
Neurodevelopmental outcomes in
Infants with prenatally diagnosed CHD
Helena Gardiner MD PhD
Fetal cardiovascular Fellowship Director

Disclosure slide
• I have no disclosures

Recognition of previously under-recognized neuro-
developmental delay in children with CHD
1988 – Boston circulatory arrest study of 171 newborns with TGA
2002 – preliminary ND outcomes
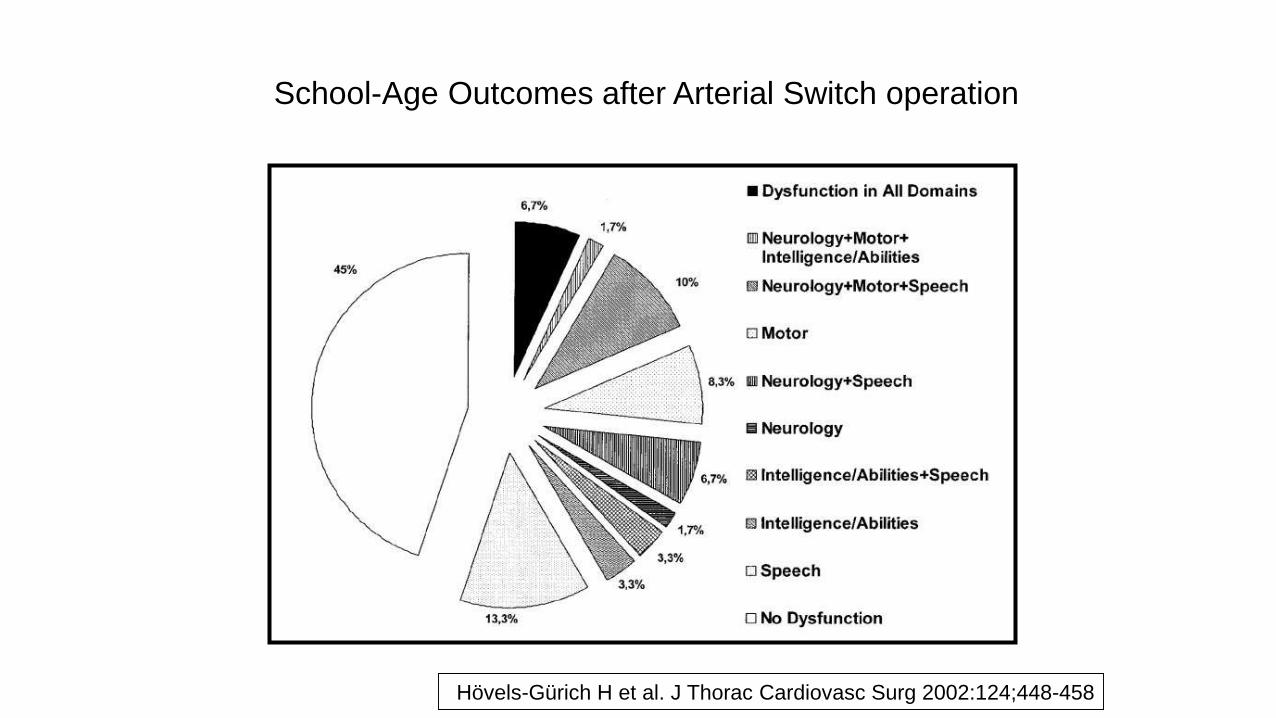
School-Age Outcomes after Arterial Switch operation
Hövels-Gürich H et al. J Thorac
Cardiovasc Surg 2002:124; 448-458Hövels-Gürich H et al. J Thorac Cardiovasc Surg 2002:124;448-458

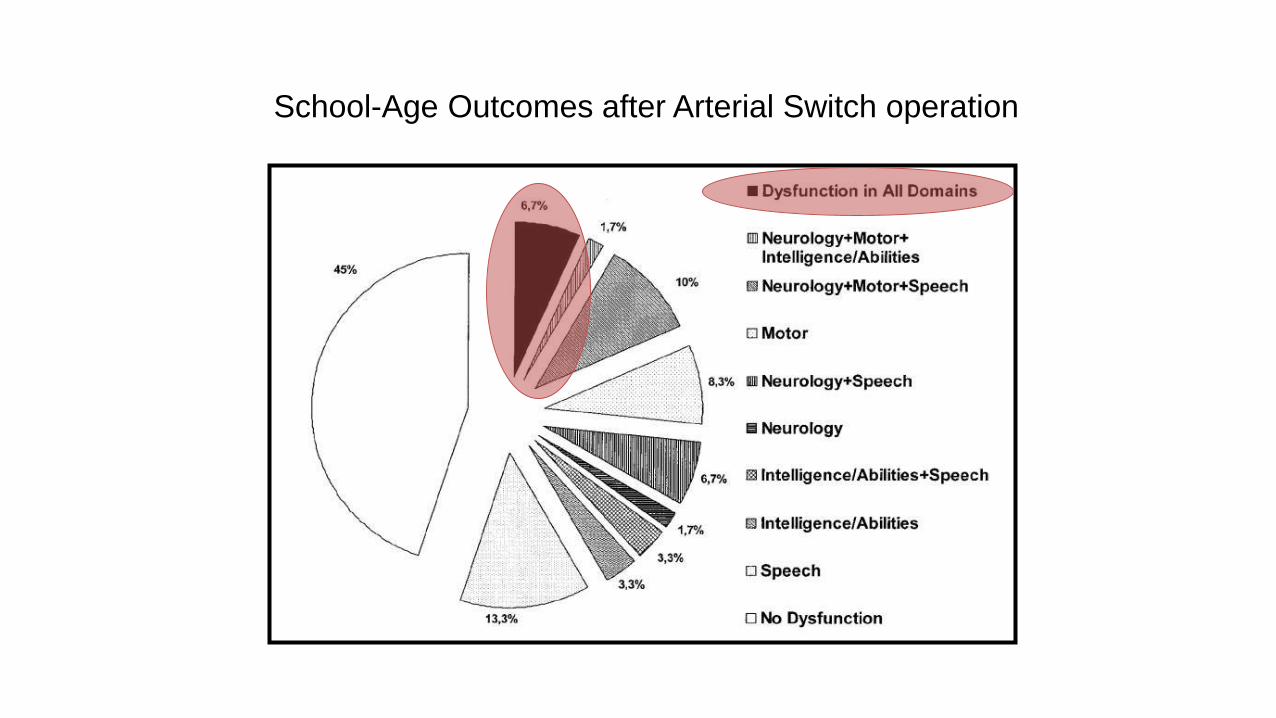
School-Age Outcomes after Arterial Switch operation
Hövels-Gürich H et al. J Thorac
Cardiovasc Surg 2002:124; 448-458
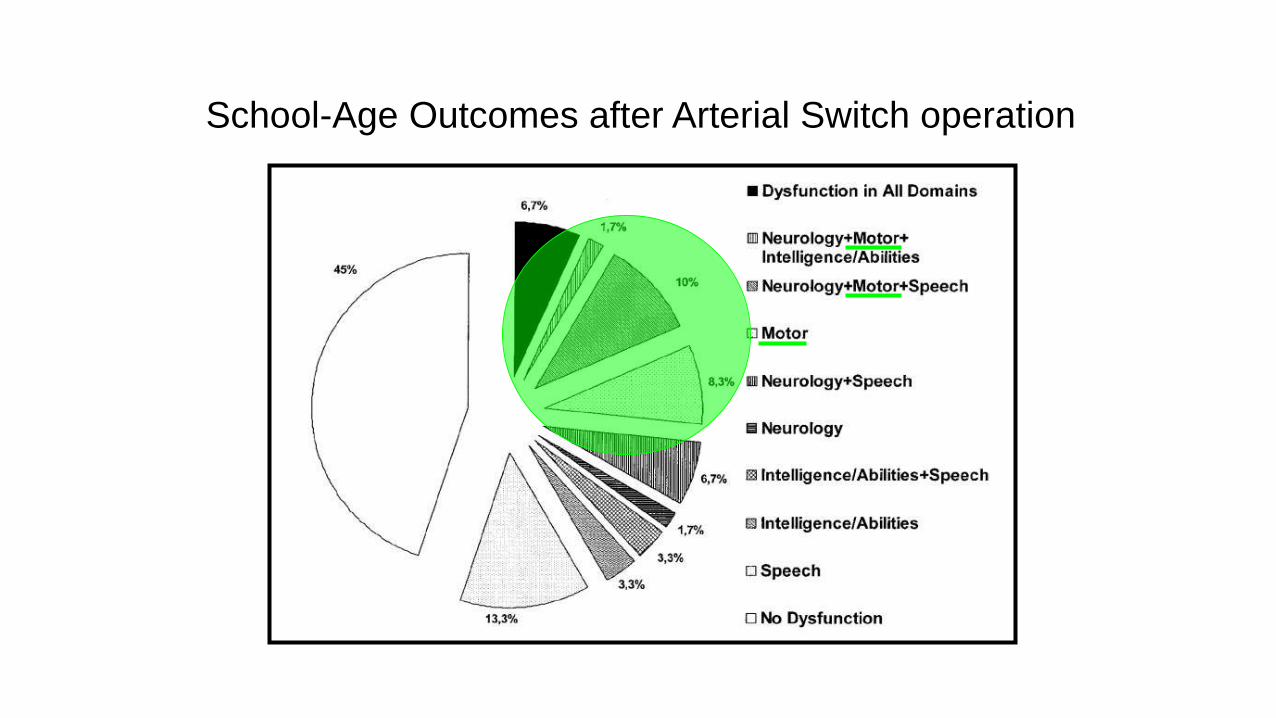
School-Age Outcomes after Arterial Switch operation
Hövels-Gürich H et al. J Thorac
Cardiovasc Surg 2002:124; 448-458
School-Age Outcomes after Arterial Switch operation
Hövels-Gürich H et al. J Thorac
Cardiovasc Surg 2002:124; 448-458

