Download - Neonatal Diseases

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 1/98
Neonatal Diseases
RC 290

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 2/98
Respiratory Distress
Syndrome
(RDS)
Also known as Hyaline MembraneDisease
(HMD)

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 3/98
Occurrence
1-2% of all births
10% of all premature births
Greatest occurrence is in the premature and low birth weight infant

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 4/98
Etiology & Predisposing Factors
Prematurity
Immature lung architecture and surfactantdeficiency
Fetal asphyxia & hypoxia
Maternal diabetes
Increased chance of premature birth
Possible periods of reflex hypoglycemia in thefetus causing impaired surfactant production

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 5/98
Pathophysiology
Surfactant deficiency
Decreased FRC
Atelectasis
Increased R-L shunt
Increased W.O.B.
Hypoxemia and
eventuallyhypercapnia becauseof V/Q mismatch

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 6/98
Pathophysiology (cont .)
Atelectasis keeps PVR
high
Increased PAP
Lung hypoperfusion
R-L shunting may re-
occur across the
Ductus Arteriosus andthe Foramen Ovale

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 7/98

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 8/98
The cycle continues until
surfactant levels are adequate to
stabilize the lung
Symptoms usually appear 2-6 hours after
birth
Why not immediately?
Disease peaks at 48-72 hours
Recovery usually occurs 5-7 days after birth

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 9/98
Clinical findings: Physical
Tachypnea
(60 BPM or >)
Retractions
Nasal flaring
Expiratory grunting
Helps generate
autoPEEP
Decreased breath
sounds with crackles
Cyanosis on room air
Hypothermia
Hypotension

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 10/98
Clinical Findings: Lab
ABGs: initially respiratory alkalosis and
hypoxemia that progresses to profound
hypoxemia and combined acidosisIncreased Bilirubin
Hypoglycemia
Possibly decreased hematocrit

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 11/98
CXR: Normal
8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 12/98
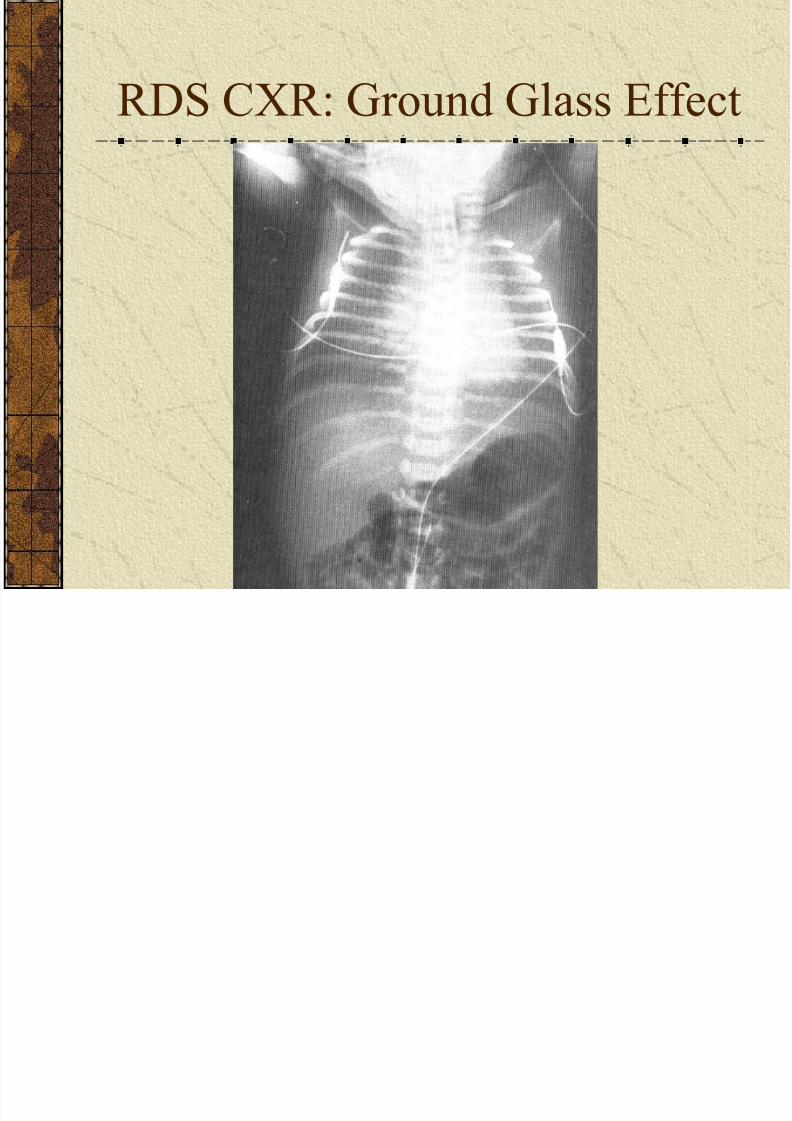
RDS CXR: Ground Glass Effect

