
National Nutrition Situation, Policies, Priorities and Programs
Dr. Shyam Raj UpretiChild Health DivisionDepartment of Health Services

NHSP II(Impact Indicators)
NFHS 1996 NDHS 2006
MMMS 2008
Lancet 2010
WHO 2012 MDG 20150
100
200
300
400
500
600539
281229 240
170134
Maternal Mortality Ratio(per 100,000 live births)
U5MR IMR NMR0
20
40
60
80
100
120
140
160139
93
58
91
64
38
6148
33
5446
3338 32
16
U5MR, IMR and NMR Trend
NFHS 1996 NDHS 2001 NDHS 2006 NDHS 2011 MDG 2015

NHSP II
OUTCOME INDICATORSTARGET
2010 2013 2015% of diarrhea cases among under -5 children treated with zinc (and ORS)
7% 25% 40%
% of children exclusively breastfed in the first 6 months 35% 48% 60%
% Vit A coverage maintained for children aged6 -59 months 90% 90% 90%
% of low birth weight (or small) babies 32% 27% 25%

NDHS 2001 NDHS 2006 NDHS 2011 MDG 20150
10
20
30
40
50
60 57
49
41
28
43 39
29
27
11 13 11
5
Stunting Underweight Wasting
Changes in nutritional status of children under 5 years of age
Source: NDHS 2011

Stunting by Sub-region
Percent of children under age 5 who are too short for
their age (based on WHO standards)
Eastern terai31%
Central terai41%
Western mountain 60%
Mid-western terai 44%
Far-westernhill 58%
Eastern hill 46%
Centralhill 31%
Western hill 36%
Mid-western hill 52%
Far-western terai32%
Western terai 40%
Central mountain 46%
Eastern mountain 45%
41%

Disparity by wealth quintile exists….
Fig 24: Stunting (-2SD) Trend for children between 6-23 months, by Wealth Index
0%
10%
20%
30%
40%
50%
60%
1996 2001 2006
Poorest
P oorer
Middle
Richer
Richest
Total
65% reduction in richest quintile!
12% increase in poorest quintile!
14% reduction overall
High Inequity
Ref: DHS 2001 and 2006. Adapted from Ramu Bishwakarma. Social Inequalities in Child Nutrition in Nepal. August 2009 (Background paper for Nepal Nutrition Assessment and Gap Analysis, November 2009)

Sustained High Vitamin A Supplementation and De-worming to Children (Focus needed: 6-11 months - 55% and Urban below 80%)

Mid Western
Hill
Far Western
Hill
Eastern Terai
Central Terai
Western Terai
Mid Western
Terai
Far Western
Terai
0
10
20
30
40
50
60
70
80
90
100
68.1
42.8
82.9 83.9
92.3
63.2 65.5
Percentage with adequately iodized salt
Percentage with adequately iodized salt
Perc
ent
Iodized salt social marketing campaign will be planned for expansion in a phase wise manner to the districts having low consumption of adequately iodized salt