School-Age Outcomes after Arterial Switch operation
Hövels-Gürich H et al. J Thorac
Cardiovasc Surg 2002:124; 448-458
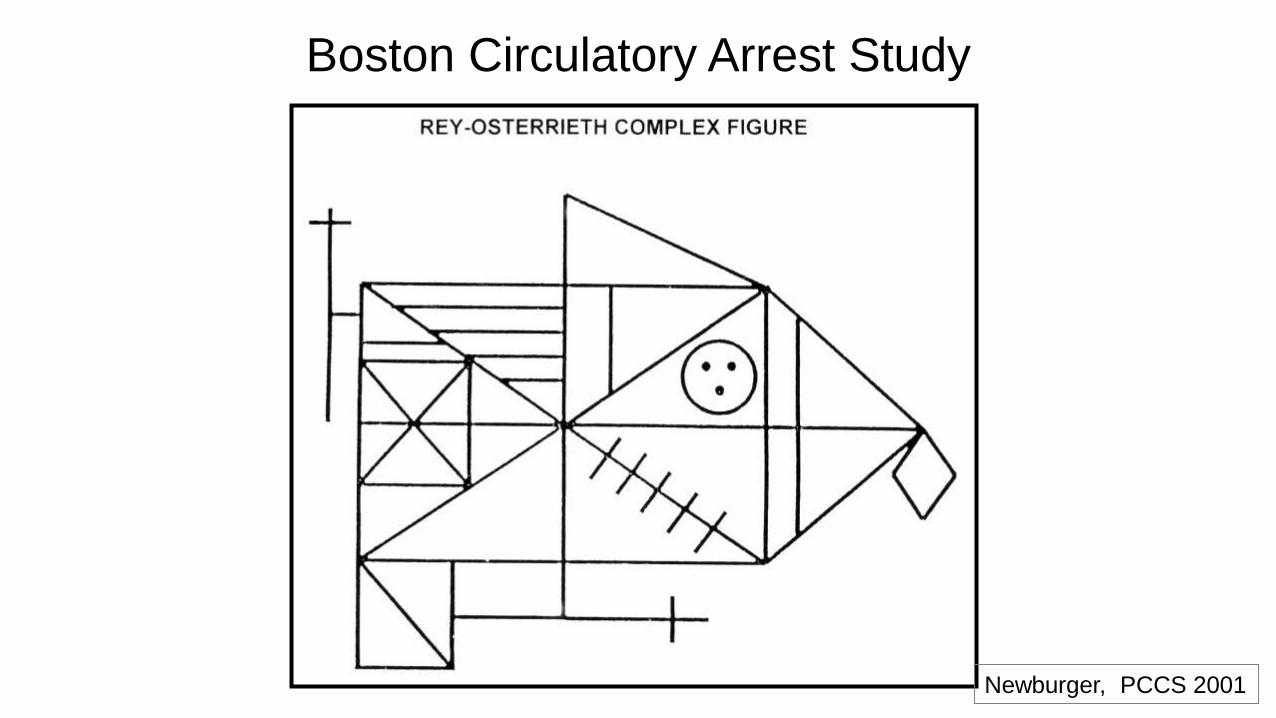
Newburger, PCCS 2001
Boston Circulatory Arrest Study
Boston Circulatory Arrest Study

Boston Circulatory Arrest Study
Boston Circulatory Arrest Study

Performance on the Rey-Osterrieth figure and academic success
0
10
20
30
40
50
60
remedial services grade retention
I(worst) 2 3 4 5 (best)%
Boston Circulatory Arrest Study

Special Education and Rehabilitative Services in Fontan Survivors
(n=240)
0%
20%
40%
60%
80%
100%
Speech
Therapist
Special
Educator
Occupational
Therapist
Physical
Therapist
Neurologist Psychiatrist Social Worker
Never Previous CurrentMitchell M et al
J Thorac Cardiovasc Surg 2006;131:172

Recognition of previously under-recognized neuro-
developmental delay in children with CHD
1988 – Boston circulatory arrest study of 171 newborns with TGA
2002 – preliminary ND outcomes
2011 - outcome aged 16 years:
17% grade retention
25% special education
25% psychotherapy/counselling
Surgical strategies did not result in any marked differences in outcome
Survivors of arterial switch procedure for TGA showed poorer academic
achievement and abnormality of fine motor function, visual spatial skills,
attention deficit and social cognition