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 13/98
RDS CXR: Air Bronchograms &
Hilar Densities

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 14/98
Time constant is decreased
since elastic resistance is so
high
Increased elastic resistance means
decreased compliance!

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 15/98
RDS Treatment: Primarily
supportive until lung stabilizes
NTE, maintain perfusion, maintainventilation and oxygenation
O2 therapy, CPAP or mechanicalventilation
May require inverse I:E ratios if oxygenationcan not be achieved with normal I:E ratio
Surfactant instillation!!!May cause a sudden drop in elastic resistance!

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 16/98
Prognosis/Complications
Prognosis is good once infant makes it past
the peak (48-72 hours)
Complications possible are:Intracranial Bleed
BPD (Bronchopulmonary Dysplasia)
PDA (Patent Ductus Arteriosus)

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 17/98
Transient Tachypnea of the
Newborn (TTN)
Also known as Type II RDS or
Retained Lung Fluid

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 18/98
Occurrence: Similar to
RDS
More common in term infants!

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 19/98
Etiology & Predisposing Factors
C-section
These infants do not have the fluid expelled
from their airways as occurs in vaginal delivery
Maternal Diabetes
Increased chance of C-section due to LGA
Cord CompressionAnesthesia

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 20/98
TTN Pathophysiology
Primary problem = retained lung fluid
Fluid not expelled from airways because of C-section
Poor absorption of remaining fluid by pulmonarycapillaries and lymphatics
If retained fluid is in interstitial spaces,compliance and TC are decreased
If retained fluid is in airways,airway resistanceand TC are increased
TTN can be restrictive , obstructive, or both!
Fluid usually clears by itself after 24-48 hoursafter birth

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 21/98
Clinical Signs
Tachypnea (usually rate is greater than seen
in RDS)
Minimal (if any) nasal flaring or expiratorygrunting
ABG’s: mild hypoxemia. PaCO2 depends
on whether problem is restrictive orobstructive

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 22/98
TTN CXR
Coarse peri-hilar streaks
Prominent lung vasculature
Flattened diaphragms if fluid is causingobstruction/air-trapping

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 23/98
TTN Treatment: Like RDS, it is
primarily supportive
Monitoring and O2 therapy
Possibly CPAP or mechanical ventilation

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 24/98
Prognosis/Complications
Prognosis is very good
Main complication is pneumonia
Often initial diagnosis

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 25/98

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 26/98
Patent Ductus Arteriosus
-PDA_
Failure of the D.A. to close at birth or
a re-opening of the D.A. after birth.
Allows shunting between the
pulmonary artery and the aorta

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 27/98
Occurrence
1 per 2000 term babies
30-50% of RDS babies

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 28/98
Etiology & Predisposing Factors
Prematurity
D.A. not as sensitive to increasing PaO2
Hypoxia
Decreasing PaO2 allows it to re-open for up to three
weeks after birth
Thus, a PDA can occur in a premature infant whois NOT hypoxic or in a term baby who is hypoxic
Worst case is a premature infant who is hypoxic!