NMSS 1998
NDHS 2006
NDHS 2011
Urban
Rural
Easte
rn M
ountain
Centra
l Mountai
n
West
ern M
ountain
Easte
rn Hill
Centra
l Hill
West
ern Hill
Mid-west
ern Hill
Far-w
estern
Hill
Easte
rn Te
rai
Centra
l Tera
i
West
ern Te
rai
Mid-west
ern Te
rai
Far-w
estern
Terai
0
10
20
30
40
50
60
70
8078
48 46.2
41.2
46.7
51.3
33.1
52.7
42.340.2
43.6
36
40.9
49.546.7
48.8
56.960.4
Prevalence of anaemia in 6-59 months children
Axis Title
NDHS 2011
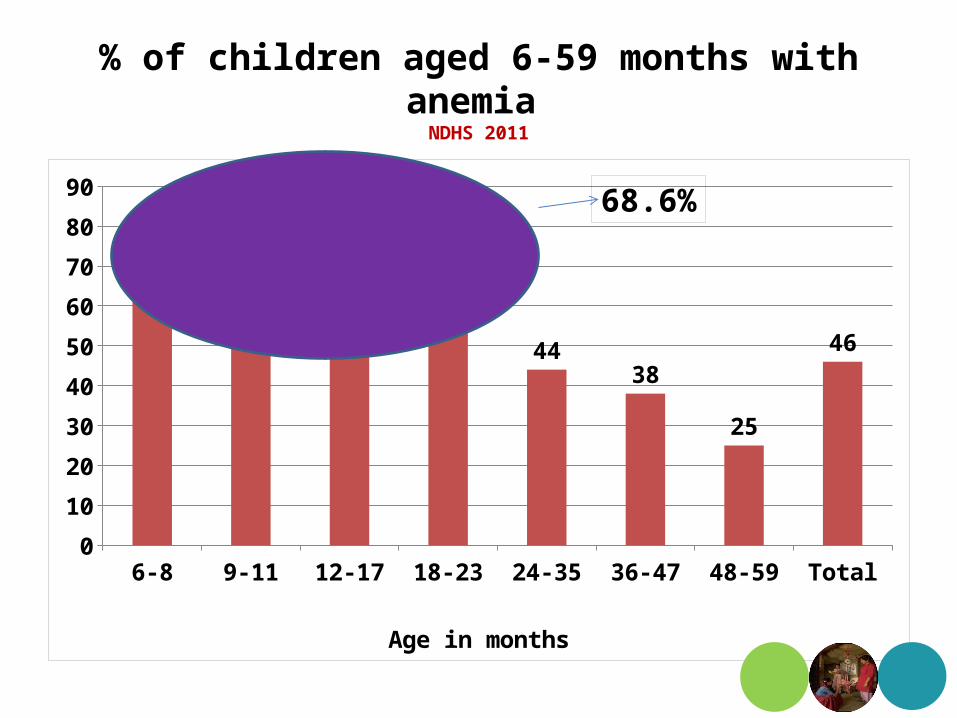
% of children aged 6-59 months with anemia NDHS 2011
6-8 9-11 12-17 18-23 24-35 36-47 48-59 Total0
10
20
30
40
50
60
70
80
9078
74 72
57
4438
25
46
Age in months
68.6%

IYCF practices among 6-23 months children
National EDR CDR WDR MWDR FWDR0
20
40
60
80
100
120
24 29.117.9
33.3
1925.7
76 70.982.1
66.7
8174.3
IYCF 3 practices Series2

