
Neurocritical care improves outcome in severe traumatic brain injury
Martin SmithConsultant & Honorary Professor in Neurocritical CareThe National Hospital for Neurology & NeurosurgeryUniversity College London Hospitals
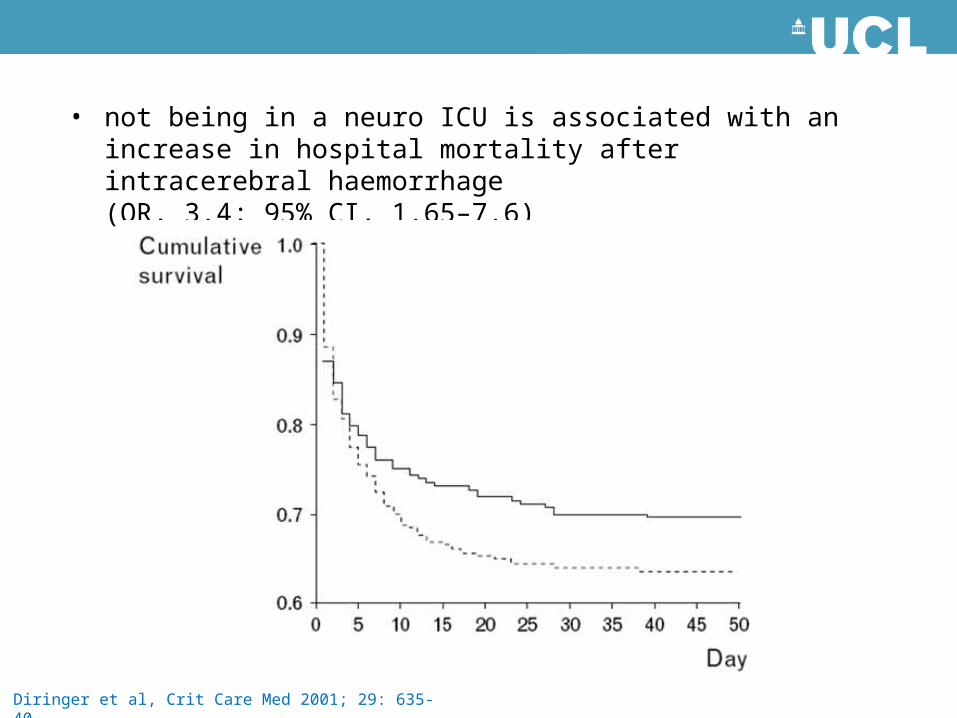
Diringer et al, Crit Care Med 2001; 29: 635-40
• not being in a neuro ICU is associated with an increase in hospital mortality after intracerebral haemorrhage(OR, 3.4; 95% CI, 1.65–7.6)
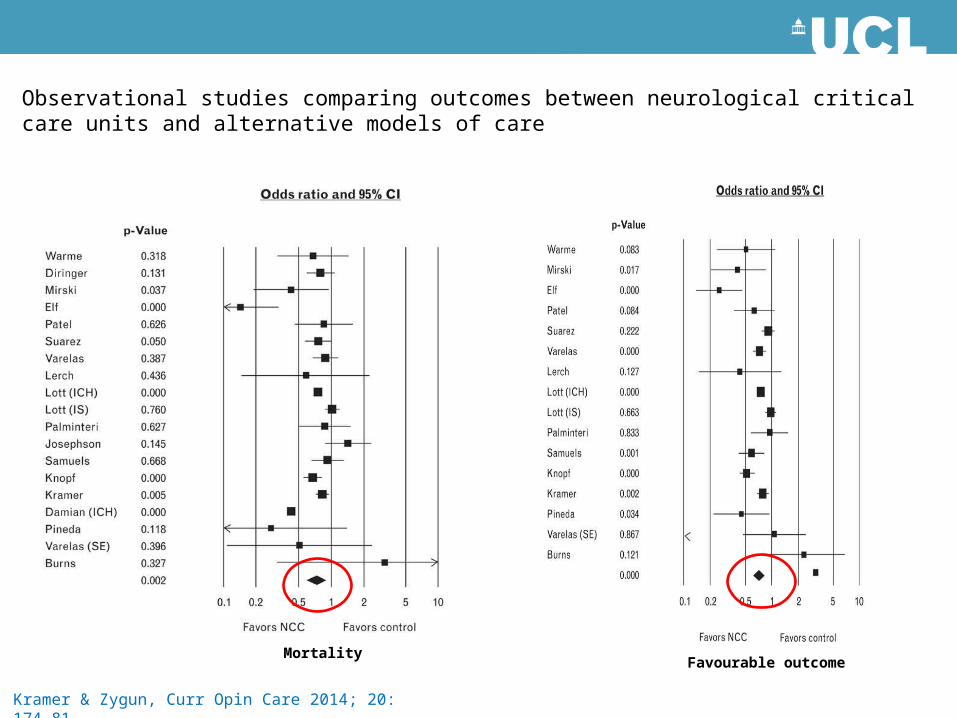
Observational studies comparing outcomes between neurological critical care units and alternative models of care
Kramer & Zygun, Curr Opin Care 2014; 20: 174-81
Mortality Favourable outcome
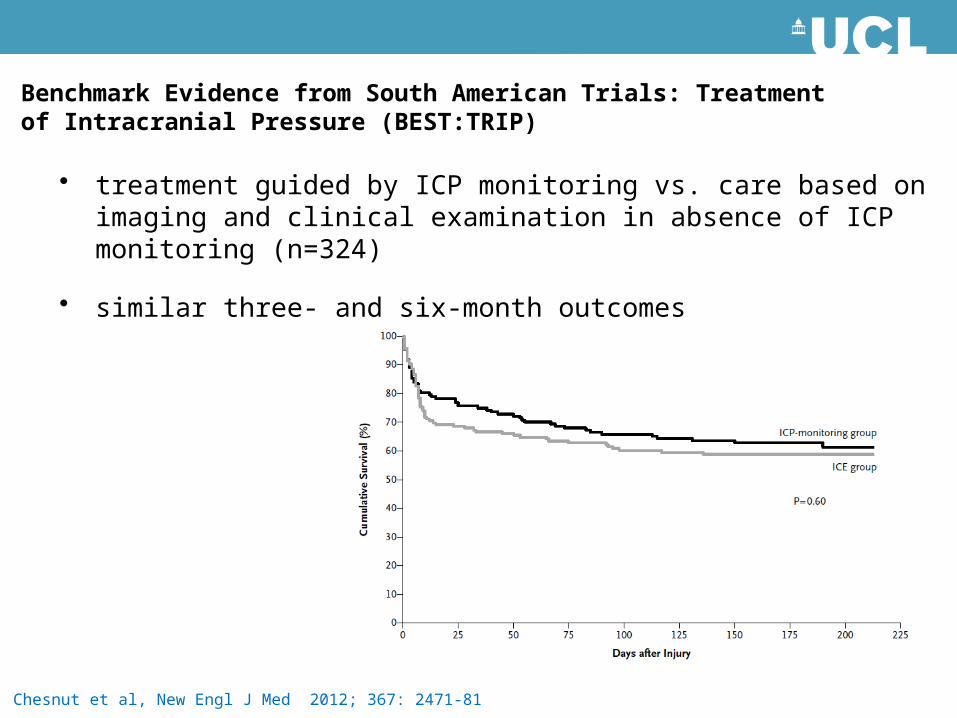
• treatment guided by ICP monitoring vs. care based on imaging and clinical examination in absence of ICP monitoring (n=324)
• similar three- and six-month outcomes
Benchmark Evidence from South American Trials: Treatment of Intracranial Pressure (BEST:TRIP)