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 29/98
Pathophysiology
D.A. fails to close or it re-opens
Then shunting occurs between the pulmonary artery and the aorta
The direction of the shunt depends on whichvessel has the higher pressure
A PDA can cause L-R shunting or R-L
shunting!Clinically, most PDA’s refer to a L-R shunt

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 30/98
Clinical Signs
Tachypnea, bounding pulses, hyperactive
pre-cordium
Decreased breath sounds and possibly somecrackles
Possible murmur over left sternal border
Murmur is loudest when D.A. just startsopening or when it is almost closed

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 31/98
Clinical Signs (cont .)
ABGs – hypoxemia with respiratory acidosis
If R-L shunting, the PaO2 in the upper extremities,ie pre-ductal, will be greater than the PaO2 in the
umbilical artery, ie post-ductal!TC – decreased if L-R shunting causes pulmonaryedema; increased if fluid spills into airways andincreases airway resistance
CXR –
if L-R shunt, butterfly pattern of pulmonaryedema with possible cardiomegaly

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 32/98
PDA Treatment
Basic – NTE, O2, may require CMV if not already
on the ventilator
Medical
L-R shunt that fails to close: Indomethacin (Indocin)
R-L shunt: Priscoline (Tolazoline) to decrease PVR;
also nitric oxide
Surgical – if medical treatment fails, the PDA may be surgically ligated

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 33/98
8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 34/98
Meconium Aspiration
Syndrome
-MAS-
Syndrome of respiratory distress that
occurs when meconium is aspirated prior to or during birth

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 35/98
Occurrence
10-20% of ALL births show meconium
staining
10-50% of stained babies may be symptomatic
More common in term and post-term babies

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 36/98
Etiology & Predisposing Factors
Intra-uterine hypoxic or asphyxic episode
Post-term
Cord compression
h h i l h k l

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 37/98
Pathophysiology: Check Valve
Effect
Causes gas trapping
(obstruction)
If complete obstruction, theneventually atelectasis occurs
Irritating to airways, so edema
and bronchospasm
Good culture ground for
bacteria, so pneumonia
possible

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 38/98
Pathophysiology (cont .)
V/Q mismatch leads to hypoxia and
acidosis which increases PVR
TC increases because it increases airwayresistance
Meconium is usually absorbed in 24-48
hours; there are still many possiblecomplications
8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 39/98
Clinical Signs
Respiratory depression
or distress at birth
Hyperinflation
Pallor
Meconium stained
body
Possible cyanosis on roomair
Moist crackles
ABGs – hypoxemia withcombined acidosis
CXR – coarse, patchyinfiltrates with areas ofatelectasis and areas of
hyperinflationMay see flatteneddiaphragms if obstruction issevere

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 40/98
M.A.S. Treatment
Amnioinfusion – artificialamniotic fluid infused intouterus to dilute meconium
Proper resuscitation at
birth(clear meconiumfrom trachea beforestimulating respiration)
Oro-gastric tube
NTEO2
NaHCO3 if severe metabolicacidosis
Broad spectrum antibiotics
Bronchial hygiene
May need mechanicalventilation
Slow rates and wide I:Eratios because of increasedTC
Low level of PEEP mayhelp prevent check valveeffect
May need HFO

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 41/98
Prognosis & Complications
Good prognosis if there are no complications
Complications:Pneumonia
Pulmonary baro/volutrauma
Persistent Pulmonary Hypertension (PPHN)

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 42/98
Persistent Pulmonary Hypertension
-PPHN-
Also known as Persistent Fetal
Circulation-PFC-

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 43/98
Failure to make the
transition from fetal to
neonatal circulation or a
reversion back to the
condition where pulmonaryartery pressure exceeds
aortic pressure
Results in R-L shunting across the
D.A. and the Foramen Ovale

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 44/98

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 45/98
Etiology & Predisposing Factors
M.A.S – most common
Hypoxia and /or acidosis, eg RDS
Any condition that causes PVR to increase

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 46/98
Pathophysiology
Primary problem is pulmonary artery hypertension
Infants arterial walls are thicker and they are more prone to vasospasm
If pulmonary artery pressure gets high enough, blood will shunt R-L across the D.A. and ForamenOvale
Remember, conditions that drive up PAP usually makethe D.A. open
Lung is hypoperfused resulting in refractoryhypoxemia and hypercapnia

