
2.7 ± 1.0 2.4 ± 0.7* 2.8 ± 1.1 2.9 ± 0.9
Septal rebound stretch
(mm)
1.4 ± 0.6 0.2 ± 0.2* 1.5 ± 0.3 2.7 ± 1.2*
Septal ejection
shortening (mm)
1.5 ± 0.9 2.4 ± 0.8* 1.8 ± 0.9 0.4 ± 0.5*
Septal systolic
shortening (mm)
1.1 ± 1.4 4.2 ± 1.3* 2.4 ± 1.6 0.3 ± 1.5*

28
Values are mean ± standard deviation. Segmental data are circumferential. *p<0.05 vs.
LBBB.
CX=circumflex coronary artery; LAD=left anterior descending coronary artery; LBBB=left
bundle branch block; LV=left ventricular.
LV lateral wall pre-
ejection lengthening
(mm)
1.2 ± 0.7 0.8 ± 0.6* 1.1 1.2 ± 0.6 1.1 ± 0.6
LV lateral wall systolic
shortening (mm)
5.0 ± 1.2 0.5 ± 1.0* 4.9 ± 1.2 4.2 ± 1.1
Systolic stretch index
(%)
8.8 ± 3.4 3.5 ± 1.8* 9.6 ± 2.5 12.0 ± 5.6
Septal work
(mmHg·mm)
5 ± 62 108 ± 47* 29 ± 70 -96 ± 72*
LV lateral wall work
(mmHg·mm)
417 ± 84 74 ± 65* 437 ± 98 310 ± 98*

29
Table 2. Characteristics of left bundle branch block (LBBB) patients
Non-ischemic (n=20) Ischemic (n=20)
Posterolateral
scar (n=10)
Anteroseptal
scar (n=10)
Age (years) 65 ± 11 67 ± 6 70 ± 5
Male gender (n) 9 10 8
Height (cm) 169 ± 10 176 ± 8 172 ± 6
Weight (kg) 75 ± 16 87 ± 21 79 ± 20
Heart rate (bpm) 68 ± 11 56 ± 10* 62 ± 8
Systolic blood pressure
(mmHg)
137 ± 25 126 ± 18 123 ± 19
Diastolic blood pressure
(mmHg)
75 ± 12 70 ± 15 63 ± 8*
NYHA class 2.4 ± 0.7 2.6 ± 0.5 2.4 ± 0.7
Medication (n)
ACE-inhibitor/ARB
Beta blocker
Aldosterone antagonists
Loop diuretics
20
19
10
12
9
10
5
6
10
8
4
8
Sinus rhythm (n) 20 10 10
LBBB (n) 20 10 10
QRS duration (ms) 165 ± 16 162 ± 19 167 ± 17

30
Table 2. Characteristics of LBBB patients (continued)
Non-ischemic (n=20) Ischemic (n=20)
Posterolateral
scar (n=10)
Anteroseptal
scar (n=10)
Dimensions end diastole (mm)
Septum
LV internal diameter
LV posterior wall
10 ± 2
63 ± 8
9 ± 2
11 ± 1
71 ± 6*
9 ± 2
9 ± 1
70 ± 11
8 ± 1
LV end diastolic volume (ml) 218 ± 79 313 ± 74* 247 ± 86
LV end systolic volume (ml) 153 ± 65 220 ± 66* 177 ± 67
LV ejection fraction (%) 31 ± 5 31 ± 6 28 ± 6
Global longitudinal shortening
(%)
10.4 ± 2.4 10.4 ± 1.7 8.0 ± 2.4*
Septal pre-ejection shortening
(%)
5.4 ± 1.9 3.8 ± 1.8 5.2 ± 3.3
Septal rebound stretch (%)Ɨ 2.6 ± 2.9 (1.8) 0.0 ± 0.0 (0.0)* 3.2 ± 3.6 (1.7)
Septal ejection shortening (%) 2.3 ± 2.7 9.5 ± 3.8* 2.5 ± 2.5
Septal systolic shortening (%) 2.2 ± 3.5 10.7 ± 4.4* 3.0 ± 3.4
LV lateral wall pre-ejection
lengthening (%)
3.3 ± 2.0 1.5 ± 1.1* 2.4 ± 1.8
LV lateral wall systolic
shortening (%)
12.3 ± 3.6 3.6 ± 1.9* 12.9 ± 4.1
Systolic stretch index (%) 9.0 ± 3.1 4.1 ± 3.6* 7.2 ± 4.3
Septal work (mmHg·%) 7 ± 377 754 ± 453* 46 ± 506

31
Values are mean ± standard deviation. *p<0.025 vs. non-ischemic. ƗDue to lack of normality
and heterogeneity of variance, a Mann-Whitney test was performed and median values given
in brackets for septal rebound stretch.
ACE-inhibitor=angiotensin-converting enzyme inhibitor; ARB=angiotensin II receptor
blocker; LBBB=left bundle branch block; LV=left ventricular; NYHA class=new york heart
association functional classification.
LV lateral wall work
(mmHg·%)
1552 ± 784 512 ± 468* 1048 ± 697

32
Figure 1

33
Figure 2

34
Figure 3
Figure 4
35
Figure 5A
Figure 5B

36
Figure 6







