
Nerve Agents:Recognition and
Treatment
Ventura County
Emergency Medical Services

Chemical Warfare Agents
• Chemical Agents– Chemicals used in military
operations to kill, injure, or incapacitate
• Incapacitating vs. Lethal
• Local vs. Systemic Effects

Nerve Agent Terrorist Attacks
• Matsumoto:– 280 injured– 7 dead
• Tokyo– 12 dead– Approximately 1,000 hospitalized– 5,500 sought medical care– 132 first responders injured

Scenario # 1
• A chemical is released in a movie theater at 7 PM. Fire and EMS respond to the scene.
One patient is dead,
Two patients are unconscious but still breathing.
Five patients are weak and complaining of eye pain, but are still ambulatory.
Others begin running from the scene.
Scenario # 1 (cont.)
• Two EMTs from the first-in unit arrive first, and while bag-mask ventilating two of the seriously injured victims, become weak, short of breath, with dim vision and eye pain.

Scenario # 1 (cont.)
• What actions should be taken immediately?
• Who should be contacted?
• What options are available for: – Protecting the EMS responders?
– Treatment for the victim?
– Stabilization and transport?

Nerve Agents
• Most toxic chemical agents: are liquids, not “gas”
• GB (Sarin): vapor or liquid hazard; non-persistent
• VX: liquid hazard; persistent
• Penetrate skin, eyes, lungs
• Loss of consciousness, seizures, apnea, death
• Diagnosis made clinically, confirmed by laboratory test

Nerve Agents
• Organophosphates
• Insecticides are easily obtained and commonly used in the community
• Like insecticides:– Malathion
– Diazinon
– Chlorpyrifos

Normal Nerve Function
ACh

Normal Nerve Function
ACh

Normal Nerve Function
ACh
AChE

How Nerve Agents Work
AChE
AChGB
• Hyperstimulation of organs of cholinergic nervous system– Muscarinic
•Smooth muscles
•Glands
– Nicotinic
•Skeletal muscles
•Ganglions
Effects of Nerve Agents

Effects of Nerve Agents - Muscarinic Sites
• Increased secretions– Saliva
– Tears
– Runny nose (rhinorrhea)
– Secretions in airways
– Secretions in gastrointestinal tract
– Sweating
Effects of Nerve Agents -Muscarinic Sites
• Smooth Muscle Contraction:– Eyes: Small pupils -> dim vision
– Airways: Narrowing -> shortness of breath
– Intestine: Hyperactivity -> nausea, vomiting, diarrhea
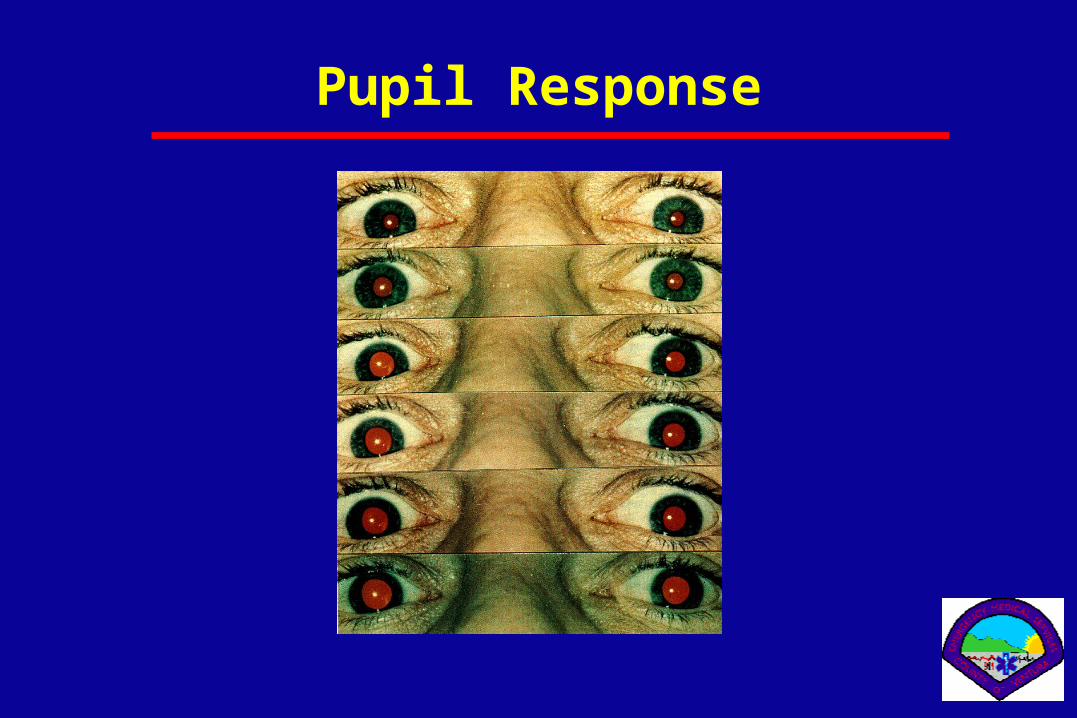
Pupil Response