Term
BirthConception
Neurulation
3-4 Wk
Migration
20 Wk
Vulnerable Periods of White Matter Development
23 Wk 32 Wk
WM precursors
vulnerability Myelination
Back J, Neurosci 2001
> 2 years
Open
operculumChen-Yu, Am J
Neuroradiol 1995
34 week Term
Closed
operculum
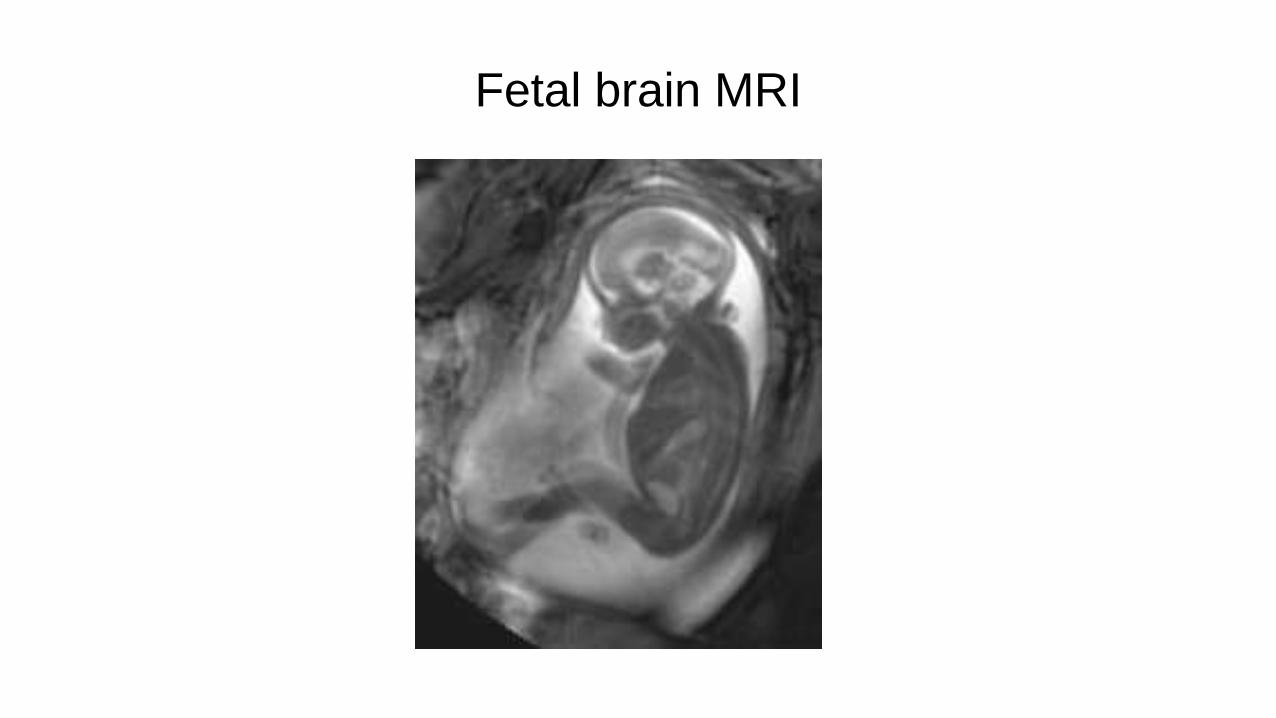
Fetal brain MRI
(a) (b) (c)
(d) (e) (f)
(g) (h) (i)
(j) (k) (l)
Jiang et al 2008
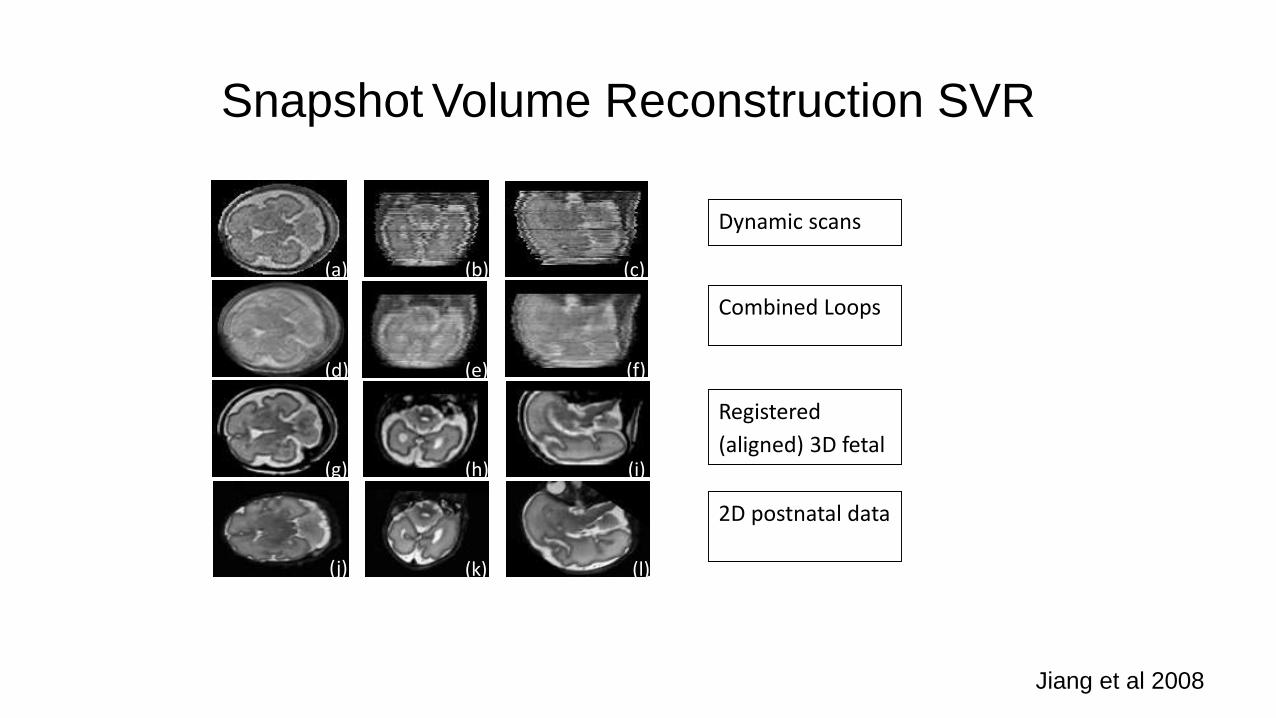
Snapshot Volume Reconstruction SVR
Jiang et al 2008
Dynamic scans
Combined Loops
Registered
(aligned) 3D fetal
2D postnatal data
Recognition of pre-surgical white matter injury
in children with CHD
2002 – MRI studies first reported about 20% infants with mixed CHD
had pre-surgical WMI, despite optimal management after delivery
and 50% after surgery
2009 - Petit, CHOP reported 38% in TGA – no post-op increase
2009 - Beca, Australasia 27% in TGA unrelated to BAS, no post-op
increase
HLHS showed post-operative increase in WMI – from 20% to 70%
potentially due to continued hemodynamic instability and lower
oxygen delivery to brain?