Chesnut et al, New Engl J Med 2012; 367: 2471-81
• moderate hypothermia one of the most effective neuroprotective strategies in preclinical studies- translated into humans
Targeted temperature management
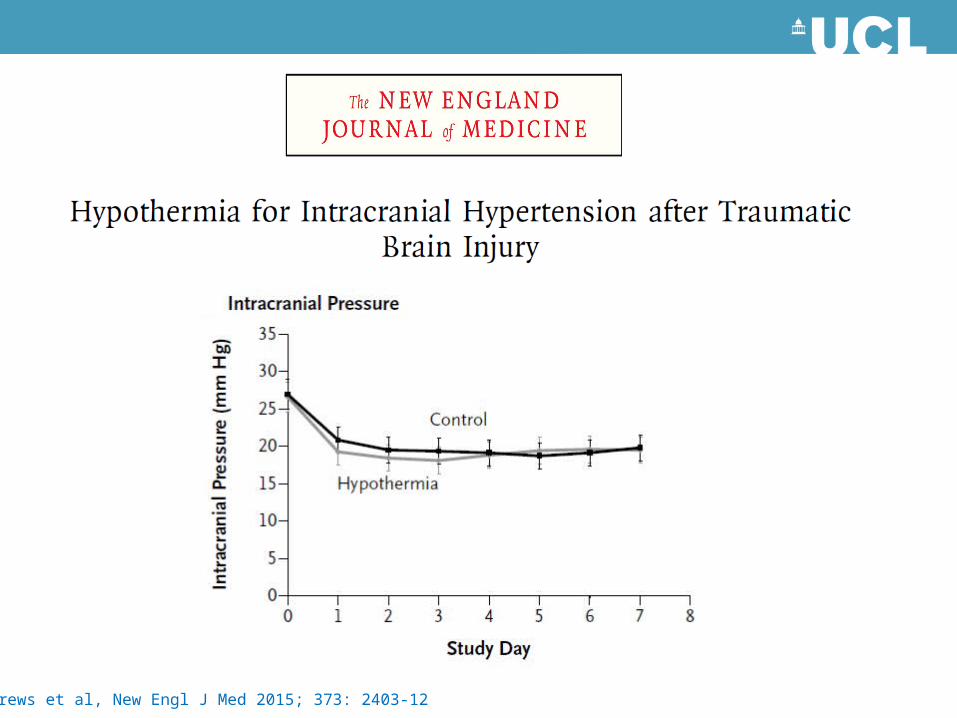
Andrews et al, New Engl J Med 2015; 373: 2403-12
• Eurotherm3235 trial randomized 387 patients from 47 centers in 18 countries – TTM (32-35˚C) as a component of ICP management of intracranial hypertension
(ICP > 20 mmHg) resistant to initial ICP-lowering therapies
• recruitment suspended early because of safety concerns in the hypothermia group– worse functional outcomes (odds ratio 1.53, 95% CI 1.02-2.30)– higher mortality rates (hazard ratio 1.45, 95% CI 1.01-2.10)
Andrews et al, New Engl J Med 2015; 373: 2403-12
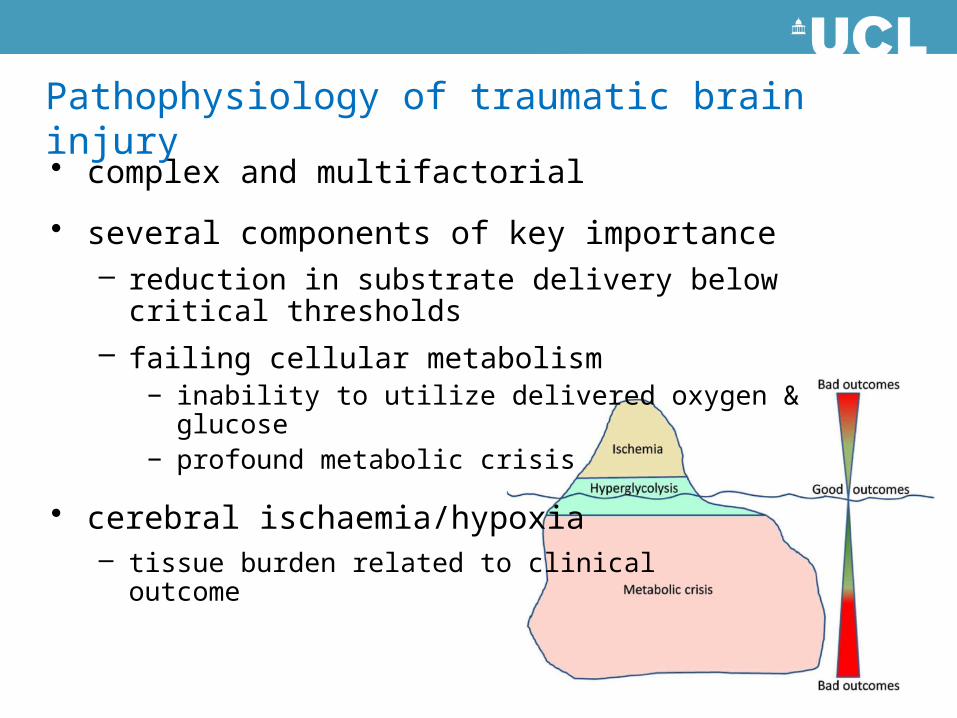
• complex and multifactorial
• several components of key importance– reduction in substrate delivery below critical thresholds – failing cellular metabolism