Nicotinic Sites
• Skeletal muscles– Fasciculations
– Twitching
– Weakness
– Flaccid paralysis
• Ganglion– Tachycardia
– Hypertension
Pinpoint pupils + muscle twitching = Nerve Agent exposure

Central Nervous System Effects
• Acute•Loss of consciousness
•Convulsions
•Apnea
• Prolonged (4 to 6 weeks)•Psychological effect

• Inhalation
• Ingestion
• Direct contact
Routes of
Exposure

Vapor Exposure
• Vapor effects occur within seconds, peak within minutes
• Low exposure– Miosis [constricted pupils] (dim vision, eye
pain)– Runny nose (rhinorrhea)– Shortness of breath
• High exposure– Immediate loss of consciousness, seizures,
apnea, flaccid paralysis
•Absorption through skin:
•All agents can be absorbed
•VX persists longer
•GB evaporates quickly, but still threat
•Scrape or cut in skin allows immediate entry
•Entry also through eyes
Direct Contact

Direct Contact
• Small amount– Localized sweating– Fasciculations
• Moderate amount (<LD50)– Gastrointestinal effects
• Large amount (LD50)– Sudden loss of consciousness– Seizures– Apnea

Skin Exposure - Time Course
Onset time: minutes to several hours • The larger the exposure the shorter the onset time • After large exposure, effects within minutes
• After asymptomatic period, first effect may be loss of consciousness • Onset time may be as long as 18 hrs after exposure; in such cases effects usually not lethal

• Access to bloodstream via digestive system
• Effects similar to inhalation, but at greater doses
Ingestion

Signs and symptoms could also be due to:
• Epilepsy
• Gastroenteritis
• Exposure to agricultural insecticides (organophosphates and carbanates)
• Heat illnesses
• Emphysema
• Stroke
• Head trauma
• Drug overdose
Other Possible Causes of Symptoms

Treatment
• Self-protection
• Decontamination

Treatment
• Airway/ventilation
• Antidotes– Atropine
– Pralidoxime
(2-PAM)
– Midazolam
Atropine
• Given IV, IM, ET
• Antagonizes muscarinic effects– Dries secretions; relaxes smooth muscles
• Does not affect miosis, fasciculations, muscle strength (nicotinic)
• May cause cardiac arrhythmias IV in hypoxic patient (v-fib)

Atropine
• Starting dose - 2 mg
• Maximum cumulative dose - 20 mg
• Side effects in normal people– Dilated pupils
– Blurred vision
– Tachycardia
– Decreased sweating

Atropine
• Atropine - How much to give?– Until secretions are drying or dry
– Until ventilation is “easy”
•If conscious, and victim is comfortable
– Don’t rely on heart rate/pupil size

Atropine Overdose
If excessive atropine is administered:
• Signs of atropinization will become even more severe and patient may also develop– blurring of vision
– delirium
– urinary retention
• When signs and symptoms of atropinization develop, no more atropine should be injected until atropinization subsides
Pralidoxime Chloride (2-PAM)
• Remove nerve agent from AChE in absence of aging (2-PAM “crowbar”)
• Does not reverse muscarinic effects on glands and smooth muscles
• Helps at nicotinic sites AChE
2-PAM Cl
Nerve Agent

• 2-PAM may cause: – blurred vision
– diplopia
– impaired accommodation
– headache
– nausea
2-PAM Adverse Reactions
These are relatively mild when compared to These are relatively mild when compared to effects of nerve agentseffects of nerve agents
– dizziness
– drowsiness
– tachycardia
– hyperventilation
– hypertension

Midazolam
• Decreases seizure activity
• Reduces seizure-induced brain injury
• Must observe carefully for respiratory depression

Autoinjectors

Auto-Injectors
Simple, compact injection systems
• Permit rapid injection of required antidotes
• Prevent needle from being subject to cross-contamination
• Enable rapid and accurate administration even if care giver or patient is in protective clothing
View the movie file that you downloaded now.