Evidence for pre-surgical white matter injury in the
fetus with CHD
2007 – diffusion tensor imaging and spectroscopy MRI studies
showed differences in white matter microstructure and biochemistry
2009 - MRI observational metric – Total Maturation Scale (TMS) demonstrated
delayed brain maturation at term = 35 weeks’ gest.
TMS was subsequently shown to predict 2 yrs Bailey Scales testing
2010 – reduced MRI brain volumes in CHD, from early 3rd trimester
spectroscopy showed markers (N-Acetyl Aspartate to Choline ratios) lagged behind
Worse in HLHS than for other lesions
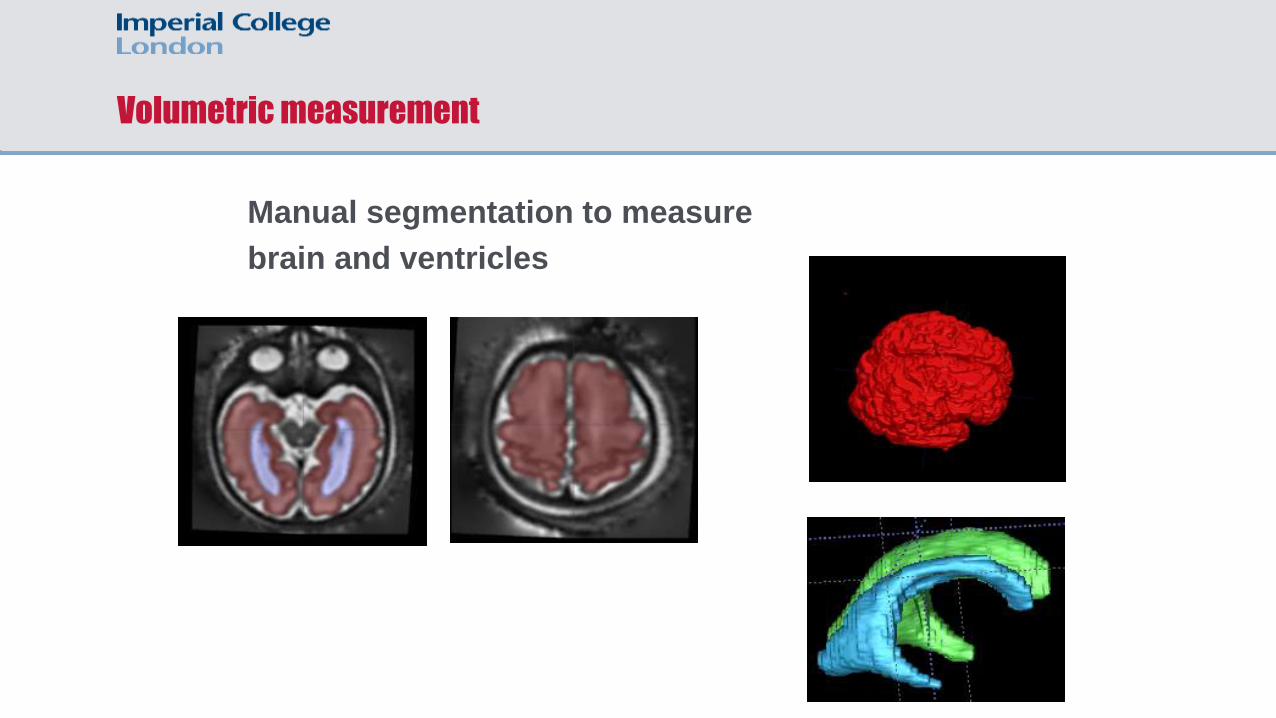
Volumetric measurement
Manual segmentation to measure
brain and ventricles

Brain Growth is Impaired in
fetuses with
Congenital Heart Disease
Jowett V, Allsop J, Fox M, Kyriakopoulou V,
Rutherford M, Gardiner H
Imperial College London
Kings College London
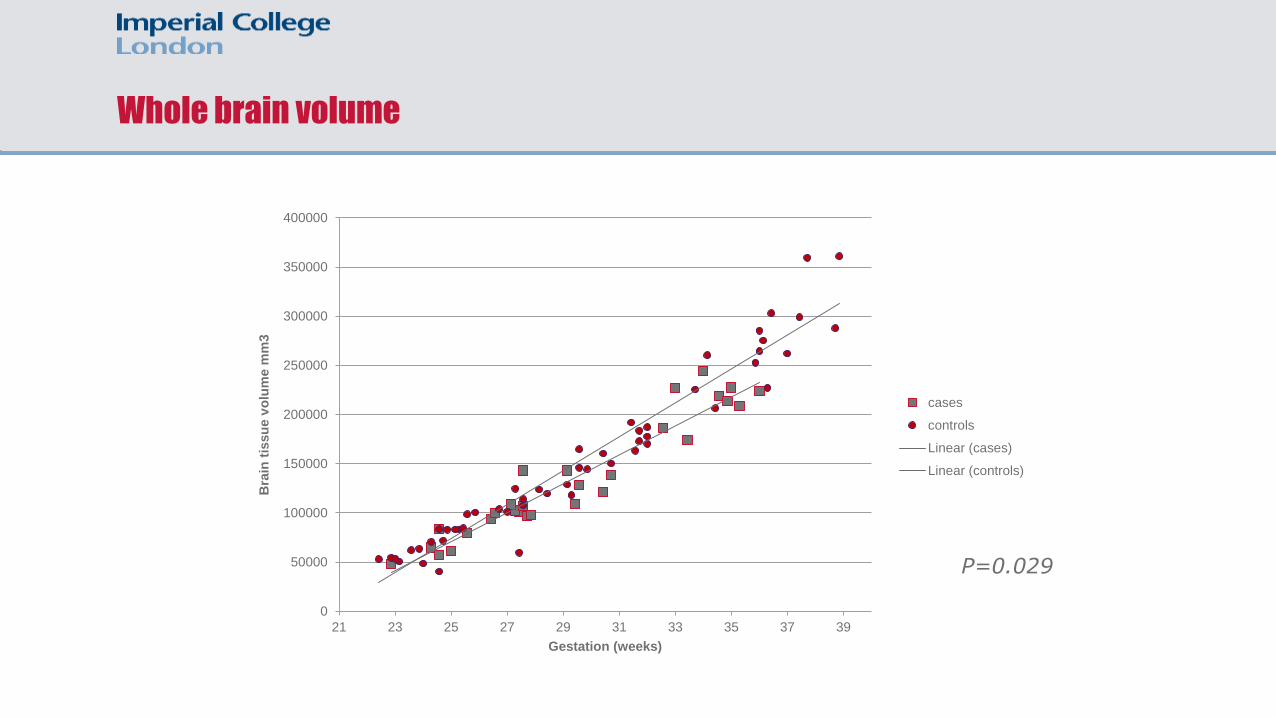
Whole brain volume
P=0.029
0
50000
100000
150000
200000
250000
300000
350000
400000
21 23 25 27 29 31 33 35 37 39
Bra
in t
issu
e v
olu
me m
m3
Gestation (weeks)
cases
controls
Linear (cases)
Linear (controls)

Longitudinal data
Longitudinal controls vs cross sectional
controls
Longitudinal cases vs cross sectional
controls
0
50000
100000
150000
200000
250000
300000
350000
400000
20 25 30 35 40
0.00
50000.00
100000.00
150000.00
200000.00
250000.00
300000.00
350000.00
400000.00
20.00 25.00 30.00 35.00 40.00
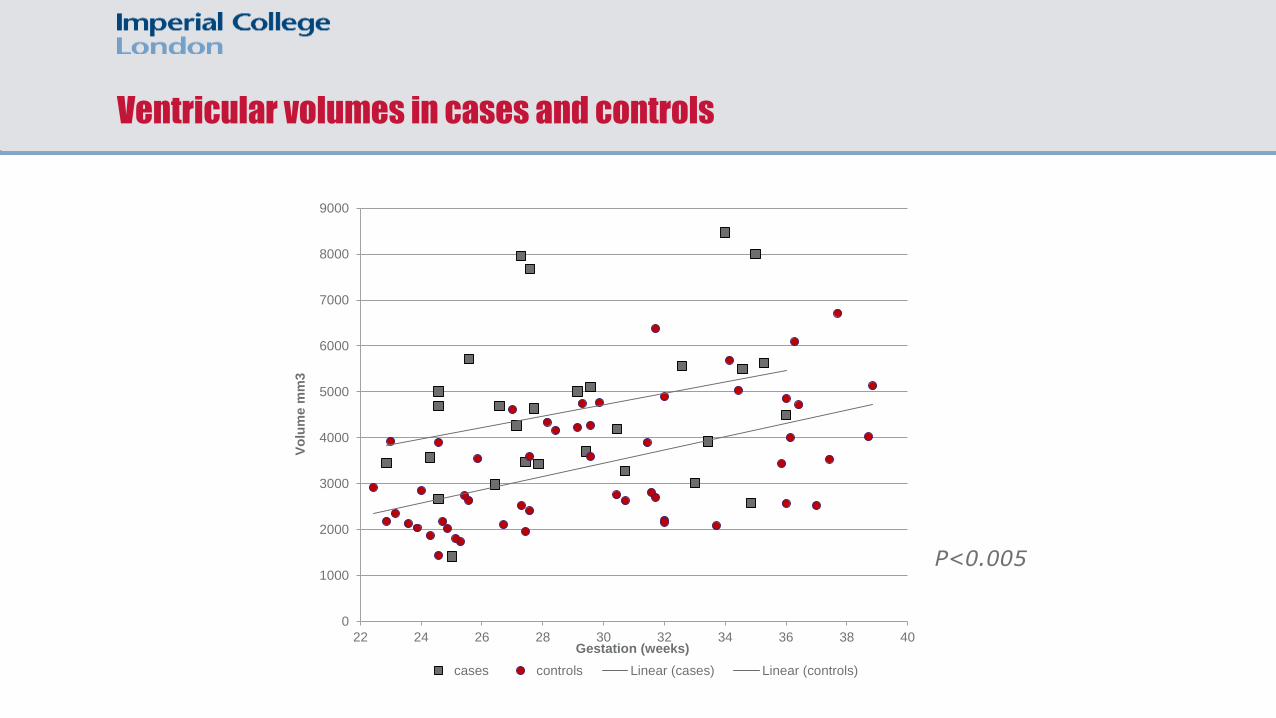
Ventricular volumes in cases and controls
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
22 24 26 28 30 32 34 36 38 40
Vo
lum
e m
m3
Gestation (weeks)
cases controls Linear (cases) Linear (controls)
P<0.005
The Journal of Thoracic and Cardiovascular Surgery 2018 155, 289-290DOI: (10.1016/j.jtcvs.2017.09.083)
Apparently, size matters…in congenital heart disease and brain injury
Paul J. Chai, MD