− inability to utilize delivered oxygen & glucose− profound metabolic crisis
• cerebral ischaemia/hypoxia– tissue burden related to clinical
outcome
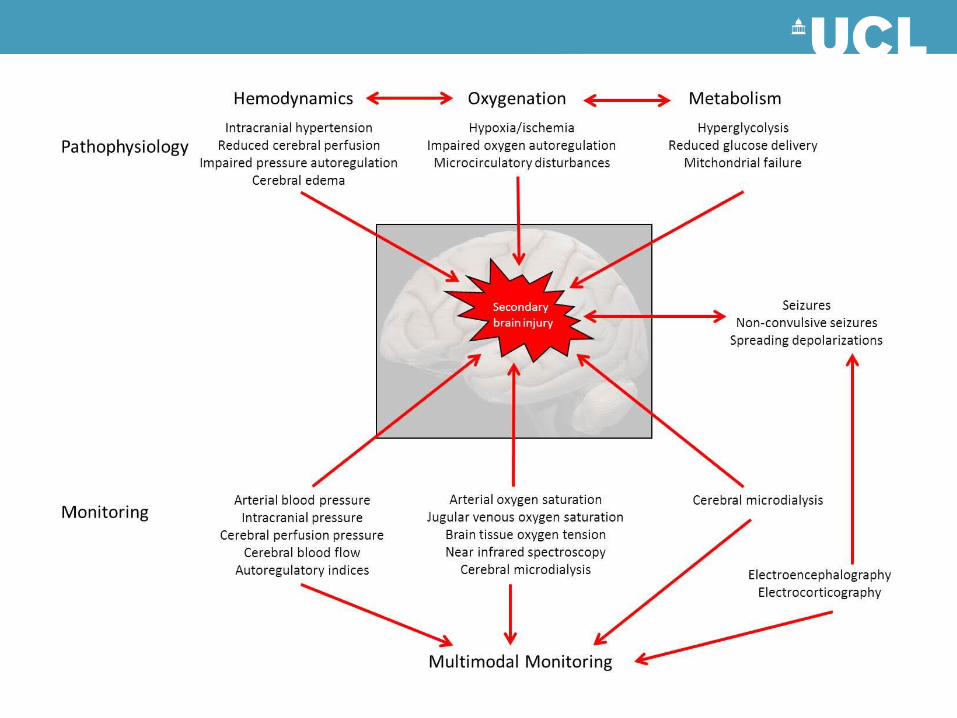
Pathophysiology of traumatic brain injury
• secondary insults adversely affect the injured brain– associated with worse outcomes– prevention/rapid treatment associated with improved
outcomes
Pathophysiology of traumatic brain injury

– hypoxia
– hypotension
– hyper- and hypocarbia
– hyper- and hypoglycaemia
– hyperthermia
– intracranial hypertension
– seizures
Secondary insults
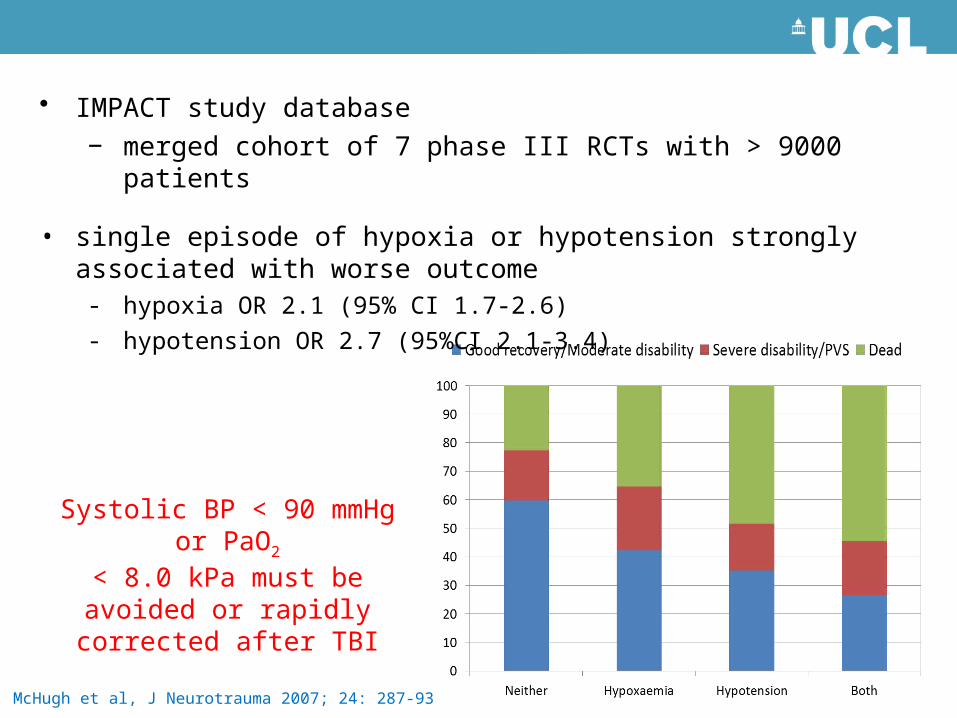
McHugh et al, J Neurotrauma 2007; 24: 287-93
• IMPACT study database− merged cohort of 7 phase III RCTs with > 9000 patients
• single episode of hypoxia or hypotension strongly associated with worse outcome- hypoxia OR 2.1 (95% CI 1.7-2.6)- hypotension OR 2.7 (95%CI 2.1-3.4)
Systolic BP < 90 mmHg or PaO2
< 8.0 kPa must be avoided or rapidly corrected after TBI
• ABG targets– PaO2 > 13.0 kPa– PaCO2 4.5 - 5.0 kPa