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 47/98
Clinical Signs
Refractory hypoxemia and cyanosis
Shock and tachypnea
Murmur possiblePre-ductal PaO2 > post-ductal PaO2
Hypoxemia with combined acidosis
CXR usually OK when compared to infantscondition

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 48/98

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 49/98
Prognosis & Complications
Prognosis depends on how well infant
responds to treatment
ComplicationsShock
Intracranial bleed
Internal bleedingEspecially a problem if Priscoline is used

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 50/98
Wilson – Mikity Syndrome
- Pulmonary Dysmaturity-Respiratory distress that develops
after the first week of life and
presents with definite CXR changes

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 51/98
Occurrence
Usually in <36 weeks gestational age and
birth weight <1500 grams
After first week of life No prior symptoms

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 52/98
Etiology & Predisposing Factors
Exact etiology unknown
Appears to be due to immature lung and
airways trying to function Not due to O2 toxicity or mechanical
ventilation!
8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 53/98
Pathology
Immature alveoli and T-B tree causes V/Q
mismatch
Areas of atelectasis and hyperinflationdevelop

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 54/98
Pathology (cont .)
3 Stages
Stage 1
1-5 weeks after birth
Diffuse areas of atelectasis and hyperinflationStage 2
1-5 months after birth
Cystic (hyperinflated) areas coalesce and cause
flattening of the diaphragmsStage 3
5-24 months after birth
Cystic areas start to clear up

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 55/98
Clinical Signs
Tachypnea
Cyanosis on room air
Some retractions and/or nasal flaringDecreased breath sounds with crackles
ABGs – respiratory acidosis with
hypoxemiaCXR consistent with the stage of the disease

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 56/98
Wilson – Mikity Treatment
Is purely supportive-there is no medicinal or
surgical treatment
O2 and NTESome cases require mechanical ventilation
Maintain fluids/electrolytes and caloric
intakeWatch for infection

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 57/98
Prognosis & Complications
Prognosis good if infant survives stage 2
Complications
PDACor Pulmonale
CNS damage

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 58/98
Bronchopulmonary Dysplasia
-BPD-A result of RDS and/or its treatment
that results in areas of fibrosis,
atelectasis, and hyperinflation

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 59/98
Etiology & Predisposing Factors
RDS and prematurity
Triad of O2, ET tube, and mechanical
ventilation

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 60/98
Pathology: 4 Stages
Stage 1
Acute phase of RDS
Stage 2
4-10 days after the onset of
RDSAreas of atelectasis andhyperinflation
Stage 3
2-3 weeks after RDS
Hyperinflated areas start tocoalesce
Fibrosis starts to develop
Stage 4
1 month after the onset of
RDS
Diaphragms start to flatten
Interstitial fibrosis evident
on CXR
PPHN may start to develop
O2 dependency develops

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 61/98
Clinical Signs
Tachypnea
Persistent retractions
A-B spells
Cyanosis on room air
Decreased breath sounds with crackles
ABGs – respiratory acidosis (may be
compensated) with hypoxemia
CXR – consistent with stage of disease

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 62/98
BPD: Stage 4 CXR
Interstitial fibrosis and flattened diaphragms

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 63/98
BPD Treatment
Prevention is best! Use the least amount ofintervention for the least amount of time!
Supportive care
O2, NTE, bronchial hygiene, maintainfluids/electrolytes
Diuretics if needed to prevent fluid overloadand heart failure
Possibly vitamin E

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 64/98
Prognosis & Complications
Good if infant survives to age 2
50% mortality if PPHN develops
ComplicationsPHTN
Cor Pulmonale
Respiratory InfectionsCNS damage

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 65/98
Diaphragmatic HerniaCongenital malformation of the
diaphragm that allows abdominal
viscera into the thorax

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 66/98
Occurrence
1 per 2200 births

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 67/98
Etiology & Predisposing Factors
Exact unknown but may be related to
vitamin A deficiency

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 68/98

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 69/98
Clinical Signs
Cyanosis
Severe respiratory distress with retractions andnasal flaring
Bowel sounds in chestUneven chest expansion
Decreased breath sounds on affected side
ABGs – profound hypoxemia with combinedacidosis
CXR – loops of bowel in chest with shift ofthoracic structures towards unaffected side, egdextrocardia