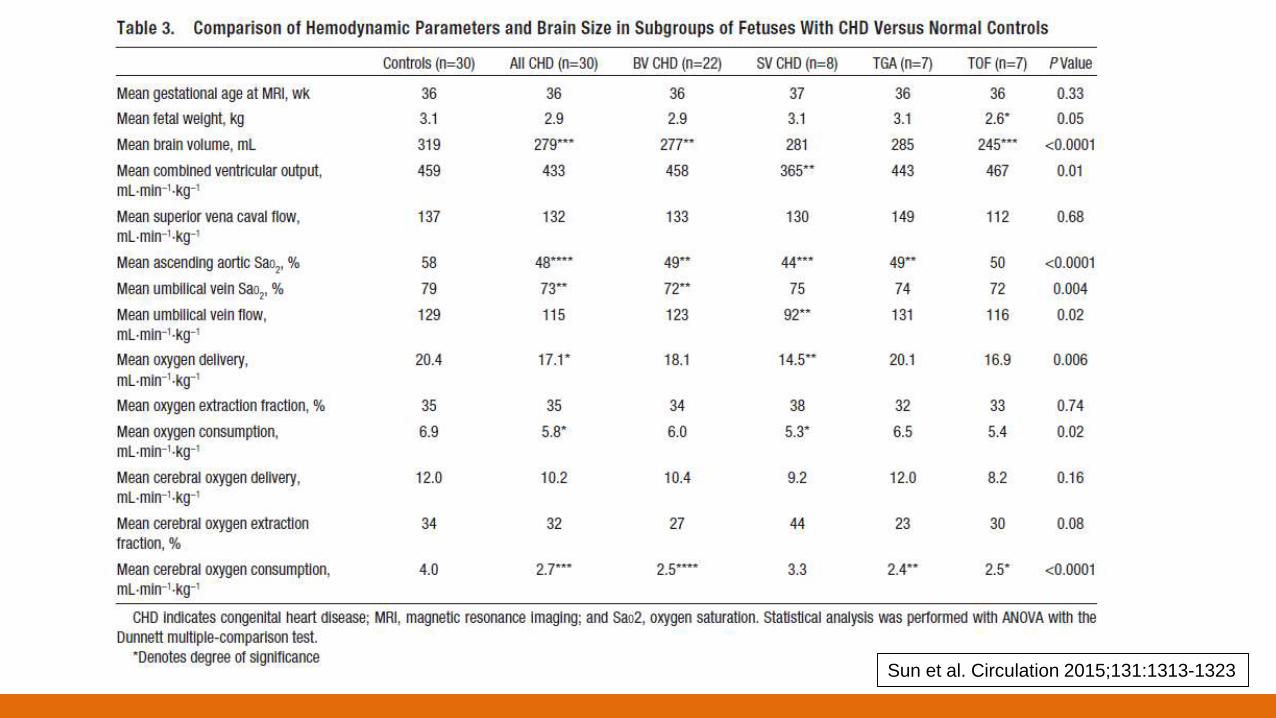
Fetal pathophysiology in the fetus with CHD
MRI technology using Metric Optimized Gating (MOG) allows phase
contrast measurements of blood flow and oximetry in large fetal
vessels
Sun et al’s case-control study of 30 CHD fetuses suggest UV return
is desaturated in CHD – implicating placental factors
Streaming to the brain is altered because of CHD – 10% reduction
The figures also suggest cerebral blood flow and oxygen extraction
were normal overall – but lesion dependent
15% reduction in cerebral oxygen delivery, 32% reduction in Vo2
and 13% reduction in fetal brain volume
Suggest using maternal oxygen therapy to rectify these differences
Sun et al. Circulation 2015;131:1313-1323

Fetal pathophysiology in the fetus with CHD
Sun et al. Circulation 2015;131:1313-1323
Sun et al. Circulation 2015;131:1313-1323
Does image abnormality = neurodevelopmental abnormality?
Thalamo-cortical and cortical to cortical connections develop in the second half
of pregnancy to produce greater functional connectivity
EEG – assess functional brain maturation and network connectivity
MRI – determines brain injury and structural development
diffusion tensor MRI – microstructural development (Fractional Anisotrophy
and Diffusivity)
Birca et al, 2016

EEG – neuronal network dysfunction
20 fetuses enrolled and studied postnatally
5/20 with MRI signs of brain injury
4 hour recordings of EEG background activity
Correlate pre-surgical brain injury on MRI with increased beta
and gamma EEG connectivity
Association with brain maturity:
Lower TMS score had higher beta frequency
High FA (mature) increased EEG connectivity
Low FA (immature) showed:
decr. EEG connectivity at low frequencies and
incr. EEG connectivity at high frequencies
White matter diffusivity not related to EEG connectivity
Spectral power density not associated with brain injury, TMS
score or microstructure scores (FA and Diffusivity)
Only brain injury was associated with background EEG pattern
spending more time in discontinuous patterns
Birca et al, 2016