• CVS targets– MAP > 90 mmHg– volume resuscitation– vasopressors/inotropes
• glucose 5.0 - 10.0 mmol/l
• core temperature < 37oC
• ICP < 20 cmH20
• CPP 50-70 mmHg
Brain Trauma Foundation, J Neurotrauma 2007; 24: S1-S106
Consensus guidelines
Brain Trauma Foundation, J Neurotrauma 2007; 24: S1-S106
Consensus guidelines
• guidelines are a tool, not a goal
• goal is individualised, targeted treatment
• treatment guided by monitor-derived physiological variables
• ABG targets– PaO2 > 13.0 kPa– PaCO2 4.5 - 5.0 kPa
• CVS targets– MAP > 90 mmHg– volume resuscitation– vasopressors/inotropes
• glucose 5.0 - 10.0 mmol/l
• core temperature < 37oC
• ICP < 20 cmH20
• CPP 50-70 mmHg
• multimodal monitoring allows delivery of tailored treatment regimens– identify physiological/pathophysiological phenotype– guide targeted therapy– assess effects of therapy– guide decisions about intensity and duration of therapy– improved patient outcomes
• confidence to withhold potentially dangerous therapy in those without evidence of brain ischaemia or metabolic disturbance
Individualized therapy
ICP-directed management
• greatly elevated ICP is fatal– ability to control it is limited
• oversimplified concepts surrounding manipulation of ICP and the association with outcome– thresholds for initiating medical and surgical management– cerebral perfusion often not compromised even if ICP is > 20 mmHg– outcome effects of current treatment probably smaller than we think– all treatments have side effects
• severe TBI is an overwhelming and complex process– involves neurones, glia and vasculature– raised ICP compresses cerebral veins creating a self-regenerating cycle
of even higher pressure
Nangunoori et al, Neurocrit Care 2012;17: 131-8
• brain resuscitation based on control of ICP & CPP alone does not prevent cerebral hypoxia in some patients
• increased hypoxia burden associated with poor outcome
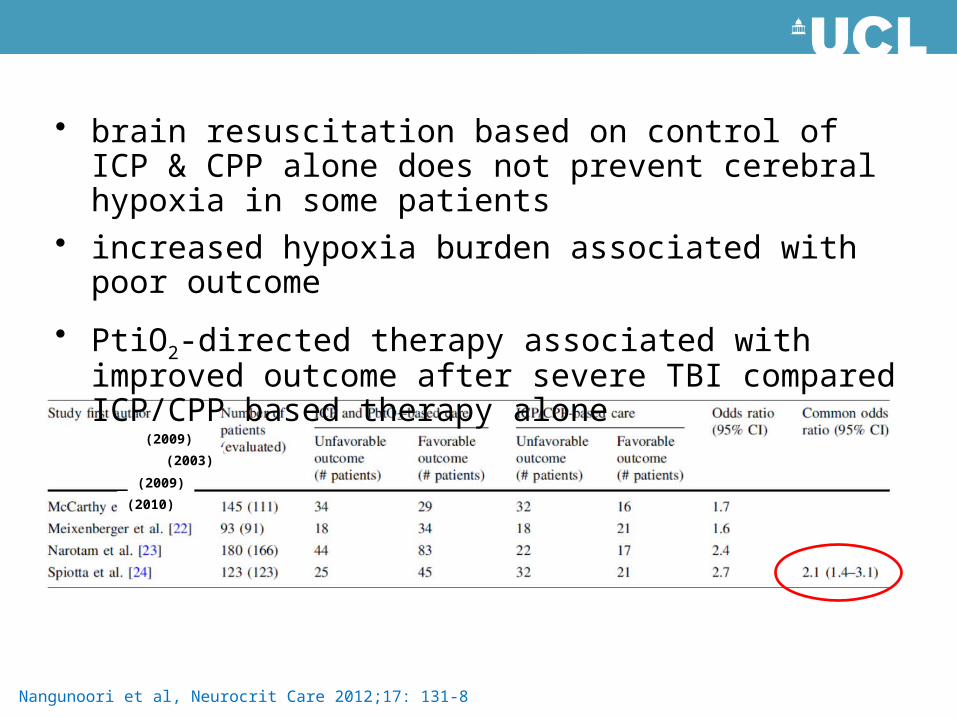
Nangunoori et al, Neurocrit Care 2012;17: 131-8