0-1 months 2-3 months 4-5 months 0-5 months0
10
20
30
40
50
60
70
80
90
100
88
74
53
70
Exclusive breastfeeding by age
NFHS 1996 NDHS 2001 NDHS 2006 NDHS 20110
5
10
15
20
25
30
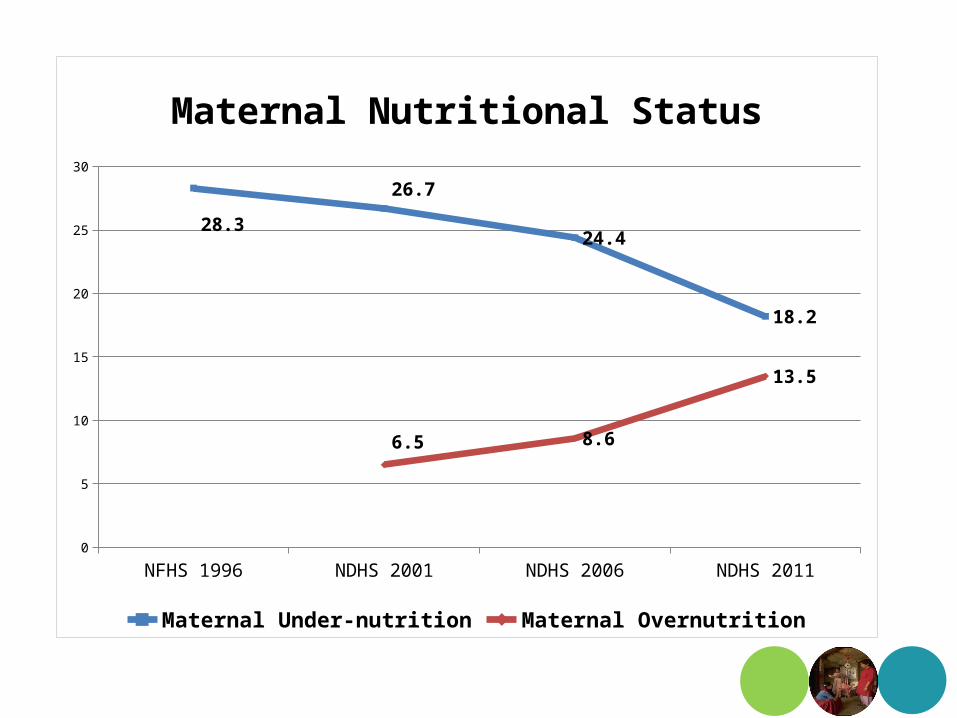
28.3
26.7
24.4
18.2
6.5 8.6
13.5
Maternal Nutritional Status
Maternal Under-nutrition Maternal Overnutrition
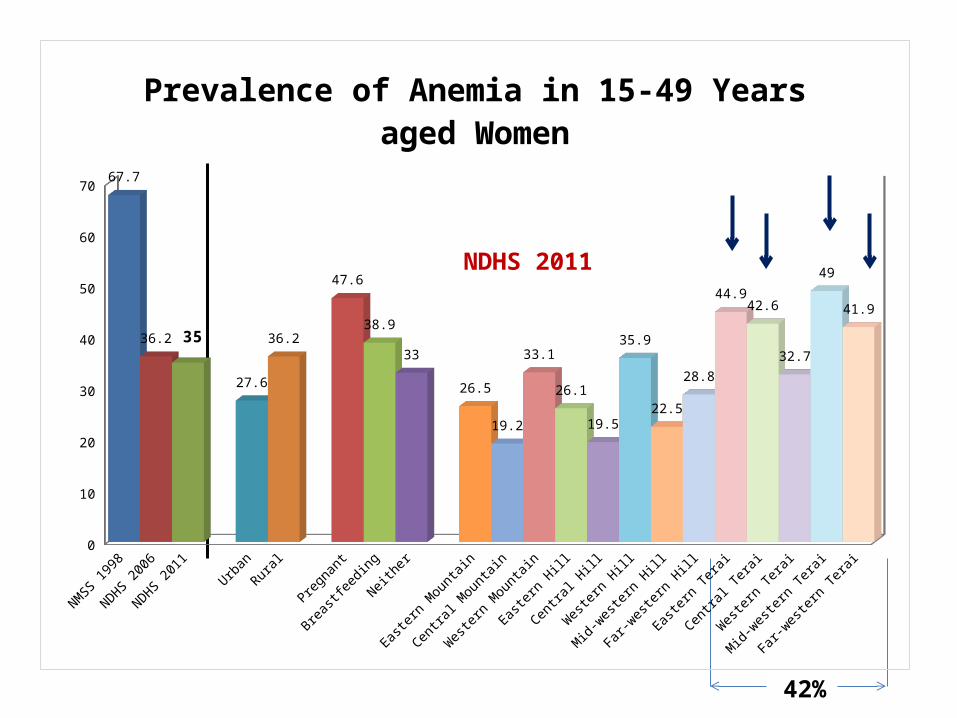
NDHS 2011
42%
NMSS 1998
NDHS 2006
NDHS 2011
Urban
Rural
Pregnan
t
Breastf
eeding
Neither
Easte
rn M
ountain
Centra
l Mountai
n
West
ern M
ountain
Easte
rn Hill
Centra
l Hill
West
ern Hill
Mid-west
ern Hill
Far-w
estern
Hill
Easte
rn Te
rai
Centra
l Tera
i
West
ern Te
rai
Mid-west
ern Te
rai
Far-w
estern
Terai
0
10
20
30
40
50
60
70 67.7
36.2 35
27.6
36.2
47.6
38.9
33
26.5
19.2
33.1
26.1
19.5
35.9
22.5
28.8
44.942.6
32.7
49
41.9
Prevalence of Anemia in 15-49 Years aged Women