Directions for Use
1. 1. Remove safety capRemove safety cap
• Yellow on atropineYellow on atropine• Gray on 2-PAMGray on 2-PAM• Mark I kit clip holds the safety Mark I kit clip holds the safety capscaps
– May not notice if using Mark I May not notice if using Mark I kitskits
• Do not touch colored end of Do not touch colored end of injector after removing capinjector after removing cap - - injector will injectinjector will inject
into fingers or handinto fingers or hand

Directions for Use
2. Hold injector - either like a pen or in 2. Hold injector - either like a pen or in fist.fist.
3. 3. Place colored end (Green on Place colored end (Green on atropine, black on 2-PAM) on thickest atropine, black on 2-PAM) on thickest part of thigh and press hard until part of thigh and press hard until injector functions.injector functions.
•Pressure automatically activates the Pressure automatically activates the spring, inserts the needle into the muscle spring, inserts the needle into the muscle and injects the medicationand injects the medication

4. After auto-injector has been activated, empty container should be disposed of properly
• It cannot be refilled nor can the protruding needle be retracted • It should be disposed of in a “sharps” container
5. Note dosage on triage tag or write on chest or forehead of patient
AI 18©
Directions for Use

Potential Exposure
• No signs or symptoms– Reassure
– Segregate in cold zone
– Observe
– Arrange transport to ED by bus or vans
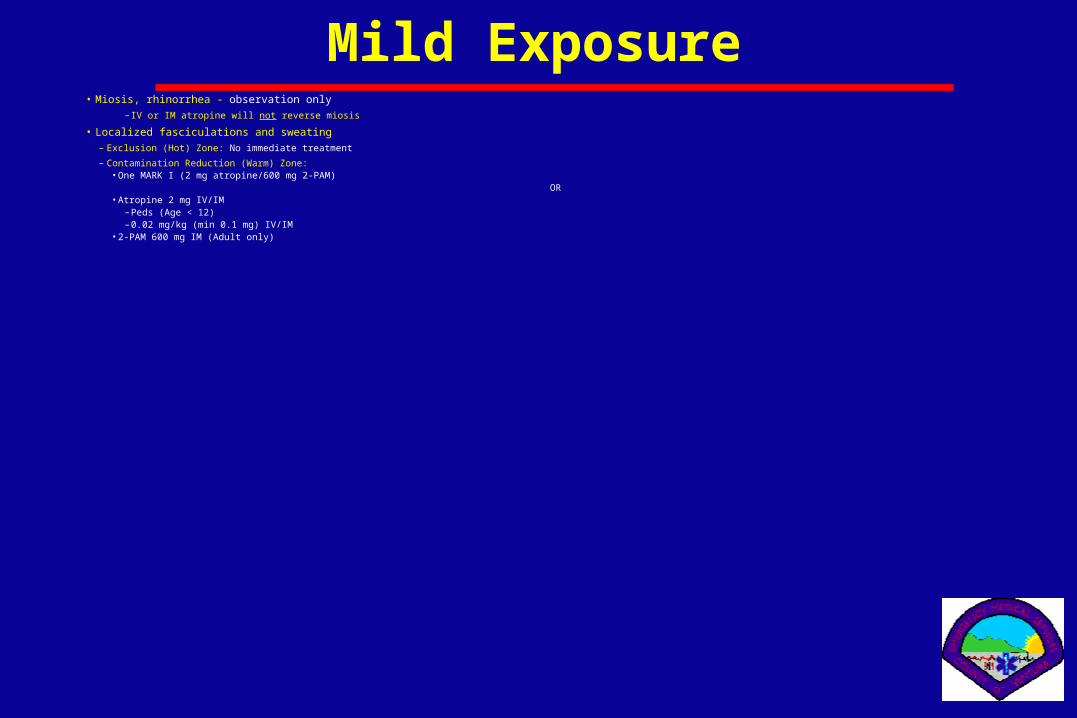
Mild Exposure• Miosis, rhinorrhea - observation only
– IV or IM atropine will not reverse miosis
• Localized fasciculations and sweating– Exclusion (Hot) Zone: No immediate treatment
– Contamination Reduction (Warm) Zone:•One MARK I (2 mg atropine/600 mg 2-PAM)
OR•Atropine 2 mg IV/IM
– Peds (Age < 12)– 0.02 mg/kg (min 0.1 mg) IV/IM
•2-PAM 600 mg IM (Adult only)
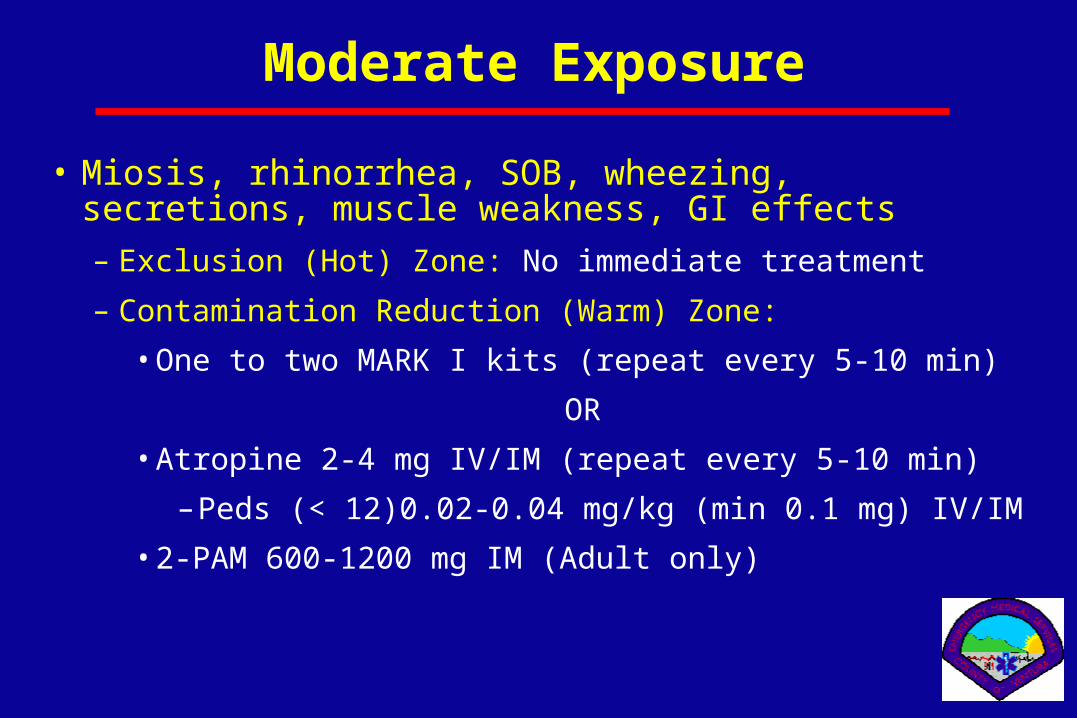
Moderate Exposure
• Miosis, rhinorrhea, SOB, wheezing, secretions, muscle weakness, GI effects– Exclusion (Hot) Zone: No immediate treatment
– Contamination Reduction (Warm) Zone:
•One to two MARK I kits (repeat every 5-10 min)
OR
•Atropine 2-4 mg IV/IM (repeat every 5-10 min)
– Peds (< 12)0.02-0.04 mg/kg (min 0.1 mg) IV/IM
•2-PAM 600-1200 mg IM (Adult only)