Debate: interpretation of fetal evidence
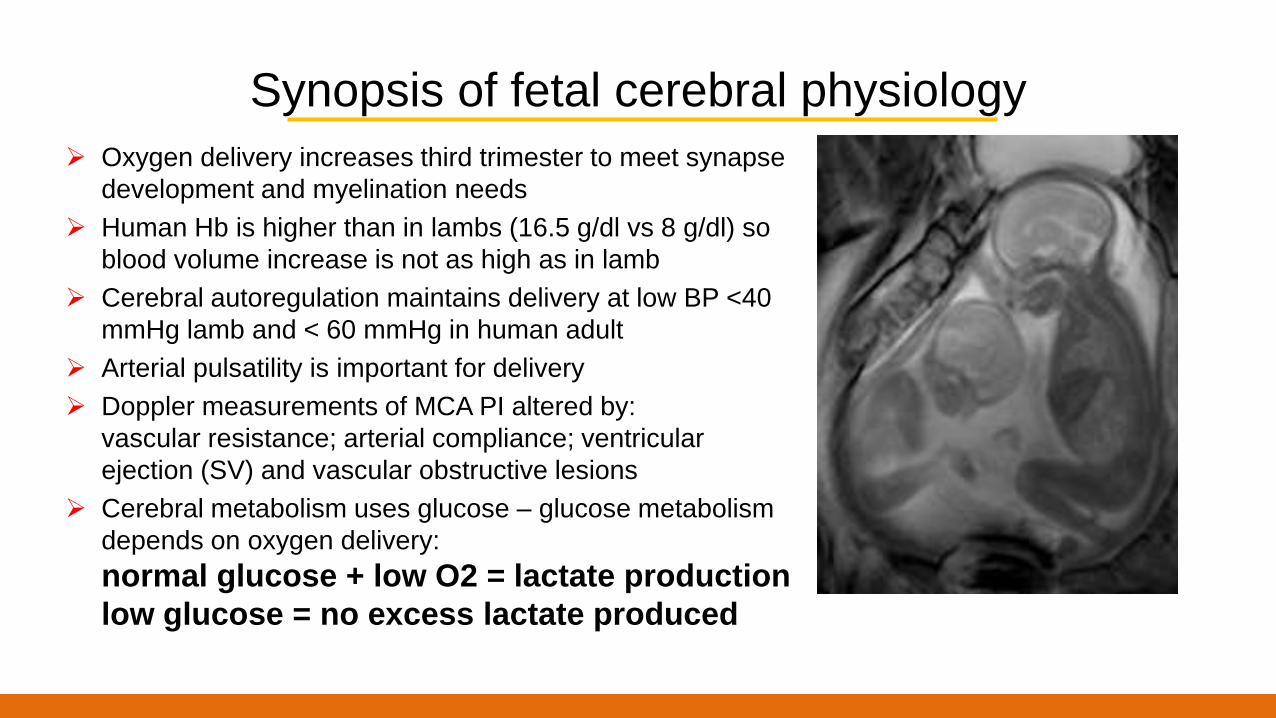
Synopsis of fetal cerebral physiology
Oxygen delivery increases third trimester to meet synapse
development and myelination needs
Human Hb is higher than in lambs (16.5 g/dl vs 8 g/dl) so
blood volume increase is not as high as in lamb
Cerebral autoregulation maintains delivery at low BP <40
mmHg lamb and < 60 mmHg in human adult
Arterial pulsatility is important for delivery
Doppler measurements of MCA PI altered by:
vascular resistance; arterial compliance; ventricular
ejection (SV) and vascular obstructive lesions
Cerebral metabolism uses glucose – glucose metabolism
depends on oxygen delivery:
normal glucose + low O2 = lactate production
low glucose = no excess lactate produced
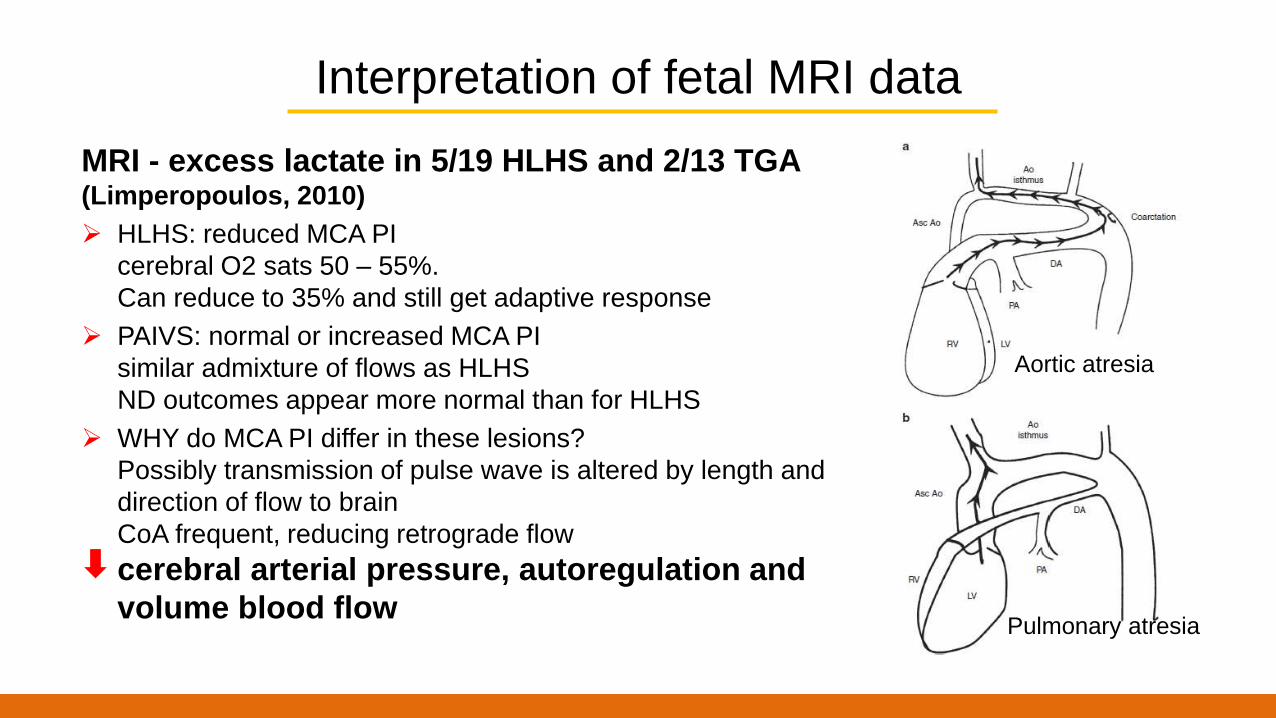
Interpretation of fetal MRI data
MRI - excess lactate in 5/19 HLHS and 2/13 TGA (Limperopoulos, 2010)
HLHS: reduced MCA PI
cerebral O2 sats 50 – 55%.
Can reduce to 35% and still get adaptive response
PAIVS: normal or increased MCA PI
similar admixture of flows as HLHS
ND outcomes appear more normal than for HLHS
WHY do MCA PI differ in these lesions?
Possibly transmission of pulse wave is altered by length and
direction of flow to brain
CoA frequent, reducing retrograde flow
cerebral arterial pressure, autoregulation and
volume blood flow
Aortic atresia
Pulmonary atresia
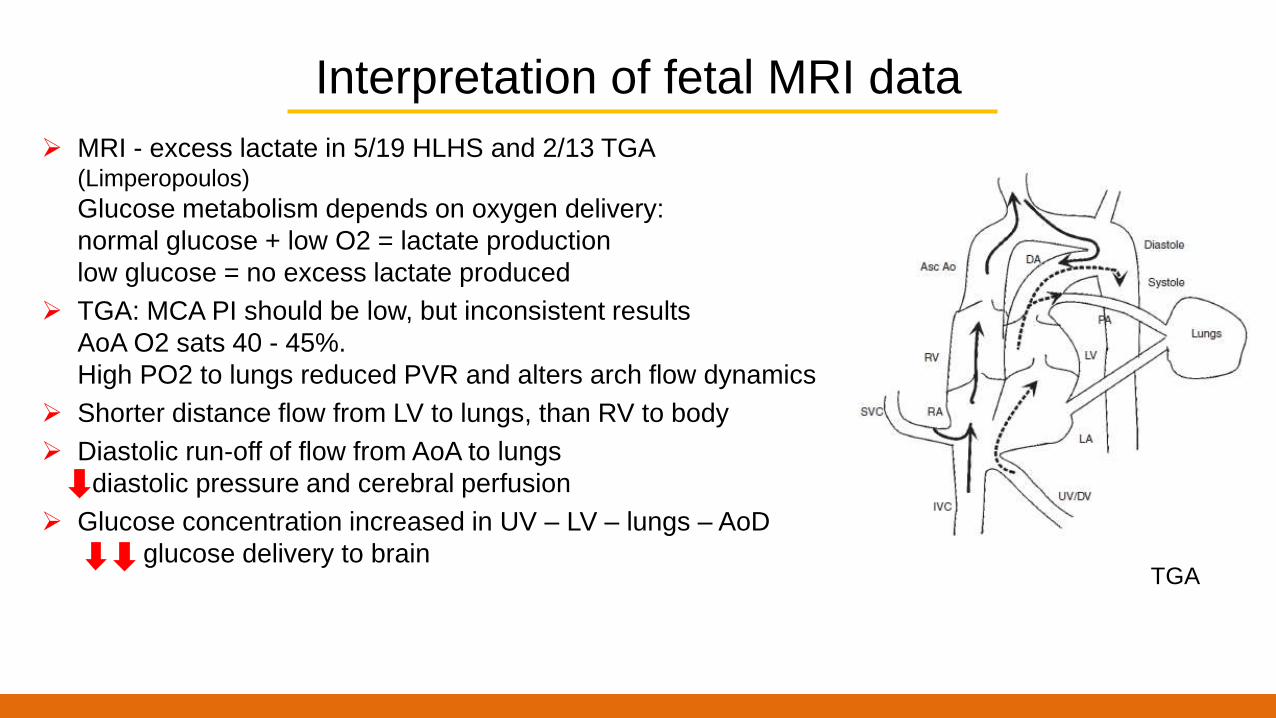
Interpretation of fetal MRI data
MRI - excess lactate in 5/19 HLHS and 2/13 TGA (Limperopoulos)
Glucose metabolism depends on oxygen delivery:
normal glucose + low O2 = lactate production
low glucose = no excess lactate produced
TGA: MCA PI should be low, but inconsistent results
AoA O2 sats 40 - 45%.
High PO2 to lungs reduced PVR and alters arch flow dynamics
Shorter distance flow from LV to lungs, than RV to body
Diastolic run-off of flow from AoA to lungs
diastolic pressure and cerebral perfusion
Glucose concentration increased in UV – LV – lungs – AoD
glucose delivery to brainTGA