National Nutrition PolicyOverall Objective:• To reduce child and maternal mortality through nutritional interventions
Specific Objectives:• Reduce general malnutrition among children and women, i.e. stunting,
underweight, wasting, low BMI• Reduce Iron Deficiency Anemia among children, children under age 2
year and pregnant women• Maintain and sustain Iodine Deficiency Disorders and Vitamin A
Deficiency control activities.• Improve maternal nutrition• Align with multi-sectoral nutrition initiative.• Improve Nutrition related behavior change and communication• Improve Monitoring of Nutrition related programs/activities

National Nutrition Strategy• Protect, promote and support optimal feeding practice of children
through IYCF scale up, increasing coverage of GM• Expansion of Community Management of Acute Malnutrition linked to
expansion of Nutrition Rehabilitation Homes• Reduce IDA through
– iron tablet supplementation to pregnant, adolescents– MNPs distribution liked to IYCF to children under 2 years – Deworming (Preschool, school and pregnant) and flour fortification
• Increase accessibility and Social Marketing of 2-Child Logo iodized packet salt
• Bi-annual mass supplementation of VA to under 5 years children• Gradual expansion of the School Health and Nutrition activities in all
districts • BCC for changing dietary practices for improved maternal and child
nutrition practices

Nutrition InterventionsNationwide
1. Growth Monitoring and counseling
2. Prevention and control of Iron Deficiency Anemia (IDA)
3. Prevention, Control and Treatment of Vitamin A deficiency (VAD)
4. Prevention of Iodine Deficiency Disorders (IDD)
5. Control of Parasitic Infestation by deworming
6. Emergency Nutrition
At scale
1. Infant and Young Child Feeding (IYCF)
2. Community Management of Acute Malnutrition (CMAM)
3. Micronutrient Powder (MNP) distribution link with IYCF
4. School Health and Nutrition Program – 14 districts+15 district under process in this FY
Piloting / small scale
1. Maternal and Child Health Care (MCHC) Program – 9 districts
2. Food supplementation
3. Vitamin A Supplementation to address the low coverage in 6-11 months children (Jumla, Chitwan & Kavre)
4. Piloting New Growth Chart (Rukum)
5. Multi-sectoral Nutrition Plan (MSNP) – (6 Districts: Bajura, Achham, Jumla, Nawalparasi , Kapilvastu & Parsa)

Nutrition Problem Current StatusGeneral Malnutrition among children under 5 years of age (Macronutrients)
Underweight - “On track” Stunting and Wasting – “Not on track”
Inequity in increasing
Vitamin A Deficiency No longer a public health problem Iodine Deficiency Disorders
“On track” (MDG Target-90%)(80% HHs Consuming adequately Iodized Salt)
Iron Deficiency Anaemia “On track”
Current Progress in Nutrition
Children 6-59 months Children 6-23 months Women 15-49 years0
10
20
30
40
50
60
70
80
90
7875
4842
46.2
68.6
36
NMSS 1998 NDHS 2006 NDHS 2011

New Initiatives
• Multi-sectoral Nutrition Plan has recently been approved by the Council of Ministers
• Strategy for IYCF, Maternal Nutrition and detailed Communication Plan for MIYCF is under development process
• Priorities programmes such as IYCF, MNP, CMAM and NRH are gradually being scaled up in different districts
• MCHC Programme review (national as well as regional) has been carried out.

Issues and Challenges
Sustained and predictable financing for scaling up priority programmes viz. IYCF, CMAM etc.
Institutional strengthening for nutrition and capacity building of HWs including management capacity at central level
Sluggish procurement process for commodities and services Weak monitoring and supervision at all levels with poor use of
available data Good progress of micronutrient deficiency control program but
maintenance and sustainability is a challenge Implementation of nutrition activities through multi-sectoral
approach
Future Priorities in Nutrition • Sustained financing for program scale-up, i.e. Infant and
Young Child Feeding Counseling (IYCF), Multiple Micronutrient Powders (MNPs) distribution linked with IYCF, Community Management of Acute Malnutrition (CMAM)
• Impact assessment of targeted food supplementation and cash grant
• Support to maintain and sustain micronutrients deficiency control programs (IDA, IDD, VAD)
• Institutional strengthening of nutrition program with institutional arrangements and capacity building of community health workers and volunteers in nutrition
• Technical and financial support to implement multi-sectoral nutrition interventions.

Thank you