(2009)(2003)
(2009)(2010)
• brain resuscitation based on control of ICP & CPP alone does not prevent cerebral hypoxia in some patients
• increased hypoxia burden associated with poor outcome
• PtiO2-directed therapy associated with improved outcome after severe TBI compared ICP/CPP based therapy alone
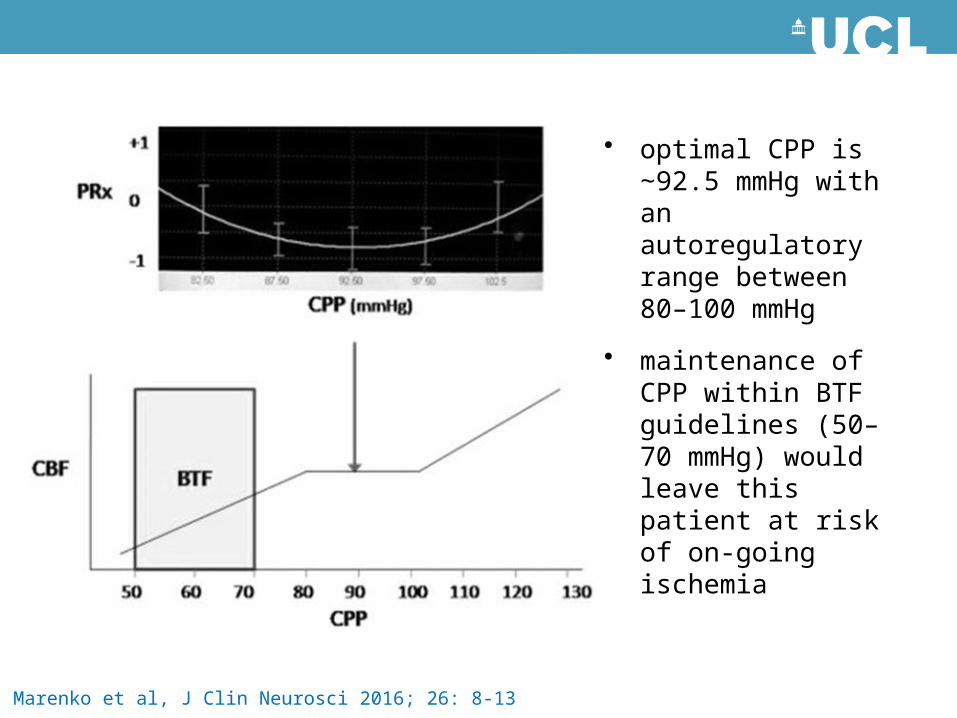
Marenko et al, J Clin Neurosci 2016; 26: 8-13
• optimal CPP is 92.5 ∼mmHg with an autoregulatory range between 80–100 mmHg
• maintenance of CPP within BTF guidelines (50–70 mmHg) would leave this patient at risk of on-going ischemia
• brain tissue destruction caused by acute injury is worsened by on-going insults- early, aggressive intervention to minimize secondary insults improves the
outcome trajectory in many patients- minimizing second insults will minimize residual disability
Critical care management of severe TBI
• get all the little things right all the time- neurocritical care is as much about meticulous systemic physiological