Severe Exposure
• Unconscious, seizing, flaccid, apnea
• Exclusion (Hot) Zone: – 3 MARK I kits IM as soon as possible
• Contamination Reduction (Warm) Zone:– 3 MARK I kits IM as soon as possible
OR
– Atropine 2-6 mg IV/IM
•Peds (<12) 0.02-0.06 mg/kg (min 0.1 mg) IV/IM
– 2PAM 600-1800 mg IM (Adult only)
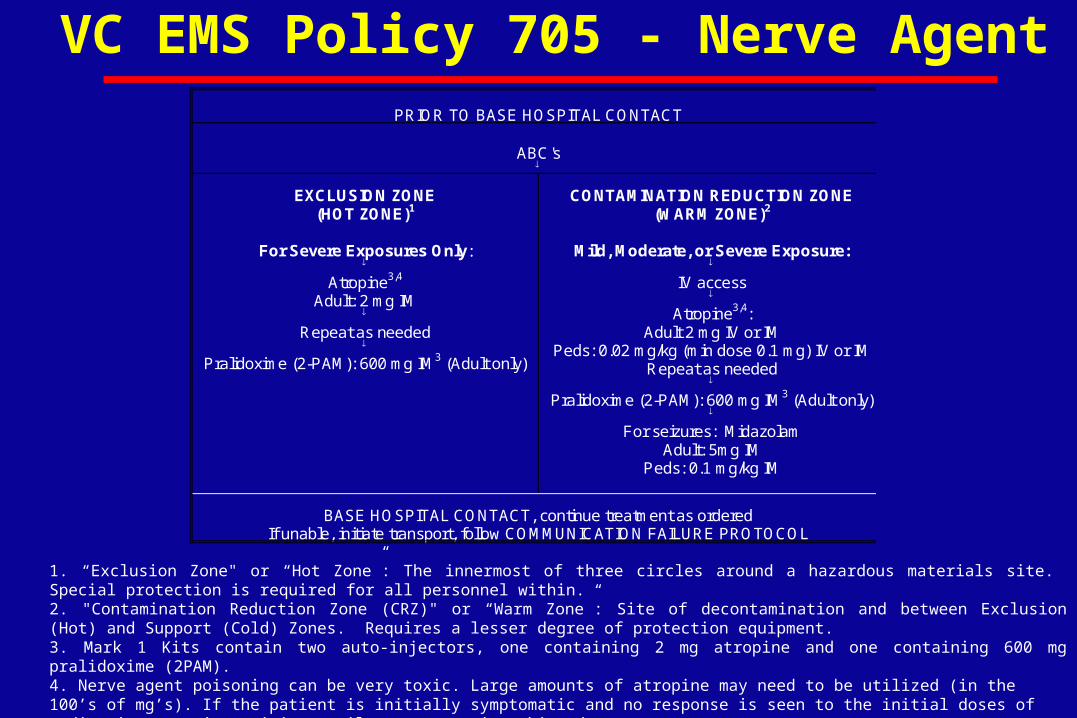
VC EMS Policy 705 - Nerve AgentPRIOR TO BASE HOSPITAL CONTACT
ABC's
EXCLUSION ZONE(HOT ZONE)1
For Severe Exposures Only:
Atropine3,4
Adult: 2 mg IM
Repeat as needed
Pralidoxime (2-PAM): 600 mg IM3 (Adult only)
CONTAMINATION REDUCTION ZONE(WARM ZONE)2
Mild, Moderate, or Severe Exposure:
IV access
Atropine3,4:Adult 2 mg IV or IM
Peds: 0.02 mg/kg (min dose 0.1 mg) IV or IMRepeat as needed
Pralidoxime (2-PAM): 600 mg IM3 (Adult only)
For seizures: MidazolamAdult: 5mg IM
Peds: 0.1 mg/kg IM
BASE HOSPITAL CONTACT, continue treatment as orderedIf unable, initiate transport, follow COMMUNICATION FAILURE PROTOCOL
1. “Exclusion Zone" or “Hot Zone”: The innermost of three circles around a hazardous materials site. Special protection is required for all personnel within.2. "Contamination Reduction Zone (CRZ)" or “Warm Zone”: Site of decontamination and between Exclusion (Hot) and Support (Cold) Zones. Requires a lesser degree of protection equipment.3. Mark 1 Kits contain two auto-injectors, one containing 2 mg atropine and one containing 600 mg pralidoxime (2PAM).4. Nerve agent poisoning can be very toxic. Large amounts of atropine may need to be utilized (in the 100’s of mg’s). If the patient is initially symptomatic and no response is seen to the initial doses of medication, continue giving until a response is achieved.5. Adult = age >= 12. Peds = age <12.