Summary: surgical strategies and neuro-developmental outcome
2011 - Boston circulatory arrest study - outcome aged 16 years:
17% grade retention
25% special education
25% psychotherapy/counselling
Survivors of arterial switch procedure for TGA showed poorer academic
achievement and abnormality of fine motor function, visual spatial skills, attention
deficit and social cognition
Surgical strategies did not result in any marked differences in outcome in TGA
Dutch study: Arch lesions repaired comparing DCHA (19) vs right sided antegrade
cerebral perfusion (18)
right –sided infarcts in 6/18 vs 0/19 DCHA - 3/23 had CP at 2 years
Bailey scores within normal limits in most children
Later surgery was associated with poorer outcome – possible NICU stay and
continuing hemodynamic instability

Meta-analyses
Meta-analyses highlight some of the conflicting parameters
MCA PI confusing – studies do not deal with the physiological variables
affecting measurement
Assessment of brain anatomy likely requires MRI techniques, rather than US,
but inconsistent reporting of some lesions – subependymal cysts
Role of placental function in brain growth and genetic influences remain
uncertain as minor CHD may also be associated with low HC, BWt and
neurodevelopmental delay

Does Prenatal Diagnosis improve neuro-developmental
outcome?
Cohort of TGA and SV neonates (2001-2013)
Term newborns with pre and post-operative MRI
Outcome measures:
presence of brain injury before surgery
trajectory of postnatal brain microstructural development
96 newborns with TGA and 57 SV
Brain injury more prevalent - postnatal diagnosis:41/86 (48%) vs 16/67 (24%), p=0.03
Brain development was faster - prenatal diagnosis group:white matter fractional anisotropy increased
grey matter apparent diffusion coefficient decreased
Peyvandi at al. JAMA Pediatr. 2016