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 70/98
Diaphragmatic Hernia CXR

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 71/98

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 72/98
Prognosis & Complications
50% mortality
Complications
PneumothoraxPDA
Hypoplastic lung

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 73/98
Pulmonary Barotrauma&
Air Leak Syndromes

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 74/98
4 Main Types
Pneumothorax
Pneumomediastinum
Pneumopericardium
PIE (Pulmonary Interstitial Emphysema)Gas from ruptured alveoli dissects along perivascularand interstitial spaces
Causes airway compression (obstruction) and alveolar
compression (restriction)May lead to pneumothorax, pneumomediastinum, or
pneumopericardium

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 75/98
Occurrence1-2% of all births
(not all are symptomatic)

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 76/98
Etiology & Predisposing Factors
Positive pressure ventilation
Increased airway resistance/airway
obstructionRDS

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 77/98
Clinical Signs
Sudden cyanosis
(except with PIE)
Respiratory distress
Mediastinal shift
Sudden hypotension
(except with PIE)
Crepitus (if sub-Q
emphysema develops)
Unequal chest expansion
Decreased breath soundsand hyperressonance
ABGs – hypoxemia with
respiratory acidosis
Transillumination

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 78/98
Transillumination

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 79/98
Transillumination

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 80/98
CXR: Pneumothorax

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 81/98
CXR: Pneumomediastinum
Note how air does NOT outline the apex of the
heart

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 82/98
CXR: Pneumopericardium
Note how air completely outlines the
heart

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 83/98
CXR: PIE

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 84/98
Air Leak Syndrome Treatment
Prevention! Use the least amount of
intervention for the shortest time possible!
Chest tube for pneumothorax
HFO may help prevent and/or resolve PIE

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 85/98
Prognosis and Complications
Good as long as shock and/or cardiac
tamponade does NOT occur
PIE puts infant at risk for BPD

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 86/98
Necrotizing Enterocolitis-NEC-
Necrosis of the intestinal mucosa

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 87/98
Occurrence
20% of all premature births
Males = Females
Most common in low birth weight babieswho experience perinatal distress

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 88/98
Etiology & Predisposing Factors
Exact cause unknown but seen with the
following:
Intestinal ischemia
Bacterial colonization
Early formula feeding

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 89/98
Pathology
Intestinal ischemia due to hypoperfusion, egshock, or vascular occlusion, eg, clot fromumbilical artery catheter
Bacterial colonization after ischemia startsnecrosis
Early formula feeding may provide
substrate needed for further bacterial growthand further necrosis

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 90/98
Clinical Signs
Abdominal distention
Poor feeding
Blood in fecal material
Lethargy
Hypotension
Apnea
Decreased urine output
Bile stained emesis
CXR – bubbles inintestinal wall

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 91/98
NEC Treatment
NPO and NG suction
IV hydration and hyperalimentation
Broad spectrum antibiotics
Ampicillin, Gentamycin
Minimum pressure on abdomen
No diapers or prone positioning
Monitor for/treat sepsis Necrotic bowel may need surgical resection

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 92/98
Prognosis & Complications
Mortality is 20-75%
Best prognosis if infant does NOT require any
surgery
Main complication is sepsis
Infants who have bowel resection may
develop malabsorption syndrome

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 93/98
Congenital Cardiac
Anomalies

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 94/98
Tetralogy of Fallot
VSD
Over-riding aorta
Pulmonary valve
stenosis
Right ventricular
hypertrophy
Significant cyanosis because of R-L shunt
Complete Transposition of the

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 95/98
Great Vessels
Pulmonary artery arisesfrom left ventricle andAorta arises from rightventricle
R-L shunt through PDA,ASD, or VSD needs to be
present for infant tosurvive until correctivesurgery
Balloon septostomy duringcardiac catheterization

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 96/98
Truncus Arteriosus
Aorta and pulmonary
artery are the same
vessel
Large VSDRequires MAJOR
surgical repair
Mortality is 40-50%

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 97/98

8/12/2019 Neonatal Diseases
http://slidepdf.com/reader/full/neonatal-diseases 98/98