optimization as it is about specific brain-directed therapies
• keep it simple - the six ‘Ns’– normoxia– normocapnia– normovolaemia– normotension– normoglycaemia– normothermia
– normonatraemia– normomagnesaemia
Critical care management of severe TBI
• get all the little things right all the time- neurocritical care is as much about meticulous systemic physiological
optimization as it is about specific brain-directed therapies
• optimise cerebral haemodynamics and oxygention– blind adherence to guidelines risks delivering potentially harmful
treatment that is of no benefit– individualize ICP and CPP-guided therapy– multimodal physiological monitoring
Critical care management of severe TBI
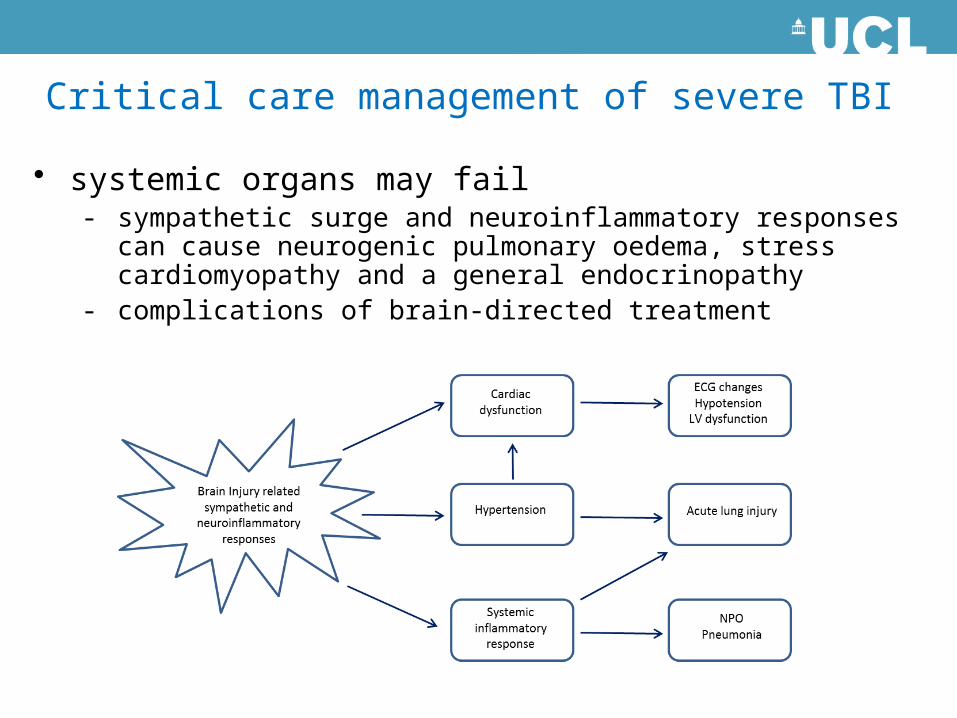
• systemic organs may fail- sympathetic surge and neuroinflammatory responses can cause
neurogenic pulmonary oedema, stress cardiomyopathy and a general endocrinopathy
- complications of brain-directed treatment