Benefits of prenatal diagnosis
Greater circulatory stability may protect the brain
Earlier surgery may minimize exposure to infection
Role of therapy pre-delivery should be explored, but is far from conclusive
BibliographyAndropoulos DB, Hunter JV, Nelson DP, Stayer SA, Stark AR, McKenzie ED, Heinle JS, Graves DE, Fraser CD Jr. Brain immaturity is associated
with brain injury before and after neonatal cardiac surgery with high-flow bypass and cerebral oxygenation monitoring. J Thorac Cardiovasc Surg.
2009; 139:543–56. [PubMed: 19909994]
Algra SO, Haas F, Poskitt KJ, Groenendaal F, Schouten AN, Jansen NJ, Azakie A, Gandhi S, Campbell A, Miller SP, McQuillen PS, de Vries LS.
Minimizing the risk of preoperative brain injury in neonates with aortic arch obstruction. J Pediatr. 2014; 165:1116–1122. e3. [PubMed: 25306190]
Algra SO, Jansen NJ, van der Tweel I, Schouten AN, Groenendaal F, Toet M, van Oeveren W, van Haastert IC, Schoof PH, de Vries LS, Haas F.
Neurological injury after neonatal cardiac surgery: a randomized, controlled trial of 2 perfusion techniques.Circulation. 2014 Jan 14;129(2):224-33.
doi: 10.1161/CIRCULATIONAHA.113.003312. Epub 2013 Oct 20.
Anderson BR, Ciarleglio AJ, Salavitabar A, Torres A, Bacha EA. Earlier stage 1 palliation is associated with better clinical outcomes and lower
costs for neonates with hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. 2015; 149:205–10. e1. [PubMed: 25227701]
Beca J, Gunn J, Coleman L, Hope A, Whelan LC, Gentles T, Inder T, Hunt R, Shekerdemian L. Pre-operative brain injury in newborn infants with
transposition of the great arteries occurs at rates similar to other complex congenital heart disease and is not related to balloon atrial septostomy. J
Am Coll Cardiol. 2009; 53:1807–11. [PubMed: 19422989]
Beca J, Gunn JK, Coleman L, Hope A, Reed PW, Hunt RW, Finucane K, Brizard C, Dance B, Shekerdemian LS. New white matter brain injury after
infant heart surgery is associated with diagnostic group and the use of circulatory arrest. Circulation. 2013; 127:971–9. [PubMed: 23371931]
Bellinger DC, Wypij D, Rivkin MJ, DeMaso DR, Robertson RL Jr, Dunbar-Masterson C, Rappaport LA, Wernovsky G, Jonas RA, Newburger JW.
Adolescents with d-transposition of the great arteries corrected with the arterial switch procedure: neuropsychological assessment and structural
brain imaging. Circulation. 2011; 124:1361–9. [PubMed: 21875911]
Birca A, Vakorin VA, Porayette P, Madathil S, Chau V, Seed M, Doesburg SM, Blaser S, Nita DA, Sharma R, Duerden EG, Hickey EJ, Miller SP,
Hahn CD. Interplay of brain structure and function in neonatal congenital heart disease. Ann Clin Transl Neurol. 2016 Aug 14;3(9):708-22. doi:
10.1002/acn3.336. eCollection 2016 Sep.PMID: 27648460
Chai PJ. Apparently size matters. The Journal of Thoracic and Cardiovascular Surgery 2018 155, 289-290DOI: (10.1016/j.jtcvs.2017.09.083
Duan AQ, Darby JRT, Soo JY, Lock MC, Zhu MY, Flynn LV, Perumal SR, Macgowan CK, Selvanayagam JB, Morrison JL, Seed M. Feasibility of
phase-contrast cine magnetic resonance imaging for measuring blood flow in the sheep fetus. Am J Physiol Regul Integr Comp Physiol. 2017 Dec
13. doi: 10.1152/ajpregu.00273.2017. [Epub ahead of print] PMID: 29351431
Goff DA, Shera DM, Tang S, Lavin NA, Durning SM, Nicolson SC, Montenegro LM, Rome JJ, Gaynor JW, Spray TL, Vossough A, Licht DJ. Risk
factors for preoperative periventricular leukomalacia in term neonates with hypoplastic left heart syndrome are patient related. J Thorac Cardiovasc
Surg. 2014; 147:1312–8. [PubMed: 23879933]
Grieve PG, Emerson RG, Fifer WP, et al. Spatial correlation of the infant and adult electroencephalogram. Clin Neurophysiol 2003;114:1594–1608.
Hansen T, Henriksen TB, Bach CC, Matthiesen NB.Congenital Heart Defects and Measures of Prenatal Brain Growth: A Systematic Review.
Pediatr Neurol. 2017 Jul;72:7-18.e1. doi: 10.1016/j.pediatrneurol.2017.03.014. Epub 2017 Apr 1.
Jansen FA, Everwijn SM, Scheepjens R, Stijnen T, Peeters-Scholte CM, van Lith JM, Haak MC. Fetal brain imaging in isolated congenital heart
defects - a systematic review and meta-analysis Prenat Diagn. 2016 Jul;36(7):601-13. doi: 10.1002/pd.4842. Epub 2016 Jun 19. Review.PMID:
27187181
Jiang S, Xue H, Glover A, Rutherford M, Rueckert D, Hajnal JV. MRI of moving subjects using multislice snapshot images with volume
reconstruction (SVR): application to fetal, neonatal, and adult brain studies. IEEE Trans Med Imaging. 2007; 26:967–80. [PubMed: 17649910]
Khalil A, Suff N, Thilaganathan B, Hurrell A, Cooper D, Carvalho JS. Brain abnormalities and neurodevelopmental delay in congenital heart
disease: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2014 Jan;43(1):14-24. doi: 10.1002/uog.12526. Epub 2013 Dec 10.
Review.
Licht DJ, Shera DM, Clancy RR, Wernovsky G, Montenegro LM, Nicolson SC, Zimmerman RA, Spray TL, Gaynor JW, Vossough A. Brain
maturation is delayed in infants with complex congenital heart defects. J Thorac Cardiovasc Surg. 2009; 137:529–36. discussion 536–7.
[PubMed: 19258059]
Licht DJ. The path forward is to look backward in time: fetal physiology: the new frontier in managing infants with congenital heart defects.
Circulation. 2015 Apr 14;131(15):1307-9. doi: 10.1161/CIRCULATIONAHA.115.016024. Epub 2015 Mar 11.
Li Y, Yin S, Fang J ,Hua Y, Wang C, Mu D,Zhou K. Neurodevelopmental delay with critical congenital heart disease is mainly from prenatal
injury not infant cardiac surgery: current evidence based on a meta-analysis of functional magnetic resonance imaging. Ultrasound Obstet
Gynecol. 2015 Jun;45(6):639-48. doi: 10.1002/uog.13436
Limperopoulos C, Tworetzky W, McElhinney DB, Newburger JW, Brown DW, Robertson RL Jr, Guizard N, McGrath E, Geva J, Annese D,
Dunbar-Masterson C, Trainor B, Laussen PC, du Plessis AJ. Brain volume and metabolism in fetuses with congenital heart disease: evaluation
with quantitative magnetic resonance imaging and spectroscopy. Circulation. 2010; 121:26–33. [PubMed: 20026783]
Lynch JM, Buckley EM, Schwab PJ, McCarthy AL, Winters ME, Busch DR, Xiao R, Goff DA, Nicolson SC, Montenegro LM, Fuller S, Gaynor
JW, Spray TL, Yodh AG, Naim MY, Licht DJ. Time to surgery and preoperative cerebral hemodynamics predict postoperative white matter injury
in neonates with hypoplastic left heart syndrome. J Thorac Cardiovasc Surg. 2014; 148:2181–8. [PubMed: 25109755]
Mahle WT, Tavani F, Zimmerman RA, Nicolson SC, Galli KK, Gaynor JW, Clancy RR, Montenegro LM, Spray TL, Chiavacci RM, Wernovsky G,
Kurth CD. An MRI study of neurological injury before and after congenital heart surgery. Circulation. 2002; 106:I109–14. [PubMed: 12354718]
Miller SP, McQuillen PS, Hamrick S, Xu D, Glidden DV, Charlton N, Karl T, Azakie A, Ferriero DM, Barkovich AJ, Vigneron DB. Abnormal brain
development in newborns with congenital heart disease. N Engl J Med. 2007; 357:1928–38. [PubMed: 17989385]
Panigrahy A, Schmithorst VJ, Wisnowski JL, et al. Relationship of white matter network topology and cognitive outcome in adolescents with D-
transposition of the great arteries. Neuroimage Clin 2015;7:438–448
Peyvandi S, De Santiago V, Chakkarapani E, Chau V, Campbell A, Poskitt KJ, Xu D, Barkovich AJ, Miller S, McQuillen P. Association of
Prenatal Diagnosis of Critical Congenital Heart Disease With Postnatal Brain Development and the Risk of Brain Injury. JAMA Pediatr. 2016
Apr;170(4):e154450. doi: 10.1001/jamapediatrics.2015.4450. Epub 2016 Apr 4.
Peyvandi S, Kim H, Lau J, Barkovich AJ, Campbell A, Miller S, Xu D, McQuillen P. The association between cardiac physiology, acquired brain
injury, and postnatal brain growth in critical congenital heart disease. J Thorac Cardiovasc Surg. 2018 Jan;155(1):291-300.e3. doi:
10.1016/j.jtcvs.2017.08.019. Epub 2017 Aug 24

Petit CJ, Rome JJ, Wernovsky G, Mason SE, Shera DM, Nicolson SC, Montenegro LM, Tabbutt S, Zimmerman RA, Licht DJ. Preoperative
brain injury in transposition of the great arteries is associated with oxygenation and time to surgery, not balloon atrial septostomy. Circulation.
2009; 119:709–16. [PubMed: 19171858]
Rivkin MJ, Watson CG, Scoppettuolo LA, et al. Adolescents with D-transposition of the great arteries repaired in early infancy demonstrate
reduced white matter microstructure associated with clinical risk factors. J Thorac Cardiovasc Surg 2013;146:543–549.
Rollins CK, Watson CG, Asaro LA, et al. White matter microstructure and cognition in adolescents with congenital heart disease. J Pediatr
2014;165:936–944.
Roy CW, Seed M, van Amerom JF, Al Nafisi B, Grosse-Wortmann L, Yoo SJ, Macgowan CK. Dynamic imaging of the fetal heart using metric
optimized gating. Magn Reson Med. 2013; 70:1598–607. [PubMed: 23382068]
Rudolph AM.Impaired cerebral development in fetuses with congenital cardiovascular malformations: Is it the result of inadequate glucose
supply? Pediatr Res. 2016 Aug;80(2):172-7. doi: 10.1038/pr.2016.65. Epub 2016 Apr 7.
Seed M. In Utero Brain Development in Fetuses With Congenital Heart Disease: Another Piece of the Jigsaw Provided by Blood Oxygen Level-
Dependent Magnetic Resonance Imaging. Circ Cardiovasc Imaging. 2017 Nov;10(11):e007181. doi: 10.1161/CIRCIMAGING.117.007181
Sun L, Macgowan C, Sled JG, Yoo SJ, Manlhiot C, Porayette P, Grosse-Wortmann L, Jaeggi E, McCrindle BW, Kingdom J, Hickey E, Miller S,
Seed M. Reduced fetal cerebral oxygen consumption is associated with smaller brain size in fetuses with congenital heart disease. Circulation.
2015; 131:1313-1323
von Rhein M, Buchmann A, Hagmann C, et al. Brain volumes predict neurodevelopment in adolescents after surgery for congenital heart
disease. Brain 2014;137:268–276.