Critical care management of severe TBI
• systemic organs may fail- sympathetic surge and neuroinflammatory responses can cause
neurogenic pulmonary oedema, stress cardiomyopathy and a general endocrinopathy
- complications of brain-directed treatment
• complex interaction between brain and systemic physiology- optimize systemic and intracranial variables- physiological neuroprotection
Critical care management of severe TBI
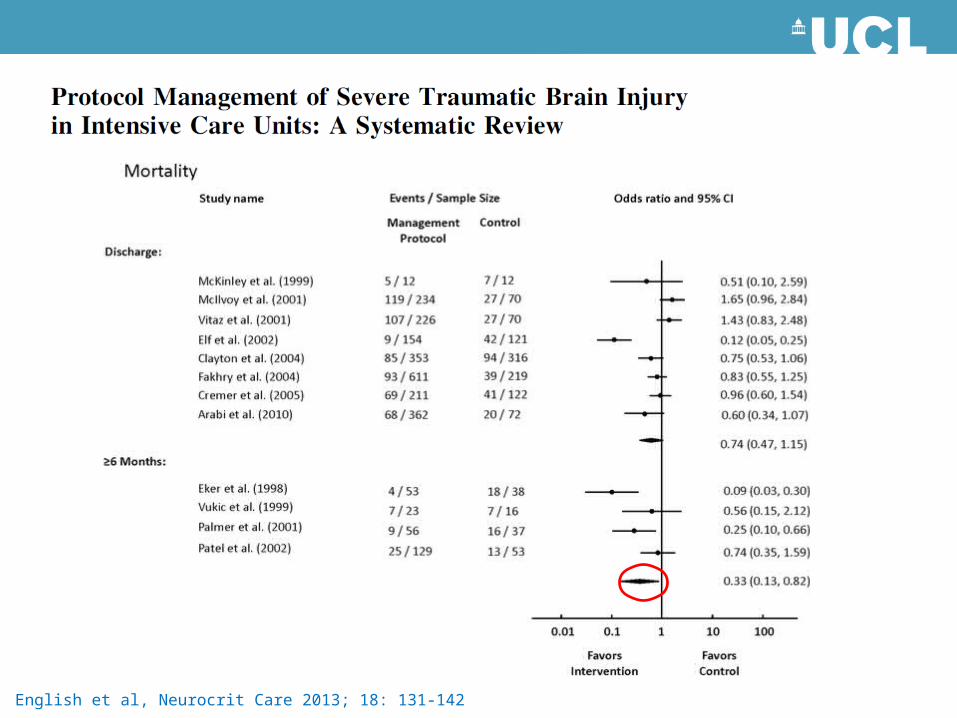
English et al, Neurocrit Care 2013; 18: 131-142
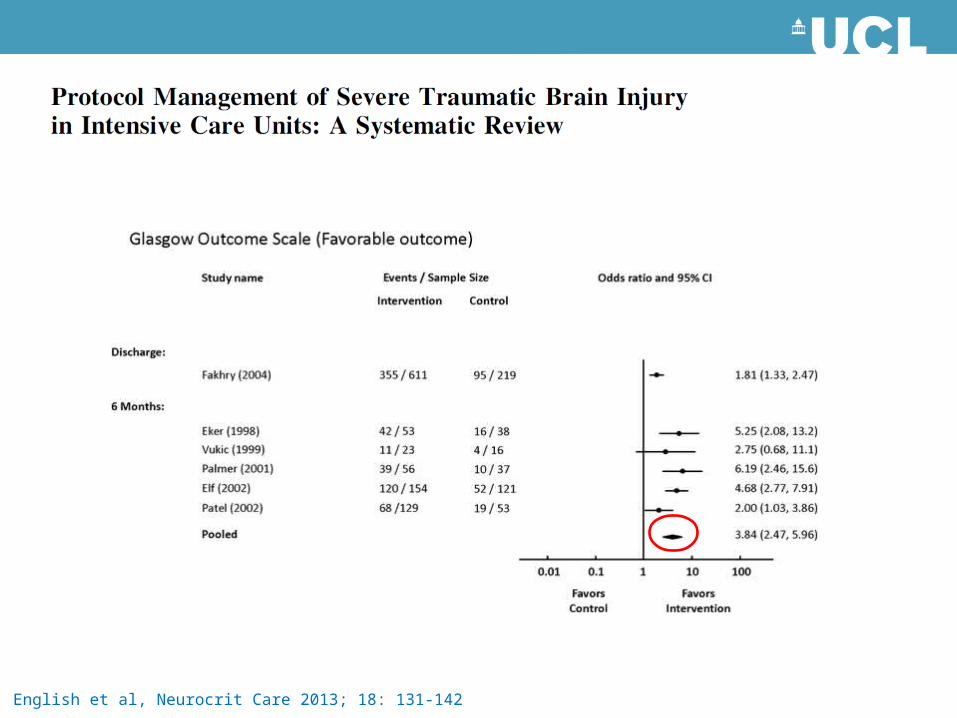
English et al, Neurocrit Care 2013; 18: 131-142
• burden of neuronal loss directly related to clinical outcomes– minimize secondary ischaemic brain injury
• clinical guidelines are a useful starting point
• individualized treatment regimens
• neurocritical care does improve outcomes after TBI
Summary

THANK YOU!

SOCIETY FOR NEUROSCIENCE IN ANESTHESIOLOGY AND CRITICAL CARE
SNACC 44th Annual MeetingOctober 20-21, 2016Chicago
www.snacc.org







